

Abstract
Aim:
To assess the prevalence of Early Childhood Caries (ECC) among preschool children of low socio- economic status in Bangalore city, India.
Materials and Methods:
A cross-sectional study was carried out among 566, 24–59 months old children attending various Anganwadi centers in Bangalore city, India, selected via cluster sampling. Caries experience was recorded using deft index (Greubbell, 1944). t Test, ANOVA, and Chi-square tests were used to find significant differences. P < 0.05 was considered as statistically significant.
Results:
Prevalence of Early Childhood Caries (ECC) was 37.3% with a mean deft of 1.90 ± 3.38 ranging from 0 to 17 teeth. Out of 211 children with ECC, 94.3% had severe Early Childhood Caries (s-ECC) with a mean deft score of 5.35 ± 3.77. All of the deft was due to untreated caries. Mean caries experience of 36–47 months age group was significantly higher than other groups (P = 0.024).
Conclusions:
The present study showed a 37.3% prevalence of ECC. There is a need for preventive and curative oral health programs in this section of the society.
Keywords: Children, early childhood caries, s-early childhood caries, prevalence, preschool
INTRODUCTION
Early childhood caries (ECC) is a serious sociobehavioral and dental problem that afflicts infants and toddlers.[1,2] The term ECC has been adopted to more accurately describe dental caries that affects primary dentitions, replacing previously used terminology that associated the disease with nursing habit. Significant percentages of preschool child population are affected by ECC today, with the disease concentrating disproportionately in deprived families.[3]
ECC can rapidly destroy the primary dentition of toddlers and small children and if left untreated, can lead to pain, acute infection, nutritional insufficiencies, and learning and speech problems.[4] The study of dental caries in primary dentition is important not only for the resulting deterioration in quality of life of young children, but also because dental caries in primary dentition is one of the best predictors of caries in the permanent dentition.[5,6]
ECC is a serious public health concern especially for social disadvantaged groups, in both developed and developing worlds. Yet, it remains relatively unexplored and poorly defined in many developing countries.[7]
India is no exception for the list. There is a lack of definite data on prevalence of ECC both at national and local levels. Hence, this study was undertaken with the aim of assessing prevalence of ECC among preschool children of low socioeconomic status in Bangalore city.
MATERIALS AND METHODS
A cross-sectional study was designed among preschool children belonging to low socioeconomic status in Bangalore city, India. The study was approved by the institutional ethical committee.
Study location
Children were selected from various anganwadi centers in Bangalore city, India. Permission and list of anganwadis was obtained from the Director, Women and Child Welfare Department, Bangalore. From that list, 25 anganwadis were selected via cluster sampling, covering the whole of Bangalore city.
Study subjects
All 24–59 months old children attending the 25 selected anganwadis, forming a total of 566 (279 boys and 287 girls). Informed consent was obtained from parents prior to the beginning of the study.
Dental examination
Clinical examination was carried out at anganwadi centers by a single calibrated examiner using mouth mirror and explorer under natural light, on an ordinary chair. Caries experience was recorded using deft index (Greubbell, 1944).[8] Caries of all the three-enamel, dentin, and pulp were included.
ECC case definition
For the purpose of this study, ECC cases were defined using AAPD criteria,[9] that is, presence of 1 or more decayed (noncavitated or cavitated lesion), missing (due to caries), or filled tooth surfaces in any primary tooth in a child 71 months of age or younger. From ages 3 through 5, 1 or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing, or filled score of ≥4 (age 3), ≥5 (age 4), or ≥6 (age 5) surfaces constitute s-ECC.
Statistical analysis
Data was analyzed using SPSS version 16.0 software. Chi-square, t test, and ANOVA were used to find significant age and genderwise differences. P value < 0.05 was considered as statistically significant.
RESULTS
Of the 566 children examined, 279 (49.3%) were boys and 287 (50.7%) were girls; 328(58%) were between 24 and 35 months, 214(37.8%) were between 36 and 47 months and 24 (4.2%) were between 48 and 59 months of age.
The prevalence of ECC was 37.3% (211 out of 566). Table 1 shows age and genderwise prevalence of ECC.
Table 1.
Age and genderwise prevalence of ECC

Out of 211(100%) with ECC, 110 (52.1%) were boys and 101 (47.9%) were girls. No significant gender differences were observed in percentage of ECC (χ2 = 1.085, P = 0.29). Whereas prevalence of ECC was significantly higher among 36–47 months old children as compared with other groups (χ2 = 14.03, P = 0.001).
Out of 211 with ECC, 199 (94.3%) had s-ECC, including 105 (52.8%) boys and 94 (47.2%) girls. Table 2 shows age and genderwise prevalence of s-ECC. No significant gender difference was found in percentage of s-ECC (χ2 = 0.55, P = 0.557). But prevalence of s-ECC was significantly higher among 24–35 months old children as compared with other groups (χ2 = 26.44, P = 0.000).
Table 2.
Age and genderwise prevalence of s-ECC

Table 3 shows mean caries experience of ECC and s-ECC cases.
Table 3.
Mean deft of ECC and s-ECC cases
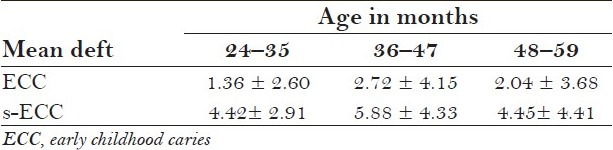
The overall mean deft for ECC was 1.90 ± 3.38 ranging from 0 to 17 teeth. t Test showed no significant differences in mean caries experience of boys and girls (P = 0.840). But mean deft was significantly higher in 36–47 months age group as compared with others (F = 10.89, P = 0.000).
The mean deft of s-ECC cases was 5.35 ± 3.77. Mean deft for s-ECC was significantly higher in 36–47 months age group as compared with others (F = 4.04, P = 0.019). Also, the mean deft of girls with s-ECC was significantly higher (5.33 ± 4.09) as compared with boys (4.90 ± 3.4), P = 0.024.
DISCUSSIONS
A total of 566, 24–59 months old children were examined for presence of ECC from over 25 Anganwadi centers in Bangalore city. Anganwadis are government run day care centers, which cater to the needs of children from 0 to 6 years of age of low socioeconomic status and most of them are located in slums in Bangalore. Anganwadis function from 10am to 2pm on all days and provide free food and informal education to these children. Hence, most of the children of preschool age belonging to low socioeconomic status attend anganwadis. As many studies have shown a high ECC prevalence in low income groups,[10,11] anganwadis were chosen for the study. A cluster sample was taken to cover the whole of Bangalore city.
Socioeconomic status was recorded from anganwadi registers. More than 70% of the parents were illiterates and worked as labourers and their per capita income ranged from Rs 500–1600 per month.
Gruebbell's index was used to record both cavitated and incipient carious lesions as studies have reported a fairly high percentage of noncavitated carious lesions in primary dentition.[12]
The prevalence of ECC in the present study was 37.3%. This is comparatively high compared with that in other places in India as per some Indian studies.[13,14,15] Studies in Udupi and Davangere showed a prevalence of 19.4% and 19.2%, respectively.[13,14] However, a study in Kerala showed a caries prevalence of 44% among 8–48 months old children.[15] The prevalence of ECC worldwide is highly variable ranging from 2.1% in Sweden to 85.5% in rural Chinese children according to a systematic review of Ismail and Sohn.[16] While the prevalence in USA is reported to be 11%–53.1%, the prevalence in UK is 6.8%–12%.[17] This could be attributed to differences in case definitions and diagnostic criteria of ECC apart from risk factors.
The present study has used AAPD criteria for defining ECC cases. Whereas many Indian studies have used the criterion, which considers decay on minimum two maxillary anterior teeth for considering it as ECC.[13,14,15] However, a study conducted at Haryana, India, on the prevalence of s-ECC among children below 5 years, which used the AAPD criteria for s-ECC showed a higher prevalence of s-ECC of 42.03%.[18]
An important finding of this study was that about 94.3% of children with ECC showed s-ECC and all the deft was due to untreated caries. There was not a single filled tooth and all the children required treatment. And another important finding is that all children in the 24–35 months age group who had caries, presented with s-ECC. This is indicative of a total lack of awareness about oral health among parents, lack of accessibility, and affordability for oral health care in this section of people. This is quite alarming, especially in a city like Bangalore with wide options for oral health care, including 4 government hospitals and more than a dozen dental colleges.
The present study showed a significant increase in the prevalence of ECC with increasing age ranging from 30.8% among 24–35 months old to 46.3% and 45.8% among 36–47 and 48–59 months old children, respectively. Some caries prevalence studies in Brazil, South Africa, and others have showed a similar pattern.[19] However, s-ECC was more prevalent in 24–35 months age group.
The mean caries experience of 36–47 months old children was significantly higher than in other groups (2.72 ± 4.15) But as the observed skewed distribution is well known for caries index, the present study also showed a high standard deviation. This could be due to the extreme deft scores with few children having a deft of 17 and their caries-free counterparts having zero deft.
Also, the mean deft for s-ECC cases was also significantly higher in 36–47 months age group with a mean caries experience of 5.88 ± 4.33. This is higher than the mean caries experience of children with s-ECC in Haryana (dmfs = 5.08 ± 5.56) as reported by a study.[18]
Many studies have shown a higher prevalence of ECC among girls than boys, which has not been significant.[18,19] The present study showed a higher prevalence among boys than girls, which did not reach significance. However, among the s-ECC cases, girls had a significantly higher mean deft (5.33 ± 4.09) than boys (4.90 ± 3.40).
In the present study, there could be a slight underestimation of caries experience. As the study was carried out at anganwadis with minimum instruments and light, few of the initial lesions may have been missed, especially on the proximal surfaces of the posteriors. And also because of limited mouth opening experienced with very young children, especially those between 2 and 3 years of age.
CONCLUSIONS
The present study shows an ECC prevalence of 37.3% among preschool children of low socioeconomic status in Bangalore and all of the deft is due to untreated caries indicating a high treatment need and lack of awareness about oral health in this section of the society. There is an urgent need to implement Preventive and Curative Oral health programs for children. As anganwadis are run by State Government, a public–private partnership between the government, Private Dental colleges, and NGOs would prove useful toward providing oral health care to these children.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Tsubouchi J, Tsubouchi M, Maynard RJ, Domoto PK, Weinstein P. A study of dental caries and risk factors among Native American infants. ASDC J Dent Child. 1995;62:283–7. [PubMed] [Google Scholar]
- 2.Douglass JM, Tinanoff N, Tang JM, Altman DS. Dental caries patterns and oral health behaviours in Arizona infants and toddlers. Community Dent Oral Epidemiol. 2001;29:14–22. [PubMed] [Google Scholar]
- 3.Vadiakas G. Case definition, aetiology and risk assessment of early childhood caries; A revisited review. Eur Arch Pediatr Dent. 2008;9:114–25. doi: 10.1007/BF03262622. [DOI] [PubMed] [Google Scholar]
- 4.Nunn ME, Brannstein NS, Krall keye EA, Dietrich T, Garcia RI, Henshaw MM. Healthy eating Index is a predictor of Early Childhood Caries. J Dent Res. 2009;88:361–6. doi: 10.1177/0022034509334043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Skeie MS, Raadal M, Strand GV, Espelid I. The relationship between caries in the primary dentition at 5 years of age and permanent dentition at 10 years of age-a longitudinal study. Int J Paediatr Dent. 2006;16:152–60. doi: 10.1111/j.1365-263X.2006.00720.x. [DOI] [PubMed] [Google Scholar]
- 6.Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth: An eight-year cohort study. J Dent Res. 2002;81:561–6. doi: 10.1177/154405910208100812. [DOI] [PubMed] [Google Scholar]
- 7.Postma TC, Ayo-Yusuf OA, van Wyk PJ. Socio-demographic correlates of early childhood caries prevalence and severity in a developing country- South Africa. Int Dent J. 2008;58:91–7. doi: 10.1111/j.1875-595x.2008.tb00182.x. [DOI] [PubMed] [Google Scholar]
- 8.Greubbell AO. A measurement of dental caries prevalence and treatment services for deciduous teeth. J Dent Research. 1944;23:163–8. [Google Scholar]
- 9.Vol. 31. Washington, DC: AAPD; 2008. Policy on ECC- Classification, consequences and Preventive Strategies; p. 6. 9,10. [Google Scholar]
- 10.Mouradian PW, Wehr E, Crall JJ. Disparities in children's oral health and access to dental care. JAMA. 2000;284:2625–31. doi: 10.1001/jama.284.20.2625. [DOI] [PubMed] [Google Scholar]
- 11.Jigjid B, Ueno M, Shinada K, Kawaguchi Y. Early childhood caries and related risk factors in Mongolian children. Community Dent Health. 2009;26:121–8. [PubMed] [Google Scholar]
- 12.Drury TF, Horowitz AM, Ismail AI, Maertens MP, Rozier RG, Selwitz RH. Diagnosing and reporting early childhood caries for research purposes. J Public Health Dent. 1999;59:192–7. doi: 10.1111/j.1752-7325.1999.tb03268.x. [DOI] [PubMed] [Google Scholar]
- 13.Tandon S, Sethi B. Caries pattern in pre-school children. J Am Dent Assoc. 1996;67:141–5. [Google Scholar]
- 14.Tyagi R. The prevalence of nursing caries in Davangere preschool children and its relationship with feeding practices and socioeconomic status of the family. J Indian Soc Pedod Prev Dent. 2008;26:153–7. doi: 10.4103/0970-4388.44030. [DOI] [PubMed] [Google Scholar]
- 15.Jose B, King NM. Early Childhood Caries Lesions in Preschool Children in Kerala, India. Pediatr Dent. 2003;25:594–600. [PubMed] [Google Scholar]
- 16.Martens L, Vanobbergen J, Willems S, Aps J, De Maeseneer J. Determinants of early childhood caries in a group of inner-city children. Quintessence Int. 2006;37:527–36. [PubMed] [Google Scholar]
- 17.Kumar VD. Early childhood caries-an insight. J Int oral Health. 2010;2:1–9. [Google Scholar]
- 18.Virdi M. Internet J Epidemiol. Haryana, India: 2010. Prevalence of severe early Childhood caries in pre-school children in Bahadurgarh; p. 8. [Google Scholar]
- 19.Rosenblatt A, Zarzar P. The prevalence of early childhood caries in 12- to 36-month-old children in Recife, Brazil. J Dent Child. 2002;69:319–24. [PubMed] [Google Scholar]