

Abstract
Purpose
Sagittal spine and pelvic alignment of adolescent idiopathic scoliosis (AIS) is poorly described in the literature. It generally reports the sagittal alignment with regard to the type of curve and never correlated to the thoracic kyphosis. The objective of this study is to investigate the relationship between thoracic kyphosis, lumbar lordosis and sagittal pelvic parameters in thoracic AIS.
Methods
Spinal and pelvic sagittal parameters were evaluated on lateral radiographs of 86 patients with thoracic AIS; patients were separated into hypokyphosis group (n = 42) and normokyphosis group (n = 44). Results were statistically analyzed. The lumbar lordosis was lower in the hypokyphosis group, due to the low proximal lordosis. The thoracic kyphosis was not correlated with any pelvic parameters but with the proximal lordosis. The pelvic incidence was correlated with sacral slope, pelvic tilt, lumbar lordosis and highly correlated with distal lumbar lordosis in the two groups. There was a significant linear regression between thoracic kyphosis and proximal lordosis and between pelvic incidence and distal lordosis.
Conclusions
We can consider that the proximal part of the lordosis depends on the thoracic kyphosis and the distal part depends on the pelvic incidence. The hypokyphosis in AIS is independent of the pelvic parameters and could be described as a structural parameter, characteristic of the scoliotic deformity.
Keywords: Adolescent idiopathic scoliosis, Thoracic hypokyphosis, Lumbar lordosis, Pelvic incidence, Sagittal pelvic, Spinal parameters
Introduction
Recent publications have shown the importance of considering the sagittal spinal and pelvic alignments for the treatment of spinal pathologies [1].
Duval-Beaupère [2] described the relationship between the pelvic anatomy and lumbar lordosis. They introduced the pelvic incidence (PI) angle, which is an anatomical parameter characteristic of the pelvic shape of each individual, unaffected by the orientation of the pelvis.
Many authors [2–12] showed that there are correlations between the adjacent pelvic and spinal sagittal parameters: PI and sacral slope (SS), PI and pelvic tilt (PT), PI and lumbar lordosis (LL), SS and LL and finally LL and thoracic kyphosis (TK). PI is the only parameter that is anatomically fixed and it determines all spine and pelvis balances. PI determines SS and PT. SS, which is also the distal part of the lordosis, determines LL. In turn, LL balances with TK. This upward successive influence provides the spino-pelvic balance of the upright position. For a normal person, we can consider that the kyphosis is related to the PI through LL.
In adult scoliotic patients [13], the authors found the same correlation between PI and LL. However, the correlation between LL and TK has been only found for lumbar or thoracolumbar curves by Legaye [5].
In some studies [14–18] regarding the adolescent idiopathic scoliosis (AIS), authors [16, 17] found the same correlation between the pelvic parameters and LL, but did not find any correlation between LL and TK. The lumbar lordosis of adolescents with idiopathic scoliosis is dependent on the PI, as with the adult population. However, unlike adults, the kyphosis of AIS patients seems to be independent of the LL. However, the correlation was not analysed according to the value of TK.
We hypothesized that this difference between normal population and AIS is due to the low value of the kyphosis characteristic of thoracic AIS. The objective of this study was to determine the relationship between TK, LL and PI in thoracic AIS, and if the hypokyphotic patients have a spino-pelvic balance different from the normokyphotic patients. A better understanding of this relationship could be beneficial for the analysis and the treatment of thoracic AIS.
Materials and methods
Radiographic preoperative measurements were extracted from a prospective database of consecutive AIS seen for surgery in one orthopaedic paediatric centre from July 2000 to June 2010. The patients were classified according to Lenke classification. 86 cases (75 females and 11 males) were selected according to inclusion criteria: Thoracic AIS (Lenke 1 to 4) and TK inferior or equal to 45°. Two groups were defined by the value of TK: hypokyphosis group (HKG; TK <20°, n = 42) and normokyphosis group (NKG; 20° ≤ TK ≤ 45°, n = 44). The mean age was 14.6 years (±1.98) (range 11–18). The mean primary Cobb angle of the main curve was 56.7° (range 40°–104°), with a mean reducibility of 48 %. No difference was observed between the two groups in terms of age, sex, mean coronal Cobb angle, reductibility of the curves, type of Lenke curves and coronal balance.
Radiographic measurements
For all patients, standing posterior–anterior (PA) and lateral digital radiographs of the spine and pelvis were taken as a part of the routine evaluation of the preoperative scoliosis cases. The lateral radiographs were taken on the same medical imaging network with the same technique in standing position with the arm lying horizontally, hand on a support and visualizing the entire spine from the auditive canals to the proximal extremity of the femur. PA radiographs in supine lateral bending position had been made before surgery to evaluate the flexibility and the reducibility of the curve. The quality of digitalized film and the possibility to change the contrast on the computer allowed good visualisation of the femoral heads and the vertebral bodies notably in the proximal part of the thoracic spine. All the measurements were done by the same operator (JLC). Two sagittal spinal parameters and three sagittal pelvic parameters (Fig. 1) were evaluated:
The thoracic kyphosis was defined as the angle between the superior end-plate of T4 and the inferior end-plate of T12.
The lumbar lordosis was the angle between the inferior end-plate of T12 and the superior end-plate of S1.
The Pelvic Incidence was defined as the angle between the perpendicular of the sacral endplate and the line which joins the middle of the sacral endplate and the hip axis.
The sacral slope (SS) was defined as the angle between the sacral endplate and a horizontal line.
The PT was defined as the angle between the vertical line and the line which joins the middle of the sacral endplate and the hip axis. PT was positive when the hips lie in front of the centre of the sacral plate.
Fig. 1.
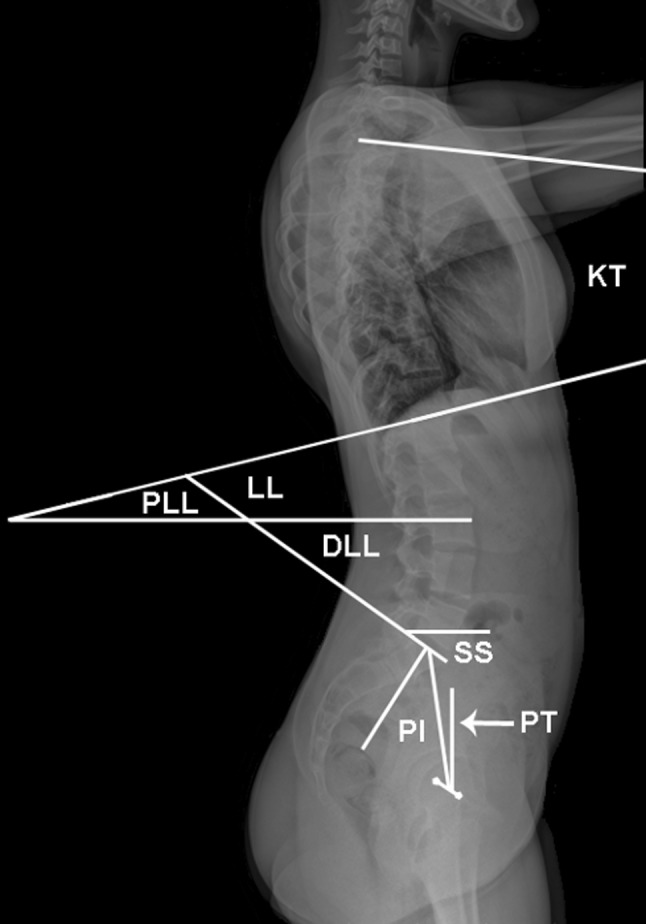
Sagittal pelvic and spine parameters. The hip axis is located midway between the centre of the femoral heads. Pelvic Incidence (PI) is always equal to the sum of sacral slope (SS) and pelvic tilt (PT). Lumbar Lordosis (LL) measured between T12 and S1, is divided in the Proximal Lumbar Lordosis (PLL) under the apex of the lordosis and Distal Lumbar Lordosis (DLL) below the apex. SS is equivalent to DLL. Thoracic kyphosis (TK) is measured between T4 and T12
Usually, the femoral heads are not superimposed, and the hip axis was defined as the middle of the line joining the centre of the two femoral heads. Geometrically, PI always equals to the sum of SS and PT.
According to Vaz and Roussouly [12], LL was divided into proximal and distal lumbar lordosis (DLL) (Fig. 1). Proximal Lumbar Lordosis (PLL) or lordosis over the apex is the angle between the inferior end-plate of T12 and the horizontal line which correspond to the apex of the lordosis. PLL is the part of the lordosis lying over the horizontal line independently to a vertebral level. DLL is the angle between the horizontal line and the sacral plate. DLL is the lordosis under the apex, DLL is geometrically equivalent to SS. PLL was calculated as the difference between LL and SS.
Global sagittal balance was also measured between the C7 sagittal plumb line (C7PL) and the posterior point of the sacral end plate. The balance was determined positive if C7 was shifted anteriorly and negative if C7 shifted posteriorly. A patient was considered imbalanced if the global sagittal balance was superior to 2 cm or inferior to −2 cm.
Statistical analysis
After testing the normal distribution of quantitative values, the Wilcoxon test was used to compare those parameters between the two independent groups. Correlations of pelvic and spinal parameters were analyzed using the Spearman test on the whole cohort and within the two groups. A linear regression plot was performed to explain lordosis’ parts by Pelvic parameters. Significant p value was considered as p < 0.05 and p < 0.016 for multiple correlation tests. All analysis were performed using JMP® software, version 8.0 (SAS Institute).
Results
Spine and pelvic parameters distribution in AIS
Mean values and standard deviations of each parameter for the global cohort, HKG and NKG are presented in Table 1 with reference to the values of healthy adolescents and adults. For adolescent normal values, we present the lower and the higher value found in the literature [17, 19–22]. As expected, TK was significantly different (p < 0.0001) between HKG (8.2°) and NKG (30.8°) and the whole cohort (19.8°). LL was lower in the HKG (43.1°) than in the NKG (49.4°). This difference was significant (p = 0.02). It is not due to DLL, which is equivalent for the two groups, but due to the PLL which is lower in the HKG (3°) compared to the NKG (11.8°) (p < 0.0001). For pelvic parameters, PI, SS and PT were not different for the two groups and close to the normal values of adolescent population. There was a trend (p = 0.08) for a higher PI for the HKG (51.1°) and a lower PI for the NKG (47.4°).
Table 1.
Spinal and pelvic parameters in thoracic adolescent idiopathic scoliosis
| Groups | TK | LL | SS = DLL | PLL = LL–SS | PI | PT |
|---|---|---|---|---|---|---|
| Total cohort (N = 86) | 19.8 ± 13.4 | 46.3 ± 11.5 | 38.8 ± 8.9 | 7.5 ± 9.5 | 49.2 ± 11.1 | 10.4 ± 7.4 |
| HKG (N = 42) | 8.2 ± 7.7 | 43.1 ± 12 | 40.1 ± 9.5 | 3 ± 10 | 51.1 ± 11.4 | 11 ± 7.5 |
| NKG (N = 44) | 30.8 ± 6.7 | 49.4 ± 10.3 | 37.6 ± 8.2 | 11.8 ± 6.7 | 47.4 ± 10.7 | 9.9 ± 7.3 |
| p value: HKG/NKG | <0.0001* | 0.0201* | NS | <0.0001* | 0.0861 | NS |
| Adolescent | 27.9–44.2 | 49.2–58.8 | 37.1–41.6 | 7.8–18 | 45.5–49.1 | 7.2–8.4 |
| Adult | 47 | 47 | 39 | 8 | 52 | 12 |
TK Thoracic kyphosis, LL lumbar lordosis, PI pelvic incidence, SS sacral slope, PT pelvic tilt PLL proximal lumbar lordosis, DLL distal lumbar lordosis, HKG hypokyphosis group, NKG normokyphosis group
Adolescent: normal adolescent lower and higher values of the literature; adult: normal adult mean values
*Statistically significant difference (p < 0.05)
Correlations
The results of the correlation analysis of pelvic and spinal parameters using the Spearman test are summarised in Tables 2 and 3 with all the significant correlation’s coefficients. TK (Table 2) was not correlated with any pelvic parameters. With regard to TK and LL, TK was only correlated with LL in the whole cohort. However, TK was correlated with PLL for the whole cohort and for the HKG, but not for the NKG. PI (Table 3) was correlated with PT and LL, and highly correlated with DLL for the two groups and the whole cohort. PI was not correlated with PLL.
Table 2.
Correlations between thoracic kyphosis and other parameters
| Groups | TK–PI | TK–PT | TK–LL | TK–DLL | TK–PLL |
|---|---|---|---|---|---|
| Total cohort (N = 86) | NS | NS | ρ = 0.33 p = 0.0022* |
NS | ρ = 0.46 p = 0.0032* |
| HKG (N = 42) | NS | NS | NS | NS | ρ = 0.34 p = 0.0237 |
| NKG (N = 44) | NS | NS | NS | NS | NS |
TK Thoracic kyphosis, LL lumbar lordosis, PI pelvic incidence, SS sacral slope, PT pelvic tilt, PLL proximal lumbar lordosis, DLL distal lumbar lordosis, HKG hypokyphosis group, NKG normokyphosis group
* With Bonferoni correction for multiple tests, the significance of p values persisted
Table 3.
Correlations between pelvic incidence and other parameters
| Groups | PI–PT | PI–LL | PI–DLL | PI–PLL |
|---|---|---|---|---|
| Total cohort (N = 86) | ρ = 0.62 p < 0.0001* |
ρ = 0.45 p < 0.0001* |
ρ = 0.73 p < 0.0001* |
NS |
| HKG (N = 42) | ρ = 0.50 p = 0.0008* |
ρ = 0.50 p = 0.0009* |
ρ = 0.75 p < 0.0001* |
NS |
| NKG (N = 44) | ρ = 0.73 p < 0.0001* |
ρ = 0.50 p = 0.0005 |
ρ = 0.67 p < 0.0001* |
NS |
TK Thoracic kyphosis, LL lumbar lordosis, PI pelvic incidence, SS sacral slope, PT pelvic tilt, PLL proximal lumbar lordosis, DLL distal lumbar lordosis, HKG hypokyphosis group, NKG normokyphosis group
* With Bonferoni correction for multiple tests, the significance of p values persisted
These correlations were confirmed by the significant linear regressions we found between TK and PLL and between PI and DLL, shown in Figs. 2 and 3.
Fig. 2.

Linear regression plots of Thoracic kyphosis (TK) in function of a lumbar lordosis (LL) and, b distal lumbar lordosis (DLL) and c proximal lumbar lordosis (PLL)
Fig. 3.

Linear regression plots of Pelvic incidence (PI) in function of a lumbar lordosis (LL) and, b distal lumbar lordosis (DLL) and c proximal lumbar lordosis (PLL)
Sagittal balance
13 (31 %) patients were imbalanced in the HKG and 17 (38 %) in the NKG. This difference was non-significant. The imbalance was independent of the value of the kyphosis.
Discussion
Because the spinal and pelvic sagittal parameters increase during the growth [20], we performed the comparison of our results to the values of healthy adolescents found in the literature [17, 19–22] and to the previously published AIS values [16–18, 23, 24].
Upasani [17] and Mac Thiong [16] found a higher PI in thoracic AIS than in normal adolescent. In our study, the pelvic parameters were similar to the parameters of healthy adolescents as well as Roussouly et al. [24]. The PI was similar to the white AIS patients of Lonner [18] but inferior to his black patients (56°).
Regarding the whole cohort, TK (19.8°) was similar to the published values of thoracic AIS [16–18] (18.9°–22.9°) but, as expected, was lower than the value of normal adolescent (27.9°–44.2°). LL (46.3°) was moderately lower compared to the normal adolescents (49.2°–58.8°), but was similar to the values of AIS of Mac-Thiong [16] (40.8°) and Lonner [18] (42.2°). The results of these studies differ from the value of publications by Roussouly [24] (53.5°) and Upasani [17] (60.5°). It seems that the low kyphosis in AIS has a trend of a low lordosis accompanied.
The correlations between the pelvic parameters (PI and SS) and LL are equivalent to the correlations in normal population. Corroborating to Yong’s study [23], the correlations are highly significant with high coefficient regression between PI and DLL in the whole cohort and in the two groups. These results could be explained by the fact that DLL is geometrically equivalent to SS, and SS is the main factor of PI (PI = SS + PT). It is confirmed by the significant regression that we observed between PI and DLL in the whole cohort and within the two groups (Fig. 3). But we did not find any correlation between PI and PLL. Therefore, we can deduct that the distal part of the lordosis is closely linked to the pelvic incidence. The proximal part of the lordosis is independent of the PI.
Regarding the relationship between TK and LL, our study showed a correlation between TK and LL with a weak coefficient. This correlation disappeared if the cohort is split into two groups by the value of TK. Authors [16, 17] did not find this correlation, or only for thoracolumbar curves [16]. However, Yong [23] described a strong correlation between TK and LL.
For the two parts of LL, we found a correlation between TK and PLL in the whole cohort, which is consistent with Yong’s results, and in the HKG. The correlation is confirmed by the significant linear regression (Fig. 2). The lack of correlation between TK and PLL in the NKG seems to demonstrate that it is the hypokyphosis which related to PLL. In any group, we did not observe any correlation between TK and DLL, neither did Yong [23]. The thoracic hypokyphosis is related with a low LL by having a low proximal lordosis. This dependence stops at the apex of the lordosis and does not affect the distal part and the pelvic parameters.
From those results, we can consider that LL is dependent on two factors. The proximal part of the lordosis depends on the thoracic hypokyphosis and the distal part depends on the pelvic incidence.
Seeing as TK is not linked with DLL and pelvic parameters, the influence of hypokyphosis stops at the apex of the lordosis. Reciprocally, as PI is not linked with PLL and TK, the pelvic incidence does not determine the kyphosis of thoracic AIS. The hypokyphosis seems to be a structural parameter, characteristic of the scoliotic deformity and independent of the pelvic parameters.
This study helps to understand the relationship between pelvic incidence, LL and TK. For a healthy person, the three parameters are linked, and the TK is under the influence of the pelvic incidence. Conversely, for adolescents with thoracic idiopathic scoliosis, the link stopped at the apex of the lordosis. The TK is independent of the pelvic incidence.
For AIS surgical treatment, it seems important to consider these relationships and the value of TK and PI. A LL adapted to the PI must be restored. With selective thoracic fusion used for thoracic scoliosis, the correction of hypokyphosis could increase the LL by the way of PLL. This could constitute a means to adapt the value of LL to the PI. Further studies are necessary to analyze the possibilities to modify the lumbar lordosis by the surgical correction of the hypokyphosis in Thoracic AIS.
Conflict of interest
None.
References
- 1.Schwab F, Lafage V, Patel A, et al. Sagittal plane considerations and the pelvis in the adult patient. Spine. 2009;34:1828–1833. doi: 10.1097/BRS.0b013e3181a13c08. [DOI] [PubMed] [Google Scholar]
- 2.Duval-Beaupère G, Schmidt C, Cosson P. Abarycentremetric study of the sagittal shape of spine and pelvis: the conditions required for an economic standing position. Ann Biomed Eng. 1992;20:451–462. doi: 10.1007/BF02368136. [DOI] [PubMed] [Google Scholar]
- 3.Legaye J, Hecquet J, Marty C, et al. Sagittal equilibration of the spine: relationship between pelvis and sagittal spinal curves in the standing position (in French) Rachis. 1993;5:215–226. [Google Scholar]
- 4.Mangione P, Sénégas J. Normal and pathologic sagittal balance of the spine and pelvis (in French) Rev Chir Orthop. 1997;83:22–32. [PubMed] [Google Scholar]
- 5.Legaye J, Duval-Beaupère G, Hecquet J, et al. Pelvic incidence: a fundamental pelvic parameter for three dimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7:99–103. doi: 10.1007/s005860050038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marty C, Boisbaubert B, Descamps H, et al. The sagittal anatomy of the sacrum among young adults, infants and spondylolisthesis patients. Eur Spine J. 2002;11:119–125. doi: 10.1007/s00586-001-0349-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rajnics P, Templier A, Skalli W, et al. The association of sagittal spinal and pelvic parameters in asymptomatic persons and patients with isthmic spondylolisthesis. J Spinal Disord. 2002;15:24–30. doi: 10.1097/00024720-200202000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Roussouly P, Berthonnaud E, Dimmet J. Geometrical and mechanical analysis of lumbar lordosis in an asymptomatic population: proposed classification (in French) Rev Chir Orthop. 2003;89:632–639. [PubMed] [Google Scholar]
- 9.Boulay C, Tardieu C, Hecquet J, et al. Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis. Eur Spine J. 2006;15:415–422. doi: 10.1007/s00586-005-0984-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gelb DE, Lenke LG, Bridwell KH, et al. An analysis of sagittal alignment in 100 asymptomatic middle and older aged volunteers. Spine. 1995;20:1351–1358. [PubMed] [Google Scholar]
- 11.Jackson RP, Peterson MD, MacMamus AC, et al. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients. Spine. 1998;23:1750–1767. doi: 10.1097/00007632-199808150-00008. [DOI] [PubMed] [Google Scholar]
- 12.Vaz G, Roussouly P, Berthonaud E, et al. Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J. 2002;11:80–87. doi: 10.1007/s005860000224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kobayashi T, Atsuta Y, Matsuno T, et al. A longitudinal study of congruent sagittal spinal alignment in an adult cohort. Spine. 2004;29:671–676. doi: 10.1097/01.BRS.0000115127.51758.A2. [DOI] [PubMed] [Google Scholar]
- 14.Öhlen G, Aaro S, Bylund P. The sagittal configuration and mobility of the spine in idiopathic scoliosis. Spine. 1988;13:413–416. doi: 10.1097/00007632-198804000-00008. [DOI] [PubMed] [Google Scholar]
- 15.Raso VJ, Russell GC, Hill DL, et al. Thoracic lordosis in idiopathic scoliosis. J Pediatr Orthop. 1991;11:599–602. [PubMed] [Google Scholar]
- 16.Mac-Thiong JM, Labelle H, Charlebois M, et al. Sagittal plans analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine. 2003;28:1404–1409. doi: 10.1097/01.BRS.0000067118.60199.D1. [DOI] [PubMed] [Google Scholar]
- 17.Upasani V, Tis J, Bastrom T, et al. Analysis of sagittal alignment in thoracic and thoracolumbar curves in adolescent idiopathic scoliosis. How do these two curve types differ. Spine. 2007;32:1355–1359. doi: 10.1097/BRS.0b013e318059321d. [DOI] [PubMed] [Google Scholar]
- 18.Lonner BS, Auerbach JD, Sponseller P, et al. Variations in pelvic and other sagittal parameters as a function of race in adolescent idiopathic scoliosis. Spine. 2010;35:E374–E377. doi: 10.1097/BRS.0b013e3181bb4f96. [DOI] [PubMed] [Google Scholar]
- 19.Hanson DS, Bridwell KH, Rhee JM, et al. Correlation of pelvic incidence with low-grade and high-grade isthmic spondylolisthesis. Spine. 2002;27:2026–2029. doi: 10.1097/00007632-200209150-00011. [DOI] [PubMed] [Google Scholar]
- 20.Mac-Thiong JM, Berthonaud E, Dinar JR, et al. Sagittal alignment of the spine and pelvis during growth. Spine. 2004;29:1642–1647. doi: 10.1097/01.BRS.0000132312.78469.7B. [DOI] [PubMed] [Google Scholar]
- 21.Mac-Thiong JM, Labelle H, Berthonnaud E, et al. Sagittalspinopelvic balance in normal children and adolescents. Eur Spine J. 2007;16:227–234. doi: 10.1007/s00586-005-0013-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mendoza-Lattes S, Ries Z, Gao Y, et al. Natural history of spinoplevic alignment differs from symptomatic deformity of the spine. Spine. 2010;35:E792–E798. doi: 10.1097/BRS.0b013e3181d35ca9. [DOI] [PubMed] [Google Scholar]
- 23.Yong Q, Zhen L, Zezhang Z, et al. Comparison of sagittal spinopelvic alignment in Chinese adolescents with and without idiopathic thoracic scoliosis. Spine. 2012;37:E714–E720. doi: 10.1097/BRS.0b013e3182444402. [DOI] [PubMed] [Google Scholar]
- 24.Roussouly P, Labelle H, Rouissi J, et al. Pre- and post-operative sagittal balance in idiopathic scoliosis: a comparison over the ages of two cohorts of 132 adolescents and 52 adults. Eur Spine J. 2013;22(suppl 2):S203–S215. doi: 10.1007/s00586-012-2571-x. [DOI] [PMC free article] [PubMed] [Google Scholar]