

Abstract
Primary laryngeal aspergillosis is an extremely rare opportunistic infection, especially in an immunocompetent host. Here we report a case of a 23-year-old female with a history of oral sex, which may be a suspected predisposing factor in this immunocompetent patient.
Keywords: Larynx, Aspergillus fumigatus, Oral sex, Itraconazole
Highlights
► Primary laryngeal Aspergillosis fumigates. ► A 23-year-old immunocompetent female (normal host). ► Had a history of oral sex 1 week before ill. ► Oral solution and capsules itraconazole completely cure in 1 month.
1. Introduction
Primary laryngeal aspergillosis is extremely rare, especially in immunocompetent patients. Up to now, we have known little about the developmental pathogenesis of this rare infection. The patient in our case was diagnosed with primary laryngeal aspergillosis. It suggests that the occurrence of the disease may have some correlation with oral sex. In review of the literature, we found that the age distribution and gender proportion of patients with laryngeal aspergillosis have changed dramatically, which may also support our unique viewpoint. However, more data are needed and more attention to oral sexual history should be paid to this rare but “rapidly increasing” disease.
2. Case
A 23-year-old female undergraduate student who had been experiencing hoarseness in the throat for 15 days was presented to our clinic. Initially, she began to experience hoarseness, severe paroxysmal cough and tachypnea without clear causes. She received laryngoscopy in a local hospital, white plaques were found on her vocal cords and laryngeal ventricle. After 10 days of hospital admission and treatment with anti-inflammatory medications, her cough and tachypnea disappeared. However, the hoarseness became worse than before. We carefully interviewed the patient, she was healthy in the past and denied any history of asthma and long-term use of antibiotics or corticosteroids. However, she revealed a history of oral sex (fellatio), the latest occurrence being 1 week before she became ill. A laryngoscopy was performed again and revealed obvious white plaques on the swollen vocal cords and laryngeal ventricle (Fig. 1a). Samples were taken from the vocal cords. Numerous hyphae branching at 45° angles were detected by microscopy, scanning electron microscopy (Fig. 1c) and pathology (Fig. 1d). A velvety and powdery colony was developed on Sabouraud Dextrose Agar (SDA) at 28 °C. Microscopic examination of a slide culture (Fig. 1e) was consistent with the features of Aspergillus fumigatus. DNA sequencing was also carried out to confirm the identification as previously described [1]. Genomic DNA was extracted using a DNA kit (Omega bio-tek, USA) and amplification of the intergenic transcribed spacer (ITS) regions flanking the 5.8S region of the rDNA was performed by PCR, employing the ITS-1 (5’–TCC GTA GGT GAA CCT GCG G) and ITS-4 (5’–TCC TCC GCT TAT TGA TAT GC) primers provided by Shanghai Invitrogen Biotech. The samples were subsequently sent to Invitrogen Life Technologies for DNA purification and bidirectional sequencing. The sequences were aligned using Clustal X software. A BLAST search in GenBank using the ITS sequence showed 99% homology to A. fumigatus (588/589). The sequence has been submitted to the gene data bank and registered under the accession number of JF958125. Moreover, routine laboratory tests showed her hepatic function, kidney function and immunity were normal, serum HIV-antibody was negative, and computerized axial tomography showed a normal image of her chest.
Fig. 1.
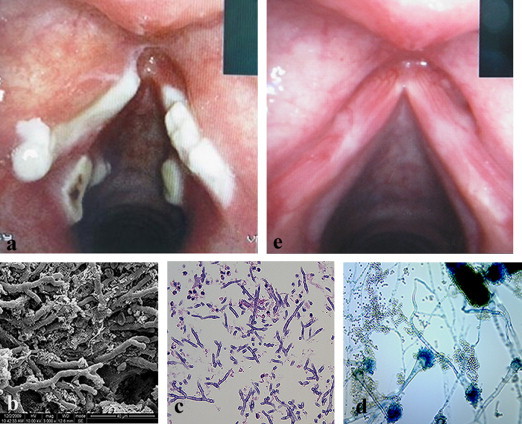
(a) Image of laryngoscopy when the patient first came to our hospital in September 21, 2009 (b) Image of laryngoscopy after 30 days of antifungal treatment in October 21, 2009, (c) SEM observation of the focus tissue, (d) Histopathological examination (HE, ×400), (e) The slide culture of the isolate (methylene blue, ×400).
The patient was diagnosed as primary laryngeal aspergillosis and treated with oral itraconazole solution (Sporanox, XIAN-JANSSEN Pharmaceutical) at 200 mg (20 ml) twice a day (keep the solution in mouth for a moment, then swallow slowly) for 5 days, followed by itraconazole capsules at 200 mg twice a day for another 25 days. The patient was cured and gradually recovered her normal voice; laryngoscopy after the treatment showed the vocal cords were smooth without any white plaque (Fig. 1b). We followed up on the patient for half a year and there was no recurrence.
3. Discussion
Primary laryngeal aspergillosis is extremely rare. So far as we know, since 1969 fewer than 50 cases have been reported in the English language literature. Advanced age, diabetes, long-term steroid therapy, chronic obstructive pulmonary disease, decline of CD4 lymphocyte cells, leukemia, lymphoma, HIV infection and other causes leading to immunocompromisation are generally the etiological factors [1]. Still, for immunocompetent patients, there are no noticeable events to explain the development of the rare infection. For our patient, fellatio may be a highly suspected predisposing factor. Although it may not be the direct cause as in the transmission of condyloma acuminata, HIV, herpes, and gonorrhea by oral-genital contact [2], by repeated friction, fellatio may cause local mucosal membrane barrier injury and edema, which may greatly contribute to the air suspended Aspergillus spores adhesion and colonization, followed by hyphae development and invasion, as the SEM shown. This patient had a relative serious symptom.
To review the related English literature, the age distribution and gender proportion of patients with laryngeal aspergillosis have changed dramatically over years (Table 1). Noticeably, the number of reported cases has increased rapidly in the past twenty years. Females among the ages of 20–40 years (who are sexually active) have a much higher incidence than males, who were the primary patients until 1997, especially in the past decade. The demographic shift from old to young and male to female, may be explained by the remarkably increased practice of oral sex [2]. However, more data are still needed, and unfortunately, many case reports lack such details. More attention to oral sexual history should be paid when this rare but “rapidly increasing” disease is diagnosed.
Table 1.
Features of 17 cases of primary laryngeal aspergillosis in immunocompetent patients.
| Authors and literatures | Published year | Patient′s gender | Patient's age (years) |
|---|---|---|---|
| 1. Rao PB [3] | 1969 | Male | 48 |
| 2. Kheir SM [4] | 1983 | Male | 50 |
| 3. Benson-Mitchell [5] | 1994 | Male | 62 |
| 4. Nong [6] | 1997 | 4 Female and 4 Male | 30–40 |
| 5. Dean [7] | 2001 | Female | 21 |
| 6. Wittkopf [8] | 2006 | Female | 62 |
| 7. Ran [1] | 2008 | Female | 36 |
| 8. Liu [9] | 2010 | 2 Female | 30/32 |
| 9. Ran [10] | 2010 | Female | 30 |
Conflict of interest
There are none.
Acknowledgments
This work was supported by Project 30570095 of the National Natural Science Foundation of China.
References
- 1.Ran Y., Yang B., Liu S., Dai Y., Pang Z., Fan J. Primary vocal cord aspergillosis caused by Aspergillus fumigatus and molecular identification of the isolate. Medical Mycology. 2008;46:475–479. doi: 10.1080/13693780701851703. [DOI] [PubMed] [Google Scholar]
- 2.Saini R., Saini S., Sharma S. Oral sex, oral health and orogenital infections. Journal of Global Infectious Diseases. 2010;2:57–62. doi: 10.4103/0974-777X.59252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rao P.B. Aspergillosis of larynx. Journal of Laryngology and Otology. 1969;83:377–379. doi: 10.1017/s0022215100070444. [DOI] [PubMed] [Google Scholar]
- 4.Kheir S.M., Flint A., Moss J.A. Primary aspergillosis of the larynx simulating carcinoma. Human Pathology. 1983;14:184–186. doi: 10.1016/s0046-8177(83)80249-4. [DOI] [PubMed] [Google Scholar]
- 5.Benson-Mitchell R., Tolley N., Croft C.B., Gallimore A. Aspergillosis of the larynx. Journal of Laryngology and Otology. 1994;108:883–885. doi: 10.1017/s0022215100128403. [DOI] [PubMed] [Google Scholar]
- 6.Nong D., Nong H., Li J., Huang G., Chen Z. Aspergillosis of the larynx: a report of 8 cases. Chinese Medical Journal. 1997;110:734–736. [PubMed] [Google Scholar]
- 7.Dean C.M., Hawkshaw M., Sataloff R.T. Laryngeal aspergillosis. Ear, Nose, and Throat Journal. 2001;80:300. [PubMed] [Google Scholar]
- 8.Wittkopf J., Connelly S., Hoffman H., Smith R., Robinson R. Infection of true vocal fold cyst with Aspergillus. Otolaryngology- Head and Neck Surgery. 2006;135:660–661. doi: 10.1016/j.otohns.2006.03.032. [DOI] [PubMed] [Google Scholar]
- 9.Liu Y., Zhou S., Ling L. Etiological factors contributing to the development of primary laryngeal aspergillosis in immunocompetent patients. Journal of Medical Microbiology. 2010;59:1250–1253. doi: 10.1099/jmm.0.021634-0. [DOI] [PubMed] [Google Scholar]
- 10.Ran Y., Li L., Cao L., Dai Y., Wei B., Zhao Y. Primary vocal cord aspergillosis and scanning electron microscopical observation of the focus of infection. Mycoses. 2011;54:e634–e637. doi: 10.1111/j.1439-0507.2010.01954.x. [DOI] [PubMed] [Google Scholar]