

Abstract
Purpose: Atrial fibrillation (AF) is the most frequent arrhythmia that follows coronary artery bypass graft (CABG). Patients developing postoperative AF (POAF) have significantly higher mortality rates. The consistent prophylactic effectiveness of statins and vitamin C are well-accepted; however, no evaluation on combined therapy has been performed. We aimed at assessing the efficacy of combination therapy with statin and vitamin C in comparison with statin alone in the prevention of post CABG-AF.
Methods: In a randomized double blind clinical trial, 120 candidates of CABG were recruited in Tabriz Madani Educational Center in a 15-month period of time. Patients were randomized into two groups of 60 receiving oral atorvastatin (40mg) plus oral vitamin C (2g/d operation day and 1g/d for five consequent days) for intervention group and oral atorvastatin (40mg) for control group. Occurrence of post CABG AF was compared between the two groups.
Results: There were 60 patients, 43 males and 17 females with a mean age of 61.0±11.5 (29-78) years, in the intervention group and sixty patients, 39 males and 21 females with a mean age of 60.5±11.3 (39-81) years, in the control group. The post CABG AF occurred in 6 cases (10%) in the interventional group and 15 patients (25%) in the controls (P=0.03, odds ratio=0.33, 95% confidence interval 0.12-0.93).
Conclusion: Based on our findings, combination prophylaxis against post CABG AF with oral atorvastatin plus vitamin C is significantly more effective than single oral atorvastatin.
Keywords: Atrial Fibrillation, Atorvastatin, Vitamin C, Coronary Artery Bypass Grafting
Introduction
Cardiac rhythm and pulse have been of great interest for the physicians of all eras.1 Atrial Fibrillation (AF) which in most of cases is self-limiting is one of the most common postoperative arrhythmias. Electrophysiological AF may be of undesirable effects on patients’ lives in short or medium term.2 Post-operative AF (POAF) has been reported as a major morbid event associated with increased post-operative thromboembolic risk and stroke, hemodynamic compromise, ventricular dysrhythmias, and iatrogenic administration complications associated with therapeutic intervention.3 Electrophysiological mechanism of AF following operation is unknown; however, atrial fibrosis or dilation could lead to AF. Pre-operation factors like atrial ischemia or damage, inflammation, adrenergic tonicity increase, catecholamine release, atrial stretch and electrolyte disorders can facilitate post-operative AF.4 Post-operative pain and emergence from anesthesia also contribute to many undesirable cardiac complications and must be treated as urgent as possible.5 Also pre-inflammatory cytokines expression, and activation of oxidases with stress oxidative increase have been suggested in the pathogenesis of the disease.4
The most consistent predictor for the development of POAF is advanced age.3 Significant increase can be seen in AF rhythm after seventies.4 More recently, obesity has also been shown to be an independent predictor of new-onset AF in the general population and in cardiac surgery patients. In a recent study, obesity was reported as a powerful risk factor for the occurrence of POAF after isolated CABG surgery in patients older than 50 years.3
Incidence rate of AF after CABG is high as some studies have demonstrated that prevalence of AF in clinical, subclinical and without cardiovascular disease are 9.1%, 4.6% and 1.6% respectively.3 In a multicenter study, most AF attacks occurred during initial days (2-5 days) of CABG.6 During initial two hours 15-30 % and within 24 hours 25-80 % of AF cases were resolved spontaneously. Persistent cases or recurrence case were treated by controlling rate and rhythm.4The post-operative period is characterized by increased adrenergic stress, and thus it might be difficult to control the ventricular rate in patients with POAF. Short acting beta-blocker agents are the therapy of choice, particularly in ischemic heart disease; but they might be poorly tolerated or relatively contraindicated in patients with known asthma or bronchospastic disease, congestive heart failure, or AV conduction block.3 Amiodarone has also been reported to be effective in controlling heart rate, and its intravenous administration has been associated with improved hemodynamic status.3
One of vitamin C mentioned mechanisms in AF pathophysiology is its inflammatory and stress oxidative role. Based on this mechanism, vitamin C prevents from creating this condition by its anti-inflammatory and anti-oxidant effect.2 Role of statins is clear in cholesterol production inhibition in declining atherosclerotic disease. Moreover statins has other effects like: on remodeling, confronting with stress oxidative, anti-inflammatory function, inhibition of effective pathologies on endothelial and providing functionality and neuro-hormonal effects.6 Song et al. studied the effect of vitamin C and statins on prevention of AF after CABG operation. Results demonstrated significant decrease in intervention group compared to placebo.6 Other study by Eslami et al. showed vitamin C accompaniment with beta-blockers decreases AF incidence significantly compared to administering beta-blockers only.2 The aim of the present study was to assess the efficacy of combination therapy with statin and vitamin C in comparison with statin alone in the prevention of post CABG-AF.
Methods
One-hundred and twenty patients who were scheduled to undergo CABG surgery were divided into two groups (each group 60 patient) for a random double-blind clinical trial. Study was completed in Tabriz Shahid Madani hospital (cardiac surgery section) for 15 months. Written informed consent was taken from all patients while they had the liberty to quit the survey in every period of study. Exclusion criteria were arterial fibrillation, left atrial hypertrophy, heart valve disease, myocardial infarction and Ejection fraction of left ventricle less than 40%. Preventive medication for AF rhythm following surgery was started by oral Atorvastatin for the control group and Atorvastatin plus Vitamin C for the intervention group.
Tablet of Atorvastatin 40 mg (daily) with oral Vitamin C (2 g in operation day and 1 g from second day until 5 day) were administered for intervention group. Tablet of Atorvastatin 40 mg plus a placebo with the same dose were used for controls.
Data were expressed in MEAN ± Standard Deviation and frequency percentage. SPSS version 15 was used for data analysis. Quantitative variables were compared by Student T-test (independent Samples). Qualitative variables were compared by Contingency Tables, Chi Square Test and Fisher‘s Exact Test (depending on circumstances). Results with P≤0.05 were recognized statistically significant.
Results
There were no significant differences between groups regarding the demographic characteristics (i.e. age, sex) distribution. No significant difference was reported between both groups regarding cardiovascular disease history, EF, history of drug use, pre-operation angiography results, ECG, ecocardiography, creatinine level, laboratory results and post-operative AF rhythm, ventricular dysrhythmia, pulmonary and renal complications, heart failure, hospitalization time in ICU and wards and drug side effects. Drug history of the Table 1.
Table 1. frequency of drug use history (percent) .
| - | Intervention | Control | P value |
| Nitrate | (85) 51 | (80) 48 | 0.47 |
| Beta-blocker | (75) 45 | (66.7) 40 | 0.32 |
| Calcium blocker | (25) 15 | (26.7) 16 | 0.84 |
| ACI | (95) 57 | (86.7) 52 | 0.12 |
| Asprin | (91.7) 55 | (90) 54 | 0.75 |
| Warfarin | (0) 0 | (1.7) 1 | 0.50 |
| Digoxin | (0) 0 | (1.7) 1 | 0.50 |
| Statin | (98.3) 59 | (93.3) 56 | 0.36 |
POAF was observed in 6 cases of the intervention group and 15 cases of the controls (Figure 1). AF rhythm percentage in the intervention group were less than controls significantly (0.95% CI: 0.12-0.93, OR= 0.33, P=0.03).
Figure 1 .
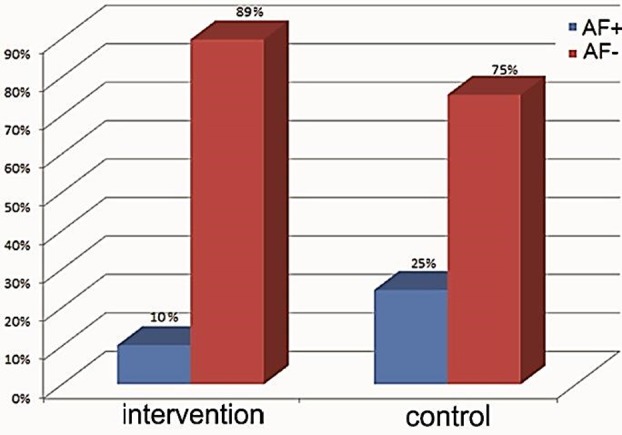
AF rhythm positive and negative percentage in the intervention group and controls
Discussion
In our study, AF rhythm cases were significantly less in the intervention group than controls (10 % vs. 25 % respectively, P=0.03, OR=0.33, 0.95% CI: 0.12-0.93). Using usual drugs (anti-arithmetic or beta-blocker) for AF rhythm prevention after heart surgeries like CABG is doubted because of their limited effects or side effects.7 Patty et el. (2006) showed significant decrease of AF rhythm incidence after using Atorvastatin (40 mg/d) as premedication compared to the control group with participation of 200 patients (35 % against 57 %, OR=0.39).8
Song et al. (2008) administered Atorvastatin 20 mg/d for 62 patients and placebo for other 62 patients. AF rhythm incidence after operation was significantly less than controls (13% vs. respectively, 27 %, OR=0.34).9-11Using vitamin C as a preventive medication for AF rhythm prevention after CABG operation was firstly studied by Carnes et al. (2001).12 Papoulidis et al. (2011) studied effects of vitamin C in 170 patients and reported significant decrease in AF rhythm incidence after CABG operation (44.7 % vs. 61.2).13 Eslami et al. (2007) used beta blocker with vitamin C (2 g for first day and 1 g for five days) in their intervention group and beta blocker for controls. AF rhythm incidence in the intervention group was significantly less than the control group (4 % vs. 26 %, OR=0.12).2 Based on the recent studies, administration of vitamin C with Atorvastatin can decline AF rhythm incidence after CABG; however, the mechanism of this effect is unknown. But some reasons like inflammation and oxidative stress decrease, electrical remodeling after CABG, decline of calcium ion aggregation and preservation of internal cellular surfaces followed by decrease in proxy nitrite damage have been introduced as AF causes in humans.2,14
Conclusion
We suggest further studies with higher sample volumes to be performed simultaneously in different matched groups to acquire more definite result.
Conflict of Interest
The authors report no conflicts of interest.
References
- 1.Khodadoust K, Ardalan M, Ghabili K, Golzari SE, Eknoyan G. Discourse on pulse in medieval Persia-the Hidayat of Al-Akhawayni (?-983AD) Int J Cardiol . 2013;166(2):289–93. doi: 10.1016/j.ijcard.2012.04.043. [DOI] [PubMed] [Google Scholar]
- 2.Eslami M, Badkoubeh RS, Mousavi M, Radmehr H, Salehi M, Tavakoli N. et al. Oral ascorbic acid in combination with beta-blockers is more effective than beta-blockers alone in the prevention of atrial fibrillation after coronary artery bypass grafting. Tex Heart Inst J . 2007;34(3):268–74. [PMC free article] [PubMed] [Google Scholar]
- 3.Echahidi N, Pibarot P, O'hara G, Mathieu P. Mechanisms, prevention, and treatment of atrial fibrillation after cardiac surgery. J Am Coll Cardiol . 2008;51(8):793–801. doi: 10.1016/j.jacc.2007.10.043. [DOI] [PubMed] [Google Scholar]
- 4.Furberg CD, Psaty BM, Manolio TA, Gardin JM, Smith VE, Rautaharju PM. Prevalence of atrial fibrillation in elderly subjects (the Cardiovascular Health Study) Am J Cardiol . 1994;74(3):236–41. doi: 10.1016/0002-9149(94)90363-8. [DOI] [PubMed] [Google Scholar]
- 5.Hosseinzadeh H, Eydi M, Ghaffarlou M, Ghabili K, Golzari SE. Esmolol: a unique beta-blocker in maintaining cardiovascular stability following neurosurgical procedures. Adv Pharm Bull . 2012;2(2):249–52. doi: 10.5681/apb.2012.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Davis Z, Jacobs HK, Bonilla J, Anderson RR, Thomas C, Forst W. Retaining the aortic fat pad during cardiac surgery decreases postoperative atrial fibrillation. Heart Surg Forum . 2000;3(2):108–12. [PubMed] [Google Scholar]
- 7.Rodrigo R, Vinay J, Castillo R, Cereceda M, Asenjo R, Zamorano J. et al. Use of vitamins C and E as a prophylactic therapy to prevent postoperative atrial fibrillation. Int J Cardiol . 2010;138(3):221–8. doi: 10.1016/j.ijcard.2009.04.043. [DOI] [PubMed] [Google Scholar]
- 8.Patti G, Chello M, Candura D, Pasceri V, D'ambrosio A, Covino E. et al. Randomized trial of atorvastatin for reduction of postoperative atrial fibrillation in patients undergoing cardiac surgery: results of the ARMYDA-3 (Atorvastatin for Reduction of MYocardial Dysrhythmia After cardiac surgery) study. Circulation . 2006;114(14):1455–61. doi: 10.1161/CIRCULATIONAHA.106.621763. [DOI] [PubMed] [Google Scholar]
- 9.Song YB, On YK, Kim JH, Shin DH, Kim JS, Sung J. et al. The effects of atorvastatin on the occurrence of postoperative atrial fibrillation after off-pump coronary artery bypass grafting surgery. Am Heart J . 2008;156(2):373 e9–16. doi: 10.1016/j.ahj.2008.04.020. [DOI] [PubMed] [Google Scholar]
- 10.Ji Q, Mei Y, Wang X, Sun Y, Feng J, Cai J. et al. Effect of preoperative atorvastatin therapy on atrial fibrillation following off-pump coronary artery bypass grafting. Circ J . 2009;73(12):2244–9. doi: 10.1253/circj.cj-09-0352. [DOI] [PubMed] [Google Scholar]
- 11.Sun YF, Mei YQ, Ji Q, Wang XS, Feng J, Cai JZ. et al. Effect of atorvastatin on postoperative atrial fibrillation in patients undergoing coronary artery bypass grafting. Zhonghua yi xue za zhi . 2009;89(42):2988–91. [PubMed] [Google Scholar]
- 12.Carnes CA, Chung MK, Nakayama T, Nakayama H, Baliga RS, Piao S. et al. Ascorbate attenuates atrial pacing-induced peroxynitrite formation and electrical remodeling and decreases the incidence of postoperative atrial fibrillation. Circ Res . 2001;89(6):E32–8. doi: 10.1161/hh1801.097644. [DOI] [PubMed] [Google Scholar]
- 13.Papoulidis P, Ananiadou O, Chalvatzoulis E, Ampatzidou F, Koutsogiannidis C, Karaiskos T. et al. The role of ascorbic acid in the prevention of atrial fibrillation after elective on-pump myocardial revascularization surgery: a single-center experience--a pilot study. Interact Cardiovasc Thorac Surg . 2011;12(2):121–4. doi: 10.1510/icvts.2010.240473. [DOI] [PubMed] [Google Scholar]
- 14.Patel D, Gillinov MA, Natale A. Atrial fibrillation after cardiac surgery: where are we now? . Indian Pacing Electrophysiol J. 2008;8(4):281–91. [PMC free article] [PubMed] [Google Scholar]