

Abstract
The objective of this study is to describe the complication of temporomandibular joint (TMJ) ankylosis consequent to otitis media. The method applied is prospective case series and data collection done in tertiary referral centre from April 2012 to April 2013. Case description of three adolescent male patients with unilateral TMJ ankylosis consequent to ipsilateral chronic suppurative otitis media. Further literature review of TMJ ankylosis in relation to otitis media for evaluation for predisposing conditions. Surgical treatment by ipsilateral canal wall down mastoidectomy and concurrent TMJ gap arthroplasty. Surgical exposure confirmed ipsilateral bony ankylosis in all three. Two cases with long standing trismus had developed contralateral disuse fibrous ankylosis and required bilateral gap arthroplasty. Relief of trismus achieved in all three cases. Literature review indicated three similar cases secondary to otitis media. A universal feature among all previous case reports and the current case series was the age at onset of trismus, being at 10 years or less in all. TMJ ankylosis is a rare but potential complication of paediatric ear suppuration. Dehiscence along the tympanosquamosal fissure, tympanic plate and the foraminae of Huschke and Santorini in the paediatric population may predispose to extension of tympanic suppuration to the TMJ.
Keywords: Chronic suppurative otitis media, Temporomandibular joint ankylosis, Gap arthroplasty
Introduction
Temporomandibular joint (TMJ) ankylosis consequent to ear suppuration is most unusual in current times. Contemporary standard textbooks of Otorhinolaryngology do not list TMJ ankylosis among the complications of otitis media [1]. This report describes three young males with such ankylosis secondary to ear infection. Similar cases in the reported literature are reviewed and the predispositions and mechanisms for such spread reviewed.
Description of Cases
The case group includes three consecutive patients of chronic suppurative otitis media with TMJ ankylosis treated at our tertiary referral centre from April 2012 to April 2013. Data pertaining to each patient has been recorded prospectively from the time of the first inpatient admission.
The clinical characteristics and treatment details of all three patients are summarized in Table 1. All patients were male adolescents with ages ranging from 12 to 18 years. Ear suppuration preceded trismus in every case by periods of 1–5 years. The age of onset of trismus ranged from 1 to 10 years, and the one patient with early onset trismus also had secondary effects of mandibular retrusion, dental malocclusion and facial asymmetry.
Table 1.
Summarizing all three cases
| Patient no. | 1 | 2 | 3 |
|---|---|---|---|
| Age/sex | 18/M | 12/M | 15/M |
| Duration of ear suppuration | 13 years | 3 years | 9 years |
| Duration of trismus | 10 years | 2 years | 8 years |
| Laterality | Left | Right | Right |
| ASOM/CSOM | CSOM | CSOM | CSOM |
| TMJ status | Bony ankylosis | Bony ankylosis | Bony ankylosis |
| Trismus | Present | Present | Present |
| Inter-incisor distance (pre-operative) (mm) | 0 | 4 | 3 |
| Surgical procedure | Left mastoidectomy with bilateral condyloidectomy | Right MRM with Rt. condyloidectomy | Right radical mastoidectomy with bilateral condyloidectomy and coronoidectomy |
| Inter-incisor distance (post-operative) (mm) | 17 | 32 | 15 |
Radiological evaluation indicated ipsilateral bony ankylosis of the TMJ in all three patients (Fig. 1). The pre-operative inter-incisor distance ranged from 0 to 4 mm (Table 1).
Fig. 1.
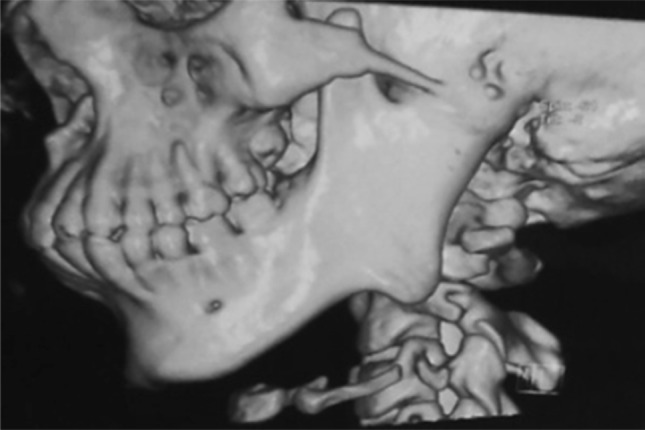
Reconstructed image showing left sided complete canal stenosis, large condylar process and severe ankylosis
All patients underwent canal wall down mastoidectomy for clearance of the ear disease, and ipsilateral TMJ exploration with condyloidectomy for ankylosis release (Table 1). Cases 1 and 3 had suffered very long term trismus for durations of 10 and 8 years respectively and also required additional contralateral TMJ condyloidectomies for the secondary disuse fibrous ankylosis of the contralateral joint.
Surgical Procedure
The patients were taken up for mastoid exploration with TMJ ankylosis release. Surgical access was via a Heerman’s C incision (combined post-aural and endaural incision—Fig. 2) for ipsilateral diseased ear and TMJ so as to expose the tympano-mastoid area, zygomatic process, glenoid fossa, and TMJ in all cases and anterior question mark incision for contralateral TMJ in two cases. An initial canal wall down mastoidectomy was done in all cases along with complete disease clearance. The canal wall down mastoidectomy was supplemented with a conchoplasty and a meatoplasty.
Fig. 2.

Schematic representation of Heerman’s incision a, b, c
The fused TMJ-zygomatic arch complex was then exposed and the periosteum over the same elevated. Two horizontal and parallel bony cuts were made through the full thickness of the ankylosed complex, and a 8–10 mm block of bone removed to create a mobile joint space (Fig. 3). An improvement in trismus resulted, but this was not complete in case 1 and 3 and it was therefore judged that the contra-lateral TMJ too had probably developed a disuse fibrous ankylosis. Exploration and condyloidectomy of the contralateral TMJ was thus undertaken in case 1 and 3. Also in case 3, bilateral coronoidectomy was performed to achieve immediate and significant mouth opening.
Fig. 3.
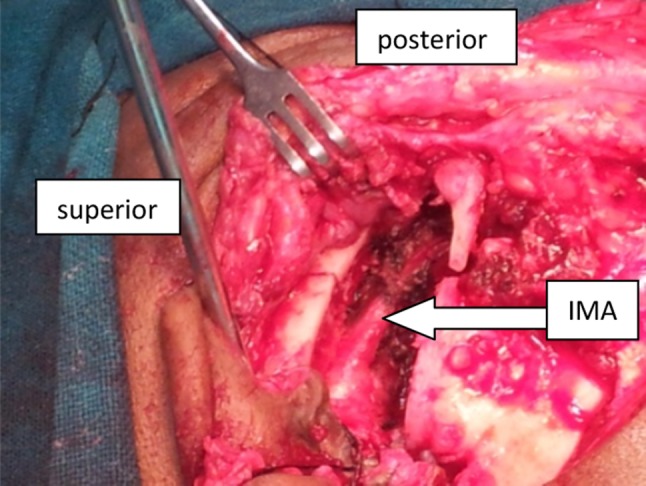
Showing left condyloidectomy and left internal maxillary artery after condyloidectomy
Appropriate physiotherapy and mouth opening exercises were initiated in the immediate post-operative period so as to maintain the correction and prevent re-ankylosis at the joints.
Post-operatively significant mouth opening was achieved in all patients. The post-operative inter-incisor distance was 1.7, 3.2 and 1.5 cm, respectively. In the follow-up period, there was no recurrence of TMJ ankylosis.
Discussion
TMJ ankylosis in current era is almost exclusively caused by trauma [2, 3]. TMJ suppuration is unusual and generally noted in association with immunosuppressive conditions [4]. Involvement of the TMJ space by effusion or abscess secondary to otitis media has been very occasionally reported [5–7], but the progression of such initial involvement to TMJ ankylosis is most unusual and outside the experience of contemporary otolaryngologists. A Pubmed and Google search for TMJ ankylosis secondary to ear suppuration yielded three such possible cases as reported in the otolaryngology and maxillofacial literature (Table 2)[2, 8, 9].
Table 2.
Summarizing previously reported case of TMJ ankylosis consequent to ear pathology
Infection of the middle and external ear space may spread to the TMJ through three potential routes (a) a dehiscent squamotympanic fissure; (b) congenital dehiscence in the cartilaginous EAC (Santorini’s fissure); and (c) patency or failure of closure of Huschke’s foramen in the bony EAC [10, 11].
The squamotympanic fissure in the temporal bone may often remain open as it extends medially into the tympanic cavity and divided into petrotympanic and petrosquamosal fissures by the presence of tegmen tympani [2]. Also the tympanic plate separating the joint space from middle ear may have incomplete or delayed ossification resulting in potential route to the spread of ear infection. Tympanic plate ossification completes approximately around 5 years of age. However incomplete ossification presenting as tiny perforation in the central part of tympanic plate has been noted consistently below 10 years of age and approximately in 20 % of adults [12]. The foramen of Huschke’s normally closes by the fifth year of life. However, Santorini’s fissures are patent till late life.
The risk of infection from the middle ear to the TMJ seems therefore to be limited to early childhood. The three reported cases in the literature, along with our series, all report of ear infection in childhood.
Inflammation of the joint space and joint surfaces leads to bone erosion and periosteal reaction and subsequent scarring with consequent bony or fibrous ankylosis. TMJ ankylosis at a young age also leads to secondary effects on mandibular growth with resultant dental malocclusion, facial asymmetry and mandibular retrusion [13, 14].
The management of TMJ ankylosis is surgical [15]. The surgical techniques for its treatment include gap arthroplasty, interpositional arthroplasty and joint reconstruction [16]. Gap arthroplasty including condyloidectomy with or without coronoidectomy, as undertaken in the our cases, is a simple and effective technique. The technique however runs the risk of recurrent ankylosis if vigorous post-operative physiotherapy is not employed.
This case series highlights a very unusual and forgotten potential complication of otitis media. These cases and the literature also indicate that such spread from the middle ear to the TMJ is probably seen exclusively in young children.
Conclusion
TMJ ankylosis is an unusual and rare complication of otitis media exclusively seen in young children due to patent or dehiscent anatomical barriers. Surgical management including gap arthroplasty is simple and effective for established TMJ ankylosis consequent to otitis media.
Acknowledgments
Conflict of Interest
None.
References
- 1.Glasscock ME, Gulya A (2005) Glasscock—Shambaugh surgery of the ear. BC Decker Inc Ontario
- 2.Faerber TH, Ennis RL, Allen GA. Temporomandibular joint ankylosis following mastoiditis: report of a case. J Oral Maxillofac Surg. 1990;48(8):866–870. doi: 10.1016/0278-2391(90)90348-6. [DOI] [PubMed] [Google Scholar]
- 3.El-Moft S. Ankylosis of the temporomandibular joint. Oral Surg Oral Med Oral Pathol. 1972;33(4):650–660. doi: 10.1016/0030-4220(72)90375-1. [DOI] [PubMed] [Google Scholar]
- 4.Dingle AF. Fistula between the external auditory canal and the temporomandibular joint: a rare complication of otitis externa. J Laryngol Otol. 1992;106:994–995. doi: 10.1017/S0022215100121565. [DOI] [PubMed] [Google Scholar]
- 5.Aarnisalo AA, Tervahartiala P, Jero J, Tornwall J. Surgical treatment of chronic otitis media with temporomandibular joint involvement. Auris Nasus Larynx. 2008;35:552–555. doi: 10.1016/j.anl.2007.10.013. [DOI] [PubMed] [Google Scholar]
- 6.Hadlock TA, Ferraro NF, Rahbar R. Acute mastoiditis with temporomandibular joint effusion. Otolaryngol Head Neck Surg. 2001;125:111–112. doi: 10.1067/mhn.2001.115664. [DOI] [PubMed] [Google Scholar]
- 7.Takes RP, Langeveld APM, De Jong RJB. Abscess formation in the temporomandibular joint as a complication of otitis media. J Laryngol Otol. 2000;114:373–375. doi: 10.1258/0022215001905607. [DOI] [PubMed] [Google Scholar]
- 8.Weteid AA, El Ekrish A, Al Mutairi K, Al Foghm S. Temporomandibular joint ankylosis caused by mastoiditis: presentation of a rare case and literature review. Saudi Dent J. 2000;12:103–105. [Google Scholar]
- 9.Kim JS, Kim MJ, Seo HK, Han SY, Chang HH. Temporomandibular joint ankylosis caused by otitis media in childhoods: report of a case. J Korean Assoc Oral Maxillofac Surg. 1998;24(1):111–117. [Google Scholar]
- 10.Wang RG, Bingham B, Hawke M, Kwok P, Li R. Persistence of the foramen of Huschke in the adult: an osteological study. J Otolaryngol. 1991;20:251–253. [PubMed] [Google Scholar]
- 11.Smith JA, Sandler NA, Ozaki WH, Braun TW. Subjective and objective assessment of the temporalis myofascial flap in previously operated temporomandibular joints. J Oral Maxillofac Surg. 1999;57:1058–1065. doi: 10.1016/S0278-2391(99)90325-7. [DOI] [PubMed] [Google Scholar]
- 12.Moffett B. The morphogenesis of the temporomandibular joint. Am J Orthod. 1986;52:401. doi: 10.1016/0002-9416(66)90120-5. [DOI] [PubMed] [Google Scholar]
- 13.Kaban LB, Perrott DH, Fisher K. A protocol for management of temporomandibular joint ankylosis. J Oral Maxillofac Surg. 1990;48:1145–1151. doi: 10.1016/0278-2391(90)90529-B. [DOI] [PubMed] [Google Scholar]
- 14.Chidzonga MM. Temporomandibular joint ankylosis: review of thirty-two cases. Br J Oral Maxillofac Surg. 1999;37:123–126. doi: 10.1054/bjom.1997.0089. [DOI] [PubMed] [Google Scholar]
- 15.Su-Gwan K. Treatment of temporomandibular joint ankylosis with temporalis muscle and fascia flap. Int J Oral Maxillofac Surg. 2001;30:189–193. doi: 10.1054/ijom.2001.0047. [DOI] [PubMed] [Google Scholar]
- 16.Zhi K, Ren W, Zhou H, Gao L, Zhao L, Hou C, Zhang Y. Management of temporomandibular joint ankylosis: 11 years’clinical experience. Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:687–692. doi: 10.1016/j.tripleo.2009.06.041. [DOI] [PubMed] [Google Scholar]