

Abstract
Background:
Population aging is a global phenomenon. In India, the size of the elderly population is growing fast. Many older adults have multiple medical conditions. Understanding elderly health problems and health-seeking behavior is prerequisite for proving comprehensive geriatric care to them.
Objectives:
To assess the morbidity pattern and study the health-seeking behavior of the elderly people of Shimla district in Himachal Pradesh.
Materials and Methods:
A total of 400 elderly people aged 60 years and above were selected from urban and rural areas of Shimla hills in North India by simple random sampling. Statistical software Epi info software version 3.2 was used for analyzing data. Descriptive statistics were used to describe sociodemographic and morbidity variables.
Results:
The most common morbidity identified among them were musculoskeletal problems (55.0%) followed by hypertension (40.5%). Two third were seeking treatment for their health problems. Among older persons not seeking treatment for their medical condition, most considered these morbidities as an age-related phenomenon. Many perceived that the health services were too far.
Conclusion:
The high morbidity load among elderly in the present study stresses for efforts to provide better health care to them and thus ensure that they remain active members of our society. Residence emerged out to be most significant determinant of healthcare-seeking behavior. Policy makers must focus on rural elderly and their beliefs which prevent them from seeking healthcare.
Keywords: Elderly, health-seeking behavior, morbidity
Introduction
Worldwide increase in longevity has shifted the age distribution toward older populations.[1] In India the size of the elderly population, that is, persons above the age of 60 years is growing fast. The absolute number in India increased from 76 millions in 2001 to 100 millions in 2011. Like other Indian states, Himachal Pradesh, a hilly state of North India is witnessing a progressive increase in proportion of aged people from 8% in 2001 to 10.2% in 2011(census data).[2,3]
Population aging generates many challenges and sparks concerns about the pace of future economic growth, the operation and financial integrity of healthcare and pension systems, and the well-being of the elderly.[4] Aging leads to a generalized deterioration of many organs and systems. It leads to a lower effectiveness of physiological functions accompanied by an increase in risk factors for various diseases. A fall in bone mass leads to osteoporosis and fractures, cartilage degeneration leads to musculoskeletal problems, muscle loss leads to functional weakness, a decline in immune function cause increases in infections and cancer, and increased neuronal degeneration leads to decline of cognitive function and dementia. Health-seeking behavior in terms of illness behavior refers to those activities undertaken by individuals in response to symptom experience. Elderly patients are generally perceived to be more reluctant to seek health care for ailments.[5,6]
The state of Himachal Pradesh is predominantly hilly. Poor road connectivity, difficult hilly terrain, and small scattered settlements contribute to problems of access to health services. Shimla, the capital city of Himachal Pradesh, has two major tertiary care government hospitals. Though there are out-patient geriatric units in these hospitals, they are virtually nonfunctional owing to shortage of manpower and resources. Also, in Shimla district there are no specific geriatric services in primary and secondary levels of care. Elderly living in hilly terrain may have different perceived needs and morbidity pattern. During the past decade, there are numerous studies highlighting the morbidity pattern in different geographical areas of India, but none relating to this hilly state of North India. The results of this study are expected to help policy makers in planning specialized services for elderly residing in this area of North India. With this background, we did a study to assess the morbidity pattern and study the health-seeking behavior in aged population of Shimla district in Himachal Pradesh.
Materials and Methods
This was a descriptive cross-sectional study conducted among rural and urban elderly population aged 60 years and above residing in Shimla hills located in North India. The study was done over a period of one year (2010-2011). The sample size was calculated based on the formula 4 pq/L2. Due to lack of information on morbidity and health-seeking among elderly in the study area, the calculation was based on the assumption of prevalence to be 50%. Assuming a confidence level of 95% and at a precision of 7%, the total sample size was 196 elderly. (200 elderly from urban areas and 200 elderly from rural areas of district Shimla of Himachal Pradesh). The study sample was obtained by multistage simple random sampling. In urban area (Shimla city), five wards were selected out of the 25 wards by simple random sampling. A total of 40 older persons were selected from each ward. Each of the selected wards was divided into four parts with equal population (approximately) so that from all the parts equal numbers of subjects were enrolled for the study. For each part, one house was selected randomly. Starting from this house, every nearest next house was surveyed until 10 subjects were enrolled for the study. A similar procedure was applied in the remaining parts of the ward. In rural areas (Mashobra), out of the 15 subcenter villages, five were selected by simple random sampling. A total of 40 older persons were selected from each selected village. With the help of key informants, sampled villages were geographically divided into four parts with equal population (approximately). For each part, one house was selected randomly. Starting from this house, every nearest next house was surveyed until 10 subjects were enrolled for the study. A similar procedure was applied in the remaining parts of the ward.
Data on sociodemographic factors and included age, gender, marital status, level of education, type of family, and living arrangement was collected. Marital status was categorized as married or widowed. Level of education was categorized as illiterate or literate. Socioeconomic status was recorded and classified as those belonging to below poverty line and above poverty line. Health status among the older persons was assessed through self-reported data on history of illness followed by examination by the physician. Informed, written consent for participation was obtained from each individual. Only those elderly who were found to have some health problem were asked questions about health-seeking behavior. Respondents were asked “Do you seek healthcare for your health problem Yes/No?” If the answer was affirmative, then the type of healthcare sought was enquired like allopathic, homeopathic, ayurveda, and so on. If the study subject said they did not seek healthcare, then the reasons for the same was ascertained from the list of options in the pretested questionnaire.
Statistical software Epi info software version 3.2 was used for analyzing data. Descriptive statistics were used to describe sociodemographic and morbidity variables. One sample t-test was used for comparisons between mean morbidities. Logistic regression model was applied to determine the predictors the health-seeking behavior after adjusting for common confounders. Differences among groups were considered statistically significant at P more than 0.05 Ethical clearance was sought from the Institute Ethics Committee of Indira Gandhi Medical College, Shimla.
Results
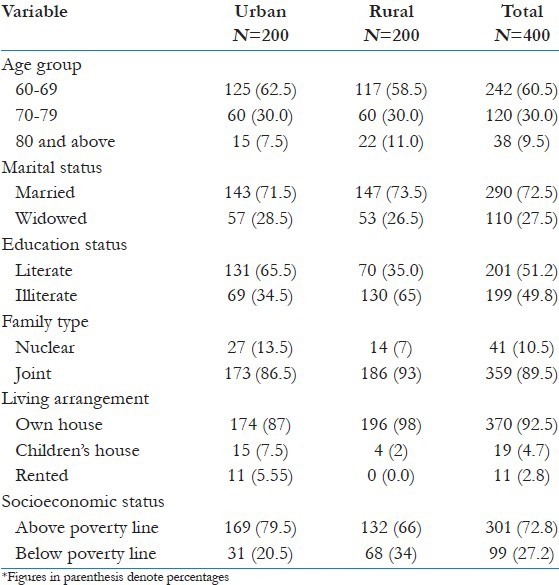
The mean age of the sample studied was 69.01 years, with age ranging from 60 to 90 years. The mean age of the study subjects in the urban areas was 68.5 years and in rural areas 69.5 years. Females represented 51% of the study sample. A total of 27.5% study participants were leading widowed life and 49.8% older persons were illiterate. Majority of the older persons (89.5%) were living in joint families. Most common living arrangement was living with spouse and children (65%) followed by living with children (24.8%) [Table 1].
Table 1.
Sociodemographic characteristics of the elderly study population of Shimla district of Himachal Pradesh
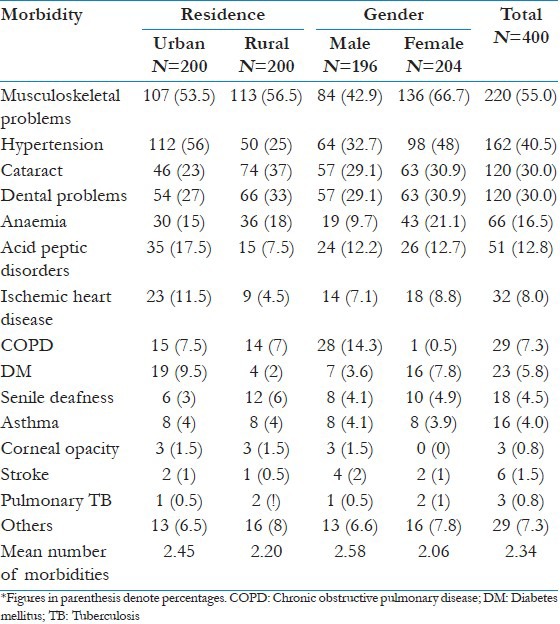
A large number of the subjects (84%) were suffering from at least one medical problem. Out of the 400 study subjects, 61 (15.3%) had one morbidity, 102 (25.5%) had two morbidities, 79 (19.7%) had three morbidities, and 94 (23.5%) had four to six morbidities. More women (88%) than men (80%) had at least one morbidity. The most frequent health problem was musculoskeletal problem, comprising 55% of the problems followed by hypertension in 40.5% of the older persons. Cataract and dental problems ranked third affecting 30% older persons. Anaemia comprised of the fourth morbidity affecting 16.5% of the study population. A significantly higher proportion of women suffered from musculoskeletal problems (females: 66.7% vs. males: 42.7%), hypertension (females: 48% vs. males: 32.7%), diabetes (females: 7.8% vs. males: 3.6%), while chronic obstructive pulmonary disease (males: 14.3% vs. females: 0.4%) was observed more in men. Hypertension was more prevalent in urban elderly (56%) as compared with rural counterparts (25%) [Table 2].
Table 2.
Prevalence of morbidity conditions stratified by residence and gender
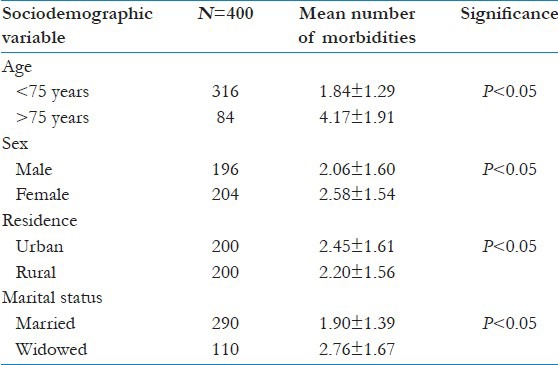
The mean number of morbidities among older persons in the present study was 2.34. There was higher mean number of morbidities in urban study subjects (2.45) as compared with rural study subjects (2.20). The mean number of morbidities increased with age. Females had more number of morbidities as compared with males. Widowed had more mean number of morbidities than married older persons [Table 3].
Table 3.
Relationship of mean number of morbidities with sociodemographic variables
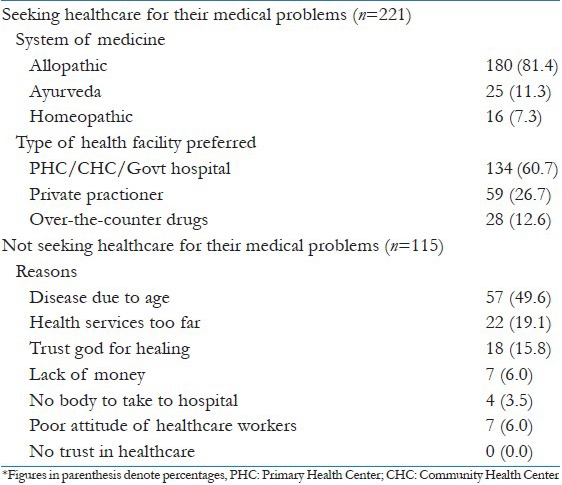
Nearly two third (65.8%) were seeking treatment for their health problems. Majority of the older persons preferred allopathic medicine (81.2%) followed by ayurvedic medicines (11.3%) and homeopathic medicine (7.3%) for their health problems. Most of the older persons preferred going to a PHC/CHC/Govt. hospital for treatment for their illness. There was considerable use of over-the-counter drugs (12.5%). Among older persons not seeking treatment for their medical condition, most considered these morbidities were an age-related phenomenon. Many perceived that the health services were too far [Table 4].
Table 4.
Distribution of study subjects by preference of system of medicine and reasons for not seeking healthcare among elderly
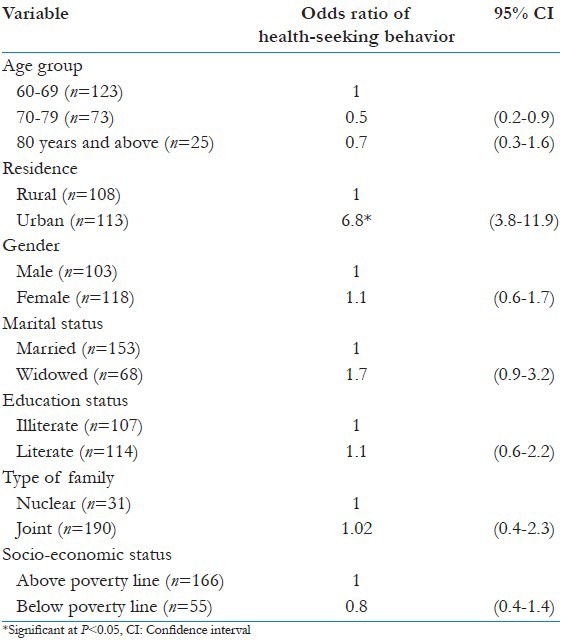
In the logistic regression model, significantly more elderly living in urban area (odds ratio = 6.7) were seeking healthcare for medical problems as compared with rural counterparts. Gender, literacy, income, and marital status were not found to be significantly related to health-seeking behavior [Table 5].
Table 5.
Multivariate logistic regression model for health-seeking behavior among elderly subjects
Discussion
The present community-based study recorded a high prevalence of morbidity (84%) in the study population. In agreement with our finding, studies carried out among older persons in Northern India,[7] Eastern India,[8] and North-east India,[9] have reported presence of high morbidity (88.9% and 88%, 68.5%, respectively). Studies from other countries[10,11,12,13] have reported presence of morbidity in 77%-95% of the older subjects. An important factor as to why morbidity pattern is high in the present study is the geography of the region. A hilly terrain may be scenic to the eyes, but it is a tough deal for those who dwell here. The hardships elderly face all their life translates into higher medical problems like musculoskeletal diseases. Another reason may be the socioeconomic problems and the literacy status. Many may evade cost of treatment and have some preconceived beliefs of aging which may increase multimorbidity in them.
Regarding health problems, more than half of older persons (55%) in the present study were suffering from musculoskeletal problems. This current data are consistent with other studies among older persons in India[14,15,16,17] and the world.[10,12,18,19] In the present study, hypertension was registered as the second most common morbidity (40.5%). Similar finding has been reported in a study among older persons in India[15,17] and abroad.[18,20] The presence of hypertension among the older persons in urban areas (56%) was about twice that in rural areas (25%). This might be explained by the fact that people in rural areas practice farming and manual labor and this lower the rate of obesity. This finding is similar to what was observed in a study by Liu et al.,.[21] The leading cause of diminished vision in developing countries is cataract, which was observed in 30% of the older persons in our study. Studies from India[22,23] and other countries[18,21] have observed cataract in 21%-37% of the older study subjects. In the present study, 30.0% of the older study subjects had dental problems. Comparable prevalence has been reported in other studies.[24,25]
Our study observed a significantly higher mean number of morbidities in urban study subjects as compared with rural counterparts. The mean numbers of morbidities were significantly higher among female elderly as compared with male elderly. Studies among older persons in India[24,25] and other countries[11,12] have reported similar finding. As older women were more likely than older men to be unemployed, and/or widowed, and to engage in less exercise, it is probable to explain their poorer health status in the study. In our study, we found the mean number of morbidities were significantly more in widowed older persons as compared with married subjects. Similar finding has been reported in a study by Shankar et al.,[8] in rural area of Varanasi which observed that compared to married people higher percentage of widowed suffered from more old age-related morbidities. The present study observed that with advancing age number of morbidities increased. This is in agreement with a study,[8] which observed that the prevalence of old age-related morbidities increased with advancing age significantly. Joshi et al.,[7] reported that the age was among the important factors which predict increased morbidity.
Logistic regression model result revealed that urban rural regional difference was the most important predictor of treatment-seeking behavior. This may be explained by better access to medical services in urban areas. We observed no gender and socioeconomic status differences in treatment-seeking practices. Similar observation was reported by Goswami et al. in their study.[23] In the present study, the main reason given by those older persons who were not taking medication for their health status was that they felt diseases are an expected part of aging. Goodwin et al.,[26] in a study on aging versus disease, the opinions of older persons; observed that substantial proportions of the subjects considered diseases to be a normal part of aging. Sarkisian et al.,[2,7] conducted a study on the association between expectations regarding aging and beliefs regarding healthcare-seeking behavior among older adults in Los Angeles and found that more than 50% of participants felt it was an expected part of aging to have more aches and pains. Contrary to our finding, a study among older persons in Nairobi reported that the main reason given by older persons for not seeking treatment for medical conditions was lack of money.[28]
The most common source of healthcare in our study was the government facility followed by private healthcare facility. We found that 12.6% of the older subjects were seeking over-the-counter drugs when ill. Similar observation was made in a study among elderly in India, which reported 10% of the older persons were seeking over-the-counter drugs.[23] Studies worldwide have documented high number of elderly seeking over-the-counter drugs for this illness.[28,29] The use of over-the-counter drugs is indicative of inefficient health facilities in meeting the health needs of the older persons.
Conclusions and Recommendations
The high morbidity load among elderly in the present study stresses for efforts to provide specialized healthcare to them, and thus ensure that they remain active members of our society. Elderly need help and support of the medical fraternity. Geriatric assessment should be done regularly. Among elderly; oldest old, female elderly, and widowed are the vulnerable group that need more attention.
Further, the study shows that elderly living in rural areas are the most vulnerable group in their healthcare-seeking behavior. To facilitate, this policy makers must focus more on rural elderly and their beliefs which prevent them from seeking healthcare. To tackle the issue of use of over-the-counter drugs, the existing laws should be strictly enforced and should govern the distribution of over-the-counter drugs. What this study adds is as follows:
This study adds to the growing body of literature on morbidity and health -seeking behavior of elderly in India.
High morbidity load among elderly in the present study stresses for efforts to provide specialized health care to them, and thus ensure that they remain active members of our society.
Elderly living in rural areas are the most vulnerable group in their healthcare-seeking behaviour.
Health care strategies specific to the elderly needs in the study area need to be formulated and tested.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Land KC, Lamb VL. Demography of Aging. In: Heggenhougen K, Stella Q, editors. International Encyclopedia of Public Health. Vol. 12. San Diego: Academic Press; 2008. pp. 89–95. [Google Scholar]
- 2.Situation analysis of elderly in India. 2011. [Last accessed on 2012 May 2]. Available from: http://mospi.nic.in/mospi_new/upload/elderly_in_india.pdf .
- 3.Research and study about old age. [Last accessed on 2012 May 2]. Available from: http://www.agewellfoundation.org/index.php?option=com_content and view=article and id=62 and Itemid=80 .
- 4.Population Aging: Facts, challenges, and responses. Working paper. 2011. [Last accessed on 2012 May 3]. Available from: http://www.hsph.harvard.edu/pgda/WorkingPapers/2011/PGDA_WP_71.pdf .
- 5.Kirkwood TB, Ritter MA. The interface between ageing and health in man. Age Ageing. 1997;26:9–14. doi: 10.1093/ageing/26.suppl_4.9. [DOI] [PubMed] [Google Scholar]
- 6.Grimley EJ. 21st Century: Review: Ageing and medicine. J Intern Med. 2000;247:159–67. doi: 10.1046/j.1365-2796.2000.00621.x. [DOI] [PubMed] [Google Scholar]
- 7.Joshi K, Kumar R, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. Int J Epidemiol. 2003;32:978–87. doi: 10.1093/ije/dyg204. [DOI] [PubMed] [Google Scholar]
- 8.Shankar R, Tondon J, Gambhir IS, Tripathi CB. Health status of elderly population in rural area of Varanasi district. Indian J Public Health. 2007;51:56–8. [PubMed] [Google Scholar]
- 9.Swain P. Health status among elderly in Northeast India. Journal of The Indian Academy of Geriatrics. 2007;3:8–14. [Google Scholar]
- 10.Cheng YH, Chi I, Boey KW, Ko LS, Chou KL. Self-rated economic condition and the health of elderly persons in Hong Kong. Soc Sci Med. 2002;55:1415–24. doi: 10.1016/s0277-9536(01)00271-4. [DOI] [PubMed] [Google Scholar]
- 11.Woo EK, Han C, Jo SA, Park MK, Kim S, Kim E, et al. Morbidity and related factors among elderly people in South Korea: Results from the Ansan Geriatric (AGE) cohort study. BMC Public Health. 2007;7:10. doi: 10.1186/1471-2458-7-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cacciatore F, Gallo C, Ferrara N, Abete P, Paolisso G, Canonico S, et al. Morbidity patterns in aged population in southern Italy. A survey sampling. Arch Gerontol Geriatr. 1998;26:201–13. doi: 10.1016/s0167-4943(98)00003-x. [DOI] [PubMed] [Google Scholar]
- 13.Fuchs Z, Blumstein T, Novikov I, Walter-Ginzburg A, Lyanders M, Gindin J, et al. Morbidity, co morbidity, and their association with disability among community-dwelling oldest-old in Israel. J Gerontol A Biol Sci Med Sci. 1998;53:447–55. doi: 10.1093/gerona/53a.6.m447. [DOI] [PubMed] [Google Scholar]
- 14.Sunder L, Chadha SL, Bhatia PC. A study on senior citizens in rural areas health for the millions. Health Millions. 1999;25:18–20. [Google Scholar]
- 15.Munshi YI, Iqbal M, Rafique H, Ahmad Z. Geriatric morbidity pattern and depression in relation to family support in aged population of Kashmir valley. Internet J Geriatr Gerontol. 2008;4:14–6. [Google Scholar]
- 16.Padda AS, Mohan V, Singh J, Deepti SS, Singh G, Dhillon HS, et al. Health profile of aged persons in urban and rural field practice areas of Medical College Amritsar. Indian J Commun Med. 1998;23:72–6. [Google Scholar]
- 17.Prakash R, Choudhary SK, Singh US. A study of morbidity pattern among geriatric population in an urban area of Udaipur, Rajasthan. Indian J Commun Med. 2004;29:35–40. [Google Scholar]
- 18.Graciani A, Banegas JR, López-García E, Rodríguez-Artalejo F. Prevalence of disability and associated social and health-related factors among the elderly in Spain: A population-based study. Maturitas. 2004;48:381–92. doi: 10.1016/j.maturitas.2003.10.004. [DOI] [PubMed] [Google Scholar]
- 19.Clausen F, Sandberg E, Ingstad B, Hjortdahl P. Morbidity and health care utilisation among elderly people in Mmankgodi village, Botswana. J Epidemiol Community Health. 2000;54:58–63. doi: 10.1136/jech.54.1.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kaplan MS, Huguet N, Feeny DH, McFarland BH. Self-reported hypertension prevalence and income among older adults in Canada and the United States. Soc Sci Med. 2010;70:844–9. doi: 10.1016/j.socscimed.2009.11.019. [DOI] [PubMed] [Google Scholar]
- 21.Liu Z, Albanese E, Li S, Huang Y, Ferri CP, Yan F, et al. Chronic disease prevalence and care among the elderly in urban and rural Beijing, China-a 10/66 Dementia Research Group cross-sectional survey. BMC Public Health. 2009;9:394. doi: 10.1186/1471-2458-9-394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kishore S, Garg BS. Sociomedical problems of aged population in a rural area of Wardha district. Indian J Public Health. 1997;41:43–8. [PubMed] [Google Scholar]
- 23.Goswami A, Reddaiah VP, Kapoor SK, Singh B, Dey AB, Dwivedi SN, et al. Health problems and health seeking behaviour of the rural aged. Indian J Gerontol. 2005;19:163–80. [Google Scholar]
- 24.Swami HM, Bhatia V, Dutt R, Bhatia SP. A community based study of morbidity profile among elderly in Chandigarh. Bahrain Med Bull. 2002;24:13–6. [Google Scholar]
- 25.Anil JP, Joy B, Malini KA, Vasudevan K, Veliath A, Panda P, et al. Morbidity pattern among the elderly population in the rural area of Tamil Nadu, India. Turk J Med Sci. 2006;36:45–50. [Google Scholar]
- 26.Goodwin JS, Black SA, Satish S. Aging versus disease: The opinions of older black, Hispanic, and non-Hispanic white Americans about the causes and treatment of common medical conditions. J Am Geriatr Soc. 1999;47:973–9. doi: 10.1111/j.1532-5415.1999.tb01293.x. [DOI] [PubMed] [Google Scholar]
- 27.Sarkisian CA, Hays RD, Mangione CM. Do older adults expect to age successfully? The association between expectations regarding aging and beliefs regarding healthcare seeking among older adults. J Am Geriatr Soc. 2002;50:1837–43. doi: 10.1046/j.1532-5415.2002.50513.x. [DOI] [PubMed] [Google Scholar]
- 28.Waweru LM, Kabiru EW, Mbithi JN, Some ES. Health status and health seeking behaviour of the elderly persons in Dagoretti division, Nairobi. East Afr Med J. 2003;80:63–67. doi: 10.4314/eamj.v80i2.8647. [DOI] [PubMed] [Google Scholar]
- 29.Abdulraheem IS. Health needs assessment and determinants of health-seeking behaviour among elderly Nigerians: A house-hold survey. Ann Afr Med. 2007;6:58–63. doi: 10.4103/1596-3519.55715. [DOI] [PubMed] [Google Scholar]