

Abstract
Background
A prospective study of a cohort of nursing staff from nursing homes was undertaken to validate the Nurse-Work Instability Scale (Nurse-WIS). Baseline investigation data was used to test reliability, construct validity and criterion validity.
Method
A survey of nursing staff from nursing homes was conducted using a questionnaire containing the Nurse-WIS along with other survey instruments (including SF-12, WAI, SPE). The self-reported number of days’ sick leave taken and if a pension for reduced work capacity was drawn were recorded. The reliability of the scale was checked by item difficulty (P), item discrimination (rjt) and by internal consistency according to Cronbach’s coefficient. The hypotheses for checking construct validity were tested on the basis of correlations. Pearson’s chi-square was used to test concurrent criterion validity; discriminant validity was tested by means of binary logistic regression.
Results
396 persons answered the questionnaire (21.3% response rate). More than 80% were female and mostly work full-time in a rotating shift pattern. Following the test for item discrimination, two items were removed from the Nurse-WIS test. According to Cronbach’s (0.927) the scale provides a high degree of measuring accuracy. All hypotheses and assumptions used to test validity were confirmed: As the Nurse-WIS risk increases, health-related quality of life, work ability and job satisfaction decline. Depressive symptoms and a poor subjective prognosis of earning capacity are also more frequent. Musculoskeletal disorders and impairments of psychological well-being are more frequent. Age also influences the Nurse-WIS result. While 12.0% of those below the age of 35 had an increased risk, the figure for those aged over 55 was 50%.
Conclusion
This study is the first validation study of the Nurse-WIS to date. The Nurse-WIS shows good reliability, good validity and a good level of measuring accuracy. It appears to be suitable for recording prevention and rehabilitation needs among health care workers. If, in the follow-up, the Nurse-WIS likewise proves to be a reliable screening instrument with good predictive validity, it could ensure that suitable action is taken at an early stage, thereby helping to counteract early retirement and the anticipated shortage of health care workers.
Keywords: Nurse-work instability scale, Nurses, Musculoskeletal disorders
Background
Demographic trends in Germany are expected to lead to a substantial increase in the number of people needing care, and therefore to a requirement for 500,000 additional health care workers [1-4].
Among other things, this means that we need to keep health care workers healthy and motivated to work until retirement age. However, health care work involves considerable strains that can present a challenge, especially for employees over 50 years of age. The literature shows that the work ability of nurses and geriatric nurses declines with increasing age [5] and that cervical spine and lumbar spine problems become more common [6-8]. Moreover, health care workers have an increased risk of developing Musculoskeletal disorders (MSDs) [9-13]. Transferring patients involves moving heavy load weights [14-17]. Additional risk factors are frequent bending and twisting of the torso, along with static body postures [18-20]. The literature shows back problem prevalence rates of 30% to 60% among health care workers [21-23]. Burnout, psychological impairments, low job satisfaction and poor general health are also common in care work [6,24-29].
MSDs and psychiatric disorders such as depression are also the most frequent reasons for long-term sick leave, and employees above the age of 50 are more likely to be affected [30].
Moreover, long-term sick leave due to such disorders is often a transitional stage on the way to reduced work capacity or work disability [31]. In Germany, if a major health impairment makes it no longer possible to work, or possible only to a limited extent, a pension for reduced work capacity is paid. Psychiatric disorders, MSDs and cancer are the most common grounds for payment of a pension for reduced work capacity [32].
Harling et al. [33] ascertained that health care workers more frequently draw a pension for reduced work capacity than other occupational groups. Additionally, MSDs are more often the reason for rehabilitation among health care workers, and after rehabilitation the risk of a pension for reduced work capacity was higher than for other occupational groups.
If the proportion of health care workers drawing a pension for reduced work capacity increases, the strained situation in the geriatric and health care sector could be further aggravated.
In efforts to counteract the forecast shortage of health care workers, maintaining their work ability will be a central concern. Many studies have shown the effectiveness of interventions targeted at individuals with onset symptoms of MSDs [34-36] or individuals who run an increased risk of reduced work ability [37]. Offers of this kind could also be useful for maintaining health care workers’ capacity to work. Until now there has been a lack of effective screening instruments to facilitate the offer of early interventions for health care workers at risk. A new questionnaire that appears to meet these requirements is the Nurse-Work Instability Scale (Nurse-WIS) [38]. Until now, however, the questionnaire was only available in English. It was therefore translated into German and this version of the Nurse-WIS was validated in a prospective study of a cohort of nursing staff from nursing homes. The results of the baseline investigation, which tested reliability, construct validity and criterion validity, are described below.
Methods
The Nurse-Work Instability scale (Nurse-WIS)
The concept of work instability was developed at the University of Leeds and has been defined as follows: “Work Instability (WI) has been defined as a state in which the consequences of a mismatch between an individual’s functional and cognitive abilities and the demands of his or her job can threaten continuing employment if not resolved” [39].
The concept is based on the premise that there is often a period before work disability when there is difficulty in fulfilling work tasks. Interventions at this point in time may prevent the impending loss of work capacity. Consequently, early identification of work instability is the key to preventing long-term sick leave or reduced work capacity. The concept of work instability has already been explored for various clinical fields such as rheumatoid arthritis [39], ankylosing spondylitis (Bechterew’s disease) [40] and for post-traumatic intracranial injuries [41].
The Nurse-WIS is an occupation-specific instrument for recording health care workers who have difficulties in performing their work. It was developed from qualitative interviews with health care workers and it covers all areas that are important to them. Along with musculoskeletal complaints, it records psychosocial factors. The scale comprises 30 items that can be answered by 1 = ‘true’ and 0 = ‘false’. The points for all the answers are added up to calculate the total score. The higher the total score, the higher the risk of work instability. A score of < 10 points signifies a low risk, 10–19 points a moderate risk and a figure of ≥ 20 points an increased risk of work instability [38].
The Nurse-WIS was translated into German with the help of a ‘forward-backward procedure’ [42]. First, the original English version was translated into German. This version was then retranslated into English. A workshop of experts (one occupational health specialist, one epidemiologist, one professor of nursing science, two health care researchers, one psychologist) compared and discussed the original English version, the German version and the retranslated version and reached a verdict by committee assessment. This version was tested in a pre-test with n = 87, with no significant changes occurring.
Study design, recruitment of participants and data protection
In order to test the reliability, validity and forecasting capabilities of the Nurse-WIS, nursing staff from nursing homes took part in a prospective cohort study. The baseline investigation involved surveying the study participants on the basis of a standard questionnaire (end of 2010). The follow-up took place one year later. Using the data obtained from the baseline investigation, we tested the reliability and validity of the Nurse-WIS and the results are described below. The plan is to use data from the follow-up to test the predictive validity of the Nurse-WIS. This data is currently being analysed and prepared for publication.
Study participants were recruited via geriatric nursing homes. The nursing homes were selected by taking a random sample of member companies of our cooperation partner, the German Institution for Statutory Accident Insurance and Prevention in the Health and Welfare Services (BGW). For randomization a random sample of the original list of member companies was drawn with SPSS. The BGW contacted the nursing homes from the random sample by telephone to inform them. Those that agreed to the study were sent the documentation, which they displayed in the workplace for their staff. A total of 83 nursing homes were contacted, of which 29 (34.9%) were willing to take part in the study. Each set of study documents was packed individually in blank form in an A4 envelope. Each envelope contained a letter of information about the study and data protection, a declaration of consent, the questionnaire and a stamped addressed envelope for return. The envelope was addressed to the University Medical Center Hamburg-Eppendorf (UKE), Competence Centre for Epidemiology and Health Services Research in Nursing (CVcare), which undertook the analysis. The health care workers could fill in the study documents either at their workplace or at home before returning them. In this way, the nursing home as employer neither knew which health care workers had taken part in the study, nor saw the documents after they had been filled in. This procedure was developed with the help of the Hamburg Data Protection Commissioner. The study was conducted following the requirements of the Helsinki Declaration and the ethics commission of the Hamburg Medical Association also gave a positive verdict on the conduct of the study (reference number PV3463). A pre-test (with a 37% response rate) was carried out from May to June 2010.
The survey instrument, criteria for inclusion and exclusion
The questionnaire was used to record socio-demographic features (gender, age, country of origin, education) and occupational data (length of service, scope of employment [e.g. full-time], rotating shifts, etc.). Two questions were used to record applications for a pension for reduced work capacity (‘Are you currently thinking about applying for a pension [early retirement pension on health grounds or pension for reduced work capacity]?’ and ‘Have you already applied for a pension?’).
Along with the Nurse-WIS, we used other validated and tested scales, as follows:
•Work Ability Index (WAI) [43,44].
•Short Form Health Survey (SF-12) [45,46].
•Subjective Prognosis of Work Capacity (SPE Scale) [47,48].
•Job satisfaction scale from the German version of the Copenhagen Psychosocial Questionnaire (COPSOQ) [49,50].
•German version of the Center for Epidemiological Studies Depression Scale/CES-D-Scale [51].
We recorded the number of days’ sick leave during the previous 12 months, along with the reason for each period of absence. This information was used to form the following central study variables:
•Total number of days’ sick leave during the previous 12 months.
•Long-term sick leave during the previous 12 months (> 42 days per period of absence).
In Germany, long-term sick leave is taken to mean an absence due to sickness of > 42 days, because after that the payment of salary by the employer is replaced by sick pay from statutory health insurance providers [30].
•Work-related MSD.
There is currently no standard definition of which disorders count as work-related MSD. The literature regards disorders affecting the back and the upper extremity as work-related MSD [52-54].
•Impairments of psychological well-being.
Conditions such as ‘burnout’, ‘total exhaustion’ or ‘depressive malaise’ mentioned by study participants as reasons for sick leave were summarised under this heading.
•Other disorders.
All other disorders, such as acute respiratory infections, gastro-intestinal illnesses, degenerative diseases and injuries were summarised under this heading.
Since the number of days’ sick leave and the reason for each period of absence are central variables for the purpose of analysis, individuals who provided no information on these items were excluded from the study. Persons who were not employed as geriatric care workers (e.g. voluntary helpers) were also excluded.
Testing reliability
We observed the psychometric item difficulty (P), the item discrimination (rjt) and the internal consistency on the basis of Cronbach’s coefficient. P describes the percentage of persons who marked the answer ‘true’ in the Nurse-WIS. Items with an extremely low or high P cannot show up differences between individuals [55]. For example, if 99% (P = 0.99) of all persons marked one Item of the Nurse-WIS with ‘true’, it can be assumed that this item is not adequate. Items with P < 0.1 or P > 0.9 were therefore excluded. In the case of r jt , as high a figure as possible is desirable. Items with negative discrimination are unsuitable for the scale [55,56]. Items with a discrimination r jt < 0.3 were therefore excluded.
The coefficient can take values between minus infinity and 1, with reliabilities between ≥ 0.8 and ≤ 0.9 regarded as being moderate and reliabilities of > 0.9 as high [56].
Testing construct validity
The construct validity of a test, given as a correlation coefficient, reflects the extent to which the construct that is to be measured is related to other variables that it should theoretically be associated with. Correlation coefficients between 0.4 and 0.6 are classified as moderate validity and coefficients of more than 0.6 as high validity [56]. For testing construct validity, we took the total score of the scale as the result of the Nurse-WIS. The hypotheses for testing construct validity are:
•‘With an increased risk according to the Nurse-WIS, health-related quality of life (SF-12) declines’.
•‘With an increased risk according to the Nurse-WIS, the Work Ability Index (WAI) declines’.
•‘With an increased risk according to the Nurse-WIS, job satisfaction (COPSOQ) is low’.
•‘With an increased risk according to the Nurse-WIS, the probability of depressive malaise (ADS) increases’.
•‘With an increased risk according to the Nurse-WIS, capacity to work is subjectively (SPE) assessed as at risk’.
Testing concurrent criterion validity
Criterion validity exists if the result from a scale for measuring a latent variable matches the results for a corresponding manifest criterion [56]. As a manifest criterion we used the variable concerning the existence of certain diseases. The risk categories of the Nurse-WIS were dichotomised so as to produce a new variable with the characteristics ‘low/moderate risk’ and ‘high risk’. We used Pearson’s chi-square to test whether the criteria correlated with the result of the Nurse-WIS. The underlying assumptions and hypotheses for testing concurrent criterion validity are described below.
•Work-related musculoskeletal disorders.
Sick leave in the previous year due to a musculoskeletal disorder is a predictor for long-term sick leave in the subsequent year [30,57]. Persons with an MSD are therefore expected to more frequently show an increased risk according to the Nurse-WIS.
•Psychological impairments to well-being.
Psychosocial factors frequently correlate with the emergence and chronification of musculoskeletal disorders (MSD) [58-61]. MSD are also associated with burnout and depression [61,62]. Impairments of psychological well-being in the previous year are also predictors for long-term sick leave in the subsequent year [30,63]. Persons with impairments of psychological well-being are therefore expected to more frequently indicate an increased risk in accordance with the Nurse-WIS scale.
Testing discriminant criterion validity
Discriminant criterion validity examines if the relationship between the criterion and the result of the scale differs in different populations [56]. Since the frequency of MSD increases with age [30,31], one can assume that MSD are more common among older health care workers. Age could therefore act as a moderating variable. Likewise, gender, educational level, the type of nursing training and length of service could also act as moderating variables. However, if the Nurse-WIS is a suitable instrument, the result of the scale, regardless of said moderating variables, can be expected to correlate with the criteria (musculoskeletal disorder, psychological impairment to well-being) for testing concurrent criterion validity.
Binary logistic regression was used to test the influence of moderating variables. To create a model, we used the ‘stepwise downwards’ methods of Hosmer & Lemeshow [64]. The final model includes the variables that have an influence on the target variable (risk according to the Nurse-WIS).
Findings
Description of the study population
Of 1,816 questionnaires sent to 29 geriatric nursing homes, 396 (21.3%) were returned fully completed by respondents who met the criteria for inclusion. More than 80% of the study participants were female and the majority were aged between 36 and 45 or between 46 and 55. More than half had a secondary school certificate. More than 60% had completed a three-year training course in geriatric care or nursing. As regards length of service, 44.4% of study participants had worked from 0 to 10 years in the health care sector, 30.6% for 11 to 20 years, 14.6% for 21 to 30 years and more than 10% had been health care workers for more than 30 years. The majority of study participants worked full time and most worked in a rotating shift pattern but not at night (Table 1).
Table 1.
Description of the study population
| n = 396 % (n) | |
|---|---|
|
Gender |
|
| Female |
82.6% (327) |
| Male |
17.4% (69) |
|
Age |
|
| 17 to 35 years |
37.9% (150) |
| 36 to 45 years |
26.8% (106) |
| 46 to 55 years |
26.3% (104) |
| Over 55 |
9.1% (36) |
|
Grew up in |
|
| Germany |
86.6% (343) |
| Other countries |
13.4% (53) |
|
Education |
|
| Lower secondary, elementary school certificate |
28.5% (113) |
| Secondary school certificate |
53.3% (211) |
| High school/university entrance certificate |
18.2% (72) |
|
Vocational training |
|
| Qualified geriatric nurse or nurse |
61.9% (245) |
| Geriatric care or nursing assistant |
23.7% (94) |
| Employee without nursing training1 |
14.4% (57) |
|
Length of service |
|
| 0–10 years |
44.4% (176) |
| 11–20 years |
30.6% (121) |
| 21–30 years |
14.6% (58) |
| More than 30 years |
10.4% (41) |
|
Scope of employment |
|
| Full time (≥ 35 hours a week) |
68.9% (273) |
| Part time (15–34 hours a week) |
29.3% (116) |
| Part time (< 15 hours a week) |
1.8% (7) |
|
Working hours |
|
| Rotating shifts excluding nights |
56.6% (224) |
| Rotating shifts including nights |
26.3% (104) |
| Day duty, always at the same times |
9.8% (39) |
| Only night work | 7.3% (29) |
1and trainees, individuals doing civilian national service and persons undertaking a voluntary year of social service.
Sick leave, pensions for reduced work capacity and Nurse-WIS
Around 20% had taken sick leave because of a musculoskeletal disorder (MSD) during the previous 12 months, and 6.3% because of a psychological impairment to well-being. The most common reason (44.9%) for an absence due to sickness was other illnesses (e.g. acute respiratory infection). The percentage that had taken long-term sick leave due to an MSD was 2.5%, while the figure for long-term sick leave due to impairments of psychological well-being was 1.3%. Two individuals (0.5%) said they had applied for early retirement or for a pension for reduced work capacity. The median total score on the Nurse-WIS was 13.1 points. The Nurse-WIS showed 35.1% as having a low risk, 41.2% a moderate risk and 23.7% an increased risk (Table 2).
Table 2.
Sick leave, applications for pensions due to reduced work capacity and results of the Nurse-WIS
| n = 396 % (n) | |
|---|---|
|
Sick leave: |
|
|
Musculoskeletal disorders |
|
| No |
79.5% (315) |
| Yes |
20.5% (81) |
|
Psychological impairments to well-being |
|
| No |
93.7% (371) |
| Yes |
6.3% (25) |
|
Degenerative disease/disease of the lower limbs |
|
| No |
94.2% (373) |
| Yes |
5.8% (23) |
|
Other illnesses |
|
| No |
44.9% (178) |
| Yes |
55.1% (218) |
|
Long-term sick leave (> 42 days): |
|
|
Long-term sick leave because of MSD |
|
| No |
97.5% (386) |
| Yes |
2.5% (10) |
|
Long-term sick leave because of impairments of psychological well-being |
|
| No |
98.7% (391) |
| Yes |
1.3% (5) |
|
Pensions for reduced work capacity: |
|
|
Application for pension for reduced work capacity |
|
| No |
99.5% (394) |
| Yes |
0.5% (2) |
|
Nurse-WIS | |
|
Total score |
|
| Median (IQR) |
13.1 pts (12.0 pts) |
| Minimum/maximum |
0.0 pts/28.0 pts |
|
Risk categories |
% (n) |
| Low risk (< 10 points) |
35.1% (139) |
| Moderate risk (10–19 points) |
41.2% (163) |
| Increased risk (≥ 20 points) | 23.7% (94) |
IQR = interquartile range.
Reliability of the Nurse-WIS
The difficulty index for all items is within an acceptable range. In the case of item discrimination, a coefficient of r jt < 3 is stated for two items. These items are therefore not suitable for recording the risk of work instability in accordance with the Nurse-WIS and were excluded from the analysis. The total score of the Nurse-WIS was calculated on the basis of the remaining 28 items. Cronbach’s coefficient is 0.927. Consequently, the scale with 28 items is highly reliable (no table).
Construct validity of the Nurse-WIS
All hypotheses for testing construct validity can be confirmed (Figure 1). The physical health (PHS) and the mental health subscale (MHS) of the SF-12 showed significant negative correlations with Nurse-WIS. Since the coefficient reflects the degree to which such relationships exist, the coefficient of the PHS (r = −0.668) indicates good validity and the MHS (r = −0.435) at least moderate validity. As regards the Work Ability Index (WAI) and job satisfaction (COPSOQ), there are significant correlations that suggest high construct validity. As the risk according to the Nurse-WIS increases, work ability (r = −0.672) and job satisfaction (r = −0.615) decline. The likelihood of depressive symptoms (r = 0.601) increases, so high validity is achieved here, too. As the risk according to the Nurse-WIS increases, the subjective prognosis of work capacity (SPE) deteriorates. Here, with r = 0.534, moderate validity is achieved.
Figure 1.
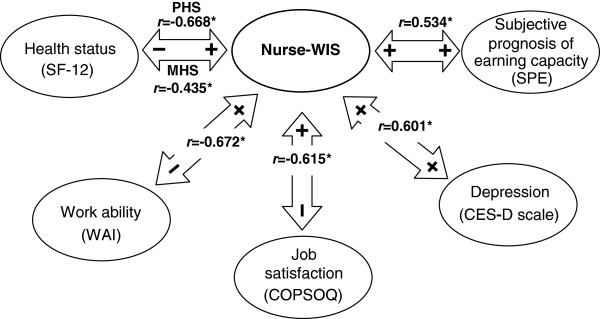
Diagram showing correlations for testing construct validity (n = 396).r = Spearman correlation PHS = Physical Health Subscale MHS = Mental Health Subscale *This correlation is significant at the 0.001 level (bilateral).
Concurrent and discriminant criterion validity
The assumptions and hypotheses for testing concurrent validity can be confirmed (Table 3). Persons with an musculoskeletal disorder (MSD) more frequently run an increased risk according to the Nurse-WIS (40.7%) than persons without an MSD (19.4%). Likewise, persons affected by a psychological impairment to well-being more often have an increased risk (44.0% versus 22.4%) according to the Nurse-WIS. As expected, no correlations appear between the risk according to the Nurse-WIS and degenerative diseases/diseases of the lower limbs or other illnesses (e.g. acute respiratory illnesses). However, there are significant differences in the case of age and length of service. Of the study participants aged between 17 and 35, 12.0% have an increased risk, while at the age of 36 to 45 and 46 to 55 the figure is around 27%, and in those over 55 years old it is 50.0%. Moreover, the proportion of persons with an increased risk according to the Nurse-WIS rises significantly with length of service. In the final binary logistic regression model, the age variable was still included and so age has an influence on risk according to the Nurse-WIS. Accordingly, study participants in the 36–45 age group (OR 2.9; 95% CI 1.47–5.63) and the 46–55 age group (OR 2.5; 95% CI 1.27–4.90) are around three times more likely to have an increased risk according to the Nurse-WIS than those aged under 35. In the case of those over the age of 55, the likelihood of having an increased risk is around seven times higher (OR 6.7; 96% CI 2.88–15.54). After controlling for age, the length of service no longer has any influence. However, the final model also includes the test criteria for criterion validity. Persons with MSD (OR 2.7; 95% CI 1.59–4.89) and those with a psychological impairment to well-being (OR 2.9; 95% CI 1.24–6.92) are around three times more likely to have an increased risk according to the Nurse-WIS.
Table 3.
Distribution of the study population among Nurse-WIS risk categories and results of the final logistic regression model for testing discriminant validity
|
Variables |
Nurse-WIS |
|||
|---|---|---|---|---|
|
Low/moderate risk |
Heightened risk |
p value* |
Final model OR (95% CI) |
|
|
76.3% |
23.7% |
|
|
|
| (n = 302) | (n = 94) | |||
|
Gender | ||||
| Female |
74.6% (244) |
25.4% (83) |
|
|
| Male |
84.1% (58) |
15.9% (11) |
0.094 |
- |
|
Age | ||||
| ≤ 35 years |
88.0% (132) |
12.0% (18) |
|
1 |
| 36 to 45 years |
72.6% (77) |
27.4% (29) |
|
2.9 (1.47–5.63) |
| 46 to 55 years |
72.1% (75) |
27.9% (29) |
|
2.5 (1.27–4.90) |
| > 55 years |
50.0% (18) |
50.0% (18) |
<0.001 |
6.7 (2.88–15.54) |
|
Grew up in | ||||
| Germany |
77.3% (265) |
22.7% (78) |
|
|
| Other countries |
69.8% (37) |
30.2% (16) |
0.236 |
- |
|
Education | ||||
| Lower secondary, elementary school certificate |
72.6% (82) |
27.4% (31) |
|
|
| Secondary school certificate |
78.7% (166) |
21.3% (45) |
|
|
| High school/university entrance certificate |
75.0% (54) |
25.0% (18) |
0.451 |
- |
|
Vocational training | ||||
| Qualified geriatric nurse or nurse |
74.3% (182) |
25.7% (63) |
|
|
| Geriatric care or nursing assistant |
75.5% (71) |
24.5% (23) |
|
|
| Employee without nursing training1 |
86.0% (49) |
14.0% (8) |
0.172 |
|
|
Length of service | ||||
| 0–10 years |
84.7% (149) |
15.3% (27) |
|
|
| 11–20 years |
71.9% (87) |
28.1% (34) |
|
|
| 21–30 years |
67.2% (39) |
32.8% (19) |
|
|
| More than 30 years |
65.9% (27) |
34.1% (14) |
0.004 |
- |
|
Scope of employment | ||||
| Full time (≥ 35 hours a week) |
77.7% (212) |
22.3% (61) |
|
|
| Part time (15–34 hours a week |
72.4% (84) |
27.6% (32) |
|
|
| Part time (< 15 hours a week) |
85.7% (6) |
14.3% (1) |
0.452 |
- |
|
Working hours | ||||
| Rotating shifts excluding nights |
77.2% (173) |
22.8% (51) |
|
|
| Rotating shifts including nights |
72.1% (75) |
27.9% (29) |
|
|
| Day duty, always at the same times |
79.5% (31) |
20.5% (8) |
|
|
| Only night work |
79.3% (23) |
20.7% (6) |
0.688 |
- |
|
Musculoskeletal disorders | ||||
| No |
80.6% (254) |
19.4% (61) |
|
1 |
| Yes |
59.3% (48) |
40.7% (33) |
<0.001 |
2.7 (1.59–4.89) |
|
Psychological impairments to well-being | ||||
| No |
77.6% (288) |
22.4% (83) |
|
1 |
| Yes |
56.0% (14) |
44.0% (11) |
<0.001 |
2.9 (1.24–6.92) |
|
Degenerative disease/disease of the lower limbs | ||||
| No |
76.9% (287) |
23.6% (88) |
|
|
| Yes |
73.9% (17) |
26.1% (6) |
0.738 |
- |
|
Other illnesses | ||||
| No |
75.9% (167) |
24.1% (53) |
|
|
| Yes | 77.8% (137) | 22.2% (39) | 0.651 | - |
1and trainees, individuals doing civilian national service and persons undertaking a voluntary year of social service.
*Pearson’s chi-square.
OR = Odds Ratio.
95% CI = 95% confidence interval.
Discussion
This is the first study to have translated the original English version of the Nurse-WIS and to have validated this version. The psychometric characteristics of the Nurse-WIS were tested for a collective of 396 nursing staff from nursing homes. Reliability and validity were tested by various methods, and initially all items achieved acceptable degrees of difficulty. However, according to the item discrimination two items were unsuitable, so the German version of the scale comprises a total of 28 items. According to Cronbach’s, good measuring accuracy is achieved for the scale of 28 items. That means that the items on the scale are suitable for recording the construct.
In the study by Gilworth et al. [38], it was also shown that the English version of the Nurse-WIS has good face validity for registered nurses and health care assistants, and meets the measurement requirements as defined by modern psychometric theory.
Since the German version of the scale corresponds to the hypotheses formed from theory and empirical research, a high degree of construct validity can be assumed. As the risk according to the Nurse-WIS increases, health-related quality of life, the ability to work and job satisfaction decline. Simultaneously, the probability of depressive symptoms increases and the subjective prognosis of work capacity deteriorates. There are good values for concurrent criterion validity, too, since persons with a increased risk according to the Nurse-WIS more often have a musculoskeletal disorder (MSD) or a psychological impairment to well-being. The scale therefore records what it is meant to record. However, in addition to this correlation, age is an influencing factor. Older persons are more likely to have an increased risk according to the Nurse-WIS. 12.0% of those under 35 have an increased risk, while the figure for those aged over 55 is 50%. This relationship seems plausible since the Nurse-WIS is designed to record work instability primarily due to symptoms of an MSD, and MSDs occur more frequently with advancing age [7,8,65-68]. A study by Kromark et al. [6] likewise showed that, at 56%, the prevalence of back complaints among health care workers aged over 50 is higher than among their younger colleagues (37%). It was also found that with increasing age, the work capacity of health care and geriatric care workers declines [5,6]. Moreover, the Nurse-WIS remains within the final binary logistic regression model, i.e. regardless of age, the Nurse-WIS shows a strong correlation with the presence of an MSD or a psychological impairment to well-being.
In order to ascertain the validity of the original English version of the Nurse-WIS, Gilworth et al. [38] arranged for some of the study participants (n = 27) to be examined individually by an occupational therapist. The occupational therapist used a standard procedure for ascertaining the status of work instability and the result was compared to the result of the Nurse-WIS. The Nurse-WIS was found to have 75% sensitivity and 100% specificity. In the present study, no values for sensitivity and specificity have been ascertained so far, as this is to be done with the help of data from the follow-up survey. The data on sick leave was taken from the questionnaire as stated by the study participants themselves. An individual assessment of a study participant by an occupational therapist, as used by Gilworth et al. [38] may be more reliable. However, Gilworth et al. [38] did not examine whether there was actually an absence due to sickness, long-term sick leave or a pension for reduced work capacity at a later date. Therefore, there was no prospective study. This prospective study was carried out for the first time in the follow-up study of the cohort of nursing staff from nursing homes presented here. The data from this survey is currently being analysed and prepared for publication.
Using the Nurse-WIS to maintain the work ability of health care workers
The Nurse-WIS seems suitable for identifying health care workers at risk and for designing offers of prevention efficiently so as to maintain the work ability of health care staff. The proportion of health care workers with an increased risk according to the Nurse-WIS was 23.7%. This proportion, with a conspicuous result on the Nurse-WIS, appears relatively high.
Other studies have not so far examined work instability among health care workers. Taking the 30%–60% prevalence of back complaints among staff [21-23] as a comparison, the proportion of health care workers with an increased risk according to the Nurse-WIS does seem plausible, however.
Nonetheless, considering that according to the Nurse-WIS result one would like to facilitate preventive action for one in two health care workers aged over 55, the proportion of 50% seems very high. Consequently, before the Nurse-WIS can be used as an instrument for managing health promotion, prevention or rehabilitation measures, the predictive values of the scale as well as its sensitivity and specificity should be ascertained.
Special features of the study design and representativeness of the sample
Study participants were recruited via geriatric nursing homes. The study documents and questionnaire were displayed for nursing staff at their workplace. So that a sufficient number of study documents were sent to the homes, they informed us of the number of health care workers employed. The response rate was 23.1%. However, we suspect that some nursing homes ordered more questionnaires than were actually needed. A number of homes gave an estimated, rounded figure of the number of study documents needed (e.g. ‘Send us about 100 questionnaires’) since the care managers in charge are often unable to say off the cuff the exact number of health care workers currently employed. Often, they gave the total number of employees (including domestic workers, cleaners, etc.). It is also likely that not all the health care workers employed were present (e.g. due to sickness, holidays, pregnancy, parental leave) when the study documents were displayed, although they remained on display for several weeks. Consequently, the response rate should be regarded as an approximate figure and can be assumed to be somewhat underestimated.
However, because of the low response rate one might think there are alternative methods to assess data from nursing staff working in geriatric nursing homes, for example telephone or face-to-face interviews or electronic questionnaires (e.g. via email or website). We considered that telephone or face-to-face interviews would not be possible, because nursing staff in nursing homes will not have the time during their shift to answer the questions on the telephone or personally. And since there is no nurses association in Germany, which could have given support to announce the study and to provide an electronic questionnaire on a website, we decided to choose the option of paper questionnaires.
The proportion of health care workers with an increased risk according to the Nurse-WIS was 23.7%. Under the focus of the low response rate this proportion appears relatively high and one can assume that there is the possibility of a selective sample. But with more than 80% of female study participants the sex distribution, just as the age distribution in the present study is comparable with the distribution in geriatric care in Germany [69].
Approximately 20% said they had taken sick leave in the previous 12 months because of a musculoskeletal disorder (MSD). Furthermore, MSDs (following other illnesses such as acute respiratory or gastro-intestinal illnesses) were the most frequent reason for absence due to sickness. Some studies have found a somewhat higher prevalence rate (30% to 60%) of lower back problems among health care workers [19,22,23,70]. However, these studies do not record sick leave due to MSDs, but only MSD symptoms such as back pain or neck pain. Pain, however, does not necessarily lead to health care workers staying away from work and therefore being on sick leave. Some of these prevalence rates were also ascertained during other observation periods. In Videman et al. [23], for example, participants were studied over a period of five years. Back pain is likely to occur more often during a period of five years than during a 12-month observation period.
The rate of impairments of psychological well-being was approximately 6%. The literature also makes it clear that health care workers are affected by burnout and psychological impairments [24-29,71]. However, due to different conceptualisations of burnout and the absence of standard survey instruments in the studies, it is not yet possible to make a precise statement about the prevalence of burnout in geriatric care [71].
The overall conclusion is that the sample in the present study is comparable with other studies and that one can therefore assume a good degree of representativeness.
Summing up, one can say that the Nurse-WIS has shown itself to be a promising instrument with good psychometric properties. So far, the Nurse-WIS has been tested on a sample of nurses for the elderly in nursing homes, but the extent to which the Nurse-WIS is generally applicable requires further testing, for example among registered nurses or health care workers in hospitals or in outpatient care. There are other more general scales (e.g. WAI, SF-12) with good psychometric properties, but these scales often focus on health-related quality of life or on disability and function. Currently, as far as we are aware, the Nurse-WIS is the first occupation-specific scale to focus on health care workers experiencing work instability. And since there is evidence that early intervention is more effective, the identification of work instability in health care workers might be very helpful for ensuring that they have rapid access to these intervenient measures.
Conclusion
The Nurse-WIS shows good reliability and validity, and one can assume good measuring accuracy. It therefore seems suitable for recording work instability. Moreover, the Nurse-WIS is a short, easy-to-use and low-cost instrument that seems suitable for practical use and for application in research and evaluation.
The background to the present study is the central task of countering the anticipated shortage of health care workers as the result of demographic change. Research, too, has confirmed that early prevention and health-promotion measures are effective in preventing the chronification of diseases and premature retirement [34-37,72]. Until now, however, there has been a lack of screening instruments for identifying health care workers at risk and for offering efficient and targeted prevention measures. That is why we validated the Nurse-Work Instability Scale (Nurse-WIS). This study, along with the study on the development of the Nurse-WIS [38], is the only validation study to date. However, the findings of the follow-up study are still pending. If the follow-up should also show the Nurse-WIS to be a reliable screening instrument with good predictive validity, the Nurse-WIS could help in taking early, targeted, suitable action to prevent or minimize sickness absence and potentially prevent loss of health care workers from the workforce through long-term sickness absence and early retirement.
Abbreviations
Nurse-WIS: Nurse-work instability scale; MSD: Musculoskeletal disorders; WAI: Work ability index; SF-12: Short form health survey; SPE Scale: Subjective prognosis of work capacity; COPSOQ: Job satisfaction scale from the German version of the Copenhagen Psychosocial Questionnaire; CES-D-Scale: German version of the Center for Epidemiological Studies Depression Scale; BGW: German Institution for Statutory Accident Insurance and Prevention in the Health and Welfare Services; CVcare: Competence Centre for Epidemiology and Health Services Research in Nursing.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AB helped to develop the Questionnaire and participated in the Data collection. MH participated in the design of the study, performed the statistical analysis and drafted the manuscript. AN conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Contributor Information
Melanie Harling, Email: m.harling@uke.de.
Anja Schablon, Email: a.schablon@uke.de.
Albert Nienhaus, Email: a.nienhaus@uke.de.
References
- Brambrink M, Rieger M, Heine U. Strategisches controlling zur berücksichtigung des soziodemographischen wandels in einem sozialmedizinischen dienst. Das Gesund. 2005;8:117–119. doi: 10.1055/s-2005-857893. [DOI] [PubMed] [Google Scholar]
- Bickel H. Life expectancy and the need for nursing care in Germany. Das Gesund. 2001;8:9–14. doi: 10.1055/s-2001-10454. [DOI] [PubMed] [Google Scholar]
- Dietz B. Entwicklung des Pflegebedarfs bis 2050: Kosten steigen schneller als erwartet. Soziale Sicherheit. 2001;8:2–9. [Google Scholar]
- Statistische Ämter des Bundes und der Länder. Demografischer Wandel in Deutschland. Heft 2. Auswirkungen auf Krankenhausbehandlungen und Pflegebedürftige im Bund und in den Ländern. Wiesbaden: Statistisches Bundesamt; 2010. [Google Scholar]
- Camerino D, Conway PM, Van der Heijden BI, Estryn-Behar M, Consonni D, Gould D, Hasselhorn HM. Low-perceived work ability, ageing and intention to leave nursing: a comparison among 10 European countries. J Adv Nurs. 2006;8:542–552. doi: 10.1111/j.1365-2648.2006.04046.x. [DOI] [PubMed] [Google Scholar]
- Kromark K, Dulon M, Nienhaus A. Gesundheitsindikatoren und Präventionsverhalten bei älteren Beschäftigten in der Altenpflege. Das Gesund. 2008;8:137–144. doi: 10.1055/s-2008-1062730. [DOI] [PubMed] [Google Scholar]
- Engels JA, van der Gulden JWJ, Senden TF, Van‘t Hof B. Work related risk factors for muskulosceletal complaints in the nursing profession: results of a questionnaire survey. Occu and envi med. 1996;8:636–641. doi: 10.1136/oem.53.9.636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Josephson M, Hagberg M, Hjelm EW. Self-reported physical exertion in geriatric care. A risk indicator for low back symptoms? Spine. 1996;8:2781–2785. doi: 10.1097/00007632-199612010-00014. [DOI] [PubMed] [Google Scholar]
- Caruso CC, Waters TR. A review of work schedule issues and musculoskeletal disorders with an emphasis on the healthcare sector. Ind health. 2008;8:523–534. doi: 10.2486/indhealth.46.523. [DOI] [PubMed] [Google Scholar]
- Lipscomb JA, Trinkoff AM, Geiger-Brown J, Brady B. Work-schedule characteristics and reported musculoskeletal disorders of registered nurses. Scand.J Work Environ.Health. 2002;8:394–401. doi: 10.5271/sjweh.691. [DOI] [PubMed] [Google Scholar]
- Ando S, Ono Y, Shimaoka M, Hiruta S, Hattori Y, Hori F, Takeuchi Y. Associations of self estimated workloads with musculoskeletal symptoms among hospital nurses. Occupational and environmental medicine. 2000;8:211–216. doi: 10.1136/oem.57.3.211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann F, Stossel U, Michaelis M, Nübling M, Siegel A. Low back pain and lumbago-sciatica in nurses and a reference group of clerks: results of a comparative prevalence study in Germany. Int Arch Occup Environ Health. 2002;8:484–490. doi: 10.1007/s00420-002-0332-6. [DOI] [PubMed] [Google Scholar]
- Menzel NN. Back pain prevalence in nursing personnel: measurement issues. AAOHN J. 2004;8:54–65. [PubMed] [Google Scholar]
- Marras WS, Davis KG, Kirking BC, Bertsche PK. A comprehensive analysis of low-back disorder risk and spinal loading during the transferring and repositioning of patients using different techniques. Ergonomics. 1999;8:904–926. doi: 10.1080/001401399185207. [DOI] [PubMed] [Google Scholar]
- Engkvist IL, Hjelm EW, Hagberg M, Menckel E, Ekenvall L. Risk indicators for reported over-exertion back injuries among female nursing personnel. Epidemiology. 2000;8:519–522. doi: 10.1097/00001648-200009000-00006. [DOI] [PubMed] [Google Scholar]
- Byrns G, Reeder G, Jin G, Pachis K. Risk factors for work-related low back pain in registered nurses, and potential obstacles in using mechanical lifting devices. J Occup Environ Hyg. 2004;8:11–21. doi: 10.1080/15459620490249992. [DOI] [PubMed] [Google Scholar]
- Jäger M, Jordan C, Theilmeier A, Wortmann N, Kuhn S, Nienhaus A, Luttmann A. Lumbar-load analysis of manual patient-handling activities for biomechanical overload prevention among healthcare workers. Ann Occup Hyg. 2013;8(Suppl 4):528–544. doi: 10.1093/annhyg/mes088. [DOI] [PubMed] [Google Scholar]
- Estryn-Behar M, Kaminski M, Peigne E, Maillard MF, Pelletier A, Berthier C, Delaporte MF, Paoli MC, Leroux JM. Strenuous working conditions and musculo-skeletal disorders among female hospital workers. Int Arch Occup Environ Health. 1990;8:47–57. doi: 10.1007/BF00397848. [DOI] [PubMed] [Google Scholar]
- Knibbe JJ, Friele RD. Prevalence of back pain and characteristics of the physical workload of community nurses. Ergonomics. 1996;8:186–198. doi: 10.1080/00140139608964450. [DOI] [PubMed] [Google Scholar]
- Freitag S, Fincke-Junos I, Nienhaus A. In: Gefährdungsprofile - Unfälle und arbeitsbedingte Erkrankungen in Gesundheitsdienst und Wohlfahrtspflege, 2. Nienhaus A, editor. Landsberg: ecomed; 2010. Messtechnische Analyse von belastenden Körperhaltungen bei Pflegekräften - Vergleich zwischen einer geriatrischen Station und anderen Krankenhausstationen; pp. 160–179. [Google Scholar]
- Lagerström M, Hansson T, Hagberg M. Work-related low-back problems in nursing. Scand J Work Environ Health. 1998;8:449–464. doi: 10.5271/sjweh.369. [DOI] [PubMed] [Google Scholar]
- Nelson A, Fragala G, Menzel N. Myths and facts about back injuries in nursing. Am J Nurs. 2003;8:32–40. doi: 10.1097/00000446-200302000-00021. [DOI] [PubMed] [Google Scholar]
- Videman T, Ojajarvi A, Riihimaki H, Troup JD. Low back pain among nurses: a follow-up beginning at entry to the nursing school. Spine. 2005;8:2334–2341. doi: 10.1097/01.brs.0000182107.14355.ca. [DOI] [PubMed] [Google Scholar]
- Zimber A. Beanspruchung und Stress in der Altenpflege: Forschungsstand und Forschungsperspektiven. Z Gerontol Geriatr. 1998;8:417–425. doi: 10.1007/s003910050069. [DOI] [PubMed] [Google Scholar]
- Zimber A, Albrecht A, Weyerer S. Die Beanspruchung in der stationären Altenpflege. Pflege aktuell. 2000;8:272–275. [PubMed] [Google Scholar]
- Siegrist J, Rödel A. In: Machbarkeitsstudie - Gesunder Wiedereinstieg in den Altenpflegeberuf. Kowalski J, Pauli G, editor. Köln: Institut für Betriebliche Gesundheitsförderung BGF GmbH; 2005. Arbeitsbelastungen im Altenpflegeberuf unter besonderer Berücksichtigung der Wiedereinstiegsproblematik - Zusammenfassung der Ergebnisse der Literaturrecherche und bibliographische Hinweise; pp. 1–36. [Google Scholar]
- Glaser J, Richter G, Lampert B, Weigl M. In: Arbeitsschutz, Gesundheit und Wirtschaftlichkeit 14. Workshop 2007. Bärenz P, Metz AM, Rothe HJ, editor. Kröning: Asanger Verlag; 2007. Belastungsscreening bei Altenpflegekräften; pp. 369–372. [Google Scholar]
- Garrett C. The effect of nurse staffing patterns on medical errors and nurse burnout. AORN journal. 2008;8:1191–1204. doi: 10.1016/j.aorn.2008.01.022. [DOI] [PubMed] [Google Scholar]
- McHugh MD, Kutney-Lee A, Cimiotti JP, Sloane DM, Aiken LH. Nurses’ widespread job dissatisfaction, burnout, and frustration with health benefits signal problems for patient care. Health Aff.(Millwood.) 2011;8:202–210. doi: 10.1377/hlthaff.2010.0100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bödeker W, Zelen K. Frühindikatoren für Langzeit-Arbeitsunfähigkeit. Entwicklung eines Vorhersageinstruments für die Praxis in Betrieben und Krankenkassen. Iga Report 14. AOK-Bundesverband GbR: BKK Bundesverband GbR, BGAG Institut Arbeit und Gesundheit der Deutschen Gesetzlichen Unfallversicherung; 2008. [Google Scholar]
- Gjesdal S, Bratberg E. The role of gender in long-term sickness absence and transition to permanent disability benefits. Results from a multiregister based, prospective study in Norway 1990–1995. Eur J Public Health. 2002;8:180–186. doi: 10.1093/eurpub/12.3.180. [DOI] [PubMed] [Google Scholar]
- Rehfeld UG. Gesundheitsbedingte Frühberentung. Gesundheitsberichtserstattung des Bundes. Heft 30. Berlin: Robert Koch Institut; 2006. [Google Scholar]
- Harling M, Schablon A, Nienhaus A. In: Gesundheit, Migration und Einkommensgleichheit. Deutsche Rentenversicherung B, editor. Berlin: Bericht vom siebten Workshop des Forschungsdatenzentrums der Rentenversicherung (FDZ-RV) im Wissenschaftszentrum Berlin für Sozialforschung (WZB) - Band 55/2010; 2010. Abgeschlossene medizinische Rehabilitationen und Erwerbsminderungsrenten bei Pflegepersonal im Vergleich zu anderen Berufsgruppen; pp. 72–85. [Google Scholar]
- Linton SJ, Andersson T. Can chronic disability be prevented? A randomized trial of a cognitive-behavior intervention and two forms of information for patients with spinal pain. Spine. 2000;8:2825–2831. doi: 10.1097/00007632-200011010-00017. [DOI] [PubMed] [Google Scholar]
- Linton SJ, Nordin E. A 5-year follow-up evaluation of the health and economic consequences of an early cognitive behavioral intervention for back pain: a randomized, controlled trial. Spine. 2006;8:853–858. doi: 10.1097/01.brs.0000209258.42037.02. [DOI] [PubMed] [Google Scholar]
- Van Oostrom SH, Driessen MT, De Vet HC, Franche RL, Schonstein E, Loisel P, Van Mechelen W, Anema JR. Workplace interventions for preventing work disability. Cochrane Database Syst Rev. 2009;8(2):CD006955. doi: 10.1002/14651858.CD006955.pub2. [DOI] [PubMed] [Google Scholar]
- de Boer AG, van Beek JC, Durinck J, Verbeek JH, van Dijk FJ. An occupational health intervention programme for workers at risk for early retirement; a randomised controlled trial. Occup Environ Med. 2004;8:924–929. doi: 10.1136/oem.2003.009746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilworth G, Bhakta B, Eyres S, Carey A, Chamberlain AM, Tennant A. Keeping nurses working: development and psychometric testing of the Nurse-Work Instability Scale (Nurse-WIS) J Adv Nurs. 2007;8:543–551. doi: 10.1111/j.1365-2648.2006.04142.x. [DOI] [PubMed] [Google Scholar]
- Gilworth G, Chamberlain MA, Harvey A, Woodhouse A, Smith J, Smyth MG, Tennant A. Development of a work instability scale for rheumatoid arthritis. Arthritis Rheum. 2003;8:349–354. doi: 10.1002/art.11114. [DOI] [PubMed] [Google Scholar]
- Gilworth G, Emery P, Barkham N, Smyth MG, Helliwell P, Tennant A. Reducing work disability in Ankylosing Spondylitis: development of a work instability scale for AS. BMC Musculoskelet Disord. 2009;8:68. doi: 10.1186/1471-2474-10-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilworth G, Carey A, Eyres S, Sloan J, Rainford B, Bodenham D, Neumann V, Tennant A. Screening for job loss: development of a work instability scale for traumatic brain injury. Brain Inj. 2006;8:835–843. doi: 10.1080/02699050600832221. [DOI] [PubMed] [Google Scholar]
- Harkness JA, Schoua-Glusberg A. In: Cross-Cultural Survey Equivalence. Harkness JA, editor. Mannheim: ZUMA; 1998. Questionnaires in Translation; pp. 87–126. [Google Scholar]
- Ilmarinen J, Tuomi K. In: Past present and Future of Work Ability - People and Work Research Report 65. Ilmarinen J, Lehtinen S, editor. Helsinki: Finnish Institute of Occupational Health; 2004. Past, present and future of work ability; pp. 1–25. [Google Scholar]
- Hasselhorn HM, Freude G. Der Work Ability Index - ein Leitfaden. Wirtschaftsverlag NW Verlag für neue Wissenschaft GmbH: Dortmund, Berlin, Dresden; 2007. [Google Scholar]
- Bullinger M, Kichberger I. SF 36 - Fragebogen zum Gesundheitszustand. Handbuch für die deutschsprachige Fragebogenversion. Göttingen: Hogrefe; 1998. [Google Scholar]
- Bullinger M, Morfeld M, Kohlmann T, Nantke J, van den Bussche H, Dodt B, Dunkelberg S, Kirchberger I, Krüger-Bödecker A, Lachmann A, Lang K, Mathis C, Mittag O, Peters A, Raspe HH, Schulz H. SF-36 health survey in rehabilitation research. Findings from the North German network for rehabilitation research, NVRF, within the rehabilitation research funding program. Rehabilitation. 2003;8:218–225. doi: 10.1055/s-2003-41645. [DOI] [PubMed] [Google Scholar]
- Mittag O, Raspe H. A brief scale for measuring subjective prognosis of gainful employment: findings of a study of 4279 statutory pension insurees concerning reliability (Guttman scaling) and validity of the scale. Rehabilitation. 2003;8:169–174. doi: 10.1055/s-2003-40095. [DOI] [PubMed] [Google Scholar]
- Mittag O, Meyer T, Glaser-Moller N, Matthis C, Raspe H. Predicting gainful employment in a population sample of 4225 statutory pension insurance members covering a prognostic period of five years using a brief subjective prognostic employment scale (SPE Scale) Das Gesundheitswesen. 2006;8:294–302. doi: 10.1055/s-2006-926781. [DOI] [PubMed] [Google Scholar]
- Nübling M, Stößel U, Hasselhorn HM, Michaelis M, Hofmann F. Methoden zur Erfassung psychischer Belastungen - Erprobung eines Messinstrumentes (COPSOQ) Dortmund, Berlin, Dresden: Wirtschaftsverlag NW, Verlag für neue Wissenschaften; 2005. [Google Scholar]
- Nübling M, Stössel U, Hasselhorn HM, Michaelis M, Hofmann F. Measuring psychological stress and strain at work - Evaluation of the COPSOQ Questionnaire in Germany. Psychosoc. Med. 2006;8:Doc05. [PMC free article] [PubMed] [Google Scholar]
- Hautzinger M, Bailer M. Allgemeine depressionsskala (ADS) 1. Beltz Test GmbH: Göttingen; 1993. [Google Scholar]
- Bernard BP. Musculoskeletal Disorders and Workplace Factors - A Critical Review of Epidemiologic Evidence for Work-Related Musculoskeletal Disorders of the Neck, Upper Extremity, and Low Back. U.S: Department of Health and Human Services, Centers for Disease Control and Prevention; 1997. [Google Scholar]
- Sluiter JK, Rest KM, Frings-Dresen MH. Criteria document for evaluating the work-relatedness of upper-extremity musculoskeletal disorders. Scand J Work Environ Health. 2001;8(Suppl 1):1–102. [PubMed] [Google Scholar]
- Hartmann B, Spallek M. Arbeitsbezogene Muskel-Skelett-Erkrankungen - Eine Gegenstandsbestimmung. Arbeitsmedizin Sozialmedizin Umweltmedizin. 2009;8:423–436. [Google Scholar]
- Bühl A. PASW 18: Einführung in die moderne Datenanalyse [ehemals SPSS] 12. München: Pearson Studium; 2009. [Google Scholar]
- Bortz J, Döring N. Forschungsmethoden und Evaluation für Human- und Sozialwissenschaftler. 4. Heidelberg: Springer; 2006. [Google Scholar]
- Waddell G. Preventing incapacity in people with musculoskeletal disorders. Br Med Bull. 2006;8:55–69. doi: 10.1093/bmb/ldl008. [DOI] [PubMed] [Google Scholar]
- Hoogendoorn WE, van Poppel MN, Bongers PM, Koes BW, Bouter LM. Systematic review of psychosocial factors at work and private life as risk factors for back pain. Spine. 2000;8:2114–2125. doi: 10.1097/00007632-200008150-00017. [DOI] [PubMed] [Google Scholar]
- Flothow A, Zeh A, Nienhaus A. Unspecific back pain - basic principles and possibilites for intervention from a psychological point of view. Das Gesundheitswesen. 2009;8:845–856. doi: 10.1055/s-0029-1192028. [DOI] [PubMed] [Google Scholar]
- Seidler A, Liebers F, Latza U. Prevention of low back pain at work. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2008;8:322–333. doi: 10.1007/s00103-008-0463-3. [DOI] [PubMed] [Google Scholar]
- Stadler P, Spieß E. Arbeit - Psyche - Rückenschmerzen. Einflussfaktoren und Präventionsmöglichkeiten. Arbeitsmedizin Sozialmedizin Umweltmedizin. 2009;8:68–76. [Google Scholar]
- Langballe EM, Innstrand ST, Hagtvet KA, Falkum E, Gjerlow AO. The relationship between burnout and musculoskeletal pain in seven Norwegian occupational groups. Work. 2009;8:179–188. doi: 10.3233/WOR-2009-0804. [DOI] [PubMed] [Google Scholar]
- Andrea H, Beurskens AJ, Metsemakers JF, van Amelsvoort LG, van den Brandt PA, Van Schayck CP. Health problems and psychosocial work environment as predictors of long term sickness absence in employees who visited the occupational physician and/or general practitioner in relation to work: a prospective study. Occup Environ Med. 2003;8:295–300. doi: 10.1136/oem.60.4.295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hosmer D, Lemeshow S. Applied logistic regression. 2. New York: Wiley, Sons; 2000. [Google Scholar]
- de Zwart BC, Frings-Dresen MH, van Dijk FJ. Physical workload and the aging worker: a review of the literature. Int Arch Occup Environ Health. 1995;8:1–12. doi: 10.1007/BF01831627. [DOI] [PubMed] [Google Scholar]
- Ueberschär I, Heipertz W. Zur Leistungsfähigkeit älterer Arbeitnehmer aus arbeits- und sozialmedizinischer Sicht. Arbeitsmedizin Sozialmedizin Umweltmedizin. 2002;8:490–497. [Google Scholar]
- Neuhauser H, Ellert U, Ziese T. Chronic back pain in the general population in Germany 2002/2003: prevalence and highly affected population groups. Das Gesundheitswesen. 2005;8:685–693. doi: 10.1055/s-2005-858701. [DOI] [PubMed] [Google Scholar]
- Burton K, Waddell G. The back pain revolution. 2. Edinburgh: Churchill Livingstone; 2004. Risk factors for back pain; pp. 91–113. [Google Scholar]
- Institut für Arbeitsmarkt- und Berufsforschung der Bundesagentur für Arbeit (IAB) Berufe im Spiegel der Sta. 2013. [ http://bisds.infosys.iab.de/bisds/faces/Start.jsp]
- Trinkoff AM, Lipscomb JA, Geiger-Brown J, Brady B. Musculoskeletal problems of the neck, shoulder, and back and functional consequences in nurses. Am J Ind Med. 2002;8:170–178. doi: 10.1002/ajim.10048. [DOI] [PubMed] [Google Scholar]
- Kuhnert S, Nienhaus A. In: Gefährdungsprofile - Unfälle und arbeitsbedingte Erkrankungen in Gesundheitsdienst und Wohlfahrtspflege. 2. Nienhaus A, editor. Landsberg: Lech: ecomed; 2010. Burnout bei Altenpflegekräften - Prävalenz, Ursachen und Interventionsansätze; pp. 129–159. [Google Scholar]
- Tullar JM, Brewer S, Amick BC III, Irvin E, Mahood Q, Pompeii LA, Wang A, Van ED, Gimeno D, Evanoff B. Occupational safety and health interventions to reduce musculoskeletal symptoms in the health care sector. J Occup Rehabil. 2010;8:199–219. doi: 10.1007/s10926-010-9231-y. [DOI] [PubMed] [Google Scholar]