

Abstract
Vitamin D plays an important role in bone metabolism and maintaining bone health. Recently, new evidence has revealed that vitamin D affects chronic diseases such as autoimmune diseases, cardiovascular diseases and certain cancers. The aim of this study was to evaluate the vitamin D status and the prevalence of vitamin D deficiency in an urban Korean population. This study included 8,976 participants (3,587 men and 5,389 women) aged 50 yr and older. Serum 25(OH)D level was measured by chemiluminescent microparticle immunoassay. The prevalence of vitamin D deficiency [25(OH)D < 20 ng/mL] was 59.7% and 86.5% in men and women, respectively. The prevalence of vitamin D deficiency increased significantly with age in men, but not in women and it decreased from April to July, more prominently in men than in women. These results suggest that sun exposure, intake of vitamin D supplement, and regular physical activities is recommended in an urban Koreans, especially in women.
Keywords: Vitamin D, Deficiency, Prevalence
Vitamin D is important for calcium homeostasis and bone metabolism. It functions as a key regulator of circulating calcium levels by ionized calcium absorption in bone and intestine, and indirectly affects parathyroid hormone (PTH) levels (1). The lack of vitamin D induces secondary hyperparathyroidism, which can cause rickets in children and osteopenia, osteomalacia, osteoporosis and fractures in adults (2, 3). Additionally, new evidence has revealed that vitamin D affects chronic diseases such as autoimmune diseases, cardiovascular diseases, and certain cancers (4).
Vitamin D deficiency affects almost 50% of the population worldwide, is common in Southern Europe, the Middle East, India, China and Japan (3, 5). According to a multinational study involving 18 countries at various latitudes, high prevalence of vitamin D insufficiency, defined as serum 25-hyroxyvitamin D levels < 30 ng/mL, was seen in Korea (92.1%), Japan (90.4%), Lebanon (84.9%), Turkey (76.7%), United Kingdom (74.5%), Germany (68.0%), Mexico (67.1%), and Spain (64.7%) (6). Serum 25(OH)D level was lowest in Korea (17.6 ng/mL). This pandemic of hypovitaminosis D is caused by different exposure to sunshine (latitude, time of day, season, outdoor activities, clothing style, and degree of urbanization), dietary intake of vitamin D and the use of supplements (4, 5, 7).
Although many studies related to vitamin D have been conducted in both young and elderly subjects (5), most studies performed in the Western populations and evidence from the Korean population are limited (8). Therefore, the aim of this study was to evaluate the prevalence and demographic distribution of vitamin D deficiency in middle-aged and older urban Koreans.
The Dong-gu Study is an ongoing prospective population-based study that was designed to investigate the prevalence, incidence, and risk for factors for chronic disease in urban elderly population (9). The Dong-gu Study enrolled 9,260 subjects (3,711 men and 5,549 women) aged 50 yr and older between April and July from 2007 to 2010 in the Dong-gu district of Gwangju Metropolitan City in Korea (35°N). After the exclusion of 228 participants who had incomplete data and 56 participants with estimated glomerular filtration rate (eGFR) values<30 mL/min/1.73 m2, a total of 8,976 subjects (3,587 men and 5,389 women) were included in the present study. All participants provided informed consent, and the study was conducted in accordance with the guidelines in The Declaration of Helsinki. The study was approved by the institutional review board of Chonnam National University Hospital (IRB No. I-2008-05-056).
Anthropometric measurements were made in light clothing and without shoes. Body mass index (BMI) was defined as a ratio of the body weight (kg) to the square of the height (m2). All the participants underwent at least 10 hr of overnight fasting before blood sampling from the antecubital vein. Serum was separated on-site and was stored at -70℃ until analyzed. Concentrations of 25(OH)D were measured by chemiluminescent microparticle immunoassay (ARCHTECT i2000, Abbott, IL, USA). The coefficient of variation for the total analytic precision of this assay was ≤10% for 25(OH)D. The lower detection limits of this assay were 3.0 ng/mL for 25(OH)D. Kidney function was assessed using eGFR, which was calculated using the Modification of Diet in Renal Disease (MDRD) formula (10).
Demographic characteristics were expressed as mean±standard deviation or percentage. Vitamin D deficiency was defined as 25(OH)D levels<20 ng/mL. Results on prevalence are presented by sex, age, and month of blood collection. The test of linear trend and interaction by sex were performed using logistic regression analysis. All the above statistical analysis were based on two-sided probability and a significant level set at P<0.05, were performed using SPSS version 20.0 (SPSS, Chicago, IL, USA).
The mean age of participants was 65 yr, and 40% were men. The mean 25(OH)D levels were 19.2 ng/mL for men and 15.1 ng/mL for women (P<0.001) (Table 1). The prevalence of vitamin D deficiency (<20 ng/mL), insufficiency (20-30 ng/mL) and sufficiency (>30 ng/mL) was 59.7%, 35.3%, and 5.0%, respectively in men, and 86.5%, 12.1%, and 1.3%, respectively in women. Although age was not associated with 25(OH)D levels in both sexes (data not shown), age was linearly associated with the prevalence of vitamin D deficiency in men (P for trend=0.013) (Fig. 1). Serum 25(OH)D concentration increased from 16.9 ng/mL in April to 21.4 ng/mL in July in men, and from 13.7 ng/mL in April to 16.5 ng/mL in July in women (data not shown). The prevalence of vitamin D deficiency decreased from April to July in both genders, but more in men (P=0.001, Fig. 2).
Table 1.
Characteristics of subjects
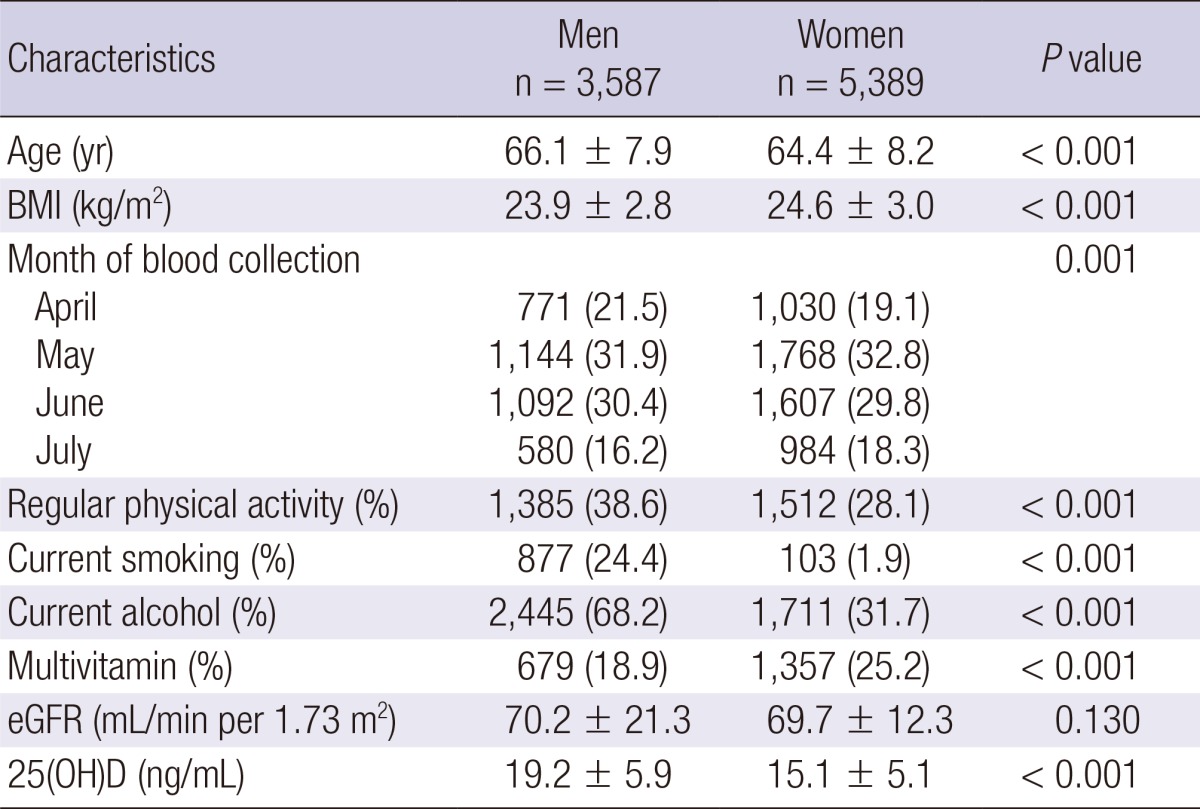
Data are mean±standard deviation, or median (interquartile range), or percentage. BMI, body mass index; eGFR, estimated glomerular filtration rate; 25(OH)D, 25-hydroxylated vitamin D.
Fig. 1.

The prevalence of vitamin D deficiency (25-hydroxyvitamin D < 20 ng/mL) by age groups.
Fig. 2.

The prevalence of vitamin D deficiency (25-hydroxyvitamin D < 20 ng/mL) according to the month of blood collection.
Although the optimal vitamin D levels in the Korean population have not been determined, Hwang et al. (11) suggested that a serum 25(OH)D of 20 ng/mL might be sufficient for bone health in older Korean adults. More than half of present study population showed a 25(OH)D level<20 ng/mL, regardless of the month of blood collection [25(OH)D<20 ng/mL, 75.8%; 25(OH)D<30, 97.7%]. Consistent with our result, Lim et al. (12) reported that the prevalence of vitamin D insufficiency [25(OH)D<30 ng/mL] was 94.0% in 921 subjects aged 65 yr and older. The possible explanations for the high prevalence of vitamin D deficiency in Korea include higher skin pigmentation, less vitamin D fortified foods, cultural habit such as avoiding direct exposure to sunlight, and low vitamin D supplementation compared with Western populations (13).
In present study, vitamin D deficiency was higher in women than in men in all age groups. The sex differences in the prevalence of vitamin D deficiency could be explained by a lack of exposure to sunlight such as more frequent sun protection in women. An interviewer survey of 547 middle-aged and elderly Chinese women reported that many women (62.3%) actively avoid sunlight exposure by staying indoors and using sunscreen products and parasols (14). Another possible explanation might be difference in sun exposure during the course of outdoor physical activity (15). Although the present study did not distinguish outdoor and indoor physical activity, the data of the present study showed that regular physical activity was higher in men than in women. Finally, the excess adiposity of women compared with men has been suggested to contribute to the lower 25(OH)D concentrations in women (16). In the present study, BMI was higher in women than in men, it may have induced the low levels of serum 25(OH)D.
In the present study, the prevalence of vitamin D deficiency increased with aging in men but not women. In general, cutaneous production of vitamin D declines with age. Vitamin D production in 70 yr-old is fourfold less than that in 20 yr-old (17). A global report showed that elderly people usually stay indoors and undertake limited physical activity due to the presence of multiple co-morbidities, further contributing to reducing sun exposure (13). Additionally, Kim et al. (18) reported that older people have higher PTH levels compared with younger people with similar 25(OH)D levels, thus older people require higher 25(OH)D levels to offset age-related compensatory hyperparathyroidism.
Consistent with a Korean study (8), our results showed fluctuation of serum 25(OH)D levels by month of the blood collection in both men and women. These changes were more marked in men than in women (P for interaction=0.001). Seasonal change of serum 25(OH)D levels is caused by the strong dependence on the exposure to sunlight. Above 37° latitude during winter, vitamin D-synthesizing UVB radiation marked decreases on the surface of the earth and therefore during this period vitamin D production in the skin is limited (19). Kull et al. (20) also found a difference in the seasonal variation of 25(OH)D between genders.
The main strength of this study lies in its population-based design and a relatively large sample size, which minimized selection bias and provided sufficient statistical power. However, a number of limitations should also be considered. First, this study used a cross-sectional design. Second, our study had comparably limited ability to explain seasonal change of 25(OH)D in part because of the lack of information on individual sun exposure during four seasons. Third, we performed only a single measurement of serum 25(OH)D level; thus, the data reflect only single point in time rather than long-term exposure. Finally, the participants were not selected randomly from the general population, and so the results may not be representative of the general population of Korea.
In conclusion, vitamin D deficiency was common in urban middle-aged and older Koreans. The seasonal change of serum 25(OH)D was more evident in men than women. These results suggest that sun exposure, intake of vitamin D supplement, and regular physical activities to increase their vitamin D levels is recommeneded in an urban Korean population, especially in women.
Footnotes
There are no conflicts of interest to report.
This study was supported by Research Institute of Medical Sciences, Chonnam National University.
References
- 1.Pilz S, Tomaschitz A, Ritz E, Pieber TR. Vitamin D status and arterial hypertension: a systematic review. Nat Rev Cardiol. 2009;6:621–630. doi: 10.1038/nrcardio.2009.135. [DOI] [PubMed] [Google Scholar]
- 2.Carnevale V, Modoni S, Pileri M, Di Giorgio A, Chiodini I, Minisola S, Vieth R, Scillitani A. Longitudinal evaluation of vitamin D status in healthy subjects from southern Italy: seasonal and gender differences. Osteoporos Int. 2001;12:1026–1030. doi: 10.1007/s001980170012. [DOI] [PubMed] [Google Scholar]
- 3.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–281. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 4.Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80:1678S–1688S. doi: 10.1093/ajcn/80.6.1678S. [DOI] [PubMed] [Google Scholar]
- 5.Lips P. Vitamin D status and nutrition in Europe and Asia. J Steroid Biochem Mol Biol. 2007;103:620–625. doi: 10.1016/j.jsbmb.2006.12.076. [DOI] [PubMed] [Google Scholar]
- 6.Lips P, Hosking D, Lippuner K, Norquist JM, Wehren L, Maalouf G, Ragi-Eis S, Chandler J. The prevalence of vitamin D inadequacy amongst women with osteoporosis: an international epidemiological investigation. J Intern Med. 2006;260:245–254. doi: 10.1111/j.1365-2796.2006.01685.x. [DOI] [PubMed] [Google Scholar]
- 7.Brot C, Vestergaard P, Kolthoff N, Gram J, Hermann AP, Sørensen OH. Vitamin D status and its adequacy in healthy Danish perimenopausal women: relationships to dietary intake, sun exposure and serum parathyroid hormone. Br J Nutr. 2001;86:S97–S103. doi: 10.1079/bjn2001345. [DOI] [PubMed] [Google Scholar]
- 8.Choi EY. 25(OH)D status and demographic and lifestyle determinants of 25(OH)D among Korean adults. Asia Pac J Clin Nutr. 2012;21:526–535. [PubMed] [Google Scholar]
- 9.Kweon SS, Shin MH, Jeong SK, Nam HS, Lee YH, Park KS, Ryu SY, Choi SW, Kim BH, Rhee JA, et al. Cohort profile: the Namwon Study and the Dong-gu Study. Int J Epidemiol. 2013 doi: 10.1093/ije/dys244. doi: 10.1093/ije/dys244. [DOI] [PubMed] [Google Scholar]
- 10.Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation: Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130:461–470. doi: 10.7326/0003-4819-130-6-199903160-00002. [DOI] [PubMed] [Google Scholar]
- 11.Hwang YC, Ahn HY, Jeong IK, Ahn KJ, Chung HY. Optimal serum concentration of 25-hydroxyvitamin D for bone health in older Korean adults. Calcif Tissue Int. 2013;92:68–74. doi: 10.1007/s00223-012-9669-3. [DOI] [PubMed] [Google Scholar]
- 12.Lim S, Shin H, Kim MJ, Ahn HY, Kang SM, Yoon JW, Choi SH, Kim KW, Song JH, Choi SI, et al. Vitamin D inadequacy is associated with significant coronary artery stenosis in a community-based elderly cohort: the Korean Longitudinal Study on Health and Aging. J Clin Endocrinol Metab. 2012;97:169–178. doi: 10.1210/jc.2011-1580. [DOI] [PubMed] [Google Scholar]
- 13.Mithal A, Wahl DA, Bonjour JP, Burckhardt P, Dawson-Hughes B, Eisman JA, El-Hajj Fuleihan G, Josse RG, Lips P, Morales-Torres J. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos Int. 2009;20:1807–1820. doi: 10.1007/s00198-009-0954-6. [DOI] [PubMed] [Google Scholar]
- 14.Kung AW, Lee KK. Knowledge of vitamin D and perceptions and attitudes toward sunlight among Chinese middle-aged and elderly women: a population survey in Hong Kong. BMC Public Health. 2006;6:226. doi: 10.1186/1471-2458-6-226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Scragg R, Camargo CA., Jr Frequency of leisure-time physical activity and serum 25-hydroxyvitamin D levels in the US population: results from the Third National Health and Nutrition Examination Survey. Am J Epidemiol. 2008;168:577–586. doi: 10.1093/aje/kwn163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Van Dam RM, Snijder MB, Dekker JM, Stehouwer CD, Bouter LM, Heine RJ, Lips P. Potentially modifiable determinants of vitamin D status in an older population in the Netherlands: the Hoorn Study. Am J Clin Nutr. 2007;85:755–761. doi: 10.1093/ajcn/85.3.755. [DOI] [PubMed] [Google Scholar]
- 17.MacLaughlin J, Holick MF. Aging decreases the capacity of human skin to produce vitamin D3. J Clin Invest. 1985;76:1536–1538. doi: 10.1172/JCI112134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kim G, Oh KW, Jang EH, Kim MK, Lim DJ, Kwon HS, Baek KH, Yoon KH, Lee WC, Cha BY, et al. Relationship between vitamin D, parathyroid hormone, and bone mineral density in elderly Koreans. J Korean Med Sci. 2012;27:636–643. doi: 10.3346/jkms.2012.27.6.636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Webb AR, Kline L, Holick MF. Influence of season and latitude on the cutaneous synthesis of vitamin D3: exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J Clin Endocrinol Metab. 1988;67:373–378. doi: 10.1210/jcem-67-2-373. [DOI] [PubMed] [Google Scholar]
- 20.Kull M, Jr, Kallikorm R, Tamm A, Lember M. Seasonal variance of 25-(OH) vitamin D in the general population of Estonia, a Northern European country. BMC Public Health. 2009;9:22. doi: 10.1186/1471-2458-9-22. [DOI] [PMC free article] [PubMed] [Google Scholar]