

Abstract
Objectives:
To assess the dental caries, periodontal health, and malocclusion of school children aged 12 and 15 years in Shimla city and to compare them in government and private schools.
Materials and Methods:
A cross-sectional study of 12- and 15-year-old children in government and private schools was conducted in Shimla city, Himachal Pradesh, India. A sample of 1011 school children (both males and females) was selected by a two-stage cluster sampling method. Clinical recordings of dental caries and malocclusion were done according to World Health Organization diagnostic criteria 1997. Periodontal health was assessed by Community Periodontal Index of Treatment Needs index. The data collected was analyzed by SPSS package 13. The statistical tests used were t-test and Chi-square tests.
Results:
The prevalence of dental caries was 32.6% and 42.2% at 12 and 15 years, respectively. At the12 years of age, the mean decayed, missing, filled teeth was 0.62 ± 1.42 and it was 1.06 ± 2.93 at 15 years of age. Females had higher level of caries than males at both the ages. At both ages, mean of decayed teeth was statistically higher in government schools as compared with private schools. Children in government schools had significantly less number of mean filled teeth at both ages as compared with private schools. The healthy component of gingiva was present in higher percentage of children in private schools as compared with government schools at both the age groups. The prevalence of malocclusion among the 12- year-old (58.1%) was more as compared with that among the 15-year-old (53.5%).
Conclusion:
The caries experience of 12- and 15-year-old children was low but the prevalence of gingivitis and malocclusion was quite high. Effective oral health promotion strategies need to be implemented to improve the oral health of school children further in Shimla city.
Keywords: Dental caries, school children, Shimla, treatment needs
INTRODUCTION
Good oral health is important because the experience of pain, problems with eating, chewing, smiling, and communication due to missing, discolored, or damaged teeth have a major impact on people's daily lives and well-being. Furthermore, oral diseases restrict activities at school, at work, and at home causing millions of school and work hours to be lost each year throughout the world.[1] Children who suffer from poor oral health are 12 times more likely to have more restricted activity days including missing school than those who do not.[2] Historically, most important global burdens of the oral health are dental caries and periodontal diseases.[1]
As dental caries is the most common dental disease with high prevalence, it is crucial to control the disease process by assessing and rendering the treatment required along with spreading awareness regarding its prevention. But for developing appropriate preventive approaches, anticipating utilization patterns, and planning effectively for organization and financing of dental resources, the knowledge of oral health status and treatment needs of populations with different characteristics is important.
The schools remain an important setting, offering an efficient and effective way to reach children worldwide and, through them, families and community members. School age is an influential stage in people's life when lifelong sustainable oral health related behaviors, as well as beliefs and attitudes, are being developed. Children are particularly receptive during this period and the earlier the habits are established, the longer lasting the impact. Moreover, the messages can be reinforced regularly throughout the school years.[3]
Various studies have been conducted in different parts of our country, but the literature is very scant for cross comparison in terms of caries status and treatment needs as well as the periodontal status of school children in India. As there are no earlier studies on oral health status of school going children aged 12 and 15 years in Shimla city, the present study was conducted with the following objectives:
To assess the dental caries, periodontal health, and malocclusion of school children aged 12 and 15 years in Shimla city
To compare the oral health status and treatment needs in government and private schools
To establish a reliable baseline data for development of national/regional oral health programs.
MATERIALS AND METHODS
A cross-sectional epidemiologic study was conducted among the school-going children aged 12 and 15 years in Shimla city. Ethical approval to conduct the study was obtained from the Institutional Review Board of H.P. Government Dental College and Hospital, Shimla. Written consent for the participation of the children in the study was obtained from the principals of the concerned schools.
A pilot study was conducted by randomly selecting one government and one private school from the available list of schools obtained from the Directorate of Education, H.P. Results from this pilot study showed the prevalence of dental caries was 23.4%. The sample size was calculated by taking this prevalence rate and computed using the Epi Info, Version 6 statistical package at 95% confidence interval which came out to be 985.
The sample frame consisted of middle and high schools (public and private) in Shimla city. The study sample was recruited by a two-stage cluster sampling technique. For the purpose of the study, Shimla city was arbitrarily divided into four geographical regions, which correspond to the four varying demographic areas of the city: Shimla municipal and three Shimla Planning Areas (Dhalli, Tutu, and New Shimla). Schools from each region were randomly selected to obtain the desired sample size, such that there was an equal representation from each of the four zones. Out of the total number (43) of government (26) and private schools (17), seven public and five private schools were randomly selected. In the second stage, eligible schoolchildren were stratified according to age and gender, and randomly selected in proportion to the total number of 12- and 15-year old students enrolled in each school to reach the sample of about 1011 subjects over a period of 3 months April-June 2009. The fluoride levels in water in Shimla city are less than 1.5.[4]
Data collection was carried out by one of the authors (SF) trained for clinical examination during several educational and clinical sessions in the Department of Public Health Dentistry, Government Dental College, Shimla. The author was assisted by an alert and co-operative recording assistant. Data regarding general information, oral hygiene practices were obtained through interview and recorded on a modified World Health Organization (WHO) proforma.[5] The various oral hygiene variables recorded were oral hygiene aids which included toothbrush, finger and tree sticks; oral hygiene material like tooth paste, toothpowder and others, and frequency of brushing that included once a day and twice a day.
The subjects were examined by Dunning type III[6] clinical examination for caries status and treatment needs, periodontal status and malocclusion in their respective schools on a comfortable chair. The procedure, diagnostic criteria, and treatment codes followed those recommended by WHO (1997)[5] for assessment of dental caries and its treatment needs and malocclusion. Clinical examination for periodontal health was done as per Community Periodontal Index of Treatment Needs (CPITN)[7] index. The periodontal indicators assessed were gingival bleeding and calculus for 12-year-old age group, while gingival bleeding, calculus, and periodontal pockets for 15 years. Intraexaminer reproducibility as determined using Kappa statistic was 0.85.
Inclusion criteria
School children (male and female) who have completed their 12 and 15 years of age.
Children present on the day of examination.
Exclusion criteria
Those children who refused to participate were excluded Medically compromised children.
Also, the children under going orthodontic treatment were excluded for analysis of malocclusion.
A referral was forwarded to the parents of the children in need of dental care. At the conclusion of the survey, an oral health education session and tooth brushing demonstration was conducted in each classroom.
Statistical analysis
The data collected was analyzed by Statistical Package for Social Sciences (SPSS) package 13. The statistical tests used were t-test for continuous variables and Chi-square tests for categorical data. A level of P ≤ 0.05 was considered statistically significant.
RESULTS
Of the total study population, 49.2% were in the 12 years age group and 50.8% were in the 15 years age group. Among the 12-year age group, there were 322 (64.8%) males and 175 (35.2%) females, while in the 15-year age group there were 304 (59.2%) males and 210 (40.8%) females. Among the 12-year age group, 46.1% of children were in government schools and 53.9% of children were in private schools, whereas in the age group of 15 years 48.6% of the children were in government schools and 51.4% were in private schools.
A total of 100% of the children in private schools used toothbrush and tooth paste as compared with government schools (95.4% used tooth brush and 93.6% used tooth paste) and the difference was statistically significant, P < 0.001. The frequency of brushing twice a day was statistically higher in private schools than government schools.
The prevalence of dental caries at 12 years was 32.6% and at the age of 15 years it was 42.2%. The prevalence of dental caries in government schools was 41.9% and in private schools it was 33.5% and the difference was statistically significant (P < 0.01).
At the age of 12 years, the mean decayed, missing, filled teeth (DMFT) was 0.62 ± 1.42 and it was 1.06 ± 2.93 at the age of 15 years. The difference at two age groups was statistically significant (P < 0.001). At both the age groups, females showed higher mean DMFT as compared with the males and difference is statistically significant at 12 years. Subjects brushing their teeth once a day had higher mean DMFT as compared to those who brush twice a day and the difference is statistically significant at 12 years [Table 1]. Females had higher number of mean decayed teeth (0.65) than males (0.44) which is statistically significant. At both ages, mean of decayed teeth was statistically higher in government schools as compared with private schools. Children in government schools had less number of mean filled teeth at both ages as compared with private schools and the difference was statistically significant.
Table 1.
Mean caries experience (DMFT) in relation to age, gender, schools, brushing frequency
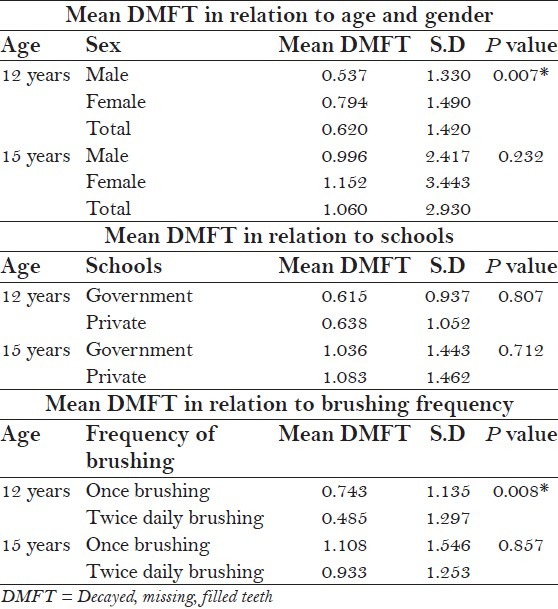
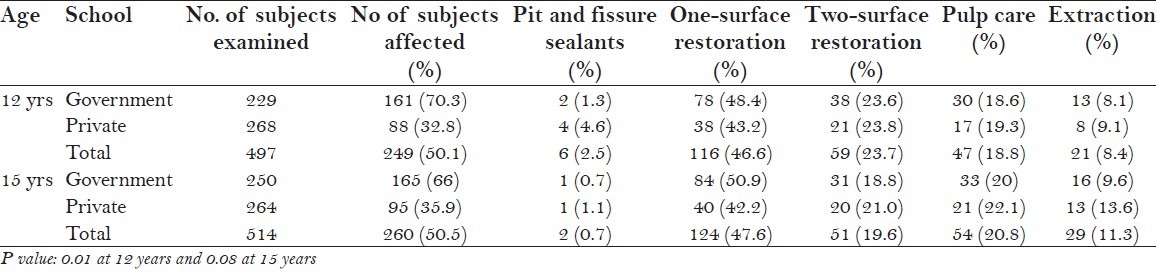
Table 2 shows that at the age of 12 years, 50.1% of children required restorative and endodontic treatment and at the age of 15 years, 50.5% of children required restorative and endodontic treatment. The greatest need was for single surface restorations (46.6% in 12 years and 47.6% in 15 years). The treatment need was higher in government schools at both the age groups but significantly higher at 12 years (P < 0.01).
Table 2.
Assessment of treatment needs among study population according to age and schools
There was significant age difference regarding CPITN scores. The percent of children with healthy component of gingiva was higher at 15 years of age than 12 years. Higher percentage of children had calculus at 15 years as compared with 12 years.
At the age of 12 years, majority of the subjects (75.4%) had a score of 1 (bleeding gums) and 14.1% had healthy periodontium, while at the age of 15 years, 57.0%had a score of 1 (bleeding gums), 18.9% had healthy periodontium, 18.7% had a score of 2 and 5.4% had a score of 3 and no one had a score of 4 [Table 3].
Table 3.
CPITN scores in relation to age, gender, and schools
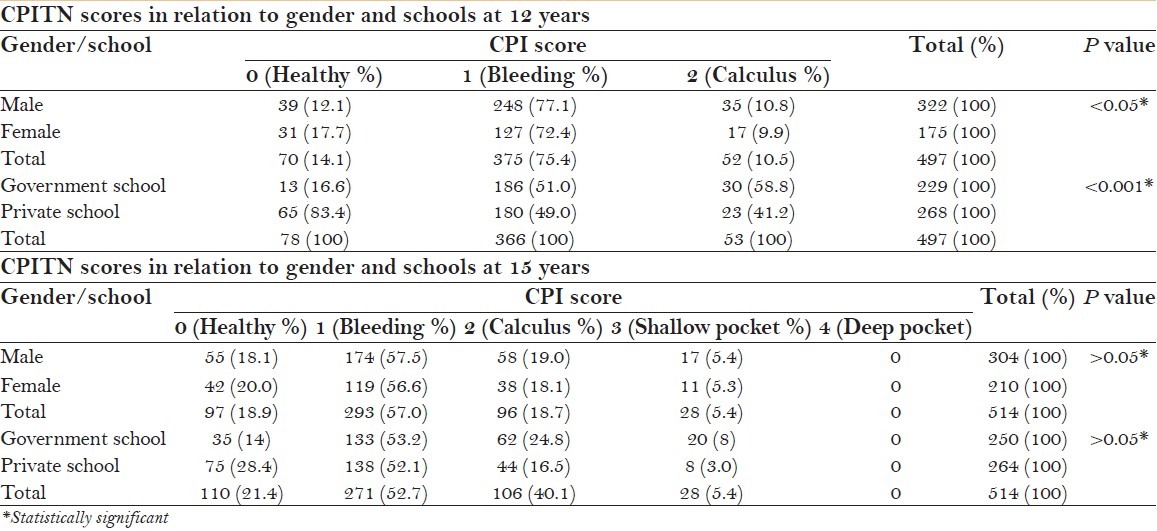
At both the age groups, higher percentages of children were having healthy sextants in private schools as compared with government schools. At 12 years, there was statistically higher percentage of children having calculus in government schools as compared with private. At the age of 15 years, there was a significant correlation between frequency of brushing and CPITN scores [Table 3].
A total of 48 children (4.7%) had already undergone or were undergoing orthodontic treatment at the time of examination and these subjects were excluded for analyzing Dental Aesthetics Index (DAI) score. It was observed that a highly significant difference existed in the number of children seeking orthodontic treatment between government and private schools in favor of private schools (P < 0.001). The prevalence of malocclusion among the 12-year-old (58.1%) was more as compared with that among the 15-year-old (53.5%). The severity percentages of malocclusion as per DAI index are shown in Table 4.
Table 4.
Prevalence of malocclusion severity according to DAI scores
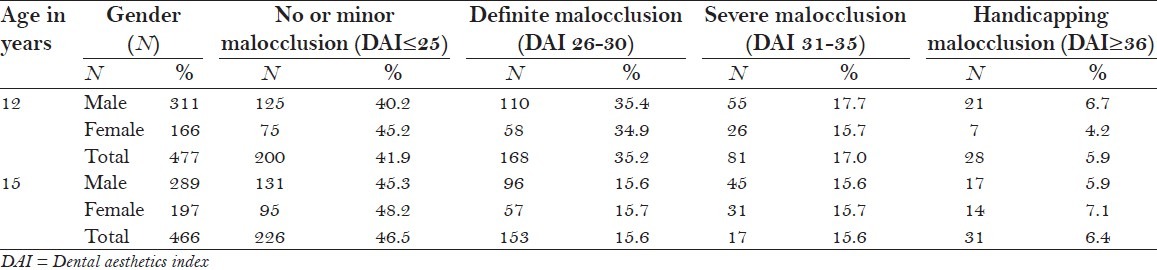
The percentage of subjects with “no or minor malocclusion” increased from 41.9% (40.2% males and 45.2% females) at 12 years to 46.5% (45.3% males and 48.2% females) at 15 years. At both ages, malocclusion was more in males than in females [Table 4].
DISCUSSION
A cross-sectional study was carried out to assess the oral health status and treatment needs among school children in Shimla city, Himachal Pradesh, India. The 12 and 15 age groups were chosen for this study, as these are global monitoring ages for dental caries for international comparisons and monitoring of disease trends. The present study sample consisted of school children from both public and private schools in order to have representation of children from all the social, economic, and cultural communities.
At both the age groups, around 97% of population used tooth brush and tooth paste for cleaning their teeth. This clearly indicates their awareness about oral hygiene. At the age of 12 years, most of them (64%) used to brush once a day which is in line with the findings of Joshi and Rajesh,[8] but high as compared with findings of Harikiran and Pallavi[9] and Peng et al.,[10] and less as compared with Petersen et al.,[11] The frequency of brushing twice was more common in private schools as compared with government schools which was also reported by Kumar et al.,[12] Tanni,[13] and Petersen.[14] In the present study, as the frequency of brushing increased prevalence of dental caries decreased. Similarly, with the increase in the frequency of brushing the prevalence and severity of periodontal diseases decreased. The reason being obvious, that there is significant corelation between plaque retention and gingival inflammation.[15]
In the present study, it was observed that the prevalence of dental caries was higher at the age of 15 years (42.2%) as compared with 12 years (32.6%) which was also reported by Rodrigues and Damle,[16] Singh et al.,[17] Naidu et al.,[18] and Goyal et al.[19] The reason for the higher prevalence of dental caries at 15 years as compared with 12 years is that caries being a continuous and cumulative process had obviously increased with a span of 3 years, as well as the number of teeth increases at the age of 15 years.
In the present study, the mean DMFT at 12 years and at 15 years was 0.62 and 1.06, respectively which was also reported by Naidu et al.,[18] and Petersen and Kaka,[20] but is less than 2.4 as reported by National Oral Health Survey in H.P.[4] Females had a significantly higher mean DMFT value than males. This is in line with the findings of Al Shammery and Guile,[21] Dummer et al.,[22] Sogi and Bhaskar,[23] and Singh et al.[17] This may be due to the fact that teeth erupt earlier in females than males which lead to prolonged exposure of the teeth to the oral environment in females.
At both the age groups, there was statistically significant difference in mean DMFT between the government and the private schools. The level of caries was higher in children attending government schools which is in line with the findings of Almeida et al.,[24] but in contrast to results reported by Tanni,[13] Ojofeitimi et al.,[25] This may be due to lack of awareness, affordability, or underutilization of dental care facilities by the children in the government schools. So, further studies are needed to assess the various barriers for utilization of services.
The mean filled teeth and missing due to other reasons were high in private schools which may be attributed to parents’ attitude and dental awareness, of children in private schools which is reflected in the child's oral health maintenance. The mean of missing teeth due to other reasons was higher in private schools probably due to intervention with orthodontic treatment in these children.
At the age of 12 years, gingivitis was the main finding in about 70% of children which was also reported by Petersen et al.,[11] and Kumar et al.,[12] but is less as compared to the results reported by Dhar et al.,[26] (85%) and Addy et al.,[27] The higher proportion of gingival bleeding may be due to mixed dentition period, shedding of primary teeth, and pubertal changes in girls.
The overall high prevalence of gingivitis at both the age groups may be due to ineffective oral hygiene measures. As the present study showed that about 97% used tooth brush, but the gingivitis present in most of the school children reflects irregular brushing methods which can be due to inadequate brushing time, ineffective brushing technique, or both factors, or it may also be possible that some of the children did not brush as they claim. Data collected through interviewing has limitations, so over reporting is possible regarding use of tooth brushing.
It was found that the children in private schools had higher proportion of healthy gingiva as compared with government schools which was also reported by Kumar et al.[12] This may be due to somewhat irregular oral hygiene practices in government school children.
A total of 41.9% of the population at 12 years and 46.5% at 15 years presented no or minor malocclusion, indicating no or slight need for treatment which was also reported by Jenny et al.,[28] The severity levels of malocclusion assessed to be 35.2% definite malocclusion with elective need for orthodontic treatment at 12 years; and 15.6% at 15 years, and 17.0% severe malocclusion at 12 years and 15.6% at 15 years; and 5.9% % handicapping malocclusion at 12 years and 6.4% at 15 years with mandatory orthodontic treatment need are similar to the results reported by Chi et al.,[29] and Jenny and Cons.[30]
There was no significant gender difference in DAI scores, though girls had a slightly lower score at 12 years age as compared with boys. This is comparable with the reports of Otuyemi et al.,[31] which did not find any significant sex differences in the mean DAI score of Nigerian children.
The limitation of the present study was that the socioeconomic status of the subjects could not be assessed because the children could not be relied upon for this information and the collection of information from the school was not feasible.
CONCLUSION
From the present study, it is concluded that the prevalence of dental caries at the age of 12 years was 32.6% and 42.2% at the age of 15 years. The mean DMFT was 0.06 at the age of 12 years and 1.02 at the age of 15 years, which means that caries prevalence in 12- and 15-year-old children in Shimla city falls within the “very low” category as defined by the WHO. Dental caries was higher in government schools as compared with private schools. The maximum need was for one-surface restoration in both the age groups. Gingivitis was higher at the age of 12 years as compared with 15 years. The children in the private schools had higher proportion of healthy gingival as compared with government schools. The prevalence of malocclusion among the 12-year-old was more as compared with that among the 15-year-old. As to improve the oral health of children in Shimla, the following recommendations are given:
Oral health promotion through well-structured oral health education program can create positive change in awareness for special groups like school children
Reinforcement of knowledge is necessary which can be done by incorporating chapters on oral health and oral hygiene in school textbooks. Also, the teachers training programs can ensure continuity of reinforcement
Implementation of school dental health programs focusing on preventive programs like fluoride mouth rinse and tooth brushing programs
Preventive services should be given high priority and needs to be started at an early age to target the primary dentition and future caries in permanent dentition
Regular interval screening programs to assess the oral health and treatment needs of school children and provision of treatment as per the need.
ACKNOWLEDGMENT
The authors would like to thank Mrs. Kusum Chopra, Statistician, without whose valuable input, this work would not have been possible.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Petersen PE, Bourgeois D, Hiroshi O. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83:661–9. [PMC free article] [PubMed] [Google Scholar]
- 2.Geneva: Oral Health Promotion: An essential element of a health promoting school; 2003. WHO Information Series on School Health Document Eleven. [Google Scholar]
- 3.Kwan SY, Petersen PE, Pine CM, Borutta A. Health Promoting schools: An opportunity for oral health promotion. Bull World Health Organ. 2005;83:677–85. [PMC free article] [PubMed] [Google Scholar]
- 4.India: 2002-2003. DCI Publication. National Oral Health Survey and Fluoride Mapping. [Google Scholar]
- 5.Basic Methods. 4th ed. Geneva: 1997. World Health Organization. Oral Health Surveys; pp. 26–9. [Google Scholar]
- 6.Dunning JM. 4th ed. Cambridge: Harvard University Press; 1986. Principles of Dental Public Health; pp. 132–3. [Google Scholar]
- 7.Cutress TW, Ainamo J, Sardo-Infirri J. The community periodontal index of treatment needs (CPITN) procedure for population groups and individuals. Int Dent J. 1987;37:222–32. [PubMed] [Google Scholar]
- 8.Joshi N, Rajesh R. Prevalence of dental caries among school children in Kulasekharam village: A correlated prevalence survey. J Indian Soc Pedod Prev Dent. 2005;23:138–40. doi: 10.4103/0970-4388.16887. [DOI] [PubMed] [Google Scholar]
- 9.Harikiran AG, Pallavi SK, Hariprakash S, Ashutosh, Nage KS. Oral health-related KAP among 11- to 12-year-old school children in a government-aided missionary school of Bangalore city. J Dent Res. 2008;19:236–42. doi: 10.4103/0970-9290.42957. [DOI] [PubMed] [Google Scholar]
- 10.Peng B, Petersen PE, Fan MW, Tai BJ. Oral health status and oral health behaviour of 12-year-old urban schoolchildren in the People's Republic of China. Community Dent Health. 1997;14:238–44. [PubMed] [Google Scholar]
- 11.Petersen PE, Hoerup N, Poomviset N, Prommajan J, Watanapa A. Oral health status and oral health behaviour of urban and rural schoolchildren in Southern Thailand. Int Dent J. 2001;51:95–102. doi: 10.1002/j.1875-595x.2001.tb00829.x. [DOI] [PubMed] [Google Scholar]
- 12.Mahesh Kumar P, Joseph T, Varma RB, Jayanthi M. Oral health status of 5 years and 12 years school going children in Chennai city–An epidemiological study. J Indian Soc Pedod Prev Dent. 2005;23:17–22. doi: 10.4103/0970-4388.16021. [DOI] [PubMed] [Google Scholar]
- 13.Tanni DQ. Caries prevalence and periodontal treatment needs in public and private school pupils in Jordan. Int Dent J. 1997;47:100–4. doi: 10.1111/j.1875-595x.1997.tb00683.x. [DOI] [PubMed] [Google Scholar]
- 14.Petersen PE, Wierzbicka M, Szatko F, Dybizbanska E, Kalo I. Changing oral health status and oral health behaviour of school children in Poland. Community Dent Health. 2002;19:243–50. [PubMed] [Google Scholar]
- 15.Kurt A, Rosenzwe G, Anselm L. Oral diseases in Yushiva students. J Dent Res. 1961;5:903–8. [Google Scholar]
- 16.Rodrigues JS, Damle SG. Prevalence of dental caries and treatment need in 12-15 year old municipal school children of Mumbai. Indian Soc Pedod Prev Dent. 1998;16:31–6. [PubMed] [Google Scholar]
- 17.Singh AA, Singh B, Kharbanda OP, Shukla DK, Goswami K, Gupta S. A study of dental caries in school children from Rural Haryana. J Indian Soc Pedod Prev Dent. 1999;17:24–8. [PubMed] [Google Scholar]
- 18.Naidu R, Prevatt I, Simeon D. The oral health and treatment needs of schoolchildren in Trinidad and Tobago: Findings of a national survey. Int J Paediatr Dent. 2006;16:412–8. doi: 10.1111/j.1365-263X.2006.00755.x. [DOI] [PubMed] [Google Scholar]
- 19.Goyal A, Gauba K, Chawla HS, Kaur M, Kapur A. Epidemiology of dental caries in Chandigarh school children and trends over the last 25 years. J Indian Soc Pedod Prev Dent. 2007;25:115–8. doi: 10.4103/0970-4388.36559. [DOI] [PubMed] [Google Scholar]
- 20.Petersen PE, Kaka M. Oral health status of children and adults in the Republic of Niger, Africa. Int Dent J. 1999;49:159–64. doi: 10.1002/j.1875-595x.1999.tb00901.x. [DOI] [PubMed] [Google Scholar]
- 21.Shammery A, Guile EF. Prevalence of caries in primary school children in Saudi Arabia. Community Dent Oral Epidemiol. 1990;18:320–1. doi: 10.1111/j.1600-0528.1990.tb00089.x. [DOI] [PubMed] [Google Scholar]
- 22.Dummer MH, Addy M, Hicks R, Kingdom A. The effect of social class on the prevalence of caries, plaque, gingivitis and pocketing in 11-12 year old children in South Wales. J Dent. 1987;15:185–90. doi: 10.1016/0300-5712(87)90107-2. [DOI] [PubMed] [Google Scholar]
- 23.Sogi G, Bhaskar DJ. Dental caries and oral hygiene status of 13-14 year old school children of Davangere. J Indian Soc Pedod Prev Dent. 2001;19:113–7. [PubMed] [Google Scholar]
- 24.Almeida CM, Petersen PE, André SJ, Toscano A Changing oral health status of 6- and 12-year-old schoolchildren in Portugal. Community Dent Health. 2003;20:211–6. [PubMed] [Google Scholar]
- 25.Ojofeitimi EO, Hollist NO, Banjo T, Adu TA. Effect of cariogenic food exposure on prevalence of dental caries among fee and non-fee paying Nigerian schoolchildren. Community Dent Oral Epidemiol. 1984;12:274–7. doi: 10.1111/j.1600-0528.1984.tb01454.x. [DOI] [PubMed] [Google Scholar]
- 26.Dhar V, Jain A, Van Dyke TE, Kohli A. Prevalence of gingival diseases, malocclusion and fluorosis in school-going children of rural areas in Udaipur district. J Indian Soc Pedod Prev Dent. 2007;25:103–5. doi: 10.4103/0970-4388.33458. [DOI] [PubMed] [Google Scholar]
- 27.Addy M, Dummer PM, Hunter ML, Kingdon A, Shaw WC. The effect of toothbrushing frequency, toothbrushing hand, sex and social class on the incidence of plaque, gingivitis and pocketing in adolescents: A longitudinal cohort study. Community Dent Health. 1990;7:237–47. [PubMed] [Google Scholar]
- 28.Jenny J, Cons NC, Kohout FJ, Jakobsen J. Differences in need for orthodontic treatment between Native Americans and the general population based on DAI scores. J Public Health Dent. 1991;51:234–8. doi: 10.1111/j.1752-7325.1991.tb02221.x. [DOI] [PubMed] [Google Scholar]
- 29.Chi J, Johnson M, Harkness M. Age changes in orthodontic treatment need: A longitudinal study of 10- and 13-year-old children, using the Dental Aesthetic Index. Aust Orthod J. 2000;16:150–6. [PubMed] [Google Scholar]
- 30.Jenny J, Cons NC. Establishing malocclusion severity levels on the Dental Aesthetic Index (DAI) scale. Aust Dent J. 1996;41:43–6. doi: 10.1111/j.1834-7819.1996.tb05654.x. [DOI] [PubMed] [Google Scholar]
- 31.Otuyemi OD, Ogunyinka A, Dosumu O, Cons NC, Jenny J. Malocclusion and orthodontic treatment need of secondary school students in Nigeria according to the dental aesthetic index (DAI) Int Dent J. 1999;49:203–10. doi: 10.1111/j.1875-595x.1999.tb00523.x. [DOI] [PubMed] [Google Scholar]