

Abstract
Background
With increasing numbers of type 2 diabetes (DM2) and hypertension patients, there is a pressing need for effective, time-efficient and sustainable strategies to help physicians support their patients to achieve higher physical activity levels. SMARTER will determine whether physician-delivered step count prescriptions reduce arterial stiffness over a one-year period, compared with usual care, in sedentary overweight/obese adults with DM2/hypertension.
Design
Randomized, allocation-concealed, assessor-blind, multisite clinical trial. The primary outcome is change in arterial stiffness over one year. The secondary outcomes include changes in physical activity, individual vascular risk factors, medication use, and anthropometric parameters. Assessments are at baseline and one year.
Methods
Participants are sedentary/low active adults with 25 ≤ BMI < 40 kg/m2 followed for DM2/hypertension by a collaborating physician. The active arm uses pedometers to track daily step counts and review logs with their physicians at 3 to 4-month intervals. A written step count prescription is provided at each visit, aiming to increase counts by ≥3,000 steps/day over one year, with an individualized rate increase. The control arm visits physicians at the same frequency and receives advice to engage in physical activity 30-60 minutes/day. SMARTER will enroll 364 individuals to detect a 10 ± 5% difference in arterial stiffness change between arms. Arterial stiffness is assessed noninvasively with carotid femoral pulse wave velocity using applanation tonometry.
Discussion
The importance of SMARTER lies not simply in the use of pedometer-based monitoring but also on its integration into a prescription-based intervention delivered by the treating physician. Equally important is the measurement of impact of this approach on a summative indicator of arterial health, arterial stiffness. If effectiveness is demonstrated, this strategy has strong potential for widespread uptake and implementation, given that it is well-aligned with the structure of current clinical practice.
Trial registration
ClinicalTrials.gov (NCT01475201)
Introduction
Longitudinal studies have demonstrated the protective effects of higher walking levels on arterial health in adults with type 2 diabetes (DM2) and hypertension. In the National Health Interview Survey [1], walking 120 minutes or more each week resulted in a 40% relative mortality rate reduction over 12 years. In the Nurses’ Health Study [2], those in the highest quartile of walking lowered their risk of heart attack, stroke, and related mortality by more than 30% over a decade. However, walking levels have declined in an era of Internet transactions, ‘smart’ phones, and ‘social networking,’ contributing to escalating rates of obesity and its detrimental consequences [3-7].
A meta-analysis indicates that the integration of physical activity promotion into primary care is associated with a 42% increase in self-reported activity [8]. The Green Prescription approach (physical activity-based prescriptions with three telephone-based support calls from trained counselors) has been widely implemented in the primary care context in New Zealand and has demonstrated sustained increases in physical activity levels [9]. These approaches, however, require paramedical staff support which may not be feasible in many settings. A more physician-driven approach had some effect on physical activity levels [10], but physicians generally lack the skills or time to provide more complex physical activity counseling, despite calls for more specific prescriptions [11]. In this regard, step count monitors such as pedometers may be a useful tool.
Pedometers permit simple, real-time tracking of walking and other step-related activity. Among NAVIGATOR trial participants (Nateglinide and Valsartan in Impaired Glucose Tolerance Outcomes Research [12]), both pedometer-assessed daily step counts at baseline (hazard ratio [HR] per 2,000 steps/day 0.90, 95% CI 0.84–0.96) and change in step counts over an average follow-up of 6 years (HR per 2,000 steps/day increase 0.92, 95% CI 0.86–0.99) led to reductions in cardiovascular disease events. These effects were independent of one another and also independent of underlying co-morbidities and changes in body mass index (BMI). Group pedometer-based programs increase physical activity levels and improve vascular risk profiles. In a meta-analysis of eight clinical trials [13], such interventions led to a 2,491 daily step increase [95% Confidence Interval (CI) 1,098 to 3,885], a -3.8 mm Hg change in systolic blood pressure (95% CI -5.9 to -1.7) and a -0.38 kg/m2 change in BMI (95% CI -0.05 to -0.72). These programs, however, may not be available or sustainable. Self-monitoring and target setting could be an inexpensive and accessible option, with assistance through web-based tools, but for many individuals this may not provide sufficient accountability and motivational support, elements deemed important to change health behaviours [14].
Integration of pedometer-based monitoring into routine medical visits, however, could help meet the need for accountability and support, without requiring additional staffing. We have developed such a strategy and we are testing it through a randomized controlled trial, as described herein. In our strategy, participants self-monitor and track step counts. They review these records with their physicians who then assist them in setting realistic step count targets, consistent with the monitoring-prescription-monitoring-adjusted prescription dynamic approach to which both physicians and patients are accustomed. Many patients with DM2 and hypertension self-monitor glucose and blood pressure levels; based on this information, their physicians are better-positioned to prescribe and adjust medications [15]. Such a strategy has not previously been evaluated for physical activity monitoring. A recent Green Prescription trial [16] integrated pedometer-based self-monitoring in a clinic setting and demonstrated higher activity levels, but again the intervention structure relied on paramedical clinic staff, rather than being routinely integrated as a component of medical visits with a physician. Thus the physician-patient relationship, an important factor in adherence to medications and physical activity, [17,18] was a less important factor in the intervention. In contrast, this is arguably the most important element of the SMARTER strategy. Another trial [19] did examine a physician-delivered intervention in DM2 and demonstrated a step count increase over a 12-week period but did not examine vascular effects; we are evaluating a one-year physician-delivered intervention and its impact on a summative indicator of arterial health, arterial stiffness, as described below.
The previously-cited meta-analysis of group-based pedometer interventions demonstrated reductions in blood pressure [13]. While blood pressure is one important indicator of arterial health, recent technological developments have allowed for a more comprehensive assessment of the arterial system through measurement of arterial stiffness, capturing the summative impact of vascular risk factors. Epidemiological studies have demonstrated that higher arterial stiffness is associated with increased risk of vascular disease and events [20-24]. In a trial among DM2 patients, a three-month supervised exercise program conferred a 20% greater reduction in arterial stiffness compared to usual care alone [25]. Higher daily step counts have been associated with lower carotid femoral pulse wave velocity (cfPWV), the gold standard measure of arterial stiffness [26,27].
We are conducting a randomized controlled trial to examine the effect of a physician-delivered step count prescriptions on arterial stiffness in sedentary overweight/obese adults with DM2 and/or hypertension. We present herein the design and methods of the SMARTER (Step Monitoring to improve ARTERial health) trial. Our primary objective is to assess the impact of the intervention on cfPWV using applanation tonometry. Our secondary objectives are to assess effects on individual vascular risk factors, medication use, anthropometric parameters, and physical activity, as detailed below.
Methods
The SMARTER trial is registered at ClinicalTrials.gov (NCT01475201). Funding is through the Canadian Institutes of Health Research (MOPP 114996). Approval of the research protocol has been granted by McGill University’s Faculty of Medicine Institutional Review Board and all participating institutions (McGill University Health Centre, St. Mary’s Hospital, Sir Mortimer General Jewish General Hospital). Written informed consent is provided by all participants.
Study design
SMARTER is a prospective, randomized, open-label, blinded-endpoint (PROBE) trial comparing two strategies to increase physical activity among overweight/obese adults followed for DM2 and/or hypertension. Allocation is concealed with an intervention to allocation ratio of 1:1.
Eligibility criteria and recruitment
Inclusion criteria include physician-diagnosis of DM2 or hypertension, age ≥18 years, and 25 kg/m2 ≤ BMI < 40 kg/m2 to permit accurate pedometer measurement [28]. Exclusion criteria include ≥ 150 minutes of leisure time physical activity per week (i.e., fulfilling physical activity recommendations) [29], co-morbid conditions with potential to affect adherence to trial procedures (e.g. inflammatory arthritis, active malignancy, major depression or other significant psychiatric disorders, and/or significant visual impairment), and pregnancy/planning a pregnancy. Further, following baseline evaluation but prior to randomization, those with a baseline step count averaging >10,000 steps/day (i.e., active) [30] are excluded. Treating physicians are free to modify medications during the trial period in both arms. Collaborating physicians are based at family medicine, internal medicine, endocrinology, and hypertension clinics in Montréal, Canada. They identify potentially eligible participants during routine clinic visits and obtain assent for contact by SMARTER personnel.
Measurements
All measurements detailed below are assessed both at baseline and following the intervention at one year so that changes during the trial may be computed. These evaluations are conducted at our Vascular Health Unit (Division of Internal Medicine, McGill University Health Centre).
Arterial stiffness
To avoid circadian variations that may affect arterial stiffness measurements, we evaluate all participants in the morning at approximately the same time of the day at baseline and again at the final evaluation. Participants are instructed to abstain from: i) caffeine and ethanol intake for at least 12 hours and flavonoid-containing foods (such as berries, grapes, apples, green tea, chocolate, nuts, herbs, and spices) for at least 24 hours before the evaluation, ii) any strenuous exercise (aerobic or anaerobic) for 24 hours before the evaluation, and iii) exposure to cigarette smoke for at least 12 hours before the evaluation. The participants are instructed to take all their medications except their antihyperglycemic medications in the morning of the baseline and final evaluations. Participants are requested to fast overnight (12 hours) prior to evaluation.
CfPWV is measured using applanation tonometry through the SphygmoCor system [31-34]. A high-fidelity micromanometer is placed on the tip of a hand-held tonometer (SPC-301; Millar Instruments, Houston, TX, USA) and applied to the skin overlying the radial artery to flatten but not occlude the artery. Using a previously validated generalized transfer function, the system software calculates an averaged radial artery waveform and derives a corresponding central pressure and other indices of pulse wave analysis, including the augmentation index and augmentation pressure [31,32,35,36]. The tonometer is then applied over the carotid and subsequently the femoral arteries with concurrent 3-lead ECG monitoring; the PWV is automatically calculated from measurements of the pulse transit time and the distance between the carotid and femoral recording sites [PWV = distance (m)/transit time (s)].
Physical activity
Participants are provided with two pedometers (Yamax SW-701; viewing windows concealed) to assess step counts and an accelerometer (Actiwatch-2; Phillips, Respironics) to capture duration, frequency, and intensity of physical activity. Participants wear one pedometer and the accelerometer for one week and then mail these to the study centre with the unused pedometer (padded, pre-addressed, pre-stamped envelope). The unused pedometer captures the “postman steps” that occur during the mailing process [37-39]; these are subtracted from the step counts recorded on the pedometer that is worn. Steps/day are computed from this corrected value.
Physical fitness
Cardiorespiratory fitness is assessed through a supervised maximal incremental test to determine VO2max (model VMax229LV, Sensorsmedics, Yorba Linda, CA, USA) with treadmill testing (MedTrackCR60 Treadmill, Quinton, Bothell, WA, USA; Bruce ramp protocol).
Anthropometric measures
Weight and height are assessed to the nearest 0.1 kg (SECA 882 electronic scale, light clothing, shoes removed) and 0.1 cm (stadiometer), respectively. BMI is calculated by dividing the weight in kilograms by height in metres squared. Waist circumference is measured midway between the iliac crest and the lower rib margin. Hip circumference is measured at the point of greatest posterior extension of the buttocks.
Blood pressure
Resting blood pressure is measured using the BpTRU Blood Pressure Monitor using a standardized protocol [40].
Serum biomarkers
Lipid profile Total cholesterol, high density lipoprotein cholesterol (HDL-C), and triglyceride levels are measured using spectrophotometry and low density lipoprotein cholesterol (LDL-C) is calculated (Friedewald equation). Apolipoproteins A1 and B are measured using the turbimetric method. In participants with DM2, hemoglobin A1C is measured with a high-performance liquid chromatography (HPLC) analyzer [41]. In those without DM2, fasting glucose and insulin levels are measured and the Homeostatic Model Assessment is calculated [(fasting insulin in μunits/ml X fasting glucose in mmol/L) ÷ 22.5] [42-47]. High sensitivity C-reactive protein is assayed through an immunonephelometric method.
Cardioprotective medications
Use of antihypertensive, antihyperglycemic, and lipid-lowering medications (number and dose) is recorded.
Adherence
We are tracking clinic visits completed, prescriptions written by collaborating physicians, and use of the step count log book.
Randomization
Patient inclusion and data entry forms (eCFRs) were created using web Electronic Data Capture software platform from Dacima™. Data are entered through a web browser into a web database that complies with regulatory requirements (FDA 21 CFR Part 11). First, data from the initial telephone-based eligibility screen are entered on the electronic eligibility check web form. The EDC system verifies the candidates’ responses to make a preliminary determination of eligibility. Candidates who fulfill preliminary assessments for eligibility present in person for informed consent procedures and baseline assessment. The baseline evaluation is considered completed once the pedometers with concealed viewing windows are received by study personnel (see Measurements, Physical activity). Pedometer-based step count data are entered into the web form. Those with more than 10,000 steps/day are determined to be ineligible by the EDC inclusion algorithm and marked as excluded.
Eligible individuals are randomized to either the control or the active trial arm through the Dacima™ Clinical software (i.e., individual-level randomization with no stratification; random permuted blocks with randomly-varied block sizes of two, four and six).
Interventions
Participants are followed by their physician at 3 to 4-month intervals over 12 months. The control arm receives advice to engage in 30-60 minutes of activity daily, consistent with usual care [48]. In the active arm, the physician writes a step count prescription at each visit. As previously noted, pedometer-based interventions led to a 2,491 daily step increase in a meta-analysis [13]. A step count increment of 2,500 to 3,000 steps is roughly equivalent to 30 minutes of walking at a moderate pace, as established through direct counts of individuals walking on a treadmill at a workload of 3 metabolic equivalents (METS)/minute [49]. In the SMARTER active arm, the aim is to achieve a net increase over baseline values of at least 3,000 steps/day over one year. DM2 and hypertension follow-up visits are recommended at 3 to 4 month intervals. Testing an intervention over 1 year permits 3 to 4 contacts with the treating physician but still respects the reality of usual clinical follow-up. This is important if the results of this trial are to be implemented in real-world practice following the trial itself. A 1-year study duration will mean that participants are examined at roughly the same time of year (i.e., season) at the baseline and final assessments. This will help ensure that any changes demonstrated are not attributable to seasonal differences [50]. Finally, many physical activity intervention studies have been criticized as being too short in duration; we suggest that a 1-year period of intervention and follow-up provides a reasonable time frame over which to evaluate effects.
The rapidity at which this is achieved is individually-tailored (Figure 1). The baseline step count value is provided by the research team as derived from the baseline assessment. The general time frame for the increase by 3,000 steps/day is 10 months for sedentary participants (<5,000 steps/day), 7 months for low active participants (5,000-7,499 steps/day), and 5 months for somewhat active participants (7,500-9,999 steps/day). Subsequent prescriptions are based on step counts achieved and individual circumstances.
Figure 1.
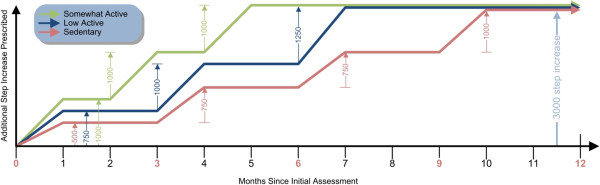
Step count prescription framework by baseline activity category. Months in red are those at which a clinic visit occurs. All participants should ultimately achieve a net increase of at least 3,000 steps/day from baseline, as indicated in light blue.
Sample size
Madden and colleagues [25] conducted a randomized controlled trial comparing a 3-month supervised exercise program with usual care in adults with DM2, hypertension, and dyslipidemia. Exercise sessions were three times per week (cycle ergometers, treadmills). They demonstrated a 13.9% reduction in cfPWV in the intervention arm compared with a 4.4% increase in the control arm (i.e., an 18.3% difference). To be conservative, we aim to detect a 10% difference between our active and control trial arms to an accuracy of ± 5% over a one-year period. This implies that our CI for the difference will be narrow enough to rule out only trivial effects. Based on the report by Madden and colleagues, we estimate a standard deviation (SD) of 28 in the active treatment arm [standard error, SE* sqrt (n) = 6.7 * sqrt(17)] and 14 for the control arm [3.3*sqrt (17)]. Under these conditions, with ± 5% CI width, we will need to retain 151 per arm (i.e., 302 in total). Allowing for a loss to follow-up of up to 17% based on our previous studies, [50,51] we require a sample size of 364 individuals (i.e., 182 per arm).
Statistical analysis
Our main outcome is percentage change in arterial stiffness (i.e., cfPWV) within each trial arm. We will calculate mean between trial arm differences in “after minus before changes”, with 95% CIs (intent-to-treat analysis). In addition to examining between trial arm differences in percentage change from baseline arterial stiffness, we will also evaluate between arm absolute differences in raw “after minus before changes” in cfPWV. Although trial arms are likely to be similar at baseline, we may use a linear model to adjust for any possible differences between arms for important covariates (e.g., baseline daily steps, baseline BMI, age, sex, changes in medications). If relevant, in a sensitivity analysis, we will use multiple imputation to impute missing data. A similar approach will be used to examine between-arm differences in daily steps and vascular risk factors. We will also correlate increments in steps to changes in arterial stiffness, anthropometric parameters, and specific vascular risk factors. Finally, we may employ additional secondary analyses (e.g., per protocol analyses; analyses in DM2 alone, hypertension alone, DM2 and hypertension; analyses in participants with and without medication changes).
Discussion
The SMARTER trial is testing an innovative step count prescription strategy delivered by physicians to their patients with DM2 or hypertension. The focus on daily step counts arguably simplifies the process of physical activity prescription. Increasingly, physicians and patients are partners in monitoring and managing chronic diseases. Such partnerships can improve patient adherence and health outcomes [15]. Less than one third of North Americans achieve the recommended 10,000 steps/day [52] and we have demonstrated that in adults with DM2 and/or hypertension, mean counts are low at approximately 5,000 steps/day, with a further 15% reduction during fall and winter months [50]. “Re-engineering” walking into daily life could be an effective means of improving the arterial health of patients with DM2 and/or hypertension.
The effects of the SMARTER intervention are being determined in terms of biological impact, particularly in terms of changes in arterial stiffness as captured by cfPWV. In the Framingham Heart Study, a one SD increment in arterial stiffness was associated with a 48% increase in arterial disease risk, independently of individual vascular risk factors [23]. A meta-analysis indicates that an increase in cfPWV by 1 m/s corresponds to an age-, sex-, and risk factor-adjusted risk increases of 14%, 15%, and 15% in total cardiovascular disease event rates, cardiovascular mortality, and all cause mortality, respectively [53]. A recent analysis of the Framingham Offspring study demonstrated that higher aortic stiffness is associated with higher risk of incident hypertension [24], suggesting that in some cases stiffness precedes the development of hypertension. Illustrating the responsiveness of cfPWV to higher activity levels, a trial among older patients with vascular risk factors including DM2 demonstrated a 3-month supervised exercise program to confer an important reduction in cfPWV compared to usual care alone [25].
We are aware of some potential limitations to the trial. Firstly, physicians cannot be blinded to the intervention given that they are delivering it. However, outcome assessors are blinded to intervention arm status, and both the primary outcome and most of the secondary outcomes are evaluated objectively (i.e., assays or automated measurements). We acknowledge the possibility of contamination of the control arm: that is, physicians may be tempted to employ the SMARTER intervention in the control arm, particularly if they perceive benefit. However, only the active trial arm receives pedometers at the onset of the intervention period. Following the final trial evaluation, the control trial arm participants will be provided with a pedometer in gratitude for their participation, and they will be free to engage in a step count prescription strategy with their treating doctor. This ‘delayed’ intervention may facilitate adherence to study procedures. Physicians are free to modify medications during the trial period and this could impact some outcomes. To address this possibility, we will perform secondary analyses with (i) adjustment for changes in medications and (ii) restriction to participants without such changes. We acknowledge that more frequent contact with physicians and/or other health care team members could strengthen the impact of the intervention; however, DM2 and hypertension follow-up frequently occurs in settings without multidisciplinary teams and the demands of clinical care may render more frequent contact challenging. We have, therefore, designed our intervention to be ‘pragmatic’ with 3 to 4 follow-up visits over one year accompanied by a written prescription. Patients with DM2 and hypertension generally have common features including insulin resistance and increased risk for vascular disease. The inclusion of participants with DM2 and hypertension, each alone or in combination, allows us to achieve recruitment targets in a reasonable time frame and to generalize our results to groups of patients seen frequently in clinical practice; we will nonetheless perform subgroup analyses (DM2 alone, hypertension alone, DM2 and hypertension in combination).
We have developed our trial in collaboration with physicians who manage DM2 and hypertension. We held several meetings with over 24 physicians to discuss the intervention. They underscored their need for physical activity promotion tools and viewed the SMARTER strategy to be feasible and easily integrated into clinical practice. They, nonetheless, expressed the need for Level A evidence as derived through a randomized controlled trial. This integrated knowledge translation approach will facilitate future knowledge translation efforts. If effectiveness is demonstrated, we are well-positioned to consider inclusion in Clinical Practice Recommendations for DM2 and hypertension.
The SMARTER intervention is novel in several respects: (i) It is physician-specific intervention that may be particularly important in understaffed clinics without the support of a full multidisciplinary team. (ii) A specific, signed, stamped written prescription is provided, focusing on step count targets. (iii) The rate of step count titration is individualized, based on baseline step counts, leveraging an existing therapeutic alliance. (iv) The primary outcome is change in arterial stiffness, a summative indicator of arterial health. Prior pedometer-based intervention studies have examined specific individual vascular risk factors but to our knowledge, none have evaluated a summative indicator of arterial health (arterial stiffness) as the primary outcome. (v) A shortcoming of prior studies has often been a lack of attention to medication use. This is being carefully recorded during our trial and we will perform subgroup analyses in those with and without medication changes (e.g., antihypertensive agents, antihyperglycemic agents, lipid-lowering agents). We will further evaluate changes in medication use as a secondary outcome. (vi) This will be one of the largest pedometer intervention trials ever conducted (364 participants).
In summary, the potential impact of the SMARTER intervention relates not only to the use of pedometers but rather to its incorporation into clinical care, leveraging the physician-patient therapeutic alliance. A key strength of the SMARTER trial is the ability to capture biological impact through measurement of arterial stiffness. Demonstration of effectiveness of the SMARTER intervention has strong potential to lead to wide and sustained adoption in clinical practice with integration in DM2 and hypertension management.
Abbreviations
BMI: Body mass index; DM2: Type 2 diabetes; CI: Confidence interval; cfPWV: Carotid femoral pulse wave velocity; PWA: Pulse wave analysis; PWV: Pulse wave velocity; ECG: Electrocardiogram; VO2max: Maximum oxygen uptake; HDL-C: High density lipoprotein cholesterol; LDL-C: Low density lipoprotein cholesterol; Hemoglobin A1C: Glycosylated hemoglobin; HPLC: High performance liquid chromatography; MET: Metabolic equivalent; CVD: Cardiovascular disease
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
KD and SSD conceived and designed the study and co-wrote the study protocol, with critical input from ER and the SMARTER collaborators. All authors read and approved the final manuscript.
Author’s information
KD and SSD are Physician Scientists and Associate Professors in the Department of Medicine at McGill University. ER is Associate Professor in the Department of Family Medicine at McGill University. KD and SSD both hold clinical investigator salary awards from the Fonds de recherche Santé du Québec. KD additionally holds the Société québécoise d’hypertension artérielle-Jacques de Champlain Award; SSD is a previous recipient of this award.
Contributor Information
Kaberi Dasgupta, Email: kaberi.dasgupta@mcgill.ca.
Ellen Rosenberg, Email: ellen.rosenberg@mcgill.ca.
Stella S Daskalopoulou, Email: stella.daskalopoulou@mcgill.ca.
Acknowledgements
The SMARTER trial group includes the following co-investigators who provided important comments during protocol development: Lawrence Joseph (biostatistician; Professor of Epidemiology, Biostatistics and Occupational Medicine, McGill University), Susan Kahn (clinical trialist and Physician Scientist; Professor of Medicine, McGill University), Louise Pilote (cardiovascular epidemiologist and Physician Scientist; Professor of Medicine, McGill University), and Simon Bacon (behavioural medicine researcher; Associate Professor of Exercise Sciences, Concordia University).
Recruitment and assessments are managed by SMARTER trial manager Deborah Chan with assistance from Cindy Ibberson, Samantha Hajna, Yessica Haydee Gomez Sandoval, Marie-Eve Robillard, Alexandra Cooke, and Rani Cruz.
Critical to the success of this trial is our network of collaborating physicians including Catherine Kudo1, Mark Sherman1, Donald Sproule2, Natasha Garfield1, Susan Still2, Walter Gregory1, Leonora Lalla2, Margaret Hughes2, Maureen Doyle2, Lynn McLaughlin2, David Shannon3, Stavroula Christopoulos4, David Morris1, Raymond Sorge2, Laurence Green3, Sara Meltzer1, Alicia Schiffrin4, Mark Yaffe2, Robert Diex d’Aux2, Paul Cruvellier2, Barry Posner1, Marie-Luce Chen2, Joanna Caron2, Maxine Dumas-Pilon2, Marie Weber2, Tim Meagher3; Roxanne Arel2, Murray Vasilevsky5, Hans Zingg1, Suzanne Morin3 , Tina Kader4, Simon Wing1, Renata Sava2, Brent Richards4, Juan Rivera1, Agnieska Majdan4, Robert Benoit1, George Tsoukas1, Khue Ly3, Jean-Francois Yale1, Florence Tremblay2, Kurt Jansen6, Karen Dahan6, Alison Doucet6, Patrick Willemot3, Todd Campbell Lee3, Bruce Campbell3, 7, Jeffrey Segal7 David Blank1, Ruxandra Bunea8, David Dawson3, Candace Lee9 and Pnina Wasser2.
1Division of Endocrinology, Department of Medicine, McGill University Health Centre and McGill University; 2Department of Family Medicine, St. Mary’s Hospital, Montreal, Quebec and McGill University; 3Division of Internal Medicine, Department of Medicine, McGill University Health Centre and McGill University; 4Division of Endocrinology, Department of Medicine, Sir Mortimer Davis Jewish General Hospital and McGill University; 5Division of Nephrology, Department of Medicine, McGill University Health Centre and McGill University; 6Queen Elizabeth Health Complex, McGill University Health Centre and McGill University; 7Division of Internal Medicine, St. Mary’s Hospital, Montreal, Quebec and McGill University; 8Division of Internal Medicine, Department of Medicine, Sir Mortimer Davis Jewish General Hospital and McGill University; 9Private Cardiology Clinic.
Funding for this trial is from the Canadian Institutes of Health Research (MOPP 114996; Nominated Principal Investigator K. Dasgupta; Co-Principal Investigators S.S. Daskalopoulou and E. Rosenberg).
References
- Gregg EW, Gerzoff RB, Caspersen CJ, Williamson DF, Narayan KM. Relationship of walking to mortality among US adults with diabetes. Arch Intern Med. 2003;163:1440–1447. doi: 10.1001/archinte.163.12.1440. [DOI] [PubMed] [Google Scholar]
- Hu FB, Stampfer MJ, Solomon C, Liu S, Colditz GA, Speizer FE. et al. Physical activity and risk for cardiovascular events in diabetic women. Ann Intern Med. 2001;134:96–105. doi: 10.7326/0003-4819-134-2-200101160-00009. [DOI] [PubMed] [Google Scholar]
- Hill JO, Wyatt HR, Reed GW, Peters JC. Obesity and the environment: where do we go from here? Science. 2003;299:853–855. doi: 10.1126/science.1079857. [DOI] [PubMed] [Google Scholar]
- Sturm R. Stemming the global obesity epidemic: what can we learn from data about social and economic trends? Public Health. 2008;122:739–746. doi: 10.1016/j.puhe.2008.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Booth GL, Kapral MK, Fung K, Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet. 2006;368:29–36. doi: 10.1016/S0140-6736(06)68967-8. [DOI] [PubMed] [Google Scholar]
- Lee WL, Cheung AM, Cape D, Zinman B. Impact of diabetes on coronary artery disease in women and men: a meta-analysis of prospective studies. Diabetes Care. 2000;23:962–968. doi: 10.2337/diacare.23.7.962. [DOI] [PubMed] [Google Scholar]
- Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339:229–234. doi: 10.1056/NEJM199807233390404. [DOI] [PubMed] [Google Scholar]
- Orrow G, Kinmonth AL, Sanderson S, Sutton S. Effectiveness of physical activity promotion based in primary care: systematic review and meta-analysis of randomised controlled trials. BMJ. 2012;344:e1389. doi: 10.1136/bmj.e1389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elley CR, Kerse N, Arroll B, Robinson E. Effectiveness of counselling patients on physical activity in general practice: cluster randomised controlled trial. BMJ. 2003;326:793. doi: 10.1136/bmj.326.7393.793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grandes G, Sanchez A, Sanchez-Pinilla RO, Torcal J, Montoya I, Lizarraga K. et al. Effectiveness of physical activity advice and prescription by physicians in routine primary care: a cluster randomized trial. Arch Intern Med. 2009;169:694–701. doi: 10.1001/archinternmed.2009.23. [DOI] [PubMed] [Google Scholar]
- Katz MH. Writing more specific exercise prescriptions. Arch Intern Med. 2012;172:1283–1284. doi: 10.1001/archinternmed.2012.3196. [DOI] [PubMed] [Google Scholar]
- Yates T, Haffner SM, Schulte PJ, Thomas L, Huffman KM, Bales CW, Association between change in daily ambulatory activity and cardiovascular events in people with impaired glucose tolerance (NAVIGATOR trial): a cohort analysis. The Lancet. 2013. [Epub ahead of print] [DOI] [PubMed]
- Bravata DM, Smith-Spangler C, Sundaram V, Gienger AL, Lin N, Lewis R. et al. Using pedometers to increase physical activity and improve health: a systematic review. JAMA. 2007;298:2296–2304. doi: 10.1001/jama.298.19.2296. [DOI] [PubMed] [Google Scholar]
- Casey D, De CM, Dasgupta K. Understanding physical activity facilitators and barriers during and following a supervised exercise programme in type 2 diabetes: a qualitative study. Diabet Med. 2010;27:79–84. doi: 10.1111/j.1464-5491.2009.02873.x. [DOI] [PubMed] [Google Scholar]
- Delamater AM. Improving patient adherence. Clinical Diabetes. 2006;24:71–77. doi: 10.2337/diaclin.24.2.71. [DOI] [Google Scholar]
- Kolt GS, Schofield GM, Kerse N, Garrett N, Ashton T, Patel A. Healthy steps trial: pedometer-based advice and physical activity for low-active older adults. Ann Fam Med. 2012;10:206–212. doi: 10.1370/afm.1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blackstock OJ, Addison DN, Brennan JS, Alao OA. Trust in primary care providers and antiretroviral adherence in an urban HIV clinic. J Health Care Poor Underserved. 2012;23:88–98. doi: 10.1353/hpu.2012.0006. [DOI] [PubMed] [Google Scholar]
- Bell RA, Arcury TA, Ip E, Grzywacz JG, Nguyen H, Kirk JK. et al. Correlates of physician trust among rural older adults with diabetes. Am J Health Behav. 2013;37:660–666. doi: 10.5993/AJHB.37.5.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De GK, Deforche B, Tudor-Locke C, De B I. Increasing physical activity in Belgian type 2 diabetes patients: a three-arm randomized controlled trial. Int J Behav Med. 2011;18:188–198. doi: 10.1007/s12529-010-9124-7. [DOI] [PubMed] [Google Scholar]
- Mancia G, De BG, Dominiczak A, Cifkova R, Fagard R, Germano G. et al. Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) J Hypertens. 2007;2007(25):1105–1187. doi: 10.1097/HJH.0b013e3281fc975a. [DOI] [PubMed] [Google Scholar]
- Willum-Hansen T, Staessen JA, Torp-Pedersen C, Rasmussen S, Thijs L, Ibsen H. et al. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation. 2006;113:664–670. doi: 10.1161/CIRCULATIONAHA.105.579342. [DOI] [PubMed] [Google Scholar]
- Mattace-Raso FU, van der Cammen TJ, Hofman A, van Popele NM, Bos ML, Schalekamp MA. et al. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study. Circulation. 2006;113:657–663. doi: 10.1161/CIRCULATIONAHA.105.555235. [DOI] [PubMed] [Google Scholar]
- Mitchell GF, Hwang SJ, Vasan RS, Larson MG, Pencina MJ, Hamburg NM. et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. 2010;121:505–511. doi: 10.1161/CIRCULATIONAHA.109.886655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaess BM, Rong J, Larson MG, Hamburg NM, Vita JA, Levy D. et al. Aortic stiffness, blood pressure progression, and incident hypertension. JAMA. 2012;308:875–881. doi: 10.1001/2012.jama.10503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madden KM, Lockhart C, Cuff D, Potter TF, Meneilly GS. Short-term aerobic exercise reduces arterial stiffness in older adults with type 2 diabetes, hypertension, and hypercholesterolemia. Diabetes Care. 2009;32:1531–1535. doi: 10.2337/dc09-0149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aoyagi Y, Park H, Kakiyama T, Park S, Yoshiuchi K, Shephard RJ. Yearlong physical activity and regional stiffness of arteries in older adults: the Nakanojo Study. Eur J Appl Physiol. 2010;109:455–464. doi: 10.1007/s00421-010-1357-2. [DOI] [PubMed] [Google Scholar]
- Jennersjo P, Ludvigsson J, Lanne T, Nystrom FH, Ernerudh J, Ostgren CJ. Pedometer-determined physical activity is linked to low systemic inflammation and low arterial stiffness in type 2 diabetes. Diabet Med. 2012;29:1119–1125. doi: 10.1111/j.1464-5491.2012.03621.x. [DOI] [PubMed] [Google Scholar]
- Cyarto EV, Myers AM, Tudor-Locke C. Pedometer accuracy in nursing home and community-dwelling older adults. Med Sci Sports Exerc. 2004;36:205–209. doi: 10.1249/01.MSS.0000113476.62469.98. [DOI] [PubMed] [Google Scholar]
- Hackam DG, Khan NA, Hemmelgarn BR, Rabkin SW, Touyz RM, Campbell NR. et al. The 2010 Canadian Hypertension Education Program recommendations for the management of hypertension: part 2 - therapy. Can J Cardiol. 2010;2010(26):249–258. doi: 10.1016/s0828-282x(10)70379-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tudor-Locke C, Bassett DR Jr. How many steps/day are enough? Preliminary pedometer indices for public health. Sports Med. 2004;34:1–8. doi: 10.2165/00007256-200434010-00001. [DOI] [PubMed] [Google Scholar]
- Chen CH, Nevo E, Fetics B, Pak PH, Yin FC, Maughan WL. et al. Estimation of central aortic pressure waveform by mathematical transformation of radial tonometry pressure. Validation of generalized transfer function. Circulation. 1997;95:1827–1836. doi: 10.1161/01.CIR.95.7.1827. [DOI] [PubMed] [Google Scholar]
- Pauca AL, O'Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension. 2001;38:932–937. doi: 10.1161/hy1001.096106. [DOI] [PubMed] [Google Scholar]
- Sharman JE, Lim R, Qasem AM, Coombes JS, Burgess MI, Franco J. et al. Validation of a generalized transfer function to noninvasively derive central blood pressure during exercise. Hypertension. 2006;47:1203–1208. doi: 10.1161/01.HYP.0000223013.60612.72. [DOI] [PubMed] [Google Scholar]
- O'Rourke M, Jiang XJ. Use of radial artery applanation tonometry. J Am Coll Cardiol. 1999;34:951–952. doi: 10.1016/s0735-1097(99)00291-0. [DOI] [PubMed] [Google Scholar]
- O'Rourke MF, Pauca A, Jiang XJ. Pulse wave analysis. Br J Clin Pharmacol. 2001;51:507–522. doi: 10.1046/j.0306-5251.2001.01400.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahmud A, Feely J. Acute effect of caffeine on arterial stiffness and aortic pressure waveform. Hypertension. 2001;38:227–231. doi: 10.1161/01.HYP.38.2.227. [DOI] [PubMed] [Google Scholar]
- Manjoo P, Joseph L, Pilote L, Dasgupta K. Sex differences in step count-blood pressure association: a preliminary study in type 2 diabetes. PLoS One. 2010;5:e14086. doi: 10.1371/journal.pone.0014086. doi:10.1371/journal.pone.0014086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manjoo P, Joseph L, Dasgupta K. Abdominal adiposity and daily step counts as determinants of glycemic control in cohort of patients with type 2 diabetes mellitus. Nutrition and Diabetes. 2012;2:e25. doi: 10.1038/nutd.2011.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dasgupta K, Chan C, Da Costa D, Pilote L, De Civita M, Ross N. et al. Walking behaviour and glycemic control in type 2 diabetes: seasonal and gender differences--study design and methods. Cardiovasc Diabetol. 2007;6:1. doi: 10.1186/1475-2840-6-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quinn RR, Hemmelgarn BR, Padwal RS, Myers MG, Cloutier L, Bolli P. et al. The 2010 Canadian Hypertension Education Program recommendations for the management of hypertension: part I - blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol. 2010;2010(26):241–248. doi: 10.1016/s0828-282x(10)70378-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran DV, Hofer TL, Lee T, Cembrowski GS. Unique approach to derivation of random error in laboratory assays: application to glycohemoglobin testing demonstrates poor clinical performance for immunochemistry assay. Diabetes Technol Ther. 2003;5:975–978. doi: 10.1089/152091503322641015. [DOI] [PubMed] [Google Scholar]
- Albareda M, Rodriguez-Espinosa J, Murugo M, de LA, Corcoy R. Assessment of insulin sensitivity and beta-cell function from measurements in the fasting state and during an oral glucose tolerance test. Diabetologia. 2000;43:1507–1511. doi: 10.1007/s001250051561. [DOI] [PubMed] [Google Scholar]
- Bonora E, Formentini G, Calcaterra F, Lombardi S, Marini F, Zenari L. et al. HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: prospective data from the Verona Diabetes Complications Study. Diabetes Care. 2002;25:1135–1141. doi: 10.2337/diacare.25.7.1135. [DOI] [PubMed] [Google Scholar]
- Chang AM, Smith MJ, Bloem CJ, Galecki AT, Halter JB, Supiano MA. Limitation of the homeostasis model assessment to predict insulin resistance and beta-cell dysfunction in older people. J Clin Endocrinol Metab. 2006;91:629–634. doi: 10.1210/jc.2005-1803. [DOI] [PubMed] [Google Scholar]
- Chen J, Wildman RP, Hamm LL, Muntner P, Reynolds K, Whelton PK. et al. Association between inflammation and insulin resistance in U.S. nondiabetic adults: results from the Third National Health and Nutrition Examination Survey. Diabetes Care. 2004;27:2960–2965. doi: 10.2337/diacare.27.12.2960. [DOI] [PubMed] [Google Scholar]
- Dixon JB, Dixon AF, O'Brien PE. Improvements in insulin sensitivity and beta-cell function (HOMA) with weight loss in the severely obese. Homeostatic model assessment. Diabet Med. 2003;20:127–134. doi: 10.1046/j.1464-5491.2003.00889.x. [DOI] [PubMed] [Google Scholar]
- Miyatake N, Nishikawa H, Morishita A, Kunitomi M, Wada J, Suzuki H. et al. Daily walking reduces visceral adipose tissue areas and improves insulin resistance in Japanese obese subjects. Diabetes Res Clin Pract. 2002;58:101–107. doi: 10.1016/S0168-8227(02)00129-8. [DOI] [PubMed] [Google Scholar]
- World Health Organization (WHO) GSoDPAaH. Facts Related to Chronic Dieases. 2003. http://www.who.int/dietphysicalactivity/publications/9789241599979/en/index.html.
- Marshall SJ, Levy SS, Tudor-Locke CE, Kolkhorst FW, Wooten KM, Ji M. et al. Translating physical activity recommendations into a pedometer-based step goal: 3000 steps in 30 minutes. Am J Prev Med. 2009;36:410–415. doi: 10.1016/j.amepre.2009.01.021. [DOI] [PubMed] [Google Scholar]
- Dasgupta K, Joseph L, Pilote L, Strachan I, Sigal RJ, Chan C. Daily steps are low year-round and dip lower in fall/winter: findings from a longitudinal diabetes cohort. Cardiovasc Diabetol. 2010;9:81. doi: 10.1186/1475-2840-9-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dasgupta K, Grover SA, Da Costa D, Lowensteyn I, Yale JF, Rahme E. Impact of modified glucose target and exercise interventions on vascular risk factors. Diabetes Res Clin Pract. 2006;72:53–60. doi: 10.1016/j.diabres.2005.09.010. [DOI] [PubMed] [Google Scholar]
- Colley RC, Garriguet D, Janssen I, Craig CL, Clarke J, Tremblay MS. Physical activity of Canadian adults: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2009;2011(22):7–14. [PubMed] [Google Scholar]
- Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55:1318–1327. doi: 10.1016/j.jacc.2009.10.061. [DOI] [PubMed] [Google Scholar]