

Abstract
Study of mass in ear was undertaken with the aim that clinical diagnosis was in most but not all cases consistent with the histo-pathological diagnosis. Therefore incisional or excisional biopsy with histo-pathological study is a must in all types of small masses in ear. A study of 50 patients, attending Ear, Nose and Throat department, was done and specimen collected from them and subjected to histopathological examination. These masses were further classified as inflammatory, benign and malignant lesions and the frequency of their occurrence in saurashtra region (Jamnagar, GUJARAT), their age and sex distribution were observed. Most common lesion was found to be inflammatory Polyps (20), followed by Cholesteatomas (12) and chronic non-specific inflammations (7), Abscess (1). In malignant lesions Squamous cell carcinoma (7) was the commonest followed by Embryonal rhabdomyosarcoma (1) and in benign lesion, Carcinoid tumor (1) and Nevus (1) were diagnosed on histo-pathological examination. Right side masses were more common than left side; males were more affected than females. Adolescents/children more affected than adults for benign lesions while reverse was true for malignant lesions.
Keywords: Ear, Polyp, Cholesteatoma, Squamous cell carcinoma, Embryonal Rhabdomyosarcoma, Carcinoid tumor
Introduction
A number of diseases can involve the ear and some of these can pose special problems at this site [1]. They rarely cause mortality but quality of life is definitely affected. The ear can be divided into external, middle and inner segments [2].
Aural polyps are non-cancerous, fleshy growths in the outer ear canal or eardrum. They can also arise from middle ear. Polyps usually arise from constant irritation of the ear canal or eardrum. External ear infections, called chronic otitis externa, are the most common cause of this irritation [3, 4].
Cholesteatomas of the external ear canal are composed of a cystic mass of keratinized squamous epithelium overlying an area of bony sequestration in the inner half of canal [5]. They are the result of chronic otitis media and may involve the peri-tympanic space, mastoid cavity and petrous part of the temporal bone [6, 7].
Squamous cell carcinomas of head and neck accounts for one-fourth of total squamous cell carcinomas [8]. Most patients are elderly. They are more common in ear pinna followed by ear canal [9, 10]. They are malignant tumors arising from epidermis of skin in elderly persons [11].
Carcinoid tumors of the middle ear are an infrequent cause of a middle ear mass. Despite previous assertions of benignancy, the findings suggest that Carcinoid tumors of the middle ear are indeed a low-grade malignancy with documented metastatic potential. Almost all middle ear adenomatous tumors (“adenoma” and “carcinoid”) show evidence of neuro-endocrine differentiation [12].
Embryonal Rhabdomyosarcomas, a highly malignant tumor of striated muscles are derived from primitive mesenchymal cells. They are the most common soft-tissue malignancy in the pediatric age group [13]. Rhabdomyosarcomas of the middle ear and mastoid are the most common malignant aural neoplasm, although they account for less than 10% of all cases of head and neck Rhabdomyosarcomas [14, 15].
Nevi of any size and shape or degree of pigmentation can occur in head and neck region and they are more or less hairy. Nevi of various types can occur in the auricle or less commonly in canal [16].
Materials and Methods
Patients attending Ear, Nose and Throat, Out patient department and admitted at Guru Gobind Singh Hospital, Jamnagar, with complain of mass in ear, were selected for this study. Fifty such patients for a period of 2 years from 1st Jan 2008 to 31st Dec 2009, including patients of all ages and both sexes were included in the study. In each patient, either incision or excision biopsy was performed and submitted for histo -pathological examination. After grossing, sectioning of tissue was done and dehydration with graded alcohol was carried out in histokinete machine, after that blocks were prepared. The slides were stained by Hematoxylin and Eosin stain and examined under microscope. Special Stains were done wherever required.
Results
Lesions of Ear are widely distributed amongst all groups of people. Out of 50 patients studied, inflammatory polyp was the most common lesion found (40%) followed closely by Cholesteatoma (24%) Fig. 1.
Fig. 1.

Frequency of distribution of various lesions
While inflammatory lesions can affect any age, benign & malignant lesions were more common in older age group. Table 1.
Table 1.
Age wise distribution of No of cases
| S. no | Age-group | No of cases |
|---|---|---|
| 1 | 0–10 | 11 |
| 2 | 11–20 | 10 |
| 3 | 21–30 | 07 |
| 4 | 31–40 | 06 |
| 5 | 41–50 | 04 |
| 6 | 51–60 | 04 |
| 7 | >60 | 08 |
| Total | 50 |
Males were affected more than females for overall lesions. Males 33: Females 17 (a ratio of approximately 2:1) Table 2.
Table 2.
Sex-wise distribution of all lesions
| S. no | Name of lesion | No of males affected | No of females affected |
|---|---|---|---|
| 1 | Inflammatory polyp | 13 | 07 |
| 2 | Cholesteatoma | 06 | 06 |
| 3 | Nonspecific Inflammations | 07 | 00 |
| 4 | Squamous cell carcinoma | 06 | 01 |
| 5 | Carcinoid tumor | 00 | 01 |
| 6 | Embryonal Rhabdomyosarcoma | 01 | 00 |
| 7 | Nevus | 00 | 01 |
| 8 | Abscess | 00 | 01 |
| Total | 33 | 17 |
Most but not in all cases Clinical presentation correlated with H. P. study. Table 3.
Table 3.
Clinical presentation with H. P. correlation
| S. no. | Name of lesion | Presentation | Histo-pathology |
|---|---|---|---|
| 1 | Polyp | As mass in external ear canal/polypoidal mass with pain and discharge | Inflammatory polyp |
| 2 | Cholesteatoma | As cystic mass in ear with discharge(white cheesy material from external ear canal) | Cholesteatoma |
| 3 | Nonspecific inflammations | As discharge and pain | Chronic non–specific inflammations |
| 4 | Squamous cell carcinoma | As growth in external ear canal (? Polyp)/on pinna, Sometimes chronic otitis media | Invading squamous cell carcinoma |
| 5 | Carcinoid tumor | As mass in external ear canal/? polyp | Carcinoid tumor |
| 6 | Embryonal rhabdomyosarcoma | Mass in external ear canal which bleeds on touch | Embryonal Rhabdomyosarcoma |
| 7 | Nevus | Swelling on pinna | Junctional nevus |
| 8 | Abscess | Pain and discharge | Acute abscess |
Inflammatory lesions (80%) were the commonest affecting all age group, followed by malignant lesions (16%) affecting older age and least common was benign tumor of ear (4%) Table 4.
Table 4.
Age-wise distribution of inflammatory, benign and malignant lesions
| Age-group | Inflammatory | Benign | Malignant | Total |
|---|---|---|---|---|
| 0–10 | Abscess-1 | Embryonal rhabdomyosarcoma -1 | 11 | |
| Polyp - 3 | ||||
| Cholesteatoma-3 | ||||
| Nonspecific inflammations-3 | ||||
| 11–20 | Polyp-6 Cholesteatoma-4 | 10 | ||
| 21–30 | Polyp-5 | 07 | ||
| Cholesteatoma-1 | ||||
| Nonspecific inflammations-1 | ||||
| 31–40 | Polyp-2 | 06 | ||
| Cholesteatoma-4 | ||||
| 41–50 | Polyp-1 | Squamous cell carcinoma-1 | 04 | |
| Nonspecific inflammations-2 | ||||
| 51–60 | Polyp-1 | Nevus -1 | 04 | |
| Nonspecific inflammations-1 | Carcinoid-1 | |||
| >60 | Polyp-2 | Squamous cell carcinoma -6 | 08 | |
| Total | 40 (80%) | 02 (4%) | 08 (16%) | 50 (100%) |
Discussion
Most lesions of ear presented either as middle ear mass protruding into external ear canal or mass on auricle (ear pinna). Symptoms included mass with sero-sanguineous or blood stained discharge with pain in the ear and sensitive to touch.
Polyps presented as mass protruding into external auditory canal with history of pain and discharge. Polyps are significant for two reasons. First, they say something about the severity and duration of middle ear inflammation. Secondly, in addition to the perforated eardrum they can cause hearing loss, dizziness, ear pain and chronic drainage from the ear [4]. Grossly, they are soft to firm in consistency with microscopic appearance of polypoidal accumulation of granulation tissue. They are composed of loose edematous well vascularized stroma diffusely infiltrated with inflammatory cells specially lymphocytes and plasma cells. They may be covered by squamous or modified respiratory epithelium [16] (Fig. 2).
Fig. 2.
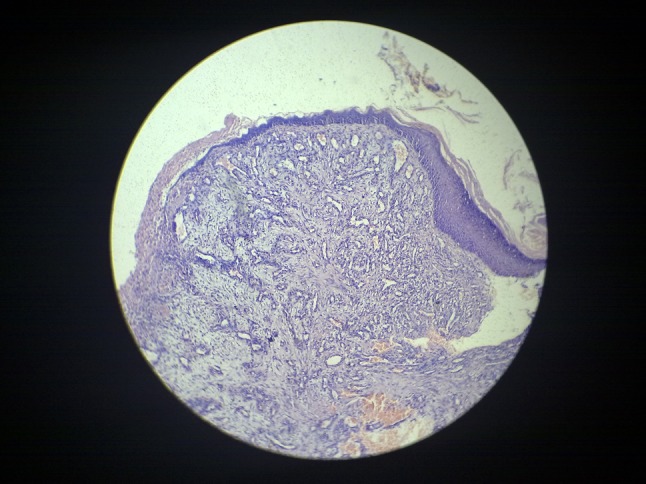
Polyp; 10×, H and E stain
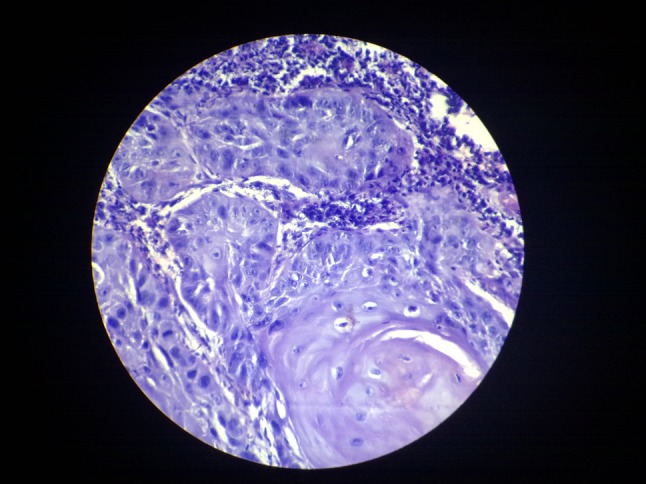
Cholesteatomas are lesions formed from keratinizing stratified squamous epithelium. In the middle ear they usually present in third or fourth decade. They may present intradurally or extradurally. Extradural lesions most commonly involve the middle ear cleft; involvement of the mastoid or external auditory canal is less common. CT scan can help in the diagnosis of Cholesteatomas. Unfortunately, it can be difficult at times to differentiate small Cholesteatomas from chronic middle ear inflammation on CT Scan alone. Hence excision biopsy with histo-pathological study becomes necessary for confirmation of diagnosis. The term Cholesteatoma is actually a misnomer as these masses rarely contain cholesterol. Although they are not true neoplasm, but clinically they can mimic malignant neoplasm because of their propensity to destroy surrounding tissue and recur after excision [16]. Cholesteatomas can be congenital (primary) or acquired. Acquired Cholesteatomas are much more common, and they typically occur in older children and young adults. Presentation of Cholesteatomas are not much different from that of polyp, except that they grossly present as cystic mass. Microscopically they consist of stratified squamous epithelium, keratin and sub-epithelial fibrous and/or granulation tissue (Fig. 3).
Fig. 3.
Cholesteotoma; 45×, H and E stain
Squamous cell carcinomas of the ear pinna are primarily the disease of older males who are exposed to sunlight for prolonged period. Squamous cell carcinomas of external ear canal are less common then that of ear pinna and can present in females between 5th and 6th decade of life. While in case of external ear canal, patient presented with long history of chronic otitis media followed by bloody discharge and hearing loss [16]. Squamous cell carcinomas tend to grow relentlessly & erode thin bony plate surrounding middle ear or reaching cranial cavity [17]. Most Squamous cell carcinomas of pinna are well differentiated and present as ulcer, crusty scale or a sessile nodule. Histo-pathological features of Squamous cell carcinoma remain important for the clinician, as they carry prognostic value and help to define the most appropriate treatment for patients. Invasive Squamous cell carcinomas are differentiated from carcinoma-in situ by the invasion of the basement membrane by malignant appearing cells in the form of nests within the dermis surrounded by an inflammatory infiltrate (Fig. 4).
Fig. 4.
Squamous Cell Carcinoma; 45×, H and E stain
Nevi occur frequently in pinna and rarely in external auditory canal. They are a synonym for mole to designate a localized abnormality of the melanocytic system. They present with brownish small swelling on pinna or external auditory canal. Histo-pathological confirmation is a must since Malignant melanoma are more common entity in ear and benignancy of nevi should be established for treatment of patient. Junctional nevi are defined as nevi restricted to basal layer of epidermis. Histo-pathologically they consist of nests of benign looking nevi cells in the junctional region. These nevi cells are small, round to oval with darkly stained nucleus and scanty amphophilic cytoplasm.
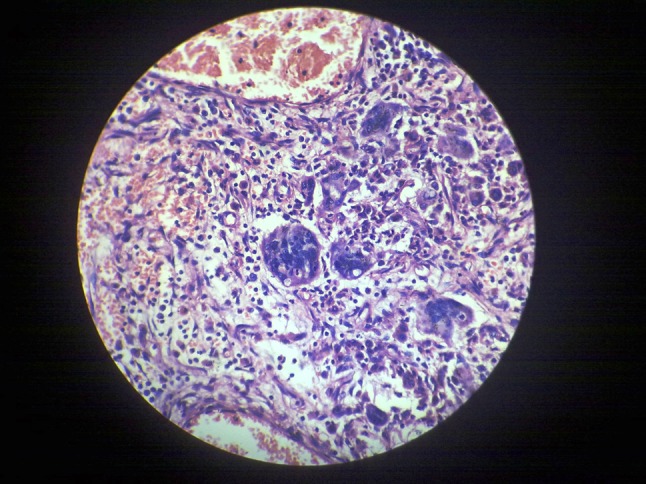
Carcinoid tumors of the middle ear although uncommon are a distinct entity from middle ear adenoma. They are considered as a variant of middle ear adenoma because clinical behaviors of both lesions are identical. They occur equally in both sexes. They present with progressive hearing loss, tinnitus and fullness of ear for the duration of months to years and white to yellow mass protruding through external ear canal [16, 18]. Histo-pathologically Carcinoid tumor shows hyperplastic squamous epithelial lining underneath which tumor cells are seen in an organoid and trabecular pattern. Cells are having vesicular nuclei with salt pepper appearance and eosinophilic to clear cytoplasm. In certain literature, it has been mentioned that histo-pathologically Carcinoid tumor and middle ear adenoma can not be differentiated many a times [2]. Although on scanner view Carcinoid tumor looks like Paraganglioma, but on high power view, features of Carcinoid tumor are very well appreciated (Fig. 5).
Fig. 5.
Carcinoid Tumor; 45×, H and E stain
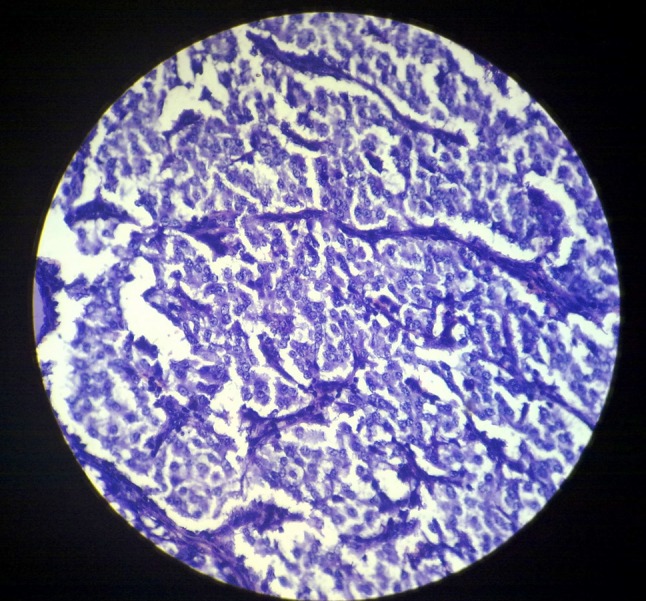
Embryonal Rhabdomyosarcomas of the middle ear/mastoid occurs invariably in 1st decade of life [2]. Typically these patients present with post auricular non tender swelling with mass in external auditory canal which bleeds on touch. Symptoms include unilateral refractory otitis media with sero-sanguineous discharge and otalgia [15]. Exact site is difficult to determine [18]. On presentation CT scan showed heterogeneously enhancing mass lesion involving right mastoid with extension to temporal lobe, middle ear cavity and temporal bone. Microscopically the surface epithelium is usually intact and separated from the neoplastic proliferation. It is made up of round to spindled cells. The appearance of the round cells is similar to that of lymphocytes, with hyperchromatic, irregular nuclei surrounded by scant, elongated eosinophilic cytoplasm. These cells imperceptibly blend with spindled cells, which are characterized by a spindled morphology, eosinophilic cytoplasm, and an elongated central hyperchromatic nucleus. These cells are surrounded by a loose myxoid stroma [19, 20]. These cellular areas are surrounding many small and large vascular spaces. Occasional rhabdomyoblasts are seen (Fig. 6).
Fig. 6.
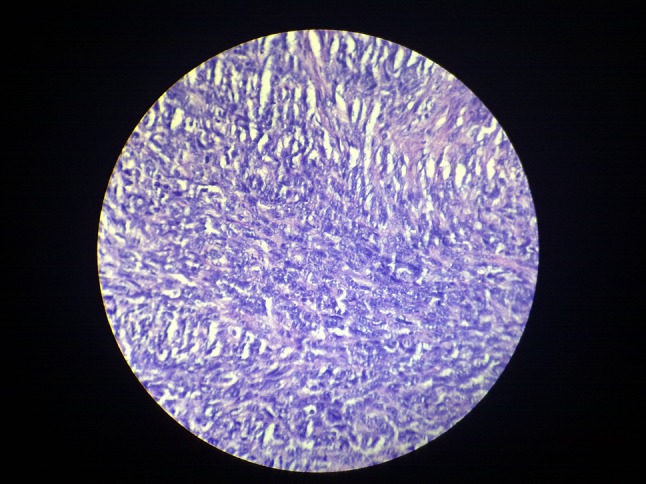
Embryonal rhabdomyosarcoma 45×, H and E stain
Statistical Analysis
In all the above cases, the observed difference is statistically significant as P value comes significant. (P < 0.05).
Conclusion
Following conclusions are drawn from this study;
Ear mass can occur in any age or sex. Inflammatory lesions are more common in children and adolescent. Benign tumor affects middle age people while malignant tumor affects older age group. Males are affected more than females for overall lesions.
Inflammatory, benign and malignant lesions affect external auditory canal and ear pinna. Inflammatory and benign lesions are more common than malignant lesions. In inflammatory lesions, Polyps are the most common lesions, closely followed by Cholesteotomas.
Benign lesions comprise only 4% of cases. Malignant lesions comprise 16% cases. Squamous cell carcinomas are the most common malignant lesions (14%).
Many times clinicians may have false impression for diagnosis of Polyp but that can be corrected by histo-pathology only because one case each of Squamous cell carcinoma, Embryonal Rhabdomyosarcoma and Carcinoid tumor presented as polyp in external auditory canal which on histo -pathological examination turned out to be malignant and benign tumor respectively.
References
- 1.Kumar, Abbas and Fausto, (2004) Robbins and Cotran’s pathological basis of disease, 7th (ed): 787–788
- 2.Rosai J. Rosai and Ackerman’s surgical pathology. 8. St. Louis: Mosby-Year Book; 1996. pp. 2509–2516. [Google Scholar]
- 3.Loury M (2002) Healthopedia.com, medical encyclopedia, disease and conditions, Aural Polyps. http://www.healthopedia.com/aural-polyps/
- 4.Hoffman, D (2009) Ear, your total health
- 5.Piepergerdes JC, Kramer BM, Behnke EE. Keratosis obturans and external auditory canal cholesteatoma. Laryngoscope. 1980;90:383–391. doi: 10.1002/lary.5540900303. [DOI] [PubMed] [Google Scholar]
- 6.Kreutzer EW, De Blanc GB. Extra aural spread of cholesteatoma. Arch Otolaryngol. 1982;108(5):320–322. doi: 10.1001/archotol.1982.00790530056014. [DOI] [PubMed] [Google Scholar]
- 7.Caponetti G, Thompson LD, Pantanowitz L. Cholesteatoma. Ear Nose Throat J. 2009;88(11):1196–1198. [PubMed] [Google Scholar]
- 8.Avila J, Bosch A, Aristizibal S, Frias Z, Marcial V. Carcinoma of pinna. Cancer. 1977;40:2891–2895. doi: 10.1002/1097-0142(197712)40:6<2891::AID-CNCR2820400619>3.0.CO;2-H. [DOI] [PubMed] [Google Scholar]
- 9.Lewis JS. Squamous carcinoma of ear. Arch Otolaryngol. 1973;97(1):41–42. doi: 10.1001/archotol.1973.00780010045011. [DOI] [PubMed] [Google Scholar]
- 10.Shiffman NJ. Squamous cell carcinoma of the skin of pinna. Can J Surg. 1975;18:279–283. [PubMed] [Google Scholar]
- 11.Metcalf PB., Jr Carcinoma of pinna. N Engl J Med. 1954;251:91–95. doi: 10.1056/NEJM195407152510303. [DOI] [PubMed] [Google Scholar]
- 12.Ramsey MJ, Nadol JB, Jr, Pilch BZ, McKenna MJ. Carcinoid tumor of the middle ear: clinical features, recurrences, and metastases. Laryngoscope. 2005;115(9):1660–1666. doi: 10.1097/01.mlg.0000175069.13685.37. [DOI] [PubMed] [Google Scholar]
- 13.Sautter NB, Thompson LDR. ENT pathology clinic: embryonal rhabdomyosarcoma of the ear USA. Ear Nose Throat J. 2004;83(5):316–317. [PubMed] [Google Scholar]
- 14.Sisodia SM, Bobhate SK, Kedar GP, Kherdekar MS. Case reports, rhabdomyosarcoma of the middle ear. Indian J Paediatr. 1986;53(1):119–121. doi: 10.1007/BF02787083. [DOI] [PubMed] [Google Scholar]
- 15.Durve DV, Kanegaonkar RG, Albert D, Levitt G. Paediatric Rhabdomyosarcoma of the ear and temporal bone. Clin Otolaryngol Allied Sci. 2004;29(1):32–37. doi: 10.1111/j.1365-2273.2004.00764.x. [DOI] [PubMed] [Google Scholar]
- 16.Silverberg SG, DeLellis RA, Frable WJ, Virginia AL, Wick MR. Silverberg’s principles and practice of surgical pathology and cytopathology, vol 2. 4. New York: Churchill Livingstone; 2006. pp. 2267–2284. [Google Scholar]
- 17.Mcgee JOD, Isaacson PG, Wright NA. Oxford’s textbook of pathology, vol 2. Oxford: Oxford University Press; 1992. pp. 1105–1111. [Google Scholar]
- 18.Fletcher CD. Diagnostic histopathology of tumors. 1. Edinburgh: Churchil Livingstone; 1995. pp. 1289–1302. [Google Scholar]
- 19.Michales L, Domjanov I, Lindel J. Anderson’s pathology, vol 2. 10. St. Louis: Mosby Yearbook, Inc; 1996. pp. 2876–2900. [Google Scholar]
- 20.Weiss SW, Goldblum JR. Enzinger and Weiss’s soft tissue tumors. 4. St. Louis: Mosby; 2001. pp. 785–836. [Google Scholar]