

Abstract
Poor complementary feeding practices and low‐quality complementary foods are significant causes of growth faltering and child mortality throughout the developing world. Ready‐to‐use foods (RUF) are energy‐dense, lipid‐based products that do not require cooking or refrigeration that have been used to prevent and treat malnutrition among vulnerable children. The effectiveness of these products in improving child nutritional status depends on household use by caregivers. To identify the key facilitators and barriers that influence appropriate in‐home RUF consumption by supplemental feeding program beneficiaries, we conducted individual interviews among caregivers (n = 80), RUF producers (n = 8) and program staff (n = 10) involved in the Byokulia Bisemeye mu Bantu supplemental feeding program in Bundibugyo, Uganda. By documenting caregiver perceptions and feeding practices related to RUF, we developed a conceptual framework of factors that affect appropriate feeding with RUF. Findings suggest that locally produced RUF is well received by caregivers and children, and is perceived by caregivers and the community to be a healthy supplemental food for malnourished children. However, child feeding practices, including sharing of RUF within households, compromise the nutrient delivery to the intended child. Interventions and educational messages informed by this study can help to improve RUF delivery to targeted beneficiaries.
Keywords: complementary feeding, cultural context, ethnographic methods, undernutrition, nutritional interventions, food intake
Introduction
Although complementary feeding programs that provide ready‐to‐use food (RUF) can both prevent and treat malnutrition (Lin et al. 2008; Matilsky et al. 2009), several clinical trials have reported low consumption of the distributed rations by targeted children (Maleta et al. 2004; 2008, 2009). In general, studies that assess RUF consumption through weekly caregiver interviews have reported high levels of compliance with RUF feeding protocols (Adu‐Afarwuah et al. 2008; Lin et al. 2008; 2008, 2009; Matilsky et al. 2009); studies that use direct observation or 24‐h recall dietary assessment methods report lower levels of intake (Maleta et al. 2004; 2008, 2009). Although supplemental feeding programs report ‘leakage’ of distributed rations within households (Beaton & Ghassemi 1982), little is known about the factors associated with low consumption of RUF in home‐based settings. To date, only the method of RUF preparation (i.e. served as a mixed dish with staple foods) and properties of the RUF (i.e. overly sweet taste) have been documented as factors associated with the low intake of RUF (2008, 2009). RUF consumption below recommended protocols might impair adequate nutrient intake and limit catch‐up growth among targeted beneficiaries (Maleta et al. 2004; Flax et al. 2010). In order to develop culturally sensitive messages to improve the consumption of distributed RUF rations, home‐based RUF feeding practices and factors influencing these practices need to be better understood.
Operated by the World Harvest Mission (WHM), the Byokulia Bisemeye mu Bantu (BBB) Program (Lubwisi for ‘Good Food for People’) is a community‐based feeding program in Bundibugyo, Uganda that uses a locally sourced and produced RUF to improve children's nutrition status through behaviour change communication and supplemental feeding. RUF is produced by four production teams, which are located near the two health centres that operate the BBB program. Production teams use hand‐powered grinders to prepare two products: (1) roasted groundnut (peanut) paste mixed with dried moringa powder and (2) roasted soy flour. Leaves of the Moringa oleifera tree, chosen because of high micronutrient content and local availability, are brought to the clinic weekly by caregivers, then transported to production teams to be dried and ground into powder (Price & Davis 2000). The RUF is delivered to two local health centres by WHM‐employed Agricultural Extension Workers and distributed by health centre staff. These two products are delivered in two plastic bags, kept separate to regulate to the proportion of ingredients, and are combined by caregivers into a homogeneous paste. This delivery method differs from other RUF products, such as Plumpy'doz© (Nutriset, Malaunay, France), which is distributed as one product in foil sachets or plastic jars. Underweight children [weight‐for‐age Z score < −2 below the World Health Organization Multicentre Growth Reference], aged 6–59 months, are enrolled in 10‐week program cycles. Although the effects of undernutrition are most effectively reversed within the first 2 years of life (Dewey & Adu‐Afarwuah 2008), the BBB program modelled the target enrolment range after supplemental feeding programs (Sandige et al. 2004; Patel et al. 2005; Ciliberto et al. 2006) due to the high prevalence of stunting among this age range in western Uganda (Jilcott et al. 2007, and because program enrolment was below capacity in the initial program cycles Jilcott et al. 2010). The ration amount and choice to provide a uniform dose of RUF across age groups was made to simplify the packaging and distribution process.
At weekly visits, local health centre staff (1) distribute a weekly ration of RUF and multivitamins with iron for enrolled children, (2) deliver nutrition education and (3) provide routine growth monitoring. A single dose of vitamin A and deworming treatment is provided upon enrolment. Weights and lengths are recorded in the program register and Ugandan Child Health Card, if available. The weekly RUF dosage (128 g day−1) provides 620 kcal and 29.5 g of protein per day.
Caregivers in the BBB program receive weekly education, delivered by community health workers and health centre staff, on the following topics: (1) the impact of early nutrition on school performance later in life; (2) antenatal nutrition; (3) growth monitoring; (4) breastfeeding; (5) healthy complementary feeding; (6) feeding children with an attentive, responsive feeding style; (7) recovery feeding after illness; and (8) hygiene (Jilcott et al. 2010). Behaviour change strategies are conveyed using the ‘BBB’ approach, developed from the Health Belief Model and Social Cognitive Theory constructs: (1) Believe benefits (perceived benefits); (2) Break down barriers (perceived barriers, self‐efficacy); and (3) Begin now (goal setting, cues to action) (Glanz et al. 2002). Initial messages specific to the RUF were to feed the food to the enrolled child only, either directly without cooking or as a thick porridge. For some commercially produced RUF products, basic instructions are often listed on the product packaging. These messages are often limited to feeding RUF directly to children with no cooking.
Follow‐up anthropometric analysis of post‐program children (n = 61) indicated that 72% of children remained underweight (Ickes 2010). Preliminary observations indicated that RUF was prepared by caregivers who diluted the supplement with a large amount of water, which raised concerns over feeding practices and subsequent nutrient delivery to enrolled children (Jilcott et al. 2010).
The purpose of this study was to identify the barriers, facilitators and cultural factors that affect in‐home feeding with RUF, distributed in the context of moderate malnutrition. These factors were used to inform culturally specific messages to promote RUF consumption by underweight children and to provide evidence for BBB program improvement strategies.
Key messages
-
•
Locally‐produced RUF is well received by Ugandan caregivers as a supplemental food for underweight children.
-
•
Sharing of RUF rations for home‐based use is common and is likely to reduce the intended dosage of RUF to targeted children.
-
•
RUF used in home‐based settings are likely to be prepared with additional cooking and are altered through the addition of other supplemental ingredients.
-
•
Education messages should highlight preparation styles that minimize adding excessive water to encourage maximum nutrient delivery to children.
-
•
Longitudinal research is needed to examine the effect of RUF‐based supplemental feeding programs on caregiver feeding practices, after free supplements are no longer provided.
Subjects and methods
Setting
Bundibugyo is in the western region of Uganda, separated from the rest of the country by the Rwenzori Mountains, and bordering the Democratic Republic of Congo. With no paved roads or electricity, Bundibugyo is one of Uganda's least developed districts and consistently ranks among the lowest districts in the country for health services and child health indicators. The majority of families rely on subsistence farming; some cultivate cocoa and coffee as cash crops. Cooking is done over open fire from wood gathered by women and children, or with charcoal in metal grills. Water for washing and drinking is collected into jerry cans where taps are available and from the local rivers in remote villages.
The Bakonjo and Babwisi are the two predominant people groups in the 290 000‐person district, which includes 52 500 (18%) children less than 5 years of age (UBOS and Macro International Inc. 2007). The prevalence of stunting [height‐for‐age Z score < −2] is 45%, compared with the national prevalence of 38% (Jilcott et al. 2007). Maternal education is directly related to stunting prevalence (Hobcraft 1993). In western Uganda, over 95% of women do not complete primary school, and 25% have never received any formal education at all (UBOS and Macro International Inc. 2007). Cultural marriage patterns also play a role in child nutrition (Hadley 2005). Women in western Uganda also are the most likely to be in a polygamous marriage with two or more co‐wives (11%). With a mean number of 7.3 total births per woman, western Uganda has one of the highest birth rates worldwide, and the median age of a woman's first marriage (17 years) is the lowest in the county (UBOS and Macro International Inc. 2007).
Participant recruitment and data collection
A total of 48 semi‐structured, in‐depth interviews were conducted with caregivers (CG), health centre staff (HC), RUF production team members (PT) and WHM agricultural extension workers (AE) (Table 1) from June to July 2008, and again in February 2009. In addition, one focus group was conducted among RUF production team members. In July–August 2009, a new set of caregivers (n = 50) who had completed the BBB program was recruited into the study to complete a post‐program survey. The purpose of the post‐program survey was to further investigate findings that arose from the initial interviews and focused specifically on the issue of sharing RUF within households and barriers to program adherence.
Table 1.
Case definitions and sample size of participants
| Participant | Case definition | Sample size (method) |
|---|---|---|
| Caregiver–child dyads (currently enrolled) | Caregiver of child currently enrolled in BBB program that brings child to weekly program or cares for child in the home. | 30 (interviews) |
| Caregiver–child dyads (post‐program) | Caregiver of child who was previously enrolled in BBB program. | 50 (surveys) |
| Health centre staff | Staff at health centres who actively participate in recruitment, education, anthropometric tracking or food distribution. | 8 (interviews) |
| Production team members | Persons who regularly (≥1/week) produce the BBB food at any of the four production sites. | 8 (interviews) and 8 (focus group) |
| Agricultural extension workers | Employees of World Harvest Mission BundiNutrition team who work with or have knowledge about the BBB program. | 2 (interviews) |
BBB, Byokulia Bisemeye mu Bantu.
Caregivers were recruited at health centres following weekly program meetings. All caregivers invited for interviews agreed to participate. Participants gave their preference for the interview location: at the health centre, home or alternative place specified by the participant. Informed consent was obtained from all participants, who were assured that shared information would be kept confidential and that participation in interviews would not affect any services received from the health centre or their relationship with the WHM. Human subjects' approval was obtained from the Institutional Review Board at the corresponding author's university and from the Bundibugyo District Health Office.
Interview questions were posed in English and translated during the interview by a trained Ugandan social worker into Lubwisi or Lukonjo, the two predominant local dialects, according to the preferred language of the participant. Responses were translated back to the interviewer. Field notes were taken during each interview to note visual cues and body language that may add to the interpretation of results. Members of the research team were not employed by the WHM and were in no way involved in the delivery of the BBB program during the research period.
Research questions and development of interview guides and caregiver survey
In order to assess the multiple levels of influence regarding BBB program utilization and child feeding practices, the social ecologic framework was used to guide the core research questions (Table 2). Briefly, interventions developed from this framework span the individual, interpersonal, community and structural (organizational) levels of influence on health behaviour (Stokols 1996) Interview guides (Table 3) were developed to explore the core research questions in depth using open‐ended questions and probes. Similar questions were posed to multiple participant groups in order to investigate corroboration or dissonance across groups. Findings from the qualitative study were used to guide the development of the structured post‐program caregiver survey.
Table 2.
Core research questions used to develop interview guides, based on the social ecological framework
| Individual level |
| • What are the current RUF‐related feeding behaviours? |
| • What challenges do caregivers face in feeding RUF to their children? |
| • What are the attitudes of health centre staff towards the BBB program? |
| • How do RUF production team members understand the purpose of their work? |
| Interpersonal level |
| • What child feeding issues and practices do caregivers discuss with one another? |
| • Which household members, including other children, influence caregiver feeding of the targeted child? |
| Institutional level |
| • What are the current educational messages that caregivers receive about RUF consumption? |
| • How are these messages perceived and implemented by caregivers? |
| • How does the interaction with BBB health centre staff influence complementary feeding practices? |
| • What challenges does the World Harvest Mission face in operating the BBB program? |
| Community level |
| • How do cultural feeding practices affect local RUF use and consumption? |
| • How do community members perceive caregivers who are enrolled in the BBB program? |
| • How do community members perceive the RUF supplement? |
RUF, ready‐to‐use food; BBB, Byokulia Bisemeye mu Bantu.
Table 3.
Sample of interview questions posed to caregivers, health centre staff, extension workers and RUF production team members involved in the BBB program
| Caregivers |
| • Who is the RUF for? What do you think the purpose of the food is for your child? |
| • What are all of the ways that your child takes (eats) the soy flour/groundnut paste? |
| • Do you do anything to prepare these foods? Tell me about these preparations. |
| • Does your child share the food with other siblings or children in the compound? |
| • How does the RUF fit into the overall diet of your child? |
| • Tell me about any ways that using the groundnut paste or soy flour with your child has affected other foods that s/he eats. |
| • Do you remember hearing any nutrition or health messages during your child's time in the BBB program? What did those messages mean to you? |
| • Is there anything that you would like the BBB program to change about the RUF that you receive? |
| Health centre staff |
| • What is the purpose of the BBB program? What is the purpose of the RUF that you distribute? |
| • What kinds of things do you discuss with the caregivers in the BBB project? |
| • Tell me about how you educate the caregivers about the RUF that you distribute. |
| • What are all of the ways that the caregivers feed the two foods to their children? |
| • What do caregivers think about the RUF that they receive? |
| • Tell me how you understand how well a child is growing as he or she continues through this program. |
| • How do the parents understand their child's growth progress throughout the program? |
| Agricultural extension workers |
| • How is the RUF that you distribute supposed to be used by caregivers? |
| • How do the caregivers actually feed the RUF to their children? |
| • What messages do the Health Centre staffs deliver during the weekly program? |
| RUF production team members |
| • What is the purpose of the RUF product that you produce? |
| • How do you get the ingredients to make the RUF? |
| • Tell me about any problems you have with obtaining the ingredients and/or making the RUF. |
| • Tell me about how the community feels about the RUF product. Has anyone asked to purchase the RUF? |
| • Tell me about the ways people use the RUF in their homes. Why do some caregivers prepare or cook the RUF for their children? |
RUF, ready‐to‐use food; BBB, Byokulia Bisemeye mu Bantu.
Data coding and analysis
All interviews were audio‐recorded, translated and transcribed into English, and back translated to the local language to monitor accuracy and clarity. Revisions were then made to the English transcripts as needed. Transcripts were read and coded by two separate analysts using AtlasTi Software Version 6.0 (Berlin, Germany). Codes were developed deductively from the interview guides and inductively from emergent themes from the interview data. After agreeing upon preliminary codes, a minimum inter‐rater reliability of >0.9 was established by testing for mutual agreement of code assignment with a sample of 10 transcripts. Direct text quotes were extracted from transcripts with participant identification numbers in order to link quotes with demographic data. Data reduction was accomplished by organizing representative quotes within each theme into schematic matrices to provide a visual display of themes. Related themes were grouped together under dimensions of the social ecological framework. Triangulation of findings from multiple participant categories was used to identify and interpret interview responses.
Survey data was tabulated into an electronic database, and response frequencies were noted. Demographic information was linked to both the interview findings and survey results in order to examine responses based on household and participant characteristics. Selected survey questions that provided further insight into qualitative interview findings are presented.
Development of conceptual framework and feeding messages
From the study findings, a conceptual framework was developed using the grounded theory approach to visually depict the interrelationships of the most important factors related to RUF feeding practices. We used the visual map feature of AtlasTi to group thematic codes that related to the key barriers and facilitators to RUF consumption that were identified from the interviews. These codes were organized around the four levels of the socio‐ecologic framework. Behaviours that contributed both positively and negatively to RUF consumption spanned the ‘facilitator’ and ‘barrier’ categories of the framework. The conceptual framework was used to guide the development of feeding messages to be incorporated into the BBB program curriculum to improve RUF consumption patterns. As a guiding principle for the development of education messages, we focused on a small number of specific key messages that can be implemented easily by the target population, instead of general advice about child feeding (Pan American Health Organization/World Health Organization 2003).
Results
Fifty codes were identified from the interview guides and from the participant responses to highlight themes related to RUF feeding practices. These codes were grouped into six families: (1) caregiver perceptions and child reactions to RUF; (2) perceptions of the BBB program's effects on child growth and health; (3) child feeding routine; (4) recall and interpretation of feeding education; (5) sharing RUF; and (6) factors affecting program adherence.
Participant perceptions and child reactions to RUF
Acceptability
Caregivers perceived the RUF positively, noting that the food helps malnourished children with ‘weak bodies’ to ‘gain strength’, ‘improve stomach problems’ or ‘gain weight’. Most participants reported high acceptability of the RUF, commenting that their child ‘likes the food so much’ and ‘eats the food well’. A mother with twins in the program noted that the RUF affected her children's energy levels: ‘When I fed them with this food they enjoyed it a lot and started playing’ (CG 8).
Perceived purpose of the RUF and comparison with home foods
While caregivers noted that the RUF was similar to the foods they usually feed young children in that the ingredients were all available locally, they commented that the RUF contained ‘more vitamins’ and was a higher‐quality food than can be made at home, where only wooden mortar and pestle are typically available for processing food.
Mothers appreciated the ‘smooth’ texture of the RUF, ‘ground well’ for small children in the hand‐powered grinders. In contrast to home foods, caregivers remarked that the RUF had a longer preservation life and could be prepared in more ways than traditional foods. Most producers noted that the key quality of the RUF was its ‘smooth texture’ and ‘softness’ compared with other local complementary foods.
Opinions about the content of the RUF
Most caregivers had no suggestions to improve the BBB food. When asked how they would feel if the two foods were mixed together in one bag, there were mixed responses. Caregivers in favour of combining the foods noted that they usually feed groundnuts and soy flour together, so combining the two beforehand would make little difference. Caregivers opposed to combining the foods valued the multiple preparation options available to them with two separate ingredients. Some providers also valued being able to control when they feed the soy flour to the children, as this product was less enjoyable than the groundnut paste. While most caregivers noted that the food lasted about 1 week, until the next distribution, many commented that the groundnut paste was finished before the soy flour.
Caregivers had mixed reactions to the moringa powder mixed into the groundnut paste. While most respondents felt that the moringa powder distinguished the RUF from other local foods and made the food ‘like medicine’ that helped the child ‘grow up well’, some others complained about the negative taste and acceptability:
My child does have problems digesting the moringa. Yesterday's groundnut paste especially had a lot of moringa and thus I am afraid to give this to my child. Therefore, I usually feed the child soybean flour because I assume that the other food [groundnut paste with moringa] may cause the child diarrhea . . . The moringa is good for you but when there is too much, it means that the food does not taste good anymore. (CG 4)
Some caregivers noted the BBB program taught them that moringa could be fed to young children. With this knowledge, and because moringa was abundant in home gardens, caregivers note that they have started including it in other child meals.
Perceptions of the BBB program's effects on child growth and health
Many caregivers felt that the BBB program was critical to improving the health of their children who were ‘sickly’, ‘weak’ or ‘malnourished’ before the program. A direct connection between the child's weight and health was clearly understood by all caregivers who often desired for their children to increase their ‘kilos’ or ‘put on more weight’. Caregivers often remarked that children's appetites increased after the program began, crediting the high nutritional quality of the RUF and children's acceptability of the supplement. Most caregivers understood the weekly weighing to be a way to monitor children's growth, ‘to see if we have been feeding our children well’. However, there was disagreement among caregivers about the quality of growth monitoring communication. Usually, health centre staff communicated the child's progress with parents and would ask questions about the child's health and feeding, especially if the weight decreased from the previous week or did not improve over time. However, in several cases, caregivers had to read the child's weight from the program register, which was problematic given the low literacy skills of many participants. Overall, the staff noted that the program improved the way the health centres treat malnutrition and felt more empowered in their growth monitoring and nutrition education skills.
As community members who did not participate in the BBB program were not included in the study, the perceptions of community members were captured indirectly through responses from caregivers and production team members. Caregivers noted that it was often a community member's concern about a child's appearance that prompted them to seek help for their malnourished children. Several caregivers learned about the BBB program from their neighbours and friends, while some caregivers received questions from neighbours about how they could enrol their children in the program. Community members noted a direct connection between the RUF and improving nutrition. One production team member noted the effects of the RUF:
When [the RUF] is given to a child – even when he had been terribly malnourished – he gains energy and good health. Even when the hair had started to become brown or reddish, it starts to change by being black and dark.
Observed as a good‐tasting and useful food for helping children ‘grow well and gain energy’, neighbours of caregivers and RUF producers inquired about where they could get the RUF for their own families.
When other people, mostly women, find when I have prepared this food for my children and they are feeding, they always get spoon and eat some, so they say the food is good and continue to say ‘that is why this food is helping your children.’ So they encourage me to continue feeding my children with this food since it tastes good. (CG 8)
When caregivers were asked how their children's growth has been affected by the RUF, most noted some improvement in their children's weight. Improvements were also attributed to other complementary foods that they began feeding as a result of the education and encouragement they received from the BBB program, such as avocados, eggs and greens, but also noted that these foods were difficult for them to obtain due to ‘lack of money’.
In cases where children did not gain weight during the program, caregivers attributed lack of improvement to pre‐existing, mostly unexplained, health conditions: ‘Despite the fact that the child is feeding on the BBB food, he is not improving. So there are definitely other factors involved here as well’ (CG 4). Others felt only partially encouraged by their child's improvement: ‘I think my child is still sick and not yet healthy. Despite him feeding on this food, my child is still weak’ (CG 20).
Production teams and other community members also recognized improvements in children's weights and energy levels, and reinforced these positive reactions to the RUF. One production team leader noted that program participants noticed different responses to the BBB RUF compared with other local foods fed to children:
Sometimes the people ask us for what we put in the soy flour to make it different and good for the children. This is because they have their soy beans in the village and try to feed them to their children, but there is no change brought. (PT 3)
Child feeding routine
RUF and the caregiver feeding schedule
Caregivers reported that the RUF was easily incorporated into the normal child feeding routine. Some caregivers credited the BBB program and RUF with helping them get on a ‘regular feeding schedule’ with their children. While some reactively fed children when they began to cry, many caregivers' noted regular daily schedules for child feeding:
I always wake up early in the morning to cook for them and feed them at eight. After they eat, I go to my garden to dig. I come back at noon, cook for them again and also prepare the evening family food and their food separately . . . I always come back quickly and in time from the garden because I always think about my children's feeding and care when I am digging. (CG 18)
One health worker remarked that most caregivers feed both RUF and breast milk to their children; however, the RUF helps when the mother is separated from the child.
But what others do is to only cook for their children in the morning the food they can eat for the long time the moms are gone for gardening. So what happens is that almost half of the day the child does not breastfeed but only feeds off the BBB, which alone cannot make the child grow well. Also some mothers only feed their children only this BBB and don't supplement it, so that one also stops a child from growing well. (HC 7)
RUF preparation
Preliminary research findings in the study setting suggested that both cooking RUF to mix with staple foods and diluting the RUF with water may impair the nutrient intake from the RUF. Therefore, the issue of RUF preparation was explicitly explored. In general, most caregivers cooked the RUF, and this method was the recommended procedure from health centre staff. Some caregivers noted instructions from health centre staff to use small pieces of groundnut paste as snacks for children, while others did not recall such messages. Feeding RUF directly to children was mostly an occasional approach used to pacify a crying child and was met with mixed reactions. Some children ‘loved it right from the bag’ and ‘immediately stopped crying’. However, in a culture where nearly all foods are boiled before eating, some caregivers feared that the ‘uncooked’ groundnut paste would cause diarrhoea or more severe sickness, or was simply not accepted by children.
The child sometimes eats the real [uncooked] paste when he sees his mother cooking it. But other members of the family always want to stop him since it is not good to eat the uncooked paste. I have not received any education about this [feeding the RUF with no preparation]. We [the family] assume that if the child continues eating the uncooked groundnut paste, he or she will die. (CG 15)
Despite pre‐cooking the ingredients during production, some producers also felt that the RUF could not be eaten without additional cooking. As one producer noted, ‘This food needs to be cooked for babies because it might not be easy for their digestion if it is not cooked’ (PT 4).
Integration of RUF into family foods
All caregivers reported feeding other foods in addition to the RUF; however, many noted that more of their child's food came from the BBB program than from family foods, and that their children preferred the RUF to other foods. The most common complementary foods fell into three categories: (1) starch‐based staples (boiled green bananas, boiled cassava flour, rice, Irish potatoes, sweet potatoes, millet flour); (2) protein‐based ‘sauces’ (groundnut sauce, beans, soy beans, fresh fish, amaranth, boiled cassava leaves); and (3) nutrient‐rich ‘supplements’ (eggs, tomatoes, avocadoes, papaya, passion fruit).
In most cases, RUF was prepared as porridge, or prepared as a ‘sauce’ and mixed with a starch‐based staple food. Table 4 summarizes the most common RUF recipes, ingredients and preparation techniques. More so than breakfast or lunch, the evening meal was the occasion for additional supplements to the children's RUF‐based meals, including foods from the family meal such as cooked greens, beans and fish.
Table 4.
Frequent recipes that contain the Byokulia Bisemeye mu Bantu and ready‐to‐use food (RUF)
| Name of RUF recipe | Ingredients and preparation |
|---|---|
| Katoga and RUF | Prepared as a sauce consisting of boiled groundnut paste and/or soy flour (1–3 tbsp each, plus water) and mixed with one or more of the following staples: mashed boiled green bananas (matoke), Irish potatoes, maize flour (posho) or rice. Sometimes includes palm oil, tomatoes, onions, boiled cabbage or greens (i.e. amaranth) and salt. |
| Kahunga and RUF | Prepared as a sauce consisting of boiled groundnut paste and/or soy flour (1–3 tbsp each, plus water), which was spooned up with a thick dough of boiled cassava flour. |
| Porridge | Boiled water with soy flour (1–3 tbsp), sugar, and sometimes groundnut paste (1–3 tbsp). |
| Directly ‘as bread’ | A piece of unprepared groundnut – moringa paste. |
Most caregivers noted feeding complementary foods between two and four times a day, in addition to regular breastfeeding. Caregivers who reported breastfeeding their children were asked how the RUF has affected their breastfeeding schedule. No caregiver reported a reduction in breastfeeding after starting the program, and some noted that the RUF helped them to supplement their breast milk, which they felt was no longer enough to feed their growing child.
Many caregivers reported preparing separate meals and using separate bowls for the enrolled child to better ‘monitoring how this child is eating’ and to improve hygiene: ‘I want to see my child in good health. I have to make sure when I am cooking, I stay around my child's food so that there is no contamination to make my child sick again’ (CG 13). Despite the considerable time taken to prepare the RUF, caregivers were not discouraged by the preparation of separate meals for the enrolled children.
I prepare [the RUF] and the family food together. But the child's food [the RUF] gets ready first because it is easy to cook, and we were told not to overcook it. So as the family food continues to get ready, I start feeding my twins. My twins eat first. (CG 18)
Recall and interpretation of feeding education
Health centre staff described the content of the program education, which emphasized continued breastfeeding, variety, hygiene, responsive feeding, meal size, thickness of complementary foods and feeding frequency. While health centre staff noted that they would educate caregivers to ‘not depend on the BBB food alone in feeding’ children, but to also feed children soft, nutrient‐rich foods such as avocados, eggs and greens, most caregivers reported that they were unable to purchase these foods, despite wishing to provide their children with these foods.
At the time of the interviews, all caregivers had been present at a minimum of three program sessions and could recall at least one education message from the BBB program. When asked to explain the activities of the BBB program, both caregivers and health centre staff recalled feeding education as a key program component. Most caregivers summarized the education in terms of providing good care and proper feeding for their children, noting both specific points (i.e. feed the child at least three times a day) and general concepts (i.e. to take good care of the child when feeding). While a few caregivers noted that their long commute to the health centre occasionally caused them to miss the education, there was an overall strong recall and understanding of messages. The most commonly recalled feeding and care topics were meal frequency, diversity of complementary foods, ‘monitoring children when they eat’ and maintaining good hygiene.
They teach us about how you should cook well the child's food, clean well the saucepan in which the child's food is cooked, clean well the plates where the child will eat the food from, when you cook the food you bring soy [flour] and gnut paste mix them together, cover the food while on fire, and when the food gets ready you find a place to sit and begin feeding a child. (CG 2)
Several mothers knew to avoid excessive dilution when preparing the RUF: ‘. . . so that the food is not too watery and the food can therefore be able to stay in the child's stomach for a longer period of time’ (CG 14). Caregivers also noted that an appropriate meal size could limit leftovers that may not be consumed: ‘We put a small amount of water for us to cook little and just enough for him so that he eats it all and does not leave anything. We don't want to waste the child's food and we want him to always eat all the food that he is given at the health centre’ (CG 22).
Sharing RUF
Caregivers in the initial interviews were asked if anyone besides the enrolled child consumed the RUF. While many caregivers could recall instructions from the health centre staff to feed to the food to only the targeted child, sharing of RUF was explicitly reported by several of the initially interviewed caregivers. To further investigate the issue of sharing, an open‐ended question was included in a follow‐up survey that was conducted 10 months after the initial interviews to ask post‐program caregivers: ‘Was it ever a challenge to you to feed the RUF to only the child enrolled in the program?’ to which 34 of 50 (68%) of respondents replied positively. The primary reasons for this challenge, assessed in a subsequent close‐ended question, ranged from food insecurity to the cultural norm of food sharing (Table 5).
Table 5.
Survey responses that highlight the primary reason that giving RUF to only one child is a challenge for caregivers (n = 50)
| Primary reason that feeding RUF to only one child is a challenge | Response | Percent (%) |
|---|---|---|
| ‘It is part of our culture. I cannot feed the food only to one child.’ | 10 | 20 |
| ‘The child in the program did not eat the food.’ | 3 | 6 |
| ‘After the one child finished eating, I gave the food to other children.’ | 10 | 20 |
| ‘There was not enough other food around to feed the other children.’ | 11 | 22 |
RUF, ready‐to‐use food.
Post‐program caregivers were also asked to describe this challenge in their own words. The responsibility of feeding many young children within a household added strain on the caregiver's ability to feed the RUF to only one child. One 28‐year‐old mother whose child was discharged from program 1 month prior to interview noted the strong cultural value to sharing food with everyone present at mealtime:
Every time I prepared the BBB food – or any other food – I called all of the other children who are the same age as this one, because these children are too much used to each other. This one (pointing to the child who participated in the BBB program) cannot eat [the RUF] with the other children just looking. They have to share it. (CG 31)
His other brothers would give me a hard time when I gave [the RUF] to him while they observed without any food for them. I sometimes prepared the food [RUF] as family sauce. (CG 44)
Providing a protein‐rich, more expensive ‘sauce’ to round out an otherwise starch‐based diet was a challenge for caregivers. Hence, the RUF was sometimes used when sauce could not be obtained for families: ‘If I would run short of sauce, I would get some of her food [RUF] to supplement ours’ (CG 65). A second mother described her preparation style as a way to stretch the RUF: ‘I add dodo [amaranth], tomatoes, cabbage – but small quantities for each of these things. Sometimes, I put more ingredients into this food, so that it can feed more people’ (CG 13).
In the case of households where sharing was not reported, caregivers recounted measures such as using a separate bowl, or setting aside a separate feeding time in order to ensure that the RUF was given only to the one child enrolled in the program.
Factors affecting regular program adherence
Caregivers walked between 500 m and 10 km each week to one of the health centres to participate in the BBB program. An attendance record abstracted from the program register indicated that among caregivers interviewed and surveyed (n = 80), the mean ± standard error attendance rate was 7.4 ± 0.3 out of 10 visits. Caregivers cited transportation to the program as a barrier to participation, particularly during bad weather. Health centre staff noted that some caregivers come from far distances, especially those residing in the Democratic Republic of Congo, who arrive late to the program, or ‘are disturbed by the soldiers at the border who do not let them through’. Caregivers with several young children also reported that it was sometimes difficult to attend the program when the enrolled child or another child in the household was sick. Program staff complained that some caregivers missed distribution days, which they believed slowed children's recovery. Staff suggested that to increase enrolment and improve attendance, they could ‘sensitize communities’ by doing outreach and home visits, especially in remote villages.
A question in the follow‐up survey further explored the barriers to program attendance. Seventy‐four per cent (37 of 50) of caregivers noted that it was a challenge to attend the BBB program every week, citing difficulties with transportation (46%), failure to complete all activities instructed by health centre staff (30%), sickness of the child (15%), personal sickness (22%) and the need to tend to domestic chores and gardening (14%). As one mother noted: ‘I would forego most of my domestic chores and garden work every Tuesday for the program. I always felt tension about bringing the child every week to the health unit because it frustrated some of my working schedule days and plans’ (CG 45).
The length of the program was also frustrating to some caregivers, who had to leave other children to attend the program.
Leaving home other children without a caregiver kept me upset at the health unit every time there was a delay. (CG 51)
Conceptual framework of factors affecting RUF consumption
The key barriers and facilitators to appropriate supplemental feeding with RUF were organized into a conceptual framework (Fig. 1) that describes the relationships between these factors and their effect on nutrient delivery to children. Factors included in the framework span the levels of the social ecological model. At the individual level, caregiver motivation to improve children's weight and health encourages regular feeding with RUF. Caregiver preparation of RUF can contribute positively to appropriate child feeding by ensuring good hygiene and by encouraging other nutrient‐rich foods to be added to child meals. At the interpersonal level, preparation of RUF may also use up a larger portion of the distributed ration at one time, may be more likely to be get shared with other children and may be diluted with water, which reduces the nutrient density of the RUF. The resemblance of the BBB RUF with locally available complementary foods was a facilitating community factor, whereas the lack of a cultural concept of food that is ‘ready to use’ was a community‐level barrier to supplemental feeding with RUF in an unprepared form. Structural factors, such as long commutes to the program clinic, combined with the competing demand of household responsibilities may prohibit caregivers from regularly obtaining the RUF at weekly program visits.
Figure 1.
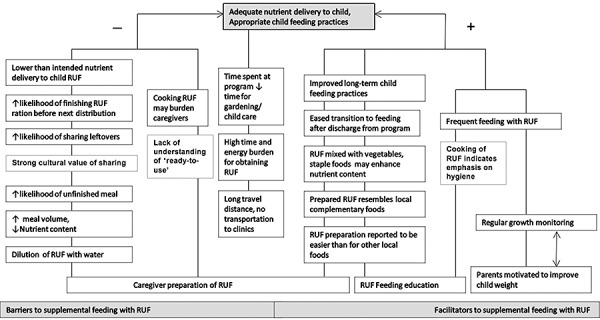
Conceptual framework of barriers and facilitators to home‐based supplemental feeding with ready‐to‐use food (RUF).
RUF feeding education messages
In response to the barriers presented in the conceptual framework, three feeding messages were developed for the BBB program curriculum (Table 6) in order to improve RUF consumption by children.
Table 6.
Key barriers to RUF consumption and corresponding program messages
| Barrier to RUF consumption | Recommended feeding message |
|---|---|
| RUF was often used as sauce on top of staple foods, rarely eaten directly and heavily diluted with water during cooking. | ‘Feed the RUF to your child as a thick sauce in small amounts so that she can finish all that you prepare. If you add water, boil and cool the RUF before feeding.’ |
| Soy and groundnut RUF supplements not always consumed together, affecting nutrient composition and quality of supplement | ‘Mix groundnut paste and soy flour bags together at the clinic so they can always be eaten together.’ |
| Caregivers unaware that they can bring home foods to grind at RUF production team sites | ‘Bring your ground nuts and soybeans to a production team near your home to make smooth foods for your child.’ |
RUF, ready‐to‐use food.
Discussion
Initially designed and demonstrated to be effective to treat severe malnutrition in hospital or outpatient settings (Collins & Sadler 2002; Diop et al. 2003; Sandige et al. 2004), RUFs have been modified and more broadly applied to treat moderate malnutrition (Maleta et al. 2004; Patel et al. 2005), to prevent moderate and severe wasting (Isanaka et al. 2009) and to support breastfeeding replacement feeding for human immunodeficiency virus‐positive mothers (van der Horst et al. 2009). With this broad application, it becomes increasingly important to understand the cultural factors that affect RUF consumption in home‐based settings. To our knowledge, this is just the second qualitative study among recipients of RUF (Flax et al. 2009) and the first within an ongoing community‐based supplemental feeding program using RUF. The purpose of this study was to identify the barriers and facilitators that affect in‐home feeding with RUF, distributed to treat undernutrition.
It has been previously demonstrated that supplemental feeding program rations are likely to be shared within households especially when they are similar to the food that families regularly eat (Beaton & Ghassemi 1982). Studies using RUF give a mixed picture with regard to sharing. Those studies that used weekly interviews indicated that there is very little sharing of the supplementary food (Lin et al. 2008; Phuka et al. 2008, 2009; Matilsky et al. 2009), whereas those that collected data through dietary recalls and direct observation found that the quantities of RUF eaten by participants was small (Maleta et al. 2004), and that there was direct and indirect sharing (Flax et al. 2010). The present study supports research showing that RUF provided to young children is shared within families and adds to the literature by describing in mothers' own words the economic and cultural norms that lead to sharing.
Health centre staff and caregivers differed in their descriptions of child feeding patterns during RUF use. While staff believed that caregivers fed RUF irregularly and without any additional complementary foods, caregivers credited the RUF with enhancing the regularity of child feeding. The integration of RUF into the complementary feeding pattern, described by mothers here, is similar to research from Malawi, which found that the introduction of RUF did not change feeding frequency (Flax et al. 2008). Although there is evidence from other studies that caregivers may choose to mix RUF with other foods, such as porridge (2008, 2010), the present study provides the first evidence of producers and mothers reporting that they feel uncomfortable using a ready‐made product due to their belief in the importance of cooking food for young children to ensure food safety. This finding points to the importance of considering cultural factors when designing child feeding interventions, as has been demonstrated in several other settings (Bentley et al. 1991; Creed‐Kanashiro et al. 2003; Kanashiro et al. 1991).
Both caregiver and health centre staff noted program attendance as a key barrier to RUF delivery. Into addition to long commutes – acknowledged by health centre staff – caregivers were frustrated by the length of program sessions, which sometime started late and caused them to forgo work and child care responsibilities at home. Moreover, caregivers described the challenge of maintaining their personal health. During a typical program session, caregivers – mainly women – commute up to 10 km by foot in hot conditions and sacrifice an entire afternoon to attend the program. Knowledge of these challenges lend support to the idea that supplemental feeding programs may improve adherence by providing supportive incentives to concurrently enrolled caregivers, and not just targeted children.
Strengths and limitations
The study may have been affected by social desirability bias, in that caregivers may have given responses about the program and their own participation in it that fit with what they thought the interviewers or program staff expected from them. However, mothers' frank discussion about sharing RUF and some of the difficulties or barriers to their participation suggest that the presence of social desirability bias was limited. The strengths of this study include the use of interviews in the local language by indigenous speakers who were trained in qualitative research methods; the inclusion of multiple participant groups who supply, administer, and participate in the BBB supplemental feeding program; and the setting of the study within a nutrition program. The program described in the present study is a variant of the many forms of community‐based feeding and is therefore of relevance to the public health nutrition planners.
Conclusions
As RUF production scales up throughout the developing world to support a multinational trend towards community‐based management of malnutrition, the practical aspects of in‐home feeding with RUF need to be understood in various cultural settings. The results of this study provide evidence that is both particular to the study setting and generally applicable to similar remote, rural regions where caregivers face the ongoing challenge of feeding their children adequately. The education that accompanies free food rations in complementary feeding interventions should continue to be informed by culturally relevant research, as presented in this study. Future studies that assess the adequacy of nutrition program beneficiaries' diets after program discharge will be helpful to understand the potential for food rations, including RUF, delivered in combination with education, to promote long‐term improvement in dietary adequacy and child feeding practices of malnourished and at‐risk children.
Source of funding
This work was funded by a GlaxoSmithKline Duke‐UNC Global Health Research Grant and through a Carolina Center for Public Service Entrepreneurship in Public Service Fellowship.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Acknowledgements
The authors would like to thank Baguma Charles for translating the interviews and Maya Mahin for assistance in coding the transcripts. We also thank the reviewers for their helpful comments on earlier versions of this paper.
References
- Adu‐Afarwuah S., Lartey A., Brown K.H., Zlotkin S., Briend A. & Dewey K.G. (2008) Home fortification of complementary foods with micronutrient supplements is well accepted and has positive effects on infant iron status in Ghana. American Journal of Clinical Nutrition 87, 929–938. [DOI] [PubMed] [Google Scholar]
- Beaton G. & Ghassemi H. (1982) Supplemental feeding programs for young children in developing countries. American Journal of Clinical Nutrition 35, 864–916. [DOI] [PubMed] [Google Scholar]
- Bentley M.E., Dickin K.L., Mebrahtu S., Kayode B., Oni G.A., Verzosa C.C., Brown K.H. & Idowu J.R. (1991) Development of a nutritionally adequate and culturally appropriate weaning food in Kwara State, Nigeria: an interdisciplinary approach. Social Science & Medicine 33, 1103–1111. [DOI] [PubMed] [Google Scholar]
- Ciliberto M.A., Manary M.J., Ndekha M.J., Briend A. & Ashorn P. (2006) Home‐based therapy for oedematous malnutrition with ready‐to‐use therapeutic food. Acta Paediatrica 95, 1012–1015. [DOI] [PubMed] [Google Scholar]
- Collins S. & Sadler K. (2002) Outpatient care for severely malnourished children in emergency relief programmes: a retrospective cohort study. The Lancet 360, 1824–1830. [DOI] [PubMed] [Google Scholar]
- Creed‐Kanashiro H.M., Bartolini R.M., Fukumoto N.M., Uribe T.G., Robert R.C. & Bentley M.E. (2003) Formative research to develop a nutrition education intervention to improve dietary iron intake among women and adolescent girls through community kitchens in Lima, Peru. Journal of Nutrition 133 (Suppl.), 3987–3991. [DOI] [PubMed] [Google Scholar]
- Dewey K.G. & Adu‐Afarwuah S. (2008) Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Maternal and Child Nutrition 4, 24–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diop H.I., Dossou N.I., Ndour M.M., Briend A. & Wade S. (2003) Comparison of the efficacy of a solid ready‐to‐use food and a liquid milk‐based diet for the rehabilitation of severely malnourished children: a randomized trial. American Journal of Clinical Nutrition 78, 302–307. [DOI] [PubMed] [Google Scholar]
- Flax V.L., Ashorn U., Phuka J., Maleta K., Manary M.J. & Ashorn P. (2008) Feeding patterns of underweight children in rural Malawi given supplementary fortified spread at home. Maternal and Child Nutrition 4, 65–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flax V.L., Thakwalakwa C., Phuka J., Ashorn U., Cheung Y.B., Maleta K. & Ashorn P. (2009) Malawian mothers' attitudes towards the use of two supplementary foods for moderately malnourished children. Appetite 53, 195–202. [DOI] [PubMed] [Google Scholar]
- Flax V.L., Phuka J., Cheung Y.B., Shorn U., Maleta K. & Ashorn P. (2010) Feeding patterns and behaviors during home supplementation of underweight Malawian children with lipid‐based nutrient supplements or corn‐soy blend. Appetite 54, 504–511. [DOI] [PubMed] [Google Scholar]
- Glanz K., Rimer B.K. & Lewis F.M. (2002) Health Behavior and Health Education, 3rd edn, Jossey Bass: San Francisco, CA. [Google Scholar]
- Hadley C. (2005) Is polygyny a risk factor for poor growth performance among Tanzanian agropastoralists? American Journal of Physical Anthropology 126, 471–480. [DOI] [PubMed] [Google Scholar]
- Hobcraft J. (1993) Women's education, child welfare and child survival: a review of the evidence. Health Transition Reviews 3, 159–175. [PubMed] [Google Scholar]
- van der Horst C., Chasela C., Ahmed Y., Hoffman I., Hosseinipour M., Knight R. et al (2009) Modifications of a large HIV prevention clinical trial to fit changing realities: a case study of the Breastfeeding, Antiretroviral, and Nutrition (BAN) protocol in Lilongwe, Malawi. Contemporary Clinical Trials 30, 24–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ickes S.B. (2010) Assessment of supplemental feeding with a locally‐produced ready‐to‐use‐food: The Byokulia Bisemeye mu Bantu Program in Bundibugyo, Uganda. Doctoral Dissertation, The University of North Carolina at Chapel Hill. Proquest Digital Dissertations, University of North Carolina at Chapel Hill Graduate School, N.C., USA.
- Isanaka S., Nombela N., Djibo A., Poupard M., Van Beckhoven D., Gabouland V. et al (2009) Effect preventive supplementation with ready‐to‐use‐therapeutic food on the nutrition status mortality, and morbidity of children aged 6 to 60 months in Niger: a cluster randomized trial. Journal of the American Medical Association 301, 277–285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jilcott S.B., Masso K.A., Ickes S.B., Myhre S.D. & Myhre J.A. (2007) Surviving but not quite thriving: anthropometric survey of children aged 6 to 59 months in a rural western Uganda district. Journal of the American Dietetic Association 107, 1983–1988. [DOI] [PubMed] [Google Scholar]
- Jilcott S.B., Ickes S.B., Myhre J.A. & Ammerman A.S. (2010) Iterative design, implementation and evaluation of a supplemental feeding program for underweight children ages 6–59 months in western Uganda. Maternal and Child Health 14, 299–306. [DOI] [PubMed] [Google Scholar]
- Kanashiro H., Fukumoto M., Bentley M.E., Jacoby E., Verzosa C. & Brown K. (1991) Use of recipe trials and ethnographic techniques for the development of a home‐prepared weaning food in the central highlands of Peru. Journal of Nutrition Education 23, 30–35. [Google Scholar]
- Lin C.A., Manary M.J., Maleta K., Briend A. & Ashorn P. (2008) An energy‐dense complementary food is associated with a modest increase in weight gain when compared with a fortified porridge in Malawian children aged 6–18 months. Journal of Nutrition 138, 593–598. [DOI] [PubMed] [Google Scholar]
- Maleta K., Kuittinen J., Duggan M.B., Briend A., Manary M.J., Wales J. et al (2004) Supplementary feeding of underweight, stunted Malawian children with a ready‐to‐use food. Journal of Pediatric Gastroenterology and Nutrition 38, 152–158. [DOI] [PubMed] [Google Scholar]
- Matilsky D., Maleta K., Maleta K., Castleman T. & Manary M.J. (2009) Supplemental feeding with fortified spreads results in higher recovery raters than with a corn/soy blend in moderately wasted children. Journal of Nutrition 139, 773–778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pan American Health Organization/World Health Organization (2003) Guiding Principles for Complementary Feeding of the Breastfed Child. PAHO: Washington, DC. [Google Scholar]
- Patel M.P., Sandige H.L., Ndekha M.J., Briend A., Ashorn P. & Manary M.J. (2005) Supplemental feeding with ready‐to‐use therapeutic food in Malawian children at risk of malnutrition. Journal of Health, Population, and Nutrition 23, 351–357. [PubMed] [Google Scholar]
- Phuka J., Maleta K., Thakwalakwa C., Cheung Y.B., Briend A., Manary M.J. & Ashorn P. (2008) Complementary feeding with fortified spread and incidence of severe stunting in 6 to 18 month old rural Malawians. Archives of Pediatrics & Adolescent Medicine 162, 619–626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phuka J., Thakwalakwa C., Maleta K., Cheung Y.B., Briend A. & Manary M.J. (2009) Supplementary feeding with fortified spread among moderately underweight 6 to 18 month old rural Malawian children. Maternal and Child Nutrition 5, 159–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price M.L. & Davis K. (2000) The Moringa Tree. ECHO technical note. Available at: http://www.food-security.info/pdf%20(English)/ECHO%20(English)/Moringa.pdf
- Sandige H., Ndekha M.J., Briend A., Ashorn P. & Manary M.J. (2004) Home‐Based Treatment of Malnourished Malawian Children with Locally Produced or Imported Ready‐to‐Use Food. Journal of Pediatric Gastroenterology and Nutrition 39, 141–146. [DOI] [PubMed] [Google Scholar]
- Stokols D. (1996) Translating social ecological theory into guidelines for community health promotion. American Journal of Health Promotion 10, 282–298. [DOI] [PubMed] [Google Scholar]
- Uganda Bureau of Statistics (UBOS) and Macro International Inc. (2007) Uganda Demographic and Health Survey 2006. UBOS and Macro International Inc.: Calverton, MD. [Google Scholar]