

Abstract
Background
Acute promyelocytic leukemia (APL) is an acute myeloid leukemia (AML) subtype with distinctive cell morphology, molecular presentation, clinical course, and treatment. About 90% of APL patients present with hemorrhagic complications due to disseminated intravascular coagulation (DIC). When APL is suspected, all-trans retinoic acid (ATRA) treatment is recommended even before confirmation by molecular tests. Specific criteria for differentiating unconfirmed APL from other AML subtypes with DIC are currently lacking. We aimed to achieve the early diagnosis of APL from other AML types with DIC by restricting the DIC criteria.
Methods
We retrospectively analyzed 29 patients newly diagnosed with AML accompanied by DIC from January 2005 to January 2013.
Results
Fibrin degradation products (FDP) (77.7 µg/mL vs. 23.7 µg/mL, p=0.026), D-dimer (7,376.2 ng/mL vs. 1,315.2 ng/mL, p=0.018), and TIBC (264.4 µg/dL vs. 206.8 µg/dL, P=0.046) were higher, while fibrinogen (133.8 mg/dL vs. 373.2 mg/dL, p<0.001), WBC (14.988×109/L vs. 70.755×109/L, p=0.015), and ESR (7.1 mm/h vs. 50.0 mm/h, p <0.001) were lower in APL patients than in the patients with other AML subtypes. FDP ≥27 µg/mL, D-dimer ≥2,071 ng/mL, and fibrinogen ≤279 mg/dL were our threshold values. These markers may be characteristic to APL and helpful in presumptive diagnosis.
Conclusion
APL may be differentiated from other AML subtypes by core markers of DIC (FDP, D-dimer, and fibrinogen). We suggest that clinicians set new diagnostic thresholds by restricting the DIC criteria. These findings support the early initiation of ATRA, prior to confirmation by PML-RARA molecular testing.
Keywords: Acute myeloid leukemia, Acute promyelocytic leukemia, Disseminated intravascular coagulation
INTRODUCTION
Acute promyelocytic leukemia (APL) accounts for 10% of the total number of acute myeloid leukemia (AML) cases. APL patients have cellular structures that are distinct from those observed in patients with other AML subtypes; further APL is accompanied by translocations in chromosomes 15 and 17 that result in a fused protein [1, 2]. Clinically, APL has a high frequency of hemorrhage due to disseminated intravascular coagulation (DIC), which contributes to the high mortality rate of this disease [2, 3]. In contrast to the treatment for other subtypes of leukemia, all-trans retinoic acid (ATRA) has been used in the early-stage treatment of APL since the 1980s. After the introduction of the ATRA treatment, complete remission and patient survival rates have increased, with many reports demonstrating complete remission in over 90% of patients. ATRA can induce the differentiation of APL cells, which decreases the frequency of coagulopathy [4]. Because of this, when APL is suspected based on cell morphology, immunophenotype, and/or coagulopathy with a positive DIC screen, physicians recommended prompt ATRA treatment before confirmation by chromosomal diagnosis [1, 5]. However, most patients with other types of AML exhibit cytopenia with DIC due to severe infection. Further, data on the differences in the patterns of laboratory characteristics including the DIC profile of patients with suspected APL and other types of AML with DIC are lacking.
MATERIAL AND METHODS
Patients
We retrospectively analyzed 29 patients newly diagnosed with AML accompanied by DIC at Chosun University hospital from January 2005 to January 2013. Blood tests were performed for all patients at admission to establish the diagnostic criteria for DIC. Fourteen patients were diagnosed with APL and the other 15 patients were diagnosed with other subtypes of AML. The APL patients were diagnosed based on the translocations in chromosomes 15 and 17.
Diagnosis
Diagnostic criteria for DIC
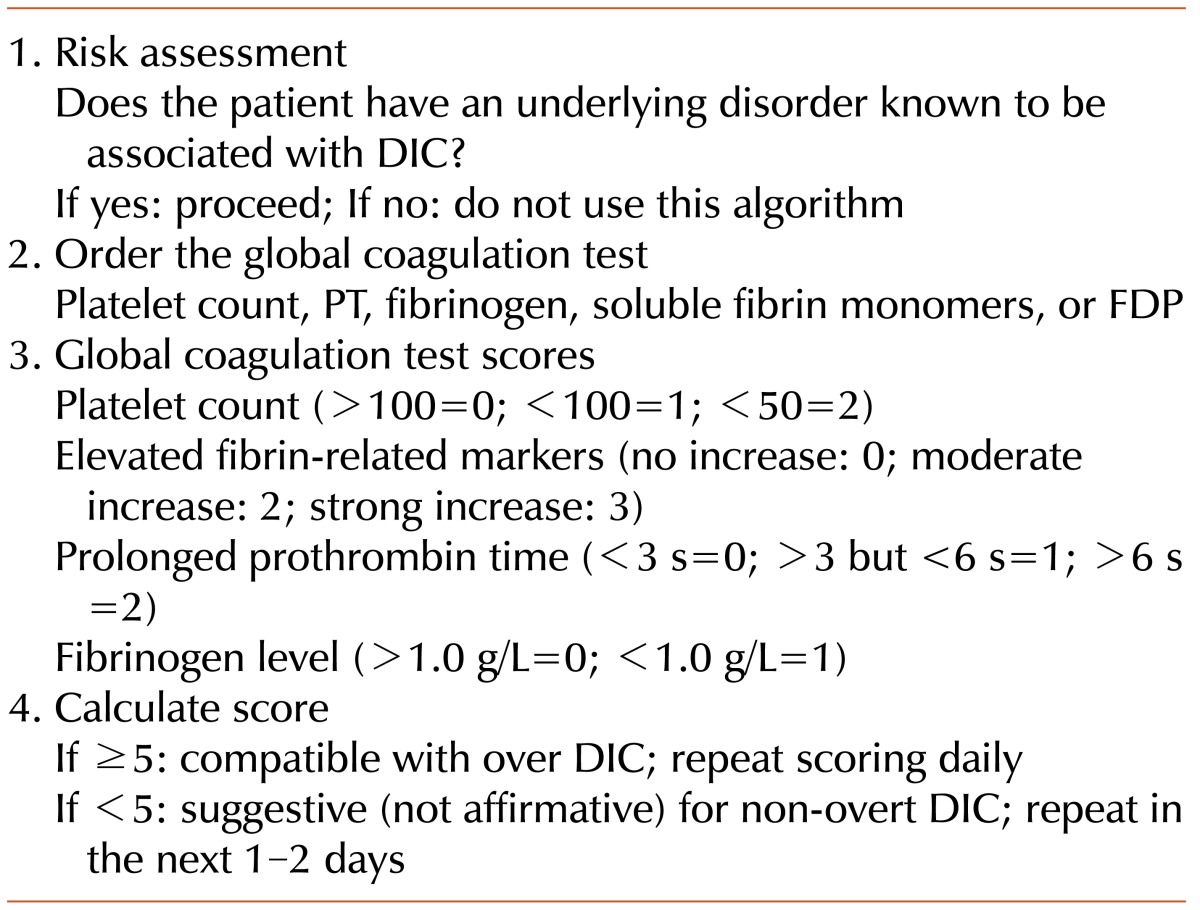
DIC was diagnosed using the overt DIC criteria of the International Society on Thrombosis and Hemostasis. The DIC score for all patients in this study was calculated based on the assumption that they had risk factors for DIC (Table 1) [6, 7].
Table 1.
Overt DIC criteria (International Society on Thrombosis and Hemostasis, 2001).
Statistical analyses
SPSS software 21.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Independent sample T test was used to compare the 2 groups and a P value less than 0.05 was considered statistically significant. Receiver operating characteristics (ROC) curve was used to set the diagnostic cut-off value for the blood test.
RESULTS
Characteristics of patients
The 14 patients (5 men and 9 women) diagnosed with APL were aged 28-79 years (mean age, 49.3 years). The 15 patients (9 men and 6 women) who were diagnosed with other subtypes of AML with DIC were aged 20-79 years (mean age, 57.5 years). There was no significant difference between the ages or genders of the 2 groups (Table 2).
Table 2.
Comparison of the findings between APL patients and patients with other AML subtypes with DIC.
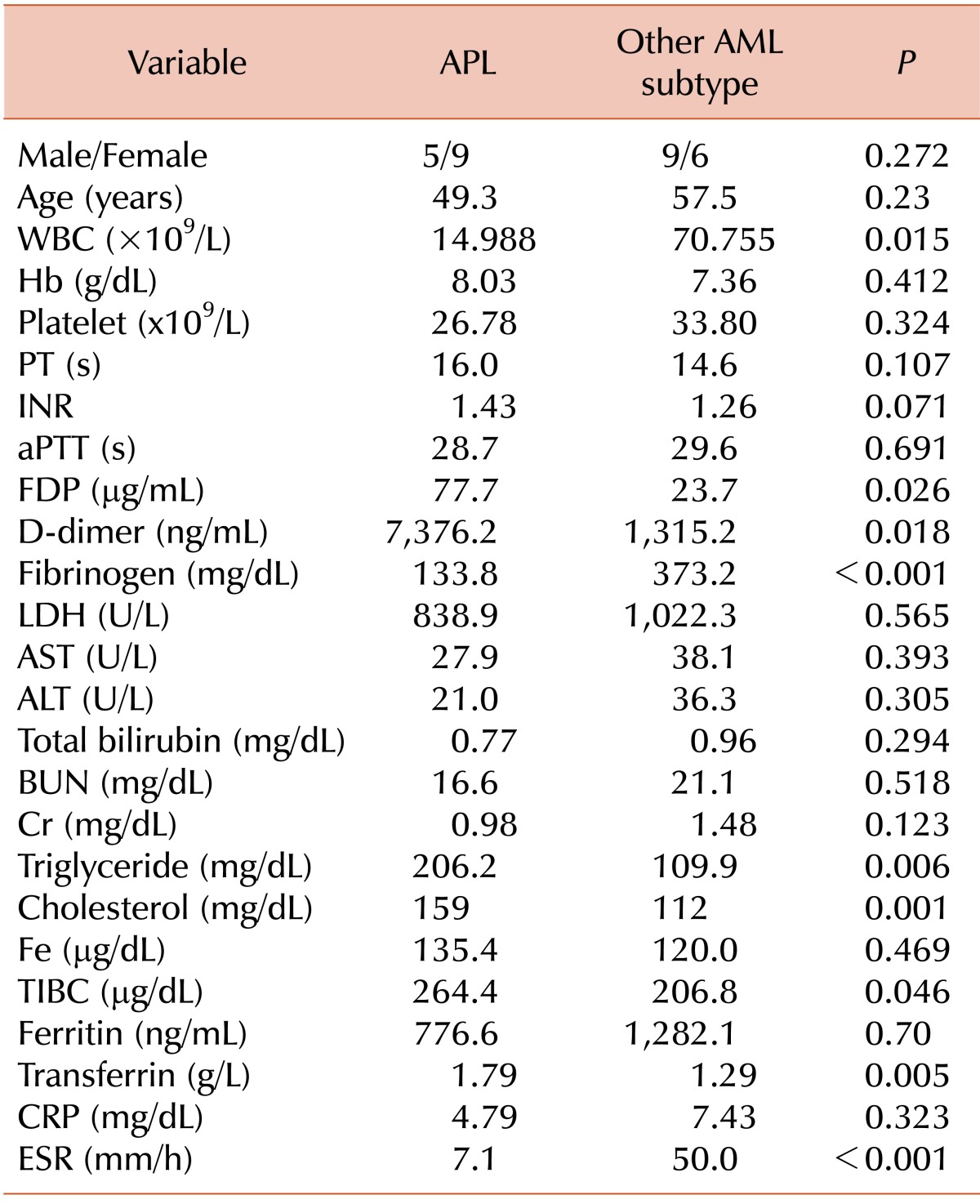
Abbreviations: APL, acute promyelocytic leukemia; AML, acute myeloid leukemia; DIC, disseminated intravascular coagulation; WBC, white blood cell; Hb, hemoglobin; PT, prothrombin time; INR, international normalized ratio; aPTT, activated partial thromboplastin time; FDP, fibrin degradation product; LDH, lactate dehydrogenase; AST, aspartate transferase; ALT, alanine transferase; BUN, blood urea nitrogen; Cr, creatinine; Fe, ferrous iron; TIBC, total iron binding capacity; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
Results of blood tests, including those for DIC
There was a significant difference in the mean number of leukocytes (WBC) between the APL group and the other AML group (APL: 14.988×109/L vs. AML: 70.755×109/L, P =0.015). However, there was no significant difference in the number of platelets (APL: 26.78×109/L vs. AML: 33.80×109/L, P =0.324) or the hemoglobin levels (APL: 8.03 g/dL vs. AML: 7.36 g/dL, P =0.412). There were significant differences in fibrin degradation product (FDP) (APL: 77.7 µg/mL vs. AML: 23.7 µg/mL, P =0.026), D-dimer (APL: 7,376.2 ng/mL vs. AML: 1,315.2 ng/mL, P =0.018), and fibrinogen (APL: 133.8 mg/dL vs. AML: 373.2 mg/dL, P <0. 001) levels. However, there was no significant difference in the prothrombin time (PT) (APL: 16.0 s vs. AML: 14.6 s, P =0.107) or the international normalized ratio (INR) (APL: 1.43 vs. AML: 1.26, P =0.071). Other laboratory findings that significantly differed were as follows: total iron binding capacity (TIBC) (APL: 264.4 µg/dL vs. AML: 206.8 µg/dL, P =0.046), transferrin (APL: 1.79 g/L vs. AML: 1.29 g/L, P =0.005), erythrocyte sedimentation rate (ESR) (APL: 7.1 mm/h vs. AML: 50.0 mm/h, P <0.001), and triglyceride (TG) (APL: 206.2 mg/dL vs. AML: 109.9 mg/dL, P =0.006) (Table 2). We determined the cut-off value of each significant factor using the ROC curve. Our established values were as follows: FDP ≥27 µg/mL, D-dimer ≥2,071 ng/mL, and fibrinogen ≤279 mg/dL. Among these laboratory markers, ESR, D-dimer, FDP, fibrinogen, and TG were reliable markers (Table 3).
Table 3.
Cut-off values for significant markers based on the ROC curve.
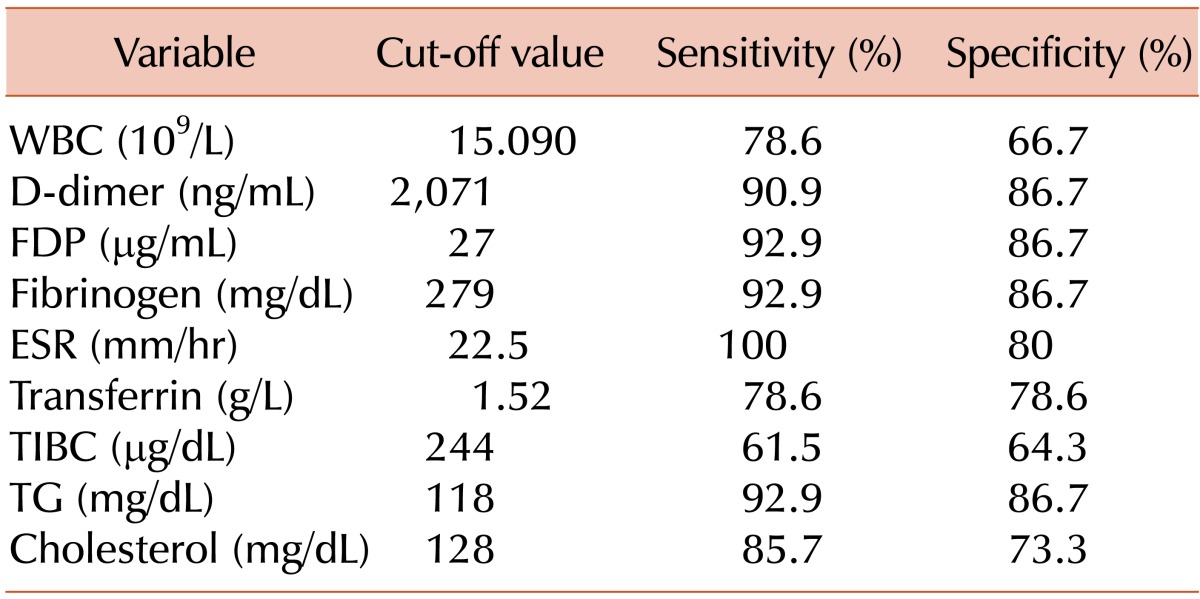
Abbreviations: WBC, white blood cell; FDP, fibrin degradation product; ESR, erythrocyte sedimentation rate; TIBC, total iron binding capacity; TG, triglyceride.
DISCUSSION
Before the introduction of ATRA in the 1980s, the mortality rate of APL was high and complete remission was only achieved in 65-80% of patients [8, 9]. Following the introduction of ATRA and its combination with other anti-cancer therapies, the complete remission rate of APL reached over 90% and the mortality rates also decreased. DIC is a distinct coagulopathy disorder, which is noted in APL patients [4]. Complications related to hemorrhages due to DIC are serious issues in APL patients; hemorrhages have been reported to occur in 90% of APL patients [3]. Moreover, many studies conclude that hemorrhage is the primary cause of deaths in APL cases [10, 11]. A prospective study conducted on 279 patients showed that 18 patients (6.5%) suffered from serious hemorrhage and 9 of them died due to the hemorrhage; further, there was a significant difference in the 5-year survival rate among patients depending on whether or not they had experienced a hemorrhage previously (68.1% vs. 31.1%; P <0.0001) [12]. In addition, a study conducted among 157 Brazilian patients diagnosed with APL reported that 50 patients (32%) died under induction therapy and 34 patients (21.6%) died because of hemorrhage [13].
AML is classified into subtypes based on cell morphology and results of cytochemistry, immunophenotyping, and cytogenetic tests. APL, a subtype of AML, is the most likely diagnosis if both an abundance of Auer Rods and cells with a high granular content are observed. However, typical morphological traits are not found in all cases. APL may be diagnosed based on the detection of the PML/RARα fusion protein; however, reverse transcriptase polymerase chain reaction (RT-PCR) for the fusion transcript takes 2 to 5 days depending on the facility. Therefore, if a clinician suspects APL based on clinical and laboratory findings (fatal coagulopathy) and peripheral blood smear results, ATRA is generally prescribed at the standard dose of 45 mg/m2 per day, without confirmation by molecular tests. This treatment is given emergently in divided doses, both to resolve the coagulopathy and to initiate induction therapy [1, 2, 5]. ATRA can cause mild side effects such as headache and arthralgia, or serious side effects such as hypotension, cardiac insufficiency, pericardial effusion, or pleural effusion. Other rare events include acute pancreatitis, hypercalcemia, male infertility, bone marrow fibrosis, bone marrow necrosis, thromboembolic events, and Sweet's syndrome [14, 15]. However, in clinical settings, owing to the adverse effects, most clinicians are cautious about starting patients on an ATRA regimen before receiving molecular confirmation of APL.
DIC can be caused by septicemia, trauma, and hemorrhage. DIC and hemorrhage are highly probable in APL patients and those with other subtypes of AML because of the accompanying thrombocytopenia and infection [6, 7]. To our knowledge, no study has compared the differences in the patterns of laboratory characteristics, including the DIC profile. Therefore, we conducted this study to establish a molecular profile for DIC between patients with suspected APL and those with other types of AML with DIC.
In this study, among the components of the DIC criteria (platelet count, prolonged PT, fibrinogen, and elevated fibrin-related markers such as FDP and D-dimer), FDP, D-dimer, and fibrinogen levels significantly differed between APL patients and the patients with other subtypes of AML with DIC. FDP and D-dimer levels were higher and the fibrinogen level was lower in APL patients. With respect to the acute phase markers, APL patients showed a significantly higher TIBC and transferrin level and lower WBC count and ESR. Moreover, the APL patients had higher TG and cholesterol levels than those with other types of AML with DIC.
Acute phase proteins are a group of blood proteins that help in restoring homeostasis and limiting microbial growth in an antibody-independent manner in animals subjected to infection, inflammation, surgical trauma, or stress [16]. The severity of the inflammatory response in sepsis is determined by measuring changes in the levels of acute phase proteins. During sepsis, ESR and CRP are increased and the transferrin level is decreased. In addition, hypocholesterolemia may be observed owing to metabolic decompensation. The level of hypocholesterolemia can be quantified based on the level of acute phase response as well [17, 18]. In conclusion, the DIC profile (increased FDP and D-dimer and decreased fibrinogen levels) and the acute phase response (increased ESR and decreased transferrin levels) as well as hypocholesterolemia observed in patients with other subtypes of AML are similar to those observed during infection. In the APL group, ESR and the levels of transferrin and cholesterol were within the reference range.
Based on our results, we established the cut-off value of significant markers. The present findings can provide an early diagnostic tool for APL. However, the study has some limitations. The numbers of patients with APL is quite small (N=14), because of which we are unsure if the proposed laboratory score to identify APL cases from other AML patients with DIC would be valid. Therefore, further investigation using comparative study with another cohort of patients is necessary. Nevertheless, thus far, there has been no study about the presumptive diagnosis of APL using a simple blood test. In addition, typical morphological traits were not found in all the APL cases studied. In such cases, physicians often require PML/RARA identification for APL diagnosis. In this case, our findings support the early initiation of ATRA treatment, prior to confirmation of PML-RARA rearrangement.
In summary, APL is a distinct subtype of AML, which is characterized by DIC. Among the components of the DIC criteria (platelet count, prolonged PT, fibrinogen, and elevated fibrin-related markers such as FDP and D-dimer), there were significant differences in the FDP, D-dimer, and fibrinogen levels. Among the acute phase reactants, the other significant markers were ESR, transferrin, and TIBC.
This study was supported by a research fund from Chosun University, 2013.
No potential conflicts of interest relevant to this article were reported.
References
- 1.Tallman MS, Altman JK. How I treat acute promyelocytic leukemia. Blood. 2009;114:5126–5135. doi: 10.1182/blood-2009-07-216457. [DOI] [PubMed] [Google Scholar]
- 2.Wang ZY, Chen Z. Acute promyelocytic leukemia: from highly fatal to highly curable. Blood. 2008;111:2505–2515. doi: 10.1182/blood-2007-07-102798. [DOI] [PubMed] [Google Scholar]
- 3.Kwaan HC, Wang J, Boggio LN. Abnormalities in hemostasis in acute promyelocytic leukemia. Hematol Oncol. 2002;20:33–41. doi: 10.1002/hon.687. [DOI] [PubMed] [Google Scholar]
- 4.Fenaux P, Chastang C, Chevret S, et al. The European APL Group. A randomized comparison of all transretinoic acid (ATRA) followed by chemotherapy and ATRA plus chemotherapy and the role of maintenance therapy in newly diagnosed acute promyelocytic leukemia. Blood. 1999;94:1192–1200. [PubMed] [Google Scholar]
- 5.NCCN Clinical practice guidelines in oncology: Acute myeloid leukemia, Version 2. Fort Washington, PA: National Comprehensive Cancer Network; 2013. [Accessed September 23, 2013]. Available from: http://www.nccn.org/professionals/physician_gls/pdf/aml.pdf. [Google Scholar]
- 6.Kaneko T, Wada H. Diagnostic criteria and laboratory tests for disseminated intravascular coagulation. J Clin Exp Hematop. 2011;51:67–76. doi: 10.3960/jslrt.51.67. [DOI] [PubMed] [Google Scholar]
- 7.Taylor FB, Jr, Toh CH, Hoots WK, Wada H, Levi M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 2001;86:1327–1330. [PubMed] [Google Scholar]
- 8.Cunningham I, Gee TS, Reich LM, Kempin SJ, Naval AN, Clarkson BD. Acute promyelocytic leukemia: treatment results during a decade at Memorial Hospital. Blood. 1989;73:1116–1122. [PubMed] [Google Scholar]
- 9.Rodeghiero F, Avvisati G, Castaman G, Barbui T, Mandelli F. Early deaths and anti-hemorrhagic treatments in acute promyelocytic leukemia. A GIMEMA retrospective study in 268 consecutive patients. Blood. 1990;75:2112–2117. [PubMed] [Google Scholar]
- 10.de la Serna J, Montesinos P, Vellenga E, et al. Causes and prognostic factors of remission induction failure in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and idarubicin. Blood. 2008;111:3395–3402. doi: 10.1182/blood-2007-07-100669. [DOI] [PubMed] [Google Scholar]
- 11.Lehmann S, Ravn A, Carlsson L, et al. Continuing high early death rate in acute promyelocytic leukemia: a population-based report from the Swedish Adult Acute Leukemia Registry. Leukemia. 2011;25:1128–1134. doi: 10.1038/leu.2011.78. [DOI] [PubMed] [Google Scholar]
- 12.Yanada M, Matsushita T, Asou N, et al. Severe hemorrhagic complications during remission induction therapy for acute promyelocytic leukemia: incidence, risk factors, and influence on outcome. Eur J Haematol. 2007;78:213–219. doi: 10.1111/j.1600-0609.2006.00803.x. [DOI] [PubMed] [Google Scholar]
- 13.Jácomo RH, Melo RA, Souto FR, et al. Clinical features and outcomes of 134 Brazilians with acute promyelocytic leukemia who received ATRA and anthracyclines. Haematologica. 2007;92:1431–1432. doi: 10.3324/haematol.10874. [DOI] [PubMed] [Google Scholar]
- 14.Tallman MS, Andersen JW, Schiffer CA, et al. All-trans-retinoic acid in acute promyelocytic leukemia. N Engl J Med. 1997;337:1021–1028. doi: 10.1056/NEJM199710093371501. [DOI] [PubMed] [Google Scholar]
- 15.Hatake K, Uwai M, Ohtsuki T, et al. Rare but important adverse effects of all-trans retinoic acid in acute promyelocytic leukemia and their management. Int J Hematol. 1997;66:13–19. doi: 10.1016/s0925-5710(96)00578-6. [DOI] [PubMed] [Google Scholar]
- 16.Murata H, Shimada N, Yoshioka M. Current research on acute phase proteins in veterinary diagnosis: an overview. Vet J. 2004;168:28–40. doi: 10.1016/S1090-0233(03)00119-9. [DOI] [PubMed] [Google Scholar]
- 17.Chiarla C, Giovannini I, Siegel JH. The relationship between plasma cholesterol, amino acids and acute phase proteins in sepsis. Amino Acids. 2004;27:97–100. doi: 10.1007/s00726-004-0064-x. [DOI] [PubMed] [Google Scholar]
- 18.Suárez-Santamaria M, Santolaria F, Perez-Ramirez A, et al. Prognostic value of inflammatory markers (notably cytokines and procalcitonin), nutritional assessment, and organ function in patients with sepsis. Eur Cytokine Netw. 2010;21:19–26. doi: 10.1684/ecn.2009.0185. [DOI] [PubMed] [Google Scholar]