

Abstract
Vaccination is one of the most effective and cost-benefit interventions that prevent the mortality and reduce morbidity from infectious pathogens. However, the licensed influenza vaccine induces strain-specific immunity and must be updated annually based on predicted strains that will circulate in the upcoming season. Influenza virus still causes significant health problems worldwide due to the low vaccine efficacy from unexpected outbreaks of next epidemic strains or the emergence of pandemic viruses. Current influenza vaccines are based on immunity to the hemagglutinin antigen that is highly variable among different influenza viruses circulating in humans and animals. Several scientific advances have been endeavored to develop universal vaccines that will induce broad protection. Universal vaccines have been focused on regions of viral proteins that are highly conserved across different virus subtypes. The strategies of universal vaccines include the matrix 2 protein, the hemagglutinin HA2 stalk domain, and T cell-based multivalent antigens. Supplemented and/or adjuvanted vaccination in combination with universal target antigenic vaccines would have much promise. This review summarizes encouraging scientific advances in the field with a focus on novel vaccine designs.
Keywords: Universal vaccines, M2 protein, Stalk domain, T cell immunity, Supplemented vaccination
Introduction
Vaccination is a deliberate attempt to protect humans against disease. The modern history of vaccination began in 1796, when Edward Jenner used a cowpox virus preparation from a milkmaid for prevention of smallpox. Since the time of Edward Jenner, vaccination has controlled the 12 major diseases, at least in some parts of the world: smallpox, diphtheria, tetanus, yellow fever, pertussis, Haemophilus influenzae type b disease, poliomyelitis, measles, mumps, rubella, typhoid and rabies. The global campaign for smallpox vaccination was very successful so that this disease has disappeared from natural occurring of smallpox in the world. Cases of poliomyelitis have been reduced by 99% thanks to vaccination in most parts of the world. Vaccinations against many other diseases including influenza have made major headway. However, much remains to be done.
Isolation of the first human influenza A virus in 1933 contributed to the identification of the cause of previous epidemics and pandemics of respiratory disease, as well as the development of influenza vaccines [1,2]. Influenza virus infections can occur in wild animals and livestock as well as in all age groups of human populations. The resulting illness substantially contributes to work and school time losses, increases in influenza-related hospitalizations, and deaths [3-5].
Influenza virus contains eight segmented negative sense RNA genomes within the lipid-bilayer envelope, which belongs to the family Orthomyxoviridae. There are three distinct types of influenza virus, designated A, B, and C, with types A and B of influenza viruses being the major pathogens in humans. Influenza A viruses occur in birds, humans, horses and other species, whereas types B and C are primarily found in man. The envelope surface of the influenza virus has viral proteins. The hemagglutinin (HA) surface protein is responsible for attachment of the virus to sialic acid-containing receptors and viral entry by membrane fusion. The neuraminidase (NA) surface protein is a receptor-destroying enzyme which plays important roles in viral release and cell-to-cell spread [6,7]. Influenza A viruses can be further divided into different subtypes of HA and NA. There are 17 HA subtypes of influenza virus whereas 9 subtypes of NA are known to be present [8].
Licensed Influenza Vaccines
Conventional inactivated influenza vaccines
The first vaccines using whole-inactivated influenza virus were approved for use in the United States in 1945 [9,10]. Inactivated influenza A and B virus vaccines have been extensively used in humans. The vaccines consist of purified virus that has been chemically inactivated with formalin or β-propiolactone. Influenza B viruses, the H1 and H3 subtypes of influenza A viruses can cause epidemic infections in the human population. Therefore, current vaccines against influenza epidemics contain two influenza A subtypes (H1N1 and H3N2) and one or two variants of influenza B virus. The composition of the trivalent vaccine contain two influenza A subtypes (H1N1 and H3N2) and one variant of influenza B virus, which is based on the strains of virus that are expected to circulate in the human population during the winter flu season. The influenza A subtypes of vaccine strains are adapted to grow in embryonated eggs, or may be reassortant viruses containing HA and NA of strains needed for vaccination and other remaining genes (polymerase basic protein [PB] 1, PB2, polymerase acidic protein [PA], nucleoprotein [NP], M1-M2, NS) which encode the internal proteins from A/Puerto Rico/8/34 (PR8) (H1N1) virus which confer high growth capacity in eggs [11].
Since the dissolution of the lipid envelope still retain the major antigen HA protein and its immunogenicity with reduction in reactogenicity, detergent mediated disrupting (splitting) influenza viruses to produce subvirion preparations has been most commonly used in recent vaccines. Although whole-virus vaccines are still in use in some countries and are highly effective, most vaccines manufactured since the 1970s have been 'split' preparations [12-15].
Live attenuated influenza virus (LAIV) vaccines
Another platform of influenza vaccines was developed to overcome the variable efficacy of the inactivated vaccine, its short duration of protective immunity, and low capacity to induce local or cellular immunity. LAIV vaccines administered via nasal spray (FluMist) have been successfully developed. These LAIV strains have the properties with cold-adapted (ca) (i.e., they replicate efficiently at 25℃, a temperature that is restrictive for replication of most wild-type viruses); temperature-sensitive (ts) (i.e., they are restricted in replication at 37℃ or 39℃); and are attenuated (att) to prevent illness. LAIV is a reassortant of internal proteins of a master donor virus and surface proteins (HA, NA) of a wild-type influenza virus. The strains of A/Ann Arbor/6/60 and B/Ann Arbor/1/66 were developed as master donor viruses which acquired the ca, ts, and att phenotypes as a result of multiple mutations in the gene segments that encode internal viral proteins [16].
The efficacy of LAIV is relatively high in children compared to the inactivated vaccines [17,18]. Intranasal delivery of LAIV is likely to induce both serum IgG and mucosal IgA antibodies [19]. Unlike inactivated vaccines, LAIV evokes mucosal and systemic humoral and cellular immunity against native HA and NA glycoproteins similar to those by natural influenza infection. LAIV is considered to be safe and well tolerated in children aged over 2 year and adults, but some concerns have been raised regarding its safety in younger children and subjects with previous asthma or recurrent wheezing [20,21]. However, LAIV is less effective in adults, and thus it is not approved for use in persons over the age of 50, and inactivated split vaccines are recommended for adult populations [18,22].
Currently, five seasonal LAIV backbone strains reached regulatory approval status: A/Len/134/17/57, A/Len/134/47/57, B/USSR/60/69, A/Ann Arbor/6/60, and B/Ann Arbor/1/66. With the exception of the A/Len/134/47/57 strain, all are presently used as master donor strains in the production of seasonal LAIV vaccines. LAIV is licensed under the trade name FluMist in the United States and Canada, and Fluenz in Europe. Early animal experimental data suggest that a new class of 'replication-deficient vaccine' could be developed in the more distant future, with the plausibility of combining the contrasting theoretical advantages of both LAIV and the inactivated vaccines [23].
Quadrivalent influenza vaccines
Circulating influenza viruses are either Yamagata-like or Victoria-like strain. Unfortunately, approximately 2% of the type B influenza viruses matched the vaccine strain (called the "Victoria" strain) during the 2007-2008 influenza season in the United States. The following season, 2008-2009, only 17% of type B influenza detected by surveillance matched the vaccine strain which was the "Yamagata" strain. Type B viruses of a strain different than the vaccine can circulate, causing disease due to a mismatch on the type B strain. Vaccine manufacturers have been working on a "quadrivalent" vaccine that contains four strains of influenza to address this type B mismatching, which contains two subtype A strains (H1N1, H3N2) and two type B strains (Victoria, Yamagata). The first quadrivalent LAIV vaccine was MedImmune's nasal spray vaccine, FluMist quadrivalent and licensed by Food and Drug Administration (FDA). Sanofi Pasteur also announced the results of its Phase II and Phase III clinical trials of their injectable quadrivalent influenza vaccine. New quadrivalent vaccines in addition to the trivalent influenza vaccines are on the market.
Experimental Universal Vaccines
Influenza viruses are continuously evolving, introducing various mutations in particular to the surface major glycoprotein HA. Most commonly, these changes result from point mutations in the viral genome RNA encoding HA, and are responsible for emergence of new strains responsible for seasonal epidemics. Influenza A viruses sometimes emerge with novel surface proteins that are completely unrelated to pre-existing human strains, as a result of introduction of new HA and/or NA genes from other species. These "major antigenic shifts" result in novel antigenic subtypes of the HA and/or NA glycoproteins that had not previously infected most of the human population, and therefore can spread rapidly causing global disease pandemics. Three global pandemics of influenza occurred during the 20th century, which were caused by H1N1 subtype viruses in 1918, H2N2 viruses in 1957, and H3N2 viruses in 1968. In addition to the human influenza subtypes, avian origin influenza viruses including H5N1, H7N2, H7N3, H7N7 and H9N2 subtypes were reported to overcome the species barrier and to infect humans [24-29]. There was a recent outbreak and report on significant mortality as a result of H7N9 avian influenza virus transmission to humans [30]. The continuous emergence of highly pathogenic avian influenza H5N1 viruses in domestic poultry and the repeated cases of direct transmission of avian viruses to humans underscore a persistent threat to public health [31-35]. The 2009 outbreak of a new swine-origin H1N1 pandemic virus represents a good example of how fast a new pandemic virus can spread in the human population once it acquires the ability to transmit among humans [36,37]. The presently used vaccination programs showed a significant delay in controlling the spread of new pandemics. Indeed, the recent experience with the 2009 H1N1 virus demonstrates the high priority to develop novel vaccines to overcome the limited efficacy of current strain-specific vaccines based on HA as well as improved methods of immunization.
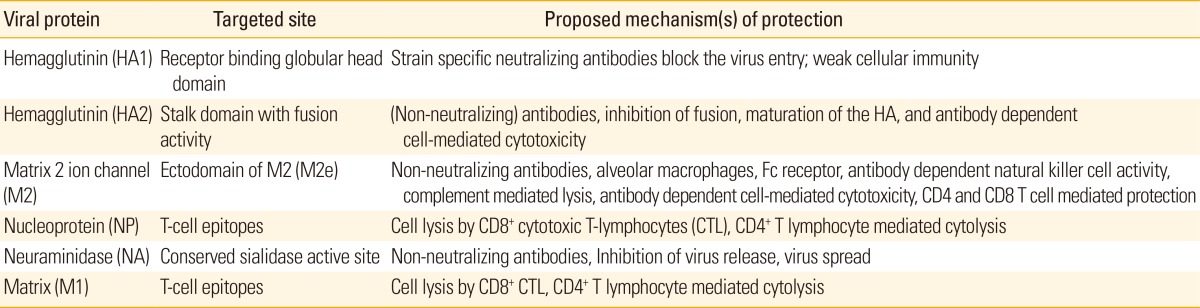
A truly universal vaccine should be able to protect against all subtypes of influenza A viruses and both lineages of influenza B viruses. However, it would be extremely difficult to develop such a universal vaccine that protects against both types of influenza A and B viruses. Due to more variants of influenza A types in both humans and animals, developing universal vaccines have been focused on influenza A viruses. It would be highly promising to develop a vaccine that is broadly cross-protective compared to currently licensed influenza vaccines. The concept behind developing universal vaccines is to utilize the highly conserved antigenic target and to make it immunogenic sufficient enough for inducing protective immunity (Table 1). The M2 ion channel protein and the stalk domain (HA2) of HA of influenza A virus have been extensively investigated as a promising antigenic target for developing a universal vaccine.
Table 1.
Viral antigenic targets of influenza vaccines
Universal vaccines based on influenza virus M2
Influenza virus M2
M2 is a pH-dependent proton-selective ion channel protein and plays a role during virus entry [38-40]. M2 is a specific target of anti-influenza drugs such as amantadine and rimantadine [41,42]. The amino acid sequence in the extracellular domain of M2 (M2e) is highly conserved among human influenza A viruses. For example, the N (amino)-terminal epitope SLLTEVET (residues 2-9) in M2e was found to be conserved at a rate of 100% among human influenza A virus isolates and approximately over 99% among all influenza A subtypes [43,44].
M2e conjugate vaccines
The extracellular 23-amino acid residue of the M2 protein (M2e) is a poor immunogen in its own. Even mice infected with influenza virus do not induce high levels of antibodies recognizing M2 (data not shown). Nonetheless, M2e specific monoclonal antibodies were shown to reduce the plaque size or the growth of some influenza A virus strains in vitro [45-47]. Passive transfer of M2 monoclonal antibodies was shown to protect mice by lowering lung virus titers upon subsequent infection with influenza A virus [48,49]. Therefore, induction of adaptive anti-M2 immunity would be a cost effective and practical strategy for controlling influenza epidemics or pandemics.
Because of low immunogenic property of M2, different approaches to link M2e peptide to carriers and/or use of potent adjuvants were explored. The first study on protection was reported with a full-length M2 vaccine expressed in insect cells after immunization of mice in the presence of incomplete Freund's adjuvant [50]. This recombinant M2 vaccine providedsurvival protection [50]. Since then, many studies have reported recombinant M2e fusion constructs using a variety of carrier molecules or systems: hepatitis B virus core (HBVc) particles [51-53], human papillomavirus L protein virus-like particles (VLPs)[54], phage Qβ-derived VLPs [55], keyhole limpet hemocyanin [56], bacterial outer membrane complex [52,57], liposomes [58], and flagellin [59]. Using various adjuvants inappropriate for human use, recombinant M2e-carrier vaccines were demonstrated to provide protection against lethal challenge with H1N1, H3N2, and H5N1 influenza A viruses. In particular, different forms of M2e vaccines fused to the HBVc VLPs were shown to induce high levels of anit-M2e antibody responses [43,51,60-62]. However, M2e-mediated protection by conjugate vaccines was relatively much weaker than HA-mediated protection [63]. Also, M2e antibodies induced by conjugate vaccines were not effective in binding to the virus [63]. Probably, chemical or genetic fusion of M2e would not be effective in inducing antibodies recognizing M2 in a native conformation on virus [63].
A novel approach was pursued in an attempt to facilitate the formation of tetrameric structure of M2e. Genetically linking M2e to the tetramer-forming leucine zipper domain of the yeast transcription factor general control nondepressible-4 (GCN4) was demonstrated to form recombinant tetrameric M2e vaccines [64]. The recombinant M2e-GCN4 conjugate vaccine induced M2e-specific antibody responses conferring 100% survival protection to vaccinated mice [64].
M2e VLP vaccines
Enveloped VLPs expressing HA and/or NA were demonstrated to be immunogenic and induce protective immunity [65-68]. Therefore, we explored an alternative approach to express M2 proteins in a membrane-anchored form mimicking the native conformation of M2. A full-length M2 was presented on influenza M1-derived VLPs containing M2 alone (M2 VLPs) without HA and NA to avoid the shielding effect by large size glycoproteins [69]. Mice vaccinated with M2 VLP vaccines induced higher levels of M2e specific antibodies than those by whole inactivated influenza virus vaccination [70]. In addition, M2e specific antibodies induced by M2 VLP vaccination via the intranasal route were cross reactive to and protective against diverse subtypes H1N1, H3N2, and H5N1 influenza viruses [69,70]. However, the wild type M2 protein was incorporated into VLPs at low levels similar to those in influenza viruses [69]. The levels of M2 specific antibodies were relatively very low and substantial weight loss was observed in M2 VLP alone immunized mice after lethal challenge [69].
There is another caveat in developing truly universal vaccines based on M2e. There are few amino acid variations depending on the host species (human, avian, swine, equine, and other hosts) where influenza viruses were isolated [43,44]. The five amino acids within the residues 10-20 of M2e (underlined residues) were observed to be host restricted: PIRNEWGCRCN (aa 10-20, human isolates), PTRNGWECKCS (aa 10-20, avian isolates), LTRNGWGCRCS (aa 10-20, avian origin human isolates), and PIRNGWECRCN (aa 10-20, swine isolates) [44,71]. Therefore, to improve the protective efficacy of M2e vaccines, we genetically engineered a tandem repeat of M2e epitope sequences (M2e5x) of human, swine, and avian origin influenza A viruses, which was expressed in a membrane-anchored form and incorporated in VLPs [71]. In addition, the chimeric M2e5x construct with the transmembrane domain being replaced by that of HA was found to incorporate heterologous M2e epitopes into VLPs at a several hundred-fold higher level than that on influenza virions or the wild type M2 VLPs [71,72]. Intramuscular immunization with M2e5x VLP vaccines was highly effective in inducing M2e specific antibodies reactive to different influenza viruses, mucosal and systemic immune responses, and cross-protection regardless of influenza virus subtypes in the absence of adjuvant. Importantly, immune sera were found to be sufficient for conferring protection in naïve mice, which was long-lived and cross protective. Anti-M2e antibodies induced by heterologous M2e5x VLP immunization conferred a wider range of cross reactivity to influenza virus at higher levels than those by live virus infection, homologous M2e VLPs, or M2e monoclonal antibody 14C2 [72]. As a protective mechanism via M2e-mediated immunity, Fc receptors were found to be important for mediating protection by immune sera from M2e5x VLP vaccination [72]. Thus, molecular designing and presenting M2e immunogens on the surfaces of VLPs provide a promising platform for developing universal influenza vaccines without using adjuvants, which can be more effective in inducing protective M2e immunity than natural virus infection and further supports an approach for developing an effective universal influenza vaccine.
M2e antibodies have virus non-neutralizing property. M2e based immunity alone is infection-permissive and is difficult to eliminate disease symptoms so far even in animal models. A desirable universal influenza vaccine should be able to diminish both morbidity and mortality. A novel approach is to use such vaccines of conserved antigenic targets as adjunct to current vaccine formulations with a variable antigenic target HA. In this regard, use of M2e-based VLP vaccines as a supplement could significantly improve the efficacy of cross protection by HA-based current vaccines. Wild type M2 presented on VLPs in a membrane-anchored form was found to significantly improve cross protection when used in combination with inactivated whole viral vaccine in mice [70]. Mice that were intranasally immunized with a mixture of an inactivated virus and wild type M2 VLP were protected against a low dose of challenge virus from both mortality and morbidity. In addition, M2 VLP-supplemented inactivated influenza virus vaccine (A/PR/8/34, H1N1) conferred broad cross protection to the immunized mice against lethal challenge with 2009 H1N1 pandemic virus, heterosubtypic H3N2, or H5N1 influenza viruses [70]. The concept of M2 VLP supplementation to improve cross protection was extended to the seasonal influenza split vaccines as well as to the more commonly used route of intramuscular immunization (unpublished data). Intramuscular immunization with H1N1 split vaccine (A/California/07/2009) supplemented with heterologous tandem repeat M2e5x VLPs induced M2e specific humoral and cellular immune responses contributing to improved cross protection of licensed split vaccines. More importantly, supplementation of M2e5x VLPs was able to shape the host responses to the split vaccine in the direction of T helper type 1 responses inducing dominant IgG2a isotype antibodies as well as interferon gamma (IFN-γ) producing cells in systemic and mucosal sites (unpublished data). These recent new approaches support evidence that supplementation of split vaccines with M2e5x VLPs is a promising new vaccination for overcoming the limitation of strain-specific protection by currently marketed influenza split vaccines.Ultimately, clinical trials should be carried out to validate this supplementation method as a potential universal vaccine for human use.
Influenza M2-mediated immunity
The protective immune mechanisms of the immune responses induced by M2 vaccination remain to be fully elucidated and further studies are needed for a better understanding (Table 1). Antibody-dependent, natural killer cell mediated cytotoxicity was found to be important for conferring protection by vaccination with M2e-hepatitis B core vaccine [63]. Another M2e-carrier vaccine using Mycobacterium tuberculosis heat shock protein 70 (M2e-HSP70359-610) was shown to provide protection via alveolar macrophages and Fc receptor-dependent elimination of influenza A virus-infected cells [73]. We demonstrated that dendritic and macrophage cells were needed for protection by immune sera of M2 VLP vaccination in a mouse model since depletion of these cells using clodronate-liposomes abrogated the protection [69,70]. Other studies suggest that M2 antibodies can restrict the growth of influenza viruses as shown by inhibiting the plaque size or replication of in vitro cultured viruses [45,74,75]. Our recent studies also found that Fc receptors played an important role in conferring protection by M2e immunity of M2e5x VLP immunization [72]. Multiple mechanisms are likely to be involved in conferring protection against influenza after immunization with M2 based vaccines.
Clinical trials of influenza M2 vaccines
The efficacy of some early recombinant M2e vaccines has been tested in human clinical trials. Sanofi Pasteur Biologics Co., formerly Acambis (Cambridge, MA, USA) reported the safety and immunogenicity of a recombinant vaccine candidate, M2e-HBc fusion protein (ACAM-FLU-A) in its Phase I trial study [76]. The ACAM-FLU-A vaccine was demonstrated to be immunogenic and well-tolerated with no significant side-effects. M2e-HBc carrier protein vaccine also conferred partial protection of 70% survival from infection by the highly lethal avian H5N1 influenza strain in ferrets a more relevant animal model. The flagellin-adjuvanted HA fusion protein vaccine was tested in a clinical trial and shown to be immunogenic in elderly vaccinees [77]. An M2e-flagellin fusion vaccine (STF2.4xM2e) was also tested in healthy young volunteers, aged 18-49 as reported in the first Phase I clinical trial study by VaxInnate Corp. (Cranbury, NJ, USA) [76,78]. Low doses of flagellin-M2 vaccines (0.3 and 1.0 µg doses) were found to be safe and tolerated in subjects tested. Also, these M2e-flagellin conjugate vaccines were immunogenic in 75% vaccinees after the first dose and 96% after the second dose [76,78]. However, two high doses (3 and 10 µg doses) of flagellin-M2 vaccines were associated with the appearance of adverse effects of illness symptoms in some of the subjects. Therefore, toxicity of flagellin adjuvant might be an issue at higher doses of vaccines. Development of a safer vaccine based on M2 will be needed and VLP-based vaccines can be an attractive candidate without using additional adjuvants. These clinical trials merit further studies for developing safe and effective universal influenza vaccines.
Cross protective immunity by hemagglutinin stalk domain (HA2) vaccines
Functionally, influenza virus HA is composed of a receptor binding globular head domain of HA1 and a membrane-fusion inducing stalk domain of HA2 for virus entry [79]. Current influenza vaccination is based on immunity to the globular head domain of HA1 surrounded by variable antigenic sites contributing to the generation of numerous escape mutants [80,81]. The failure or low efficacy of influenza vaccination is primarily due to mutations occurring in the HA1 globular head domains of predicted influenza virus pathogens [82,83].
In an effort to identify conserved epitopes, recent studies have provided evidence that the HA stalk domain can be a potential target for developing universal vaccines. The sequence homology of the HA2 subunit among different subtypes is in a range of 51-80%, and the sequence conservation of HA2 is relatively higher than that of the HA1 subunit domain which is in a wider range between 34% and 59% [84]. The sequence conservation of the HA2 subunit among influenza virus strains within the same subtype is even higher [84]. In particular, specific regions in the HA stalk domains were identified to be highly conserved among different subtypes of influenza viruses, which can be divided into two main phylogenetic groups [8]. The group 1 includes the subtypes of H1, H2, H5, H6, H8, H9, H11, H12, H13, H16, and H17. The group 2 contains the subtypes of H3, H4, H7, H10, H14, and H15. A long α-helix domain in the HA2 subunit (the 76-130 amino acid region) was shown to have this conservation among different HA subtypes [85,86].
Recent studies demonstrate the feasibility of stalk domain-based vaccines. The chemically synthesized fusion peptide (amino acids 1-38 of HA2) was conjugated to the keyhole limpet hemocyanin and tested in mice as a vaccine [87,88]. Similarly, this vaccine provided survival protection against a low dose challenge with homologous and heterologous virus in immunized mice but showed severe weight loss, indicating its incapability of preventing illness [87,88]. A long α-helix HA2 vaccine consisting of the amino acid 76-130 polypeptide was coupled to the carrier protein keyhole limpet hemocyanin and its vaccine efficacy was tested I a mouse model [85,86]. Sera from immunized mice with an α-helix HA2 conjugate vaccine showed substantial binding antibodies reactive to heterosubtypic viruses [86]. This α-helix HA2 vaccine could confer partial survival protection against heterosubtypic challenge viruses (A/PR8 H1N1, A/Vietnam/04 H5N1 virus) and the homologous virus H3 subtype. Although the HA2 vaccine immune sera showed broader cross-reactivity with different HA molecules, the breadth was limited to the group 2 HAs (subtypes H3, H4, H7, H10, H14, and H15).
Using recombinant genetic engineering techniques, headless HA constructs that were composed of membrane-proximal portions of both the HA1 signal peptide region and HA2 subunits were stably expressed on the cell surfaces [89]. As well, these headless HA constructs were intended to avoid the highly immunogenic head domain. Co-expression of the human immunodeficiency virus (HIV) Gag core protein and headless HA protein by transient DNA co-transfections produced chimeric Gag VLPs containing headless HA molecules [89]. Two times vaccinations with DNA constructs (Gag+HA) were followed by boost immunization with chimeric headless HA VLP vaccines in the presence of Freund's complete adjuvant [89]. Immunization of mice with Headless HA VLP vaccines provided protection against homologous challenge with moderate body weight loss. The neutralizing activity in immune sera of mice with headless HA VLP vaccines was not conclusively confirmed [89]. Nonetheless, headless HA (A/PR8) VLP immune sera were likely to show greater reactivity to heterologous strains than the full-length HA vaccine [89]. A/Hong Kong/68 headless HA VLP vaccines did not induce antibodies cross reactive to different group 1 HAs (subtypes H1, H2, H5, H6, H8, H9, H11, H12, H13, and H16). Vaccines of influenza virions stripped of HA1 by treatment with acid or dithiothreitol were found not to be effective in inducing cross reactive antibodies and cross protection compared to the untreated control vaccines [90,91]. Possible limitations of these approaches include a low yield of headless HA VLPs produced by transient DNA transfection, use of Freund's adjuvant, and limited breadth due to the specificity of reactivity to certain HA subtypes.
Heterologous prime-boost immunization strategies may elicit cross-reactive anti-HA antibodies. A recent study from the Palese group demonstrated that prime-boost immunizations with chimeric HA influenza vaccine constructs could elicit broadly cross reactive stalk-specific antibodies [92]. Mice were repeatedly immunized with serial chimeric HA protein constructs of H7 HA head domain plus the H3 stalk domain, H5 HA head domain plus the H3 stalk domain, and H4 HA head domain plus the H3 stalk domain. After challenge of mice that were multiple times immunized with chimeric HA proteins, the immune sera were found to contain cross protective antibodies likely targeted to the stalk domain [92]. Interestingly, the stalk domain responsive antibodies were induced by H3N2 influenza virus infection but not by immunization with inactivated influenza virus vaccines [93]. Interestingly, when human subjects who were first primed with an H5 HA DNA vaccine were then boosted with an inactivated H5 vaccine, substantial levels of anti-HA stalk domain antibodies were elicited, which showed cross neutralizing activity against the group 1 viruses [94]. However, no promising and effective vaccines capable of inducing antibodies targeted to the stalk domain, which are protective regardless of HA subtypes, have been developed yet. Further development of these vaccines based on the stalk domain of HA would likely contribute toward universal influenza vaccines.
T Cell-Based Vaccines for Heterosubtypic Protection
Seasonal influenza viruses undergo continuous mutation in the antigenic sites of HA and NA molecules, which allow variants to escape from the neutralizing antibody responses. Since the majority of cytotoxic T lymphocytes (CTLs) can recognize relatively conserved viral proteins such as the NP, the PA and the matrix 1 protein (M1), they are able to contribute to heterosubtypic immunity between different subtypes [95,96].
It has been recognized that CTLs play a key role in eliminating influenza virus infected cells by inducing apoptosis through contact-dependent interactions [97]. There is evidence for the role of influenza virus-specific CTLs, which are elicited by vaccination or virus infection, in protection against infection with influenza A virus of different subtypes (Table 2). Previous studies have demonstrated that influenza virus-specific CTLs provide protective heterosubtypic immunity, which are confirmed by depletion in influenza virus-infected mice or adoptive transfer of influenza virus-specific CTLs into naïve mice [95,98,99].
Table 2.
The evidence of the role of T cells in heterosubtypic immunity
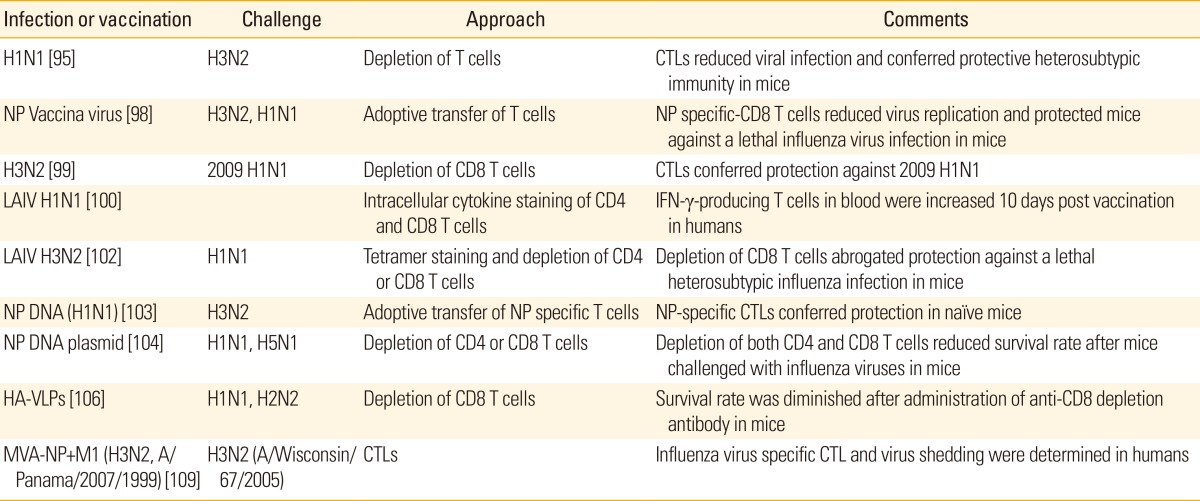
CTL, cytotoxic T-lymphocyte; NP, nucleoprotein; LAIV, live attenuated influenza virus; IFN-γ, interferon gamma; VLP, virus-like particle.
The majority of T cell-mediated vaccines target highly conserved internal proteins such as NP, PA and M1 proteins. The different approaches for T cell-based vaccine development have been used, which include the LAIVs, plasmid DNAs, viral vectors (modified vaccinia Ankara strain), and VLPs (Table 2). These T cell-based vaccines can also induce humoral antibody responses. One of popular trial is the use of LAIV which can be generated by adaptation at low temperatures. In humans, LAIV vaccination induced strong IFN-γ-producing CTLs than inactivated influenza vaccine [100]. Of interest, conserved NP-, PA-, and PB1-specific CD4 and CD8 T cells generated after attenuated cold-adapted H3N2 or a 2009 pandemic H1N1 vaccine conferred protection against heterosubtypic lethal challenges in mice [101,102].
In addition to LAIV, DNA vaccination can be another candidate. A previous study has shown that NP DNA vaccination increased CTL precursor frequency and provided better protection in NP DNA-immunized mice compared to mice vaccinated with HA DNA in response to challenges with heterologous influenza viruses [103,104]. Furthermore, other vaccine types have been described to induce influenza virus specific-CTL responses. Vaccination with complex adenovirus vector encoding H5, N1 and M1 genes induced antigen specific CTLs that were able to producing IFN-γ [105]. Recently, mice that were immunized with VLPs containing HA protein derived from PR8 were protected against homologous and heterosubtypic influenza virus infections and this protection was dependent on HA-specific CTL responses [106].
There is evidence that virus-specific CTLs can afford protection against a variety of influenza virus subtypes, but it is also important to consider generating antigen-specific antibody responses directed to external proteins HA and NA as well as internal proteins. Interestingly, CTLs specific for NP protein cooperatively synergize protective immunity with non-neutralizing antibodies [107,108]. Thus, it suggests that generation of both antigen-specific CTLs and antibodies is prerequisite for robust protective immunity against heterosubtypic influenza virus infections in human.
The replication defective vaccinia Ankara strain (MVA) expressing M1 and NP from A/Panama/2007/1999 virus (H3N2) (MVA-NP+M1) was tested in recent clinical trials [109]. Individuals were immunized with MVA-NA+M1 or unimmunized prior to challenge with A/Wisconsin/67/2005 H3N2 virus. Higher levels of influenza-specific CTL responses were observed compared to unvaccinated controls. Also, those who were vaccinated showed fewer days of virus shedding than unvaccinated control subjects. However, fewer numbers of subjects were enrolled and further validation with a larger number of subjects is warranted.
Roles of Innate Immunity in Vaccination
Recognition of microbial pathogens and vaccine antigens is an essential element for initiating adaptive immune responses as well as determining the quality of resulting host immune responses. Dendritic cells (DCs) and macrophages play a critical role in inducing protective adaptive immune responses of both T and B cells. We found that presenting HA antigen on VLPs was significantly much more effective in inducing protective T cell and B cell responses than the soluble HA protein antigen [110]. Effective induction of protective immunity by antigens in a VLP form is probably because particulate antigens are more likely to activate innate immune cells such as DCs.
Antigen-presenting cells (APCs) such as DCs and macrophages prominently express toll-like receptors (TLRs) which recognize pathogen, vaccine antigen, or adjuvant components. APCs play critical roles in activating innate immunity by recognizing and capturing pathogens or vaccine antigens at the site of infection or vaccination via receptors such as TLRs. Antigen-loaded APCs initiate the events of inducing the activation of adaptive T and B cells [111]. In cases where vaccine antigens (such as subunit vaccines) are not effective in stimulating APCs, adjuvants should be included in the vaccine formulation to activate APCs. Some compounds enhancing antigen depot or activating innate immunity by interacting with pathogen recognizing receptors (PRRs) such as TLRs have shown some promise. For example, alum, MF59, or AS04 (TLR agonist) adjuvants are often added to the subunit vaccine formulations. But live attenuated (cold-adapted) influenza vaccines are likely to activate TLR3 and 7 during viral replication intra-cellularly leading to the up-regulation of inflammatory cytokines [112], and thus adjuvants are not needed. Also, the live attenuated yellow fever vaccine, one of the most effective vaccines, was demonstrated to activate multiple DC subsets via TLRs 2, 7, 8, and 9 [113]. Activated DCs up-regulate costimulatory molecules through receptor-mediated recognition of a pathogen or vaccine antigen and can elicit the differentiation of naïve T cells into different effector T cells leading to the generation of cytotoxic CD8 T cells and activated B cells [111].
B cells are one of the important adaptive immune cells. Previous studies suggest that follicular B cells express TLR 1, 2, 4, 7, and 9. These B cells also showed proliferative responses and isotype switching upon the in vitro stimulation with TLR2 (Pam3Cys), TLR3 [poly(I:C)], TLR4 (lipopolysaccharide [LPS]), TLR7, and TLR9 agonists [114]. There have been controversies concerning whether TLR signaling is essential for B cell responses after vaccination. The addition of TLR9 ligand CpGs to B cells in vitro cultures induced the production of IgG2a, IgG2b and IgG3 antibodies [115]. An innate adaptor signaling molecule, myeloid differentiation factor-88 (MyD88), is known to be a key adaptor componentfor activation from the most TLRs except the TLR3 [116]. MyD88-deficient mice have been shown to have a defect in inducing T helper type 1 immune responses to ovalbumin plus complete Freund adjuvant [117]. Importantly, we found that MyD88-deficient mice showed a significant defect in generating T helper type 1 isotype switched antibodies, and interferon (IFN-γ) secreting T cell responses as well as for eliciting long-lived antibody secreting plasma cells and protective immunity after vaccination with influenza VLP vaccines [118]. Better understanding of stimulating innate immune components by vaccine antigens will provide informative insight into developing effective and safe vaccines.
Initially, TLRs were recognized as a family of PRR host cell proteins that recognize a wide range of pathogen-associated molecular patterns (PAMPs) in the microbial pathogens or vaccine antigens [116,119]. To date, 10 and 13 functional TLRs have been identified in humans and mice, respectively. TLR1, TLR2, TLR4, TLR5, TLR6, and TLR11 are expressed on the host cell surface. TLR3, TLR7, TLR8, TLR9, and orphan receptor TLR13 are expressed within intracellular compartments such as endosome and recognize nucleic acids [116,120]. TLR1, TLR2, and TLR6 recognize pathogen-derived molecules such as lipoproteins. TLR3 binds to double-stranded (ds) RNAs that are present in many RNA viruses including influenza virus. TLR4 recognizes bacterial LPS, fusion protein of respiratory syncytial virus, fibronectin, and heat-shock proteins. TLR5 is known to recognize bacterial flagellin molecules. TLR7 and TLR8 are activated by single-stranded (ss) RNA molecules that are present in RNA viruses such as influenza virus whereas TLR9 recognizes bacterial unmethylated DNA molecules. Once TLRs recognize various components of vaccine antigens or microorganisms including viruses, inflammatory cytokines are produced, which initiate the activation of signaling cascade leading to the induction of adaptive immune responses to pathogens or vaccine antigens.
Another important family of PRRs includes the C-type lectin receptors (CLRs), cytosolic proteins such as NOD-like receptors (NLRs) and cytoplasmic RNA helicase retinoic acid inducible gene I (RIG-I) or melanoma differentiation associated gene 5 (named RIG-I like receptors, RLRs) [121]. The representative CLRs are DC-specific ICAM-3 grabbing non-integrin and DC-associated C-type lectin-1 (dectin-1), both of which play key roles in inducing immune responses in response to fungal, bacterial or virus pathogen molecules. NLRs are expressed intracellulary and respond to various PAMPs to trigger inflammatory responses [121].
TLRs are expressed on various immune cells including macrophages, DCs, B cells, specific T cells and even expressed on non-immune cells such as fibroblasts and epithelial cells [114, 122,123]. All TLRs except TLR3 use the downstream adaptor molecule MyD88, whereas TLR3 and TLR4 in part use Toll receptor-associated activator of interferon (TRIF). After TLRs-ligand interaction, TLR activation results in triggering of downstream signaling cascades through the engagement of signaling intermediates, MyD88, Toll-interleukin (IL)-1 receptor-associated-protein (also known as MAL), TRIF, Toll receptor-associated molecule, IL-1 receptor associated kinase, and tumor necrosis factor receptor-associated factor 6. TLR ligation can result in activation of transcription factors (IRF3, IRF7, activator protein-1, nuclear factor-κB) and consequently produce the proinflammatory cytokines and chemokines. Furthermore some TLRs (TLR3, 4, 7, 8, 9) are capable of inducing type 1 interferons (IFN-α/β) to elicit antiviral responses [116].
Vaccine Adjuvants
Adjuvants are used as vaccine additives to lower antigen loads in a vaccine or to increase vaccine efficacy [124]. Adjuvants modulate host immune responses and magnify immunogenicity of the vaccine. In general, influenza vaccine such as split vaccine or live attenuated vaccine can elicit host immune responses in primed healthy individuals without adjuvants. However, in the elderly or immune-compromised populations, adjuvants are needed to increase responsiveness to the vaccine [125]. Adjuvants have a critical role in inducing innate, adaptive and memory immune responses to some vaccine antigens.
Representative adjuvants and their possible action mechanisms are listed in the Table 3. Aluminium adjuvant (Alum) is the most commonly used vaccine adjuvants. It has been used for more than 70 years because of its safety and capacity of making antigen depot [126]. Alum adsorbs the vaccine antigen and makes the antigen stay longer in the injection site, so that immunogenicity of the antigen is increased. In an immunological mechanism study, alum was shown to activate NALP3 inflammasome and induce IL-1β production to stimulate the innate immune system. Alum is likely to induce T helper type 2 immune responses to co-administered antigens in humans [127].
Table 3.
Various adjuvants used in vaccines
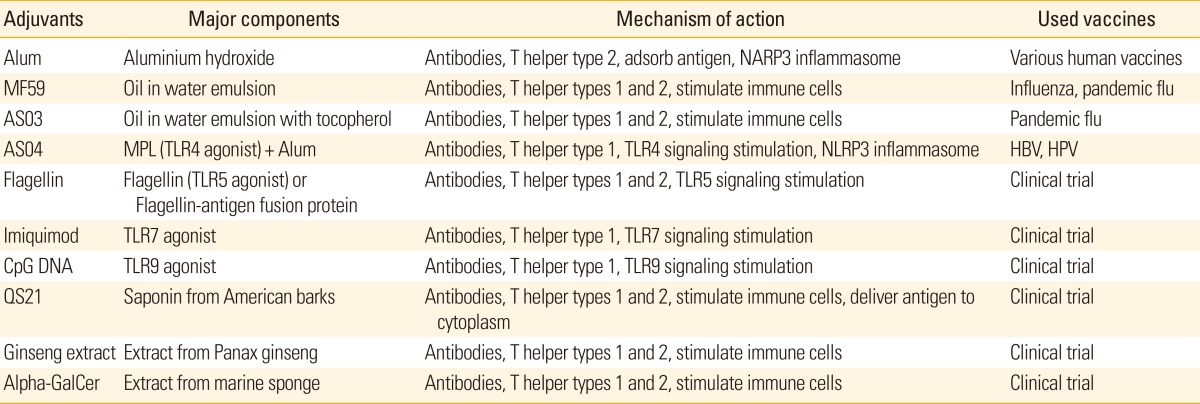
MPL, monophosphoryl lipid A; TLR, toll-like receptor; HBV, hepatitis B virus; HPV, human papillomavirus.
MF59 is an oil-in-water emulsion type of adjuvants, and composed of squalene, polysorbate 80, sorbitan trioleate, trisodium citrate dehydrate, citric acid monohydrate and water for injection [128]. MF59 adjvuant is used in influenza vaccine (Fluad) and pandemic flu vaccine. Use of MF59 adjvuant resulted in stronger antibody responses and vaccine antigen dose sparing effects [129]. MF59 stimulates cells in the sites of injection to express chemokines and cytokines. These chemokines and cytokines recruit innate immune cells and APCs. Some antigen presenting cells subsequently uptake antigen-MF59 complex and migrate to draining lymph nodes for the induction of adaptive immune responses [130,131]. AS03 is a modified form of MF59 and is an oil-in-water emulsion with a tocopherol. This form of adjuvant was used in pandemic influenza vaccine (Pandemrix) [132]. TLR agonists are considered as potential adjuvants, so many different kinds of TLR agonists have been tried in experimental animal models and clinical trials. AS04, which contains Alum and monophosphoryl lipid A (MPL), is a licensed adjuvant in hepatitis B virus (HBV) vaccine (Fendrix) [133] and human papillomavirus vaccine (Cervarix) [134]. MPL is a detoxified form of LPS, which is a TLR4 agonist. It can activate immune cells such as monocytes and myeloid dendritic cells directly to induce immune responses to the vaccine antigen [124]. Flagellin, a TLR5 agonist and a motor apparatus of bacteria, can induce mixed T helper types 1 and 2 immune responses. Flagellin-antigen fusion proteins were developed to magnify the vaccine and adjuvant effects [135]. Imiquimod, a TLR7 agonist, and CpG DNA, a TLR9 agonist, stimulate plasmacytoid dendritic cells which can produce type 1 interferons to induce immune responses to intracellular pathogens such as virus [124].
Recently, natural substances have received attention as a potential adjuvant compounds. QS21, derived from American bark, is a saponin-based adjuvant. QS21 can stimulate dendritic cells directly and also destabilize the membrane of the endosome to deliver antigen to the cytoplasm, so that it can elicit cellular immune responses [136]. Another example of the natural adjuvants is an extract from Panax ginseng. It induced a balanced T helper types 1 and 2 immune response [137]. Many marine organisms, for example, sponge and algae extracts, are also investigated actively in experimental and clinical level. Alpha-galactosylceramide (alpha-GalCer), an extract from marine sponge, is known to stimulate natural killer T cells and induce antibody production, and balanced T helper types 1 and 2 immune responses [138].
Conclusion
Until now, most licensed influenza vaccines are manufactured by methods that were established more than 50 years ago despite recent scientific advances in vaccinology. New vaccines against influenza viruses to improve the breadth of protection would be feasible but some technical, regulatory, and logistical challenges remain to be resolved.
Many studies reporting universal influenza vaccines have focused on conserved single peptides or proteins as target antigens (M2e, HA2 stalk domain, NP, M1) in the presence of adjuvants in animal models. These conserved antigenic targets have relatively weak immunogenicity (Table 1). Experimental vaccines based on the HA2 stalk domain or M2e external domain of ion channel protein are not capable of inducing neutralizing antibodies although some monoclonal antibodies binding to the HA2 stalk domain are known to have cross neutralizing activity. Immunization with T-cell vaccines could provide survival protection but not prevent infection. Therefore, the protective efficacy of these candidate universal vaccines would be lower than strain-specific HA based vaccines of inducing neutralizing antibodies.
It is needed to develop new qualitative and quantitative methods to define the potency of the vaccine as well as to identify immune correlates of cross protection. The path to licensure of novel influenza vaccines will require demonstration of efficacy in humans. Vaccines that do not prevent infection but ameliorate disease will need a larger scale of clinical trials. Public health authorities will evaluate how truly universal novel influenza vaccines are. Challenging decisions include whom to vaccinate and how often the universal vaccine may require updating.
As alternative approaches to developing truly universal vaccines, supplementation concept will be proven to be feasible by complementing and broadening the efficacy of current vaccines based on the strain-specific immunity. We have shown that supplementing the whole inactivated virus with the conserved M2 VLP vaccine was found to significantly improve the heterosubtypic cross protection [70]. With the emergence of drafting epidemic strains or an outbreak of pandemic, the supplemented vaccination would significantly prevent the mortality and ameliorate morbidity.
It will provide highly informative insight into developing novel new vaccines and adjuvants if we better understand the immunological mechanisms how cross protective vaccines work and by which certain adjuvants enhance the immunogenicity of vaccines. Also, deciphering the roles of innate immune components in contributing to long term protective immunity will be an important area to be explored for designing and developing effective vaccines. In addition, current vaccines are mostly given by intramuscular injection using syringe-needles and administered by medical personnel. It is also an important area in vaccine field to develop new vaccine technologies and alternative routes of immunization such as needle-free skin delivery, oral, nasal, and sublingual immunization.
Footnotes
No potential conflict of interest relevant to this article was reported.
This work was partially supported by NIH/NIAID grants AI105170 (S.M.K.) and AI093772 (S.M.K.).
References
- 1.Stokes J, Chenoweth AD, Waltz AD, Gladen RG, Shaw D. Results of immunization by means of active virus of human influenza. J Clin Invest. 1937;16:237–243. doi: 10.1172/JCI100853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Davenport FM. Current knowledge of influenza vaccine. JAMA. 1962;182:11–13. doi: 10.1001/jama.1962.03050400013003. [DOI] [PubMed] [Google Scholar]
- 3.Glaser CA, Gilliam S, Thompson WW, et al. Medical care capacity for influenza outbreaks, Los Angeles. Emerg Infect Dis. 2002;8:569–574. doi: 10.3201/eid0806.010370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Poehling KA, Edwards KM, Weinberg GA, et al. The underrecognized burden of influenza in young children. N Engl J Med. 2006;355:31–40. doi: 10.1056/NEJMoa054869. [DOI] [PubMed] [Google Scholar]
- 5.Thompson WW, Shay DK, Weintraub E, et al. Influenza-associated hospitalizations in the United States. JAMA. 2004;292:1333–1340. doi: 10.1001/jama.292.11.1333. [DOI] [PubMed] [Google Scholar]
- 6.Palese P, Compans RW. Inhibition of influenza virus replication in tissue culture by 2-deoxy-2,3-dehydro-N-trifluoroacetylneuraminic acid (FANA): mechanism of action. J Gen Virol. 1976;33:159–163. doi: 10.1099/0022-1317-33-1-159. [DOI] [PubMed] [Google Scholar]
- 7.Matrosovich MN, Matrosovich TY, Gray T, Roberts NA, Klenk HD. Neuraminidase is important for the initiation of influenza virus infection in human airway epithelium. J Virol. 2004;78:12665–12667. doi: 10.1128/JVI.78.22.12665-12667.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pica N, Palese P. Toward a universal influenza virus vaccine: prospects and challenges. Annu Rev Med. 2013;64:189–202. doi: 10.1146/annurev-med-120611-145115. [DOI] [PubMed] [Google Scholar]
- 9.Francis T, Jr, Salk JE, Brace WM. The protective effect of vaccination against epidemic influenza B. J Am Med Assoc. 1946;131:275–278. doi: 10.1001/jama.1946.02870210011003. [DOI] [PubMed] [Google Scholar]
- 10.Salk JE, Pearson HE, Brown PN, Francis T. Protective effect of vaccination against induced influenza B. J Clin Invest. 1945;24:547–553. doi: 10.1172/JCI101634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Robertson JS, Nicolson C, Newman R, Major D, Dunleavy U, Wood JM. High growth reassortant influenza vaccine viruses: new approaches to their control. Biologicals. 1992;20:213–220. doi: 10.1016/s1045-1056(05)80040-5. [DOI] [PubMed] [Google Scholar]
- 12.al-Mazrou A, Scheifele DW, Soong T, Bjornson G. Comparison of adverse reactions to whole-virion and split-virion influenza vaccines in hospital personnel. CMAJ. 1991;145:213–218. [PMC free article] [PubMed] [Google Scholar]
- 13.Cate TR, Couch RB, Kasel JA, Six HR. Clinical trials of monovalent influenza A/New Jersey/76 virus vaccines in adults: reactogenicity, antibody response, and antibody persistence. J Infect Dis. 1977;136(Suppl):S450–S455. doi: 10.1093/infdis/136.supplement_3.s450. [DOI] [PubMed] [Google Scholar]
- 14.Wright PF, Cherry JD, Foy HM, et al. Antigenicity and reactogenicity of influenza A/USSR/77 virus vaccine in children: a multicentered evaluation of dosage and safety. Rev Infect Dis. 1983;5:758–764. doi: 10.1093/clinids/5.4.758. [DOI] [PubMed] [Google Scholar]
- 15.Quinnan GV, Schooley R, Dolin R, Ennis FA, Gross P, Gwaltney JM. Serologic responses and systemic reactions in adults after vaccination with monovalent A/USSR/77 and trivalent A/USSR/77, A/Texas/77, B/Hong Kong/72 influenza vaccines. Rev Infect Dis. 1983;5:748–757. doi: 10.1093/clinids/5.4.748. [DOI] [PubMed] [Google Scholar]
- 16.Murphy BR, Coelingh K. Principles underlying the development and use of live attenuated cold-adapted influenza A and B virus vaccines. Viral Immunol. 2002;15:295–323. doi: 10.1089/08828240260066242. [DOI] [PubMed] [Google Scholar]
- 17.Harper SA, Fukuda K, Uyeki TM, et al. Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2004;53:1–40. [PubMed] [Google Scholar]
- 18.Belshe RB, Ambrose CS, Yi T. Safety and efficacy of live attenuated influenza vaccine in children 2-7 years of age. Vaccine. 2008;26(Suppl 4):D10–D16. doi: 10.1016/j.vaccine.2008.06.083. [DOI] [PubMed] [Google Scholar]
- 19.Treanor J, Keitel W, Belshe R, et al. Evaluation of a single dose of half strength inactivated influenza vaccine in healthy adults. Vaccine. 2002;20:1099–1105. doi: 10.1016/s0264-410x(01)00440-6. [DOI] [PubMed] [Google Scholar]
- 20.Belshe RB, Newman FK, Wilkins K, et al. Comparative immunogenicity of trivalent influenza vaccine administered by intradermal or intramuscular route in healthy adults. Vaccine. 2007;25:6755–6763. doi: 10.1016/j.vaccine.2007.06.066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bergen R, Black S, Shinefield H, et al. Safety of cold-adapted live attenuated influenza vaccine in a large cohort of children and adolescents. Pediatr Infect Dis J. 2004;23:138–144. doi: 10.1097/01.inf.0000109392.96411.4f. [DOI] [PubMed] [Google Scholar]
- 22.Block SL, Yogev R, Hayden FG, Ambrose CS, Zeng W, Walker RE. Shedding and immunogenicity of live attenuated influenza vaccine virus in subjects 5-49 years of age. Vaccine. 2008;26:4940–4946. doi: 10.1016/j.vaccine.2008.07.013. [DOI] [PubMed] [Google Scholar]
- 23.Wacheck V, Egorov A, Groiss F, et al. A novel type of influenza vaccine: safety and immunogenicity of replication-deficient influenza virus created by deletion of the interferon antagonist NS1. J Infect Dis. 2010;201:354–362. doi: 10.1086/649428. [DOI] [PubMed] [Google Scholar]
- 24.Peiris M, Yuen KY, Leung CW, et al. Human infection with influenza H9N2. Lancet. 1999;354:916–917. doi: 10.1016/s0140-6736(99)03311-5. [DOI] [PubMed] [Google Scholar]
- 25.Fouchier RA, Schneeberger PM, Rozendaal FW, et al. Avian influenza A virus (H7N7) associated with human conjunctivitis and a fatal case of acute respiratory distress syndrome. Proc Natl Acad Sci U S A. 2004;101:1356–1361. doi: 10.1073/pnas.0308352100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wong SS, Yuen KY. Avian influenza virus infections in humans. Chest. 2006;129:156–168. doi: 10.1378/chest.129.1.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cheung CL, Rayner JM, Smith GJ, et al. Distribution of amantadine-resistant H5N1 avian influenza variants in Asia. J Infect Dis. 2006;193:1626–1629. doi: 10.1086/504723. [DOI] [PubMed] [Google Scholar]
- 28.de Jong MD, Tran TT, Truong HK, et al. Oseltamivir resistance during treatment of influenza A (H5N1) infection. N Engl J Med. 2005;353:2667–2672. doi: 10.1056/NEJMoa054512. [DOI] [PubMed] [Google Scholar]
- 29.Le QM, Kiso M, Someya K, et al. Avian flu: isolation of drug-resistant H5N1 virus. Nature. 2005;437:1108. doi: 10.1038/4371108a. [DOI] [PubMed] [Google Scholar]
- 30.Gao R, Cao B, Hu Y, et al. Human infection with a novel avian-origin influenza A (H7N9) virus. N Engl J Med. 2013;368:1888–1897. doi: 10.1056/NEJMoa1304459. [DOI] [PubMed] [Google Scholar]
- 31.Subbarao K, Klimov A, Katz J, et al. Characterization of an avian influenza A (H5N1) virus isolated from a child with a fatal respiratory illness. Science. 1998;279:393–396. doi: 10.1126/science.279.5349.393. [DOI] [PubMed] [Google Scholar]
- 32.Claas EC, Osterhaus AD, van Beek R, et al. Human influenza A H5N1 virus related to a highly pathogenic avian influenza virus. Lancet. 1998;351:472–477. doi: 10.1016/S0140-6736(97)11212-0. [DOI] [PubMed] [Google Scholar]
- 33.Buranathai C, Amonsin A, Chaisigh A, Theamboonlers A, Pariyothorn N, Poovorawan Y. Surveillance activities and molecular analysis of H5N1 highly pathogenic avian influenza viruses from Thailand, 2004-2005. Avian Dis. 2007;51(1 Suppl):194–200. doi: 10.1637/7594-040306R.1. [DOI] [PubMed] [Google Scholar]
- 34.Van Borm S, Thomas I, Hanquet G, et al. Highly pathogenic H5N1 influenza virus in smuggled Thai eagles, Belgium. Emerg Infect Dis. 2005;11:702–705. doi: 10.3201/eid1105.050211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Wan XF, Nguyen T, Davis CT, et al. Evolution of highly pathogenic H5N1 avian influenza viruses in Vietnam between 2001 and 2007. PLoS One. 2008;3:e3462. doi: 10.1371/journal.pone.0003462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Nava GM, Attene-Ramos MS, Ang JK, Escorcia M. Origins of the new influenza A(H1N1) virus: time to take action. Euro Surveill. 2009;14:19228. doi: 10.2807/ese.14.22.19228-en. [DOI] [PubMed] [Google Scholar]
- 37.Solovyov A, Palacios G, Briese T, Lipkin WI, Rabadan R. Cluster analysis of the origins of the new influenza A(H1N1) virus. Euro Surveill. 2009;14:19224. doi: 10.2807/ese.14.21.19224-en. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Pinto LH, Holsinger LJ, Lamb RA. Influenza virus M2 protein has ion channel activity. Cell. 1992;69:517–528. doi: 10.1016/0092-8674(92)90452-i. [DOI] [PubMed] [Google Scholar]
- 39.Chizhmakov IV, Geraghty FM, Ogden DC, Hayhurst A, Antoniou M, Hay AJ. Selective proton permeability and pH regulation of the influenza virus M2 channel expressed in mouse erythroleukaemia cells. J Physiol. 1996;494(Pt 2):329–336. doi: 10.1113/jphysiol.1996.sp021495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mould JA, Drury JE, Frings SM, et al. Permeation and activation of the M2 ion channel of influenza A virus. J Biol Chem. 2000;275:31038–31050. doi: 10.1074/jbc.M003663200. [DOI] [PubMed] [Google Scholar]
- 41.Leonov H, Astrahan P, Krugliak M, Arkin IT. How do aminoadamantanes block the influenza M2 channel, and how does resistance develop? J Am Chem Soc. 2011;133:9903–9911. doi: 10.1021/ja202288m. [DOI] [PubMed] [Google Scholar]
- 42.Lin TI, Heider H, Schroeder C. Different modes of inhibition by adamantane amine derivatives and natural polyamines of the functionally reconstituted influenza virus M2 proton channel protein. J Gen Virol. 1997;78(Pt 4):767–774. doi: 10.1099/0022-1317-78-4-767. [DOI] [PubMed] [Google Scholar]
- 43.Fiers W, De Filette M, Birkett A, Neirynck S, Min Jou W. A "universal" human influenza A vaccine. Virus Res. 2004;103:173–176. doi: 10.1016/j.virusres.2004.02.030. [DOI] [PubMed] [Google Scholar]
- 44.Liu W, Zou P, Ding J, Lu Y, Chen YH. Sequence comparison between the extracellular domain of M2 protein human and avian influenza A virus provides new information for bivalent influenza vaccine design. Microbes Infect. 2005;7:171–177. doi: 10.1016/j.micinf.2004.10.006. [DOI] [PubMed] [Google Scholar]
- 45.Zebedee SL, Lamb RA. Influenza A virus M2 protein: monoclonal antibody restriction of virus growth and detection of M2 in virions. J Virol. 1988;62:2762–2772. doi: 10.1128/jvi.62.8.2762-2772.1988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hughey PG, Roberts PC, Holsinger LJ, Zebedee SL, Lamb RA, Compans RW. Effects of antibody to the influenza A virus M2 protein on M2 surface expression and virus assembly. Virology. 1995;212:411–421. doi: 10.1006/viro.1995.1498. [DOI] [PubMed] [Google Scholar]
- 47.Roberts PC, Lamb RA, Compans RW. The M1 and M2 proteins of influenza A virus are important determinants in filamentous particle formation. Virology. 1998;240:127–137. doi: 10.1006/viro.1997.8916. [DOI] [PubMed] [Google Scholar]
- 48.Treanor JJ, Tierney EL, Zebedee SL, Lamb RA, Murphy BR. Passively transferred monoclonal antibody to the M2 protein inhibits influenza A virus replication in mice. J Virol. 1990;64:1375–1377. doi: 10.1128/jvi.64.3.1375-1377.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Wang R, Song A, Levin J, et al. Therapeutic potential of a fully human monoclonal antibody against influenza A virus M2 protein. Antiviral Res. 2008;80:168–177. doi: 10.1016/j.antiviral.2008.06.002. [DOI] [PubMed] [Google Scholar]
- 50.Slepushkin VA, Katz JM, Black RA, Gamble WC, Rota PA, Cox NJ. Protection of mice against influenza A virus challenge by vaccination with baculovirus-expressed M2 protein. Vaccine. 1995;13:1399–1402. doi: 10.1016/0264-410x(95)92777-y. [DOI] [PubMed] [Google Scholar]
- 51.Neirynck S, Deroo T, Saelens X, Vanlandschoot P, Jou WM, Fiers W. A universal influenza A vaccine based on the extracellular domain of the M2 protein. Nat Med. 1999;5:1157–1163. doi: 10.1038/13484. [DOI] [PubMed] [Google Scholar]
- 52.Fan J, Liang X, Horton MS, et al. Preclinical study of influenza virus A M2 peptide conjugate vaccines in mice, ferrets, and rhesus monkeys. Vaccine. 2004;22:2993–3003. doi: 10.1016/j.vaccine.2004.02.021. [DOI] [PubMed] [Google Scholar]
- 53.De Filette M, Fiers W, Martens W, et al. Improved design and intranasal delivery of an M2e-based human influenza A vaccine. Vaccine. 2006;24:6597–6601. doi: 10.1016/j.vaccine.2006.05.082. [DOI] [PubMed] [Google Scholar]
- 54.Ionescu RM, Przysiecki CT, Liang X, et al. Pharmaceutical and immunological evaluation of human papillomavirus viruslike particle as an antigen carrier. J Pharm Sci. 2006;95:70–79. doi: 10.1002/jps.20493. [DOI] [PubMed] [Google Scholar]
- 55.Bessa J, Schmitz N, Hinton HJ, Schwarz K, Jegerlehner A, Bachmann MF. Efficient induction of mucosal and systemic immune responses by virus-like particles administered intranasally: implications for vaccine design. Eur J Immunol. 2008;38:114–126. doi: 10.1002/eji.200636959. [DOI] [PubMed] [Google Scholar]
- 56.Tompkins SM, Zhao ZS, Lo CY, et al. Matrix protein 2 vaccination and protection against influenza viruses, including subtype H5N1. Emerg Infect Dis. 2007;13:426–435. doi: 10.3201/eid1303.061125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Fu TM, Grimm KM, Citron MP, et al. Comparative immunogenicity evaluations of influenza A virus M2 peptide as recombinant virus like particle or conjugate vaccines in mice and monkeys. Vaccine. 2009;27:1440–1447. doi: 10.1016/j.vaccine.2008.12.034. [DOI] [PubMed] [Google Scholar]
- 58.Ernst WA, Kim HJ, Tumpey TM, et al. Protection against H1, H5, H6 and H9 influenza A infection with liposomal matrix 2 epitope vaccines. Vaccine. 2006;24:5158–5168. doi: 10.1016/j.vaccine.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 59.Huleatt JW, Nakaar V, Desai P, et al. Potent immunogenicity and efficacy of a universal influenza vaccine candidate comprising a recombinant fusion protein linking influenza M2e to the TLR5 ligand flagellin. Vaccine. 2008;26:201–214. doi: 10.1016/j.vaccine.2007.10.062. [DOI] [PubMed] [Google Scholar]
- 60.De Filette M, Ramne A, Birkett A, et al. The universal influenza vaccine M2e-HBc administered intranasally in combination with the adjuvant CTA1-DD provides complete protection. Vaccine. 2006;24:544–551. doi: 10.1016/j.vaccine.2005.08.061. [DOI] [PubMed] [Google Scholar]
- 61.De Filette M, Min Jou W, Birkett A, et al. Universal influenza A vaccine: optimization of M2-based constructs. Virology. 2005;337:149–161. doi: 10.1016/j.virol.2005.04.004. [DOI] [PubMed] [Google Scholar]
- 62.Heinen PP, Rijsewijk FA, de Boer-Luijtze EA, Bianchi AT. Vaccination of pigs with a DNA construct expressing an influenza virus M2-nucleoprotein fusion protein exacerbates disease after challenge with influenza A virus. J Gen Virol. 2002;83(Pt 8):1851–1859. doi: 10.1099/0022-1317-83-8-1851. [DOI] [PubMed] [Google Scholar]
- 63.Jegerlehner A, Schmitz N, Storni T, Bachmann MF. Influenza A vaccine based on the extracellular domain of M2: weak protection mediated via antibody-dependent NK cell activity. J Immunol. 2004;172:5598–5605. doi: 10.4049/jimmunol.172.9.5598. [DOI] [PubMed] [Google Scholar]
- 64.De Filette M, Martens W, Roose K, et al. An influenza A vaccine based on tetrameric ectodomain of matrix protein 2. J Biol Chem. 2008;283:11382–11387. doi: 10.1074/jbc.M800650200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Kang SM, Kim MC, Compans RW. Virus-like particles as universal influenza vaccines. Expert Rev Vaccines. 2012;11:995–1007. doi: 10.1586/erv.12.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kang SM, Pushko P, Bright RA, Smith G, Compans RW. Influenza virus-like particles as pandemic vaccines. Curr Top Microbiol Immunol. 2009;333:269–289. doi: 10.1007/978-3-540-92165-3_14. [DOI] [PubMed] [Google Scholar]
- 67.Rodríguez-Limas WA, Sekar K, Tyo KE. Virus-like particles: the future of microbial factories and cell-free systems as platforms for vaccine development. Curr Opin Biotechnol. 2013;24:1089–1093. doi: 10.1016/j.copbio.2013.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Roldão A, Mellado MC, Castilho LR, Carrondo MJ, Alves PM. Virus-like particles in vaccine development. Expert Rev Vaccines. 2010;9:1149–1176. doi: 10.1586/erv.10.115. [DOI] [PubMed] [Google Scholar]
- 69.Song JM, Wang BZ, Park KM, et al. Influenza virus-like particles containing M2 induce broadly cross protective immunity. PLoS One. 2011;6:e14538. doi: 10.1371/journal.pone.0014538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Song JM, Van Rooijen N, Bozja J, Compans RW, Kang SM. Vaccination inducing broad and improved cross protection against multiple subtypes of influenza A virus. Proc Natl Acad Sci U S A. 2011;108:757–761. doi: 10.1073/pnas.1012199108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Kim MC, Song JM, O E, et al. Virus-like particles containing multiple M2 extracellular domains confer improved cross-protection against various subtypes of influenza virus. Mol Ther. 2013;21:485–492. doi: 10.1038/mt.2012.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Kim MC, Lee JS, Kwon YM, et al. Multiple heterologous M2 extracellular domains presented on virus-like particles confer broader and stronger M2 immunity than live influenza A virus infection. Antiviral Res. 2013;99:328–335. doi: 10.1016/j.antiviral.2013.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.El Bakkouri K, Descamps F, De Filette M, et al. Universal vaccine based on ectodomain of matrix protein 2 of influenza A: Fc receptors and alveolar macrophages mediate protection. J Immunol. 2011;186:1022–1031. doi: 10.4049/jimmunol.0902147. [DOI] [PubMed] [Google Scholar]
- 74.Pei S, Xiong N, Zhang Y, Chen S. Increasing M2 epitope density enhances systemic and mucosal immune responses to influenza A virus. Biotechnol Lett. 2009;31:1851–1856. doi: 10.1007/s10529-009-0102-6. [DOI] [PubMed] [Google Scholar]
- 75.Wei G, Meng W, Guo H, et al. Potent neutralization of influenza A virus by a single-domain antibody blocking M2 ion channel protein. PLoS One. 2011;6:e28309. doi: 10.1371/journal.pone.0028309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Vaxinnate. VaxInnate's universal flu vaccine candidate shown safe and immunogenic in Phase I clinical study [Internet] Cranbury: Vaxinnate; 2013. [cited 2013 Sep 1]. Available from: http://www.vaxinnate.com/pages/pressreleases/20081026_001.html. [Google Scholar]
- 77.Taylor DN, Treanor JJ, Strout C, et al. Induction of a potent immune response in the elderly using the TLR-5 agonist, flagellin, with a recombinant hemagglutinin influenza-flagellin fusion vaccine (VAX125, STF2.HA1 SI) Vaccine. 2011;29:4897–4902. doi: 10.1016/j.vaccine.2011.05.001. [DOI] [PubMed] [Google Scholar]
- 78.Turley CB, Rupp RE, Johnson C, et al. Safety and immunogenicity of a recombinant M2e-flagellin influenza vaccine (STF2.4xM2e) in healthy adults. Vaccine. 2011;29:5145–5152. doi: 10.1016/j.vaccine.2011.05.041. [DOI] [PubMed] [Google Scholar]
- 79.Wilson IA, Skehel JJ, Wiley DC. Structure of the haemagglutinin membrane glycoprotein of influenza virus at 3 A resolution. Nature. 1981;289:366–373. doi: 10.1038/289366a0. [DOI] [PubMed] [Google Scholar]
- 80.Laver WG, Gerhard W, Webster RG, Frankel ME, Air GM. Antigenic drift in type A influenza virus: peptide mapping and antigenic analysis of A/PR/8/34 (HON1) variants selected with monoclonal antibodies. Proc Natl Acad Sci U S A. 1979;76:1425–1429. doi: 10.1073/pnas.76.3.1425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Laver WG, Air GM, Dopheide TA, Ward CW. Amino acid sequence changes in the haemagglutinin of A/Hong Kong (H3N2) influenza virus during the period 1968-77. Nature. 1980;283:454–457. doi: 10.1038/283454a0. [DOI] [PubMed] [Google Scholar]
- 82.Gerhard W, Yewdell J, Frankel ME, Webster R. Antigenic structure of influenza virus haemagglutinin defined by hybridoma antibodies. Nature. 1981;290:713–717. doi: 10.1038/290713a0. [DOI] [PubMed] [Google Scholar]
- 83.Wiley DC, Skehel JJ. The structure and function of the hemagglutinin membrane glycoprotein of influenza virus. Annu Rev Biochem. 1987;56:365–394. doi: 10.1146/annurev.bi.56.070187.002053. [DOI] [PubMed] [Google Scholar]
- 84.Krystal M, Elliott RM, Benz EW, Jr, Young JF, Palese P. Evolution of influenza A and B viruses: conservation of structural features in the hemagglutinin genes. Proc Natl Acad Sci U S A. 1982;79:4800–4804. doi: 10.1073/pnas.79.15.4800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Wang TT, Tan GS, Hai R, et al. Vaccination with a synthetic peptide from the influenza virus hemagglutinin provides protection against distinct viral subtypes. Proc Natl Acad Sci U S A. 2010;107:18979–18984. doi: 10.1073/pnas.1013387107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Wang TT, Tan GS, Hai R, et al. Broadly protective monoclonal antibodies against H3 influenza viruses following sequential immunization with different hemagglutinins. PLoS Pathog. 2010;6:e1000796. doi: 10.1371/journal.ppat.1000796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Bommakanti G, Citron MP, Hepler RW, et al. Design of an HA2-based Escherichia coli expressed influenza immunogen that protects mice from pathogenic challenge. Proc Natl Acad Sci U S A. 2010;107:13701–13706. doi: 10.1073/pnas.1007465107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Staneková Z, Kiraly J, Stropkovska A, et al. Heterosubtypic protective immunity against influenza A virus induced by fusion peptide of the hemagglutinin in comparison to ectodomain of M2 protein. Acta Virol. 2011;55:61–67. doi: 10.4149/av_2011_01_61. [DOI] [PubMed] [Google Scholar]
- 89.Steel J, Lowen AC, Wang TT, et al. Influenza virus vaccine based on the conserved hemagglutinin stalk domain. MBio. 2010;1:e00018–e00010. doi: 10.1128/mBio.00018-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Graves PN, Schulman JL, Young JF, Palese P. Preparation of influenza virus subviral particles lacking the HA1 subunit of hemagglutinin: unmasking of cross-reactive HA2 determinants. Virology. 1983;126:106–116. doi: 10.1016/0042-6822(83)90465-8. [DOI] [PubMed] [Google Scholar]
- 91.Quan FS, Li ZN, Kim MC, et al. Immunogenicity of low-pH treated whole viral influenza vaccine. Virology. 2011;417:196–202. doi: 10.1016/j.virol.2011.05.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Krammer F, Pica N, Hai R, Margine I, Palese P. Chimeric hemagglutinin influenza virus vaccine constructs elicit broadly protective stalk-specific antibodies. J Virol. 2013;87:6542–6550. doi: 10.1128/JVI.00641-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Margine I, Krammer F, Hai R, et al. Hemagglutinin stalk-based universal vaccine constructs protect against group 2 influenza A viruses. J Virol. 2013;87:10435–10446. doi: 10.1128/JVI.01715-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Ledgerwood JE, Wei CJ, Hu Z, et al. DNA priming and influenza vaccine immunogenicity: two phase 1 open label randomised clinical trials. Lancet Infect Dis. 2011;11:916–924. doi: 10.1016/S1473-3099(11)70240-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Liang S, Mozdzanowska K, Palladino G, Gerhard W. Heterosubtypic immunity to influenza type A virus in mice. Effector mechanisms and their longevity. J Immunol. 1994;152:1653–1661. [PubMed] [Google Scholar]
- 96.Nguyen HH, Moldoveanu Z, Novak MJ, et al. Heterosubtypic immunity to lethal influenza A virus infection is associated with virus-specific CD8(+) cytotoxic T lymphocyte responses induced in mucosa-associated tissues. Virology. 1999;254:50–60. doi: 10.1006/viro.1998.9521. [DOI] [PubMed] [Google Scholar]
- 97.Holt PG, Strickland DH, Wikstrom ME, Jahnsen FL. Regulation of immunological homeostasis in the respiratory tract. Nat Rev Immunol. 2008;8:142–152. doi: 10.1038/nri2236. [DOI] [PubMed] [Google Scholar]
- 98.Taylor PM, Askonas BA. Influenza nucleoprotein-specific cytotoxic T-cell clones are protective in vivo. Immunology. 1986;58:417–420. [PMC free article] [PubMed] [Google Scholar]
- 99.Guo H, Santiago F, Lambert K, Takimoto T, Topham DJ. T cell-mediated protection against lethal 2009 pandemic H1N1 influenza virus infection in a mouse model. J Virol. 2011;85:448–455. doi: 10.1128/JVI.01812-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Antonis AF, Bruschke CJ, Rueda P, et al. A novel recombinant virus-like particle vaccine for prevention of porcine parvovirus-induced reproductive failure. Vaccine. 2006;24:5481–5490. doi: 10.1016/j.vaccine.2006.03.089. [DOI] [PubMed] [Google Scholar]
- 101.Powell TJ, Strutt T, Reome J, et al. Priming with cold-adapted influenza A does not prevent infection but elicits long-lived protection against supralethal challenge with heterosubtypic virus. J Immunol. 2007;178:1030–1038. doi: 10.4049/jimmunol.178.2.1030. [DOI] [PubMed] [Google Scholar]
- 102.Chen GL, Lau YF, Lamirande EW, McCall AW, Subbarao K. Seasonal influenza infection and live vaccine prime for a response to the 2009 pandemic H1N1 vaccine. Proc Natl Acad Sci U S A. 2011;108:1140–1145. doi: 10.1073/pnas.1009908108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Fu TM, Guan L, Friedman A, et al. Dose dependence of CTL precursor frequency induced by a DNA vaccine and correlation with protective immunity against influenza virus challenge. J Immunol. 1999;162:4163–4170. [PubMed] [Google Scholar]
- 104.Laddy DJ, Yan J, Kutzler M, et al. Heterosubtypic protection against pathogenic human and avian influenza viruses via in vivo electroporation of synthetic consensus DNA antigens. PLoS One. 2008;3:e2517. doi: 10.1371/journal.pone.0002517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Holman DH, Wang D, Raja NU, et al. Multi-antigen vaccines based on complex adenovirus vectors induce protective immune responses against H5N1 avian influenza viruses. Vaccine. 2008;26:2627–2639. doi: 10.1016/j.vaccine.2008.02.053. [DOI] [PubMed] [Google Scholar]
- 106.Hemann EA, Kang SM, Legge KL. Protective CD8 T cell-mediated immunity against influenza A virus infection following influenza virus-like particle vaccination. J Immunol. 2013;191:2486–2494. doi: 10.4049/jimmunol.1300954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Carragher DM, Kaminski DA, Moquin A, Hartson L, Randall TD. A novel role for non-neutralizing antibodies against nucleoprotein in facilitating resistance to influenza virus. J Immunol. 2008;181:4168–4176. doi: 10.4049/jimmunol.181.6.4168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Laidlaw BJ, Decman V, Ali MA, et al. Cooperativity between CD8+ T cells, non-neutralizing antibodies, and alveolar macrophages is important for heterosubtypic influenza virus immunity. PLoS Pathog. 2013;9:e1003207. doi: 10.1371/journal.ppat.1003207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Lillie PJ, Berthoud TK, Powell TJ, et al. Preliminary assessment of the efficacy of a T-cell-based influenza vaccine, MVA-NP+M1, in humans. Clin Infect Dis. 2012;55:19–25. doi: 10.1093/cid/cis327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Song JM, Hossain J, Yoo DG, et al. Protective immunity against H5N1 influenza virus by a single dose vaccination with virus-like particles. Virology. 2010;405:165–175. doi: 10.1016/j.virol.2010.05.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Pulendran B, Ahmed R. Translating innate immunity into immunological memory: implications for vaccine development. Cell. 2006;124:849–863. doi: 10.1016/j.cell.2006.02.019. [DOI] [PubMed] [Google Scholar]
- 112.Diebold SS. Recognition of viral single-stranded RNA by Toll-like receptors. Adv Drug Deliv Rev. 2008;60:813–823. doi: 10.1016/j.addr.2007.11.004. [DOI] [PubMed] [Google Scholar]
- 113.Querec T, Bennouna S, Alkan S, et al. Yellow fever vaccine YF-17D activates multiple dendritic cell subsets via TLR2, 7, 8, and 9 to stimulate polyvalent immunity. J Exp Med. 2006;203:413–424. doi: 10.1084/jem.20051720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Gururajan M, Jacob J, Pulendran B. Toll-like receptor expression and responsiveness of distinct murine splenic and mucosal B-cell subsets. PLoS One. 2007;2:e863. doi: 10.1371/journal.pone.0000863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Lin L, Gerth AJ, Peng SL. CpG DNA redirects class-switching towards "Th1-like" Ig isotype production via TLR9 and MyD88. Eur J Immunol. 2004;34:1483–1487. doi: 10.1002/eji.200324736. [DOI] [PubMed] [Google Scholar]
- 116.Akira S, Uematsu S, Takeuchi O. Pathogen recognition and innate immunity. Cell. 2006;124:783–801. doi: 10.1016/j.cell.2006.02.015. [DOI] [PubMed] [Google Scholar]
- 117.Schnare M, Barton GM, Holt AC, Takeda K, Akira S, Medzhitov R. Toll-like receptors control activation of adaptive immune responses. Nat Immunol. 2001;2:947–950. doi: 10.1038/ni712. [DOI] [PubMed] [Google Scholar]
- 118.Kang SM, Yoo DG, Kim MC, et al. MyD88 plays an essential role in inducing B cells capable of differentiating into antibody-secreting cells after vaccination. J Virol. 2011;85:11391–11400. doi: 10.1128/JVI.00080-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Beutler BA. TLRs and innate immunity. Blood. 2009;113:1399–1407. doi: 10.1182/blood-2008-07-019307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Blasius AL, Beutler B. Intracellular toll-like receptors. Immunity. 2010;32:305–315. doi: 10.1016/j.immuni.2010.03.012. [DOI] [PubMed] [Google Scholar]
- 121.Lavelle EC, Murphy C, O'Neill LA, Creagh EM. The role of TLRs, NLRs, and RLRs in mucosal innate immunity and homeostasis. Mucosal Immunol. 2010;3:17–28. doi: 10.1038/mi.2009.124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Cairns B, Maile R, Barnes CM, Frelinger JA, Meyer AA. Increased Toll-like receptor 4 expression on T cells may be a mechanism for enhanced T cell response late after burn injury. J Trauma. 2006;61:293–298. doi: 10.1097/01.ta.0000228969.46633.bb. [DOI] [PubMed] [Google Scholar]
- 123.Geng HL, Lu HQ, Zhang LZ, et al. Increased expression of Toll like receptor 4 on peripheral-blood mononuclear cells in patients with coronary arteriosclerosis disease. Clin Exp Immunol. 2006;143:269–273. doi: 10.1111/j.1365-2249.2005.02982.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Coffman RL, Sher A, Seder RA. Vaccine adjuvants: putting innate immunity to work. Immunity. 2010;33:492–503. doi: 10.1016/j.immuni.2010.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Even-Or O, Samira S, Ellis R, Kedar E, Barenholz Y. Adjuvanted influenza vaccines. Expert Rev Vaccines. 2013;12:1095–1108. doi: 10.1586/14760584.2013.825445. [DOI] [PubMed] [Google Scholar]
- 126.Mbow ML, De Gregorio E, Valiante NM, Rappuoli R. New adjuvants for human vaccines. Curr Opin Immunol. 2010;22:411–416. doi: 10.1016/j.coi.2010.04.004. [DOI] [PubMed] [Google Scholar]
- 127.Eisenbarth SC, Colegio OR, O'Connor W, Sutterwala FS, Flavell RA. Crucial role for the Nalp3 inflammasome in the immunostimulatory properties of aluminium adjuvants. Nature. 2008;453:1122–1126. doi: 10.1038/nature06939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.El Sahly H. MF59™ as a vaccine adjuvant: a review of safety and immunogenicity. Expert Rev Vaccines. 2010;9:1135–1141. doi: 10.1586/erv.10.111. [DOI] [PubMed] [Google Scholar]
- 129.Durando P, Icardi G, Ansaldi F. MF59-adjuvanted vaccine: a safe and useful tool to enhance and broaden protection against seasonal influenza viruses in subjects at risk. Expert Opin Biol Ther. 2010;10:639–651. doi: 10.1517/14712591003724662. [DOI] [PubMed] [Google Scholar]
- 130.O'Hagan DT, Ott GS, De Gregorio E, Seubert A. The mechanism of action of MF59 - an innately attractive adjuvant formulation. Vaccine. 2012;30:4341–4348. doi: 10.1016/j.vaccine.2011.09.061. [DOI] [PubMed] [Google Scholar]
- 131.Seubert A, Monaci E, Pizza M, O'Hagan DT, Wack A. The adjuvants aluminum hydroxide and MF59 induce monocyte and granulocyte chemoattractants and enhance monocyte differentiation toward dendritic cells. J Immunol. 2008;180:5402–5412. doi: 10.4049/jimmunol.180.8.5402. [DOI] [PubMed] [Google Scholar]
- 132.Clark TW, Pareek M, Hoschler K, et al. Trial of 2009 influenza A (H1N1) monovalent MF59-adjuvanted vaccine. N Engl J Med. 2009;361:2424–2435. doi: 10.1056/NEJMoa0907650. [DOI] [PubMed] [Google Scholar]
- 133.Thoelen S, Van Damme P, Mathei C, et al. Safety and immunogenicity of a hepatitis B vaccine formulated with a novel adjuvant system. Vaccine. 1998;16:708–714. doi: 10.1016/s0264-410x(97)00254-5. [DOI] [PubMed] [Google Scholar]
- 134.Harper DM. Currently approved prophylactic HPV vaccines. Expert Rev Vaccines. 2009;8:1663–1679. doi: 10.1586/erv.09.123. [DOI] [PubMed] [Google Scholar]
- 135.Huleatt JW, Jacobs AR, Tang J, et al. Vaccination with recombinant fusion proteins incorporating Toll-like receptor ligands induces rapid cellular and humoral immunity. Vaccine. 2007;25:763–775. doi: 10.1016/j.vaccine.2006.08.013. [DOI] [PubMed] [Google Scholar]
- 136.Ragupathi G, Damani P, Deng K, et al. Preclinical evaluation of the synthetic adjuvant SQS-21 and its constituent isomeric saponins. Vaccine. 2010;28:4260–4267. doi: 10.1016/j.vaccine.2010.04.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Song X, Zang L, Hu S. Amplified immune response by ginsenoside-based nanoparticles (ginsomes) Vaccine. 2009;27:2306–2311. doi: 10.1016/j.vaccine.2009.02.040. [DOI] [PubMed] [Google Scholar]
- 138.Youn HJ, Ko SY, Lee KA, et al. A single intranasal immunization with inactivated influenza virus and alpha-galactosylceramide induces long-term protective immunity without redirecting antigen to the central nervous system. Vaccine. 2007;25:5189–5198. doi: 10.1016/j.vaccine.2007.04.081. [DOI] [PubMed] [Google Scholar]