

Abstract
In men and women sexual arousal culminates in orgasm, with female orgasm solely from sexual intercourse often regarded as a unique feature of human sexuality. However, orgasm from sexual intercourse occurs more reliably in men than in women likely reflecting the different types of physical stimulation men and women require for orgasm. In men, orgasms are under strong selective pressure as orgasms are coupled with ejaculation and thus contribute to male reproductive success. By contrast, women's orgasms in intercourse are highly variable and are under little selective pressure as they are not a reproductive necessity.. The proximal mechanisms producing variability in women's orgasms are little understood. In 1924 Marie Bonaparte proposed that a shorter distance between a woman's clitoris and her urethral meatus (CUMD) increased her likelihood of experiencing orgasm in intercourse. She based this on her published data which were never statistically analyzed. In 1940 Landis and colleagues published similar data suggesting the same relationship, but these data too were never fully analyzed. We analyzed raw data from these two studies and found that both demonstrate a strong inverse relationship between CUMD and orgasm during intercourse. Unresolved is whether this increased likelihood of orgasm with shorter CUMD reflects increased penile-clitoral contact during sexual intercourse or increased penile stimulation of internal aspects of the clitoris. CUMD likely reflects prenatal androgen exposure, with higher androgen levels producing larger distances. Thus these results suggest that women exposed to lower levels of prenatal androgens are more likely to experience orgasm during sexual intercourse.
Keywords: orgasm in intercourse, genital anatomy, sex differences, clitoral position, prenatal androgens
Introduction
Although approximately 90% of women report orgasm from some form of sexual stimulation, most women do not routinely (and some never) experience orgasm solely from sexual intercourse (Lloyd, 2005). By contrast, nearly 100% of men routinely experience orgasm solely from sexual intercourse. This gender disparity in the reliability of reaching orgasm during sexual intercourse has been thought to reflect evolutionary (Lloyd, 2005) or social (Hite, 1976) processes. An anatomical explanation for this disparity has also been proposed such that variation in the distance between a woman's clitoral glans and her vagina predicts the likelihood that she will experience orgasm in intercourse (Narjani, 1924). Specifically it was proposed that if this distance is less than 2.5cm a woman is very likely to have orgasms solely from sexual intercourse. This relationship has not been statistically evaluated, but two historical studies provide data supporting such a relationship (Narjani, 1924; Landis, Landis, and Bowles, 1940). We use an unconventional approach to investigate the proposed relationship between variation in women's genitals and orgasm during intercourse. We first explore the history of this idea in the scientific and popular literature and then present statistical analysis of the two available historical datasets with data relevant to the proposed relationship (Narjani, 1924; Landis, Landis, and Bowles, 1940). While there are challenges to the validity of these data, we find them sufficiently supportive of a relationship between women's genital anatomy and the occurrence of orgasm in intercourse to feel that they can serve as the basis for developing modern well-controlled studies of the relationship between women's genital anatomy and the occurrence of orgasm in intercourse.
Orgasm is the culmination of sexual arousal, and the promise of orgasm may provide primary motivation for individuals to engage in sexual intercourse. However, sexual arousal itself is rewarding and likely common to the sexuality of all mammals. Studies of animals have shown that sexual arousal is rewarding even when sexual intercourse doesn't occur (Meisel, Camp and Robinson, 1993). Certainly humans, at least men, sometimes seek out activities, such as strip clubs, where sexual arousal without orgasm is the primary goal and where sexual intercourse is unlikely to occur. In male mammals, sufficient sexual arousal leads to ejaculation and orgasm. Thus it is possible that orgasm occurs in all male mammals. The case in females is less clear. While there is evidence that female sexual arousal is rewarding (Meisel, Camp and Robinson, 1993), it is unclear whether humans, or possibly primates, (Goldfoot, et al., 1980), are unique in being the only animals where heightened female sexual arousal culminates in orgasm. Even in primates female orgasm is not universal, with little evidence of its occurrence outside of humans. Even among women, at least 10% report never having experienced orgasm. To further complicate matters, there remains a lack of complete agreement on what constitutes female orgasm (Meston, et al., 2004; Komisaruk, Beyer-Flores, and Whipple 2006). Although sexual arousal precedes orgasm in women, the specific sexual stimulation that triggers orgasm varies greatly among women. Women reach orgasm from direct clitoral stimulation, indirect clitoral stimulation, vaginal stimulation or stimulation of internal areas surrounding the vagina. Some women experience orgasm solely from sexual intercourse, whereas other women require concurrent stimulation of the external parts of the clitoris in order to reach orgasm during sexual intercourse, and some women never experience orgasm in intercourse under any conditions.
A period of increasing sexual arousal precedes orgasm, typically from genital stimulation, in those women who experience orgasm. Given the differences in male and female genitals it is likely that the nature and extent of genital stimulation necessary for orgasm differs between men and women. This appears to certainly be the case for orgasms which occur solely from sexual intercourse.
A striking sex difference in the onset of the occurrence of orgasm has been known for more than 50 years (Figure 1). Post-pubertal males routinely, and apparently easily, experience orgasm, as indicated by their reliable ejaculatory reflex, but female orgasm appears to develop more slowly and is less predictable than male orgasm. While there are women who reach orgasm as easily and routinely as do men, and some women who experience orgasm more easily and multiple times during a single session of sexual intercourse, this is not women's typical experience with orgasm. This sex difference in the onset of orgasm is illustrated by when the maximum number of men or women have experienced orgasm. Figure 1 illustrates the cumulative incidence, across time, of males ejaculating (Kinsey, Pomeroy and Martin, 1948) in comparison to the cumulative occurrence of orgasm in women (Kinsey, Pomeroy, Martin, and Gebhard, 1953). Ejaculation, and thus presumably orgasm, increases from less than 5% of boys ejaculating, to 100% within a 5 year span. By contrast, a more gradual developmental curve is evident in women where the incidence of women experiencing orgasm increases gradually across 25 years and never exceeds 90% (Figure 1). Taken together these data suggest that orgasm is a different phenomenon in women than in men, occurring under different developmental influences and likely reflecting genital differences between men and women.
Figure 1.
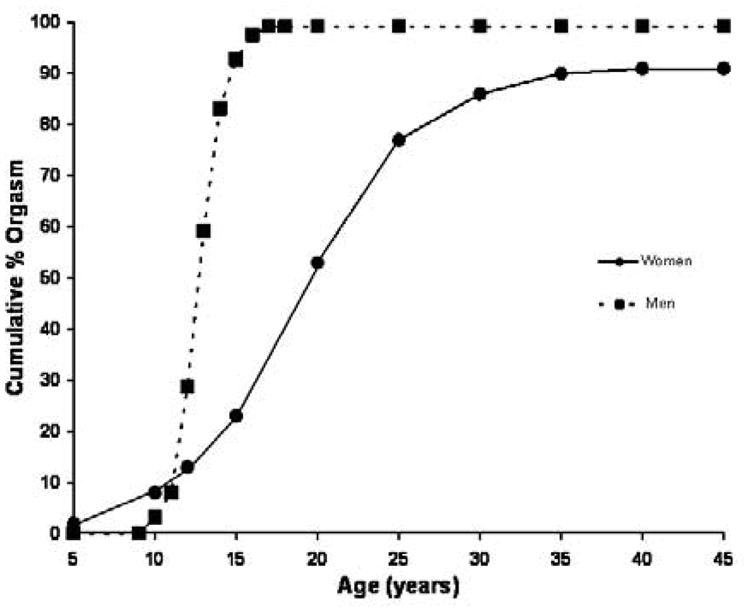
Illustrates the sex difference in the occurrence of orgasm in males and females in relation to age. Males show a rapid transition from few boys experiencing orgasm prior to puberty to all men experiencing orgasm soon after puberty. Women, by contrast show a much more gradual developmental curve. Male data are adapted from Kinsey, Pomeroy, and Martin, 1948 and the female data are adapted from Kinsey, et al., 1953.
When orgasm is limited to orgasm occurring during sexual intercourse, a striking difference in the distribution of its occurrence emerges between men and women such that the distributions of men and women who “never”, “rarely”, “sometimes”, “often”, “nearly always” or ”always” experience orgasm during sexual intercourse differ markedly. In men this distribution has a single sharp peak centered on “always” or “nearly always” experiencing orgasm during intercourse. By contrast, the women's distribution is relatively flat across categories with an elevation in the middle and smaller frequencies at the endpoints of “never” and “always” (Lloyd 2005). Lloyd (2005) argued that this sex difference in the distribution of orgasm supports strong evolutionary selective pressure on orgasm during intercourse in men, but not women. The direct connection between male ejaculation during intercourse and reproductive success makes understandable the almost certainty of male orgasm during intercourse. However, the source of the striking variability in the occurrence of orgasm in intercourse among women is unknown, though a number of theories have been proposed concerning its origin.
Freud posited that women's capacity to experience orgasm during intercourse varied according to their psychoanalytic development. In his view, girls initially experienced clitoral eroticism analogous to boy's penile eroticism. As girls matured psychologically they transitioned from clitoral eroticism to vaginal eroticism, which allowed them to experience orgasm during vaginal intercourse (Freud, 1905). In Freud's view, orgasm from vaginal intercourse reflected mature, psychologically healthy, sexuality whereas continued reliance on clitoral arousal for orgasm reflected psychologically immature development. Since the publication of Freud's theory of women's sexuality “clitoral” orgasms have been contrasted to “vaginal” orgasms, with vaginal orgasms regarded as reflecting appropriate psychological development. The names don't actually indicate different types of orgasms, but indicates the type of genital stimulation triggering the orgasm. Since a majority of women do not routinely and reliably experience orgasm solely from sexual intercourse (Lloyd, 2005), Freud's psychoanalytic arguments have resulted in feelings of sexual inadequacy for those many women whose orgasms do not result from vaginal stimulation. This view, that there is a mature and psychologically healthy form of female orgasm, has become less prevalent, but is still promoted more than 100 years after Freud's proposals. For example, there are those who argue that women experiencing orgasms in intercourse have better mental health than women who reach orgasms through other means (Brody and Costa, 2008). Similarly, there are self-help programs whose goal is for women to achieve orgasm solely from vaginal intercourse (Kline-Graber and Graber, 1975). Thus orgasm solely from sexual intercourse continues to occupy a significant place in women's sexuality. Given that a majority of women do not routinely experience orgasm from such stimulation (Lloyd, 2005), it seems incomprehensible that this reflects that a majority of women are psychologically immature. Instead this demonstrates the variability in women's orgasms and that orgasm solely from sexual intercourse is not routine for most women. The question remains unanswered as to why a minority of women routinely experience orgasm solely from sexual intercourse, whereas most women require other types of stimulation.
Women differ markedly in the type of genital stimulation that reliably induces orgasm. On the one hand are women who reliably trigger orgasm through vaginal or cervical stimulation without any direct contact with the clitoral glans or shaft (Alzate, 1985; Komisaruk, et al., 2006). On the other hand are women who reliably reach orgasm during intercourse only when there is concurrent direct clitoral stimulation (Masters and Johnson, 1966; Fisher, 1973; Hite, 1976). Surprisingly, since the ‘60s, the notion that some women experience orgasm during intercourse solely from vaginal stimulation has been questioned and currently the most common view is that all women's orgasms during intercourse are triggered by direct or indirect clitoral stimulation (Masters and Johnson, 1966; Sherfey, 1972; Hite 1976). As Sherfey, a psychoanalyst, put it, “The term ‘vaginal orgasm’ is perfectly permissible as long as it is understood that the (penile) thrusting is effective because it stimulates the clitoris”, (Sherfey, 1972, p.86). Thus there is a long history of the notion that clitoral stimulation, direct or indirect, is required for women to experience orgasm in intercourse.
Unfortunately, survey data on the occurrence of orgasm in intercourse do not typically distinguish intercourse without concurrent clitoral stimulation from intercourse with concurrent clitoral stimulation (see Lloyd, 2005 for a more complete discussion of this issue). Thus current estimates provide imprecise information on the proportion of women who routinely experience orgasm solely from vaginal intercourse without concurrent direct clitoral stimulation. Still, whether or not concurrent clitoral stimulation is specified, only a minority of women report reliably experiencing orgasm from vaginal intercourse. As Lloyd concluded, “… approximately 25% of women always have orgasm from intercourse, while a narrow majority of women have orgasm with intercourse more than half the time … roughly one third of women rarely or never have orgasm from intercourse”, (Lloyd, 2005; p36). It seems unlikely that most women in these studies have concurrent clitoral stimulation during intercourse because such stimulation is almost uniformly successful in inducing orgasm (Fisher, 1973; Hite 1976) and thus the percentages of women experiencing orgasm in intercourse would be correspondingly higher. It seems clear, however, that some of the variability in female orgasm during intercourse stems from whether or not intercourse itself produces clitoral stimulation.
Clitoral stimulation during sexual intercourse might reflect how closely the clitoral glans and shaft are positioned relative to the vaginal opening, affecting the likelihood that the male's penis would stimulate the clitoris during vaginal thrusting. This distance varies markedly among women, ranging from 1.6cm to 4.5cm between a woman's clitoral glans and her urethral opening (a proxy for the vaginal opening; Lloyd, Crouch, Minto, and Creighton, 2005). However the relationship between variation in this distance and variation in the occurrence of orgasm during intercourse is not fully known.
The notion that women's orgasm during intercourse is related to the location of the clitoral glans in relation to a woman's vagina was suggested more than 85 years ago (Narjani, 1924, Dickinson, 1933, Landis, Landis, and Bowles, 1940). Marie Bonaparte, using the pseudonym Narjani, published the first data relating clitoral glans position to the occurrence of women's orgasm during sexual intercourse (Narjani, 1924). Bonaparte measured the distance between the underside of the clitoral glans and the centre of the urinary meatus (CUMD)2 and compared that distance to the likelihood that the woman experienced orgasm during sexual intercourse. Bonaparte claimed that shorter CUMD resulted in a higher incidence of orgasm in intercourse, whereas longer CUMD produced a lesser likelihood (Narjani, 1924). Published in 1924, Bonaparte's data were never subjected to statistical analysis, as the appropriate statistical tests had not yet been invented. Thus Bonaparte's conclusion of a relationship between CUMD and orgasm in intercourse was based on inspection of the data leaving unresolved whether there really is such a relationship and if there is, the reliability and magnitude of the relationship.
Bonaparte (Narjani, 1924) argued that there were two types of sexual nonresponsiveness in women, ‘frigidities’ as she termed them. The first was a sexual anesthesia reflected in an inability to reach orgasm from any type of stimulation, “internal or external”. Women with the second ‘frigidity’ were very sexually responsive, orgasmic, but were unable to achieve orgasm solely from coitus “Implacablement insensibles pendant le coit, et le coit seul”, (Narjani, 1924, p. 770). According to Bonaparte, the first ‘frigidity’ resulted from psychogenic sources and was amenable to psychoanalytic treatment. It was the second ‘frigidity’, the lack of orgasm during intercourse, that Bonaparte thought nonresponsive to psychotherapy because she though it was biological, caused by the woman's clitoris being located too far from her vaginal opening to be stimulated by the man's penis during sexual intercourse.
Bonaparte believed so strongly in this anatomical influence on women's sexual response that she proposed treating this second type of “frigidity” by surgically relocating the clitoral glans closer to the vaginal opening in women not experiencing orgasm in intercourse (Narjani, 1924). With the Austrian surgeon, Josef Halban, Bonaparte created the Halban-Narjani procedure (Bonaparte, 1933) in which the suspensory ligament of the clitoris was transected allowing repositioning of the clitoral glans closer to the vagina. Bonaparte, who reported having high sexual interest, but never experiencing orgasm from intercourse, received this treatment three times when the initial treatment was ineffective (Thompson, 2003). Her genital surgeries were ineffective in allowing her to experience orgasm from intercourse. Similar to Bonaparte's experience, the surgical procedure was not effective in the five women who received the clitoral surgery (one of whom may have been Bonaparte) because they did not experience orgasm during intercourse. Of the five, two disappeared from follow-up, two experienced no clear change in their sexual response, and one improved somewhat, but only while the surgical site was healing from an infection. Once the surgical site healed, she no longer experienced orgasm from intercourse (Bonaparte, 1933). These results do not necessarily invalidate the theoretical premise of the surgery, as the clitoral area is heavily innervated (O'Connell, Sanjeevan, and Hutson, 2005) and it is likely that the surgical procedure, while repositioning the clitoris closer to the vagina, may have also deinervated the clitoris. Whatever the reality of the surgery, by 1933, Bonaparte was unconvinced by her 1924 data and rejected her earlier anatomical interpretation as inaccurate. Making an argument that Dickinson (1949) would later employ against the anatomical argument, Bonaparte pointed out that there were women in her 1924 sample with short CUMD who did not experience orgasm in intercourse and women with long CUMD who did. Instead, she argued, psychoanalytical processes, not clitoral placement, determined whether or not a woman experienced orgasm in intercourse (Bonaparte, 1933). Her changed viewpoint likely reflected her experience as Freud's student since 1927 (Thompson, 2003), as her 1933 paper recapitulated Freud's conceptualizations of women's sexuality which were absent from her original study (Bonaparte, 1933).
R.L. Dickinson (1933) and Carney Landis (Landis, Landis, and Bowles, 1940) next collected data on CUMD and orgasm during intercourse. Although Dickinson collected data on the genitalia of more than 5000 women during his career as a gynecologist, he never summarized or published his data, specifically the data on 200 women where he recorded their CUMD and their occurrence of orgasm in intercourse. He referred to this sample in his 1933 book, “Atlas of Human Sexual Anatomy” (Dickinson, 1933), to refute, by example, Marie Bonaparte's contention that CUMD predicted orgasm in intercourse. Dickinson claimed, as Bonaparte had in 1933, that his sample had women with short CUMDs who never experienced orgasm in intercourse, and women with long CUMDs who routinely did (Dickinson, 1933). However, Dickinson presented no actual data to support his argument and to our knowledge, no summary of the data from these 200 women he measured has been published. Thus it is unknown whether the cases Dickinson cites were isolated exceptions to a more common pattern in which CUMD predicted the occurrence of orgasm in intercourse or reflected the absence of a relationship between CUMD and orgasm in intercourse as Dickinson claimed.
Carney Landis, along with his wife Agnes and a colleague Marjorie Bowles collected systematic data on CUMD and the occurrence of orgasm in intercourse. Although there were 153 nonmentally ill women in the study (the other 142 women in the study were psychiatric inpatients), data on CUMD and orgasm were presented only for the 44 married women in the study, for which there were complete data for only 37. In addition, Landis and colleagues (1940) only minimally analyzed their data, publishing a single 2×2 table comparing the incidence of orgasm during intercourse (divided into two groups, 40-100% and 0-30% orgasm incidence) in relation to whether the subject's clitoris was “high” (CUMD of 3.5cm or more) or “low” (CUMD of less than 3.5cm). The authors claimed the comparison was significant with 81% of women with low clitoral placement experiencing orgasm in intercourse more than 40% of the time, in contrast to 50% of the women with high clitoral placement. However, neither the method of statistical comparison employed, nor how an exact probability of 0.038 was derived, or whether one or two-tailed probabilities were used was described for this analysis. While this single analysis supports that short CUMD is associated with a higher probability of orgasm in intercourse, it is unclear whether there is more convincing evidence within this dataset that might be revealed by a more extensive statistical analysis.
Regardless of the lack of analytical detail in all of these studies the notion that the placement of the clitoris relative to the vagina affected orgasm response had a popular distribution and was presented as a settled fact by authors of “marital sex manuals” of the era as well as being presented in other publications over the last 80 years.
For example, van de Velde (1930; 1965), author of the most popular marital sex manual of the 1930's to the 1950's, “Ideal Marriage” offered the view that:
“… coital stimulation depends very much on individual structure, For example, on the size of the clitoris, on the development of the frenulum, on the position of the clitoris (and there is considerable diversity in these respects, especially in position, i.e., whether the little organ is situated higher up on the front of the symphysis pubis, or almost below it).” (van de Velde, 1930, p178-179)
Later in the same chapter van de Velde (1930) asserted that such high clitoral placement is associated with a small clitoris and terms this clitoral size “… a certain degree of arrested development of genital infantilism.”, stating that such “underdevelopment” is common in Europe and America and concluding that “The small size and high position of the clitoris which prevent its full stimulation in coitus have therefore special significance.” This reference to “genital infantilism” should not be seen as echoing Freud's distinction between clitoral and vaginal eroticism. Van de Velde was specifically referring to the size of the clitoris as his book promoted clitoral stimulation by the husband as a crucial part of marital sexuality. He even offered encouragement that regular stimulation of the clitoris would produce permanent enlargement because as he put it, “… practice makes perfect” (van de Velde, 1930). Of course no evidence is presented, nor has any been found, that sexual activity permanently alters clitoral size. Still, the clear message conveyed in these passages is that the configuration of women's genitals significantly influences the likelihood that they will experience orgasm from intercourse.
A similar conclusion was offered by Hannah and Abraham Stone (1935) authors of another best-selling marriage manual, “A Marriage Manual”, where they stated:
“It is likely that the distance between the clitoris and the opening of the vagina in the individual woman may have some bearing upon her capacity to reach an orgasm during intercourse. The higher the clitoris is located and the further away from the vaginal entrance the less contact there is apt to be and the greater the difficulty in obtaining a satisfactory climax.” (Stone and Stone, 1935, p198-199).
The Stones described that they had measured the genitals of “a large number of women”. Although they present no actual data, they claim that the distance between the vagina and clitoris in their sample varied from “one-half to two and a half inches with an average of one and a half inches” (Stone and Stone, 1935). They concluded that, although there is no consistent relationship, women with shorter distances were “more apt to belong to the group who reach satisfactory climax”, (Stone and Stone, 1935). Thus the idea, first presented in Marie Bonaparte's work had widespread popular dissemination. The origin of this idea in popular marriage manuals is unclear as neither van de Velde, nor the Stones cite Bonaparte's, or any other, research, as the source of the principle that distance from the clitoris to the vagina influences the likelihood that a woman will experience orgasm in intercourse.
Judd Marmor (1954), a psychoanalyst and sex therapist, presented the idea that the distance between the clitoris and vagina was important to women's achieving orgasm in intercourse, an idea that was repeated in the “Hite Report”, (Hite, 1976). Both of these authors present the same conclusion as did Van de Velde and the Stones, but do not cite any supporting data. We could find no more recent data on the relationship between clitoral placement and women's orgasmic response in sexual intercourse than those presented in Narjani (1924) and the Landis study (Landis, Landis, and Bowles, 1940).
In exploring the history of the idea that variability in women experiencing orgasm in intercourse reflect genital variability we discovered that Bonaparte (Narjani, 1924) published her raw data in her 1924 paper and that the raw data for the married sample in Landis, Landis, and Bowles (1940) were archived in the library of the Kinsey Institute for Research in Sex, Gender and Reproduction. As both samples had either never been statistically analyzed (Narjani, 1924) or only minimally analyzed (Landis, Landis, and Bowles, 1940), we analyzed these samples using modern statistical techniques unavailable when these data were collected. The analyses presented here of both the Bonaparte (Narjani, 1924) and Landis (Landis, Landis, and Bowles, 1940) samples support Bonaparte's original contention that CUMD predicts the likelihood of women experiencing orgasm during sexual intercourse. Although there are significant differences between the two samples in both the characteristics of the data and the extent of the relationship revealed between CUMD and orgasm in intercourse, the results support the likelihood than genital configuration contributes significantly to a woman's potential to experience orgasm solely from sexual intercourse.
Methods
Data for the analyses reported here were derived from raw data on 43 women published in Narjani, (1924) and the original data records obtained from The Kinsey Institute for Research in Sex, Gender and Reproduction on the 44 married women described in Landis, Landis, & Bowles (1940).
Bonaparte sample subjects
Marie Bonaparte's data (Narjani, 1924) were published under the pseudonym “A. E. Narjani” (as described in Bonaparte, 1933) and will be referred to as the Bonaparte sample in this paper. The 1924 paper contained summaries of genital measurements on 200 women in Vienna and France, but for these women no data were presented on orgasm occurrence. The raw data for an additional 43 women, likely from France, possibly a subset of the 200 women, were presented in table 2 of the original article. These data consisted of genital measurements (cm) and the occurrence of orgasm in intercourse (yes or no) along with occurrence of orgasm from masturbation, age of first intercourse, age of menarche, chronological age, and height. Women in Narjani (1924) ranged in age from 20 to 62 with a mean age of 33.7yr No information is provided about the samples' ethnic makeup. All women had experienced sexual intercourse.
Table 2.
Classification of subjects from the Bonaparte and Landis samples when using discriminant functions generated from either the Bonaparte or the Landis samples. (Table cells with a gray background are those where the discriminant function misclassified significantly more subjects than expected by chance.)
| Classification using discriminant function | ||||
|---|---|---|---|---|
| A. Bonaparte subjects used to generate discriminant function | No Orgasm | Orgasm | ||
| Bonaparte Sample | (Actual Classification) | No Orgasm | 81 (100) |
19 (0) |
| Orgasm | 7 (0) |
93 (100) |
||
| Landis Sample | (Actual Classification) | Orgasm < 67% | 90 (100) |
10 (0) |
| Orgasm > 67% | 56 (0) |
44* (100) |
||
| Classification using discriminant function | ||||
| B. Landis subjects used to generate discriminant function | No Orgasm | Orgasm | ||
| Bonaparte Sample | (Actual classification) | No Orgasm | 62* (100) |
38 (0) |
| Orgasm | 0 (0) |
100 (100) |
||
| Landis Sample | (Actual classification) | Orgasm < 67% | 74* (100) |
26 (0) |
| Orgasm > 67% | 38 (0) |
62* (100) |
||
Classification not significantly different from chance classification using Press's Q statistic
Bonaparte sample genital measurement
A detailed description of how the genital measurements were obtained was included in the 1924 article. Figure 2, derived from the original article, illustrates how the distance from the glans clitoris to the center of the urinary meatus (CUMD) was measured. The distance from the clitoral glans to the urethral meatus is the primary independent measure in this study. Bonaparte described that the distance measured was from a small triangular area on the underside of the clitoris delineated to the left and right by convergence of the labia minora, which would correspond to the frenulum of the clitoris, to the middle of the urinary meatus. Thus Bonaparte's measurements did not include the clitoral glans itself, but were taken from its base or underside. The arc in figure 2 illustrates the pubic arch but the relationship between the arch and the clitoral glans is either poorly illustrated or in error. As drawn it would suggest that in some women the clitoral glans is actually well above the pubic arch, a location which has never been reported for women's genitals.
Figure 2.
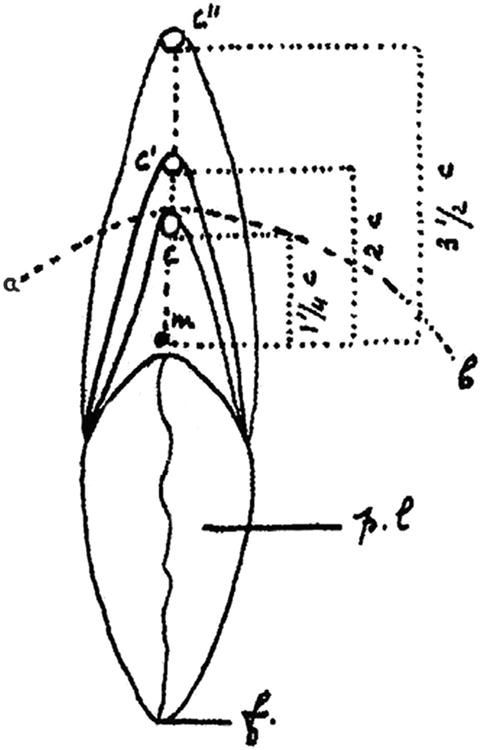
Illustrates the measurements used to determine the clitoral-urinary meatus distance (CUMD) in a sample of adult women. C, C′, and C″ are the location of the clitoris, M is the location of the urinary meatus, p.l. are the labia minora (petites lèvres in french), F is the fourchette of the vagina, and a,b is the arch of the symphysis pubis. Bonaparte's CUMD measure was from the frenulum of the clitoris (underside of the clitoral glans) to the center of the urinary meatus (Adapted from Narjani, 1924).
Bonaparte sample measurement of orgasm
Description of the measurement of occurrence of orgasm is limited to subjects being asked whether or not they had “a normal reaction during sexual intercourse” (Narjani, 1924), with the “normal reaction” undefined. However, Bonaparte clearly separates orgasm solely from intercourse from other types of orgasms, including ones in which the women's partner stimulates her clitoris during intercourse (Narjani, 1924). From the manner in which Bonaparte discusses “normal” sexual intercourse and from her own concern about being unable to experience orgasm solely from intercourse (Thompson, 2003), it is apparent that to Bonaparte a normal reaction means orgasm solely from intercourse without any concurrent clitoral stimulation. Thus, even though the article does not provide a specific description of exactly what the women were asked, it is most likely that the women were being asked whether they experience orgasm during intercourse without any direct clitoral stimulation. Subjects were also asked whether they experienced orgasm from masturbation.
Landis sample subjects
The Landis, Landis, & Bowles (1940) data, referred to as the Landis sample in this paper, were derived from 44 married women ranging in age from 22-35yr with a mean age of 29.1yr. The primary focus of the Landis study was comparing the sexuality of “normal” and mentally ill women. Thus, the 44 married women were compared to a group of women with diagnosed mental illness. Because of the diagnosis of mental illness, none of the data from the mentally ill comparison group were used in the analyses presented here.
Little ethnic information on the sample is available, but 78% were Jewish, with 11% Catholic and 11% protestant. Fifty nine percent of the sample were foreign born, but it is unclear what this means. Complete data, which included both a genital measurement and an assessment of the occurrence of orgasm in intercourse, was available for 37 of the 44 subjects.
Landis sample genital measurement
All subjects in the Landis sample received a gynecological examination which included measuring the clitoris to urinary meatus distance. The same male MD gynecologist, who was not one of the study's authors, collected all physical examination data, including CUMD. It is not stated whether he was blind to the hypothesis under test. However from the published study and the raw records there is no evidence that the gynecologist had access to the interview data or participated in any other part of the study other than the gynecological examinations.
No detail is provided on exactly how CUMD measures were made either in the published text, or on the raw data sheets. The data sheet entry is simply “clitoral-meatus distance … cm” with a space to enter the CUMD and signed at the bottom by the MD. It is not known for certain whether CUMD was measured from the clitoral glans or from the clitoral frenulum, as in Bonaparte's study, to the urinary meatus. However, because the MD also measured clitoral glans width and recorded clitoral size, it seems likely that the measurement was taken from the clitoral glans to the urinary meatus. This possible difference in measurement between the two studies does not create problems for analysis within the Landis sample, but makes comparisons between the Landis and Bonaparte samples more difficult as measuring from the tip of the clitoral glans would result in a larger CUMD than if the frenulum is used as the clitoral marker.
Landis sample measurement of orgasm
Orgasm occurrence during intercourse was assessed during a lengthy face to face interview, done by one of the study's authors with Bowles doing the majority of the interviews according to the published text. This interview was more than 20 pages long and encompassed much more than questions about sexual activity. The relevant questions for the purpose of assessing the occurrence of orgasm were in section V.4 of the interview (Landis, Landis, & Bowles, 1940) in which the subject was asked the following questions
“How long were you married or how long had you been having relations before you experienced your first satisfactory orgasm with your present husband? Do you usually experience a climax or orgasm when you have intercourse? About what proportion of the time do you fail to experience it, i.e. about how many times out of ten?” (Landis, Landis, & Bowles, 1940, p.248).
An assistant transcribed the narrative answers on the raw data sheets to a text file. These text entries were used to code whether or not the woman had described ever experiencing orgasm in intercourse. In addition, the reported failure rate for orgasm in intercourse was used to calculate the percentage of intercourse that produced orgasm for those subjects who experienced orgasm during intercourse. Data derived from the text files were independently coded by the first author and another investigator blind to the hypothesis that CUMD influenced the likelihood of orgasm in intercourse. The data sheets for coding contained only the answers to the questions described above and contained no other information about the subject, except the unique subject identifier assigned in the original study. Thus there was no information about CUMD when the orgasm data were coded. Initial comparison between the coders revealed disagreement for what percentage of the occurrence of intercourse was reflected in qualitative terms subjects used, such as rarely or usually. A scale was created in which the following values were used rarely=10%, sometimes=20%, often=60%, usually=80%, and almost always=90%. When these values were applied to the uncoded data there were no disagreements between the two coders, with the exception of two cases. Two subjects were dropped because it was not possible to determine whether these subjects experienced orgasm in intercourse with direct clitoral stimulation or from intercourse alone. In both cases the subject described themselves as “helping their orgasm along”. While there are a number of interpretations of this statement it seemed most conservative to drop these subjects resulting in a total of 35 subjects for analysis.
Statistical analysis
Raw data from both studies were evaluated using SPSS 17 for Windows. In addition to the data on CUMD, whether the woman ever experienced orgasm in intercourse, and height, three additional categories were obtained by dividing 100 percent orgasmic response into thirds resulting in the following categories: a) whether women experienced orgasm 33% of the time or less, b) whether they experienced orgasm 34 to 66% of intercourse, and c) Whether they experienced orgasm 67 to 100% of the time. All of these are “yes”or “no” categories. For the Landis sample actual percentages could be used for analysis in addition to the derived categories, Because the data in the Bonaparte sample were either 1 or 0 for the occurrence of orgasm in intercourse, the derived percentage categories each provided the same distribution of answers as did the occurrence of orgasm in intercourse.
To determine the comparability of the two samples they were compared on CUMD and height using independent t tests. Because the records we obtained for the Landis sample didn't contain individual ages, it was not possible to compare the samples' ages, but the average age, which was reported in the 1940 book suggests that the age distributions in the two studies were likely comparable. For both samples Pearson product-moment correlations were made between CUMD, height, and the occurrence of orgasm in intercourse for each sample and for a combined sample of all of the data.
To assess whether CUMD is an effective diagnostic for predicting the likelihood that a woman will experience orgasm in intercourse, Receiver Operator Characteristic (ROC) curve functions (Griner, et al., 1981; Zweig and Campbell, 1993) were calculated for each sample and the combined sample. ROC curve functions determine how much the test factor, CUMD in this case, predicts the value of the dependent factor, orgasm in intercourse in this study, expressed as the area under the ROC curve that results from the relationship. A chance relationship accounts for 0.5 of the area under the curve. Accounting for 1.0 of the area under the curve means that the test variable perfectly predicts the dependent variable. A probability estimate of the likelihood that the indicated area under the curve accounted for occurred by chance is generated by the ROC function allowing comparisons of different areas from different populations.
We tested whether CUMD can accurately classify individuals by performing discriminant analysis on CUMD to predict orgasm in intercourse. We performed two analyses, in the first, data from the Bonaparte sample were used to generate the discriminant function and that function was then used to classify both the Bonaparte and Landis subjects. The second analysis reversed the process using the data from the Landis sample to generate the discriminant function and then using that function to classify individuals in both data sets. Whether the discriminant function classified subjects significantly better than chance was assessed using Press's Q statistic (Chan, 2005) calculated as follows:
N = total sample size
n = number of observations correctly classified
K = number of groups
Press's Q is distributed as a Chi-square with K-1 degrees of freedom.
Although the previous data allows directional predictions, two-tailed probabilities were used with a p<=0.05 considered significant. Where appropriate, effects sizes (Cohen's d, Cohen, 1992) were calculated for group differences. Unless stated otherwise all data are presented as mean±S.E.M. (standard error of the mean).
Results
Sample characteristics
The Bonaparte (Narjani, 1924) and Landis (Landis, Landis, and Bowles, 1940) samples differed in subject height with the Bonaparte sample being taller than the Landis sample (Bonaparte=64±2.6in, Landis=63±1.8in, t65=2.1, p=0.038, d=0.5). Similarly, CUMD measurements differed between the two studies with the Bonaparte sample having significantly smaller CUMD measurements than did the Landis sample (Bonaparte=2.3±0.1cm, Landis=2.9±0.1cm, t76=4.8, p<0.001, d=1.1). Figure 3 represents the frequency distribution of CUMD in the two samples, showing that the Bonaparte sample had shorter distances than did the Landis sample with no overlap at the extremes. Whether this reflected an actual difference in the two samples or a consistent difference in how CUMD was measured cannot be directly determined from the methods described in the two articles. However it seems likely that the Landis measurement may have included the clitoral glans, whereas the Bonaparte measurement, having been taken from the underside of the clitoral glans, did not. Thus Bonaparte's CUMD measurements would be shorter than the Landis CUMD measurements. We tested this hypothesis by subtracting 0.5cm, the approximate length of the clitoral glans (Verkauf, Von Thron, and O'Brien, 1992) from the Landis CUMD measures and compared these derived CUMDs to those reported by Bonaparte. This eliminated the difference in average CUMD (Bonaparte=2.3±0.1cm, Landis=2.4±0.1cm, t76=0.8, p=0.46, d=0.2). It thus seems likely that there were systematic differences in measurement methodology that contributed to differences in CUMD between the two samples. However, because we cannot be certain that this was the case, we used the original measurements as reported in the raw data of each study for all subsequent analyses.
Figure 3.
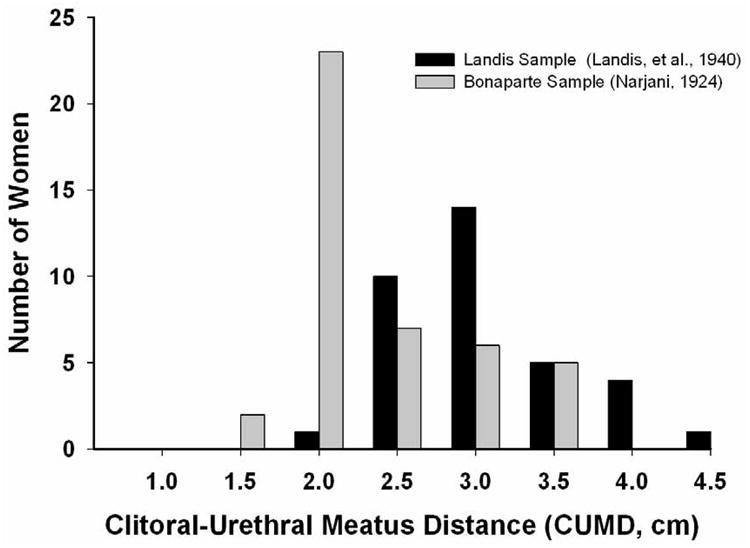
The distribution of CUMD measures in the Bonaparte (Narjani, 1924) and Landis (Landis, Landis, and Bowles, 1940) samples. The Bonaparte sample (N=43) had significantly shorter CUMDs than did the Landis sample (N=35) possibly reflecting a difference in the clitoral measuring point used in the two studies.
Height and CUMD were strongly correlated in the Bonaparte sample (r=0.8, n=38, p<0.001), but not in the Landis sample (r=0.2, n=29, p=0.3) suggesting that in addition to any systematic measurement differences, the two samples also differed in subject characteristics.
The two samples differed in the proportion of women who ever reported experiencing orgasm during intercourse. In the Bonaparte sample 65% of women reported experiencing orgasm during sexual intercourse compared to 83% of women in the Landis sample (χ2=3.8, df=1, p=0.05). However, only 46% of women in the Landis sample reported routinely experiencing orgasm in intercourse (67% or more of the time) which was not significantly different from the 65% of women in the Bonaparte sample reporting having orgasm in intercourse (χ2=2.3, df=1, p=0.13). We do not know what criteria Bonaparte's subjects used when determining whether they experienced orgasm in intercourse, but it seems likely that their “yes” response would reflect regular orgasm in intercourse and not whether such orgasm had ever occurred. Thus it appears that the two samples did not differ overall in the proportion of women who usually experience orgasm in intercourse.
Relationship between orgasm and CUMD
The relationship between the reported occurrence of orgasm during intercourse and CUMD was investigated by determining whether women in each sample who reported orgasm in intercourse had shorter CUMD measurements than did women who never reported orgasm in intercourse. This comparison was made for women who ever reported orgasm in intercourse or reported orgasm with intercourse 67% or more of the time. For the Bonaparte sample, both”ever” and 67% or greater have the same distribution, thus there is only one comparison possible and this showed that women who reported orgasm in intercourse (O) had significantly shorter CUMD measures than did women who did not report experiencing orgasm during intercourse (NoO) with an effect size greater than two standard deviation units (O=2.0±0.1cm, NoO=2.8±0.1cm; t41=7.5, p<0.001; d=2.2, Figure 4). For the Landis data, there was a nearly significant difference in CUMD for women who had ever reported orgasm during intercourse, compared to women who had never reported orgasm in intercourse and the corresponding effects size was moderate (O=2.9±0.1cm, NoO=3.1±0.3cm; t33=2.0, p=0.054;d=0.5).
Figure 4.
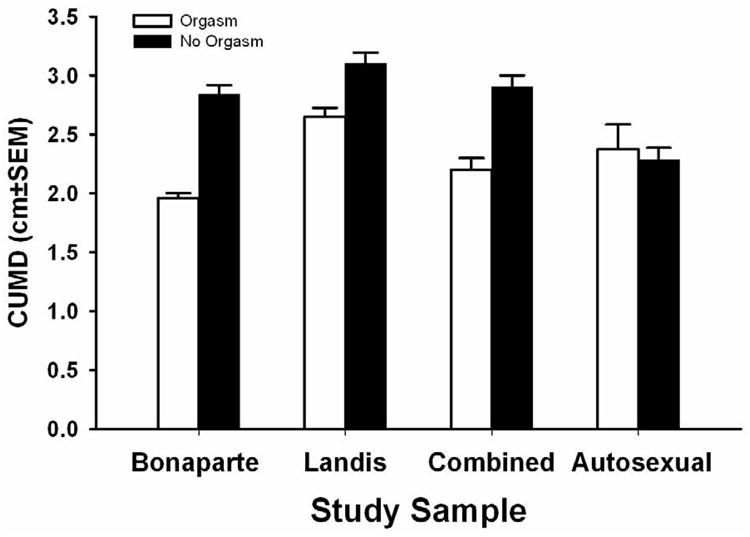
Average CUMD measurements in the Bonaparte and Landis samples for those women routinely experiencing orgasm in intercourse (orgasm 66% of the time or more) and those not, or experiencing orgasm in intercourse less than 67% of the time (Landis sample). Data are shown for the samples combined and for the CUMD measurements of women in the Bonaparte sample experiencing autosexual orgasms. For the Bonaparte, Landis and Combined samples the differences are statistically significant, although the magnitude of the difference is substantially greater in the Bonaparte than the Landis sample. The difference in CUMD for the autosexual sample is not statistically significant.
When only those women in the Landis sample who reported orgasm in intercourse more than 66% of the time (MoreO) were compared to women reporting less regular or no orgasm in intercourse (LessO), the results were very comparable to those found using the Bonaparte data with women reporting regular orgasm in intercourse having significantly smaller CUMD measurements and a large effect size (MoreO=2.7±0.1cm, LessO=3.1±0.1cm; t33=2.5, p=0.018; d=0.9, Figure 4). When CUMD measurements from women regularly experiencing orgasm in intercourse (RegularO; defined as more than 67% of intercourse with orgasm in either sample) were combined from both samples and compared to the CUMD measurements of women with less regular orgasm in intercourse (Less RegularO) the women regularly experiencing orgasm had significantly smaller CUMD measurements with a large effect size describing the difference (RegularO=2.2±0.1cm, Less regularO=2.9±0.1cm; t76=6.5, p<0.001; d=1.5, figure 4). Thus for each sample and for the combined sample women who report regularly experiencing orgasm in intercourse had substantially shorter CUMD measurements than did women not reporting experiencing orgasm or experiencing orgasm in intercourse less than 2/3 of the time they have intercourse.
The Bonaparte and Landis samples did not agree in the absolute CUMD measurement associated with the occurrence of orgasm in intercourse having a mean difference of 0.7cm in CUMD for women who regularly experienced orgasm in intercourse. In all cases the CUMD measures in the Bonaparte were shorter than in the Landis sample, which likely reflects that Bonaparte used the clitoral frenulum as her measuring point for the clitoris, whereas the Landis group likely used the clitoral glans. This methodological difference would make the Landis sample CUMD measurements consistently longer than the Bonaparte sample CUMD measurements.
We further investigated the relationship between CUMD and orgasm in intercourse by correlating CUMD with the occurrence of orgasm in intercourse. In both sets of data CUMD was significantly correlated with reported occurrence of orgasm in intercourse (Bonaparte: r=0.8, n=43, P<0.001; Landis: r=0.4, N=35, P=0.018). Combining the two samples revealed a strong relationship between regular orgasm (more than 67% of intercourse resulting in orgasm) in intercourse and CUMD (r=0.6, N=78, p<0.001). Thus both mean differences in CUMD as well as correlations between CUMD and orgasm provide strong evidence of a relationship between CUMD and the regular occurrence of orgasm in intercourse.
This relationship between CUMD and orgasm was not evident for autosexual orgasms. The Bonaparte sample contained data for 33 of the 43 women on the occurrence of orgasm from masturbation (autosexual orgasm). Of these 33 women, 79% experienced autosexual orgasms (AO), but their CUMDs did not differ from women who didn't experience autosexual orgasms (NoAO), (AO=2.4±0.2cm, NoAO=2.3±0.1cm; t31=0.4, p=0.7; d=0.2, figure 4). This finding is consistent with CUMD influencing orgasm in sexual intercourse and being unrelated to the occurrence of orgasm in general.
Receiver Operator Characteristic curves
To determine whether CUMD reliably predicts orgasm in intercourse we calculated Receiver Operator Characteristic (ROC) curves, a technique developed for signal detection, but often used to assess the validity of medical diagnoses (Hanley and McNeil, 1982, 1983; Zweig and Campbell, 1993). In ROC curves, the area accounted for under the curve by the test variable is the principle measure of whether the test variable, CUMD in this case, distinguishes between two outcomes, orgasm in intercourse or not in this case. Figure 5 illustrates that CUMD accounted for a significant proportion of area under the curve in both samples, supporting the claim that CUMD accurately distinguishes between regular and less regular orgasm in intercourse. In the Bonaparte sample (Figure 5a) 0.9±0.1, p<0.001 of the area under the ROC curve was accounted for by CUMD, while in the Landis sample (Figure 5b) CUMD accounted for 0.7±0.1, p=0.023 of the area under the ROC curve. While both show significant predictive value the Bonaparte data show a greater predictive value than do the Landis data.
Figure 5.
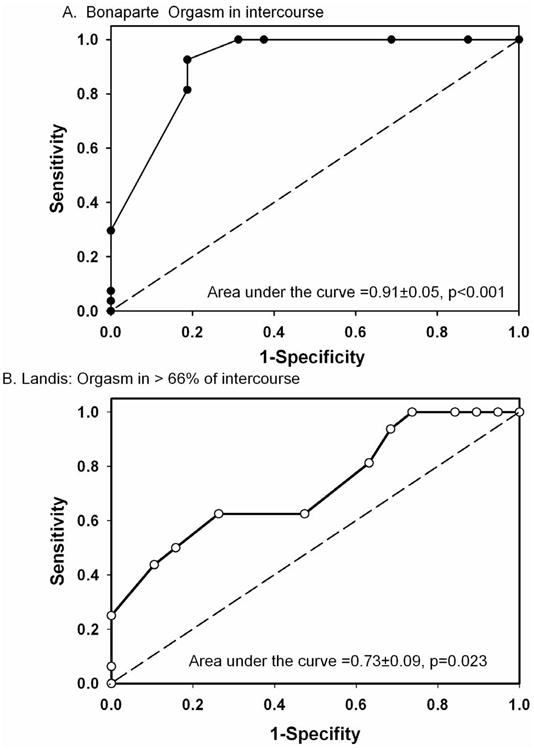
Receiver Operating Characteristic curves (ROC) for the relationship between CUMD and orgasm in intercourse for the Bonaparte (5a) and Landis samples (5b). Although both ROCs accounted for significant area under the curve, the Bonaparte sample accounted for more area than did the Landis sample and showed greater sensitivity and specificity. The dashed diagonal like represents 0.5 area under the curve, which would reflect a chance relationship between CUMD and orgasm in intercourse.
The ROC curve for the Bonaparte sample indicates that a CUMD less than or equal to 2.4cm would encompass 93% of the true positive cases (women who actually report orgasm in intercourse), with only 19% false positives (Women classified as having orgasm in intercourse, but who don't actually experience such orgasms). The ROC curve from the Landis data (Figure 5b) deviates less from the diagonal that indicates 0.5 area under the curve than does the Bonaparte ROC curve. This is reflected in the balance of true positives and false positives for the Landis data where the best balance between true and false positives occurs for a CUMD of 2.7cm or less which would encompass only 63% of the true positives and have a false positive rate of 26%. Thus the Landis data distinguish between the two groups of women much less reliably than do the Bonaparte data. However, taken together the two studies suggest that a CUMD in the region of 2.5cm distinguishes between those women likely to experience orgasm in intercourse and those where such orgasm is unlikely to occur. Whether the difference in diagnostic power between the two samples reflects subject selection, in that the Bonaparte data were biased towards shorter CUMD size than the Landis sample, or whether this reflects differences in how genital measurements in the two studies were collected cannot be determined. However, both samples suggest that CUMD provides substantial information for predicting whether or not a woman will experience orgasm in intercourse.
We calculated an ROC curve on data from the Bonaparte sample for the relationship between CUMD and the likelihood of reaching orgasm from masturbation. The ROC curve accounted for 0.5±0.1, p=0.86 of the area under the curve, almost exactly what would be expected by chance Table 1 illustrates how a CUMD cutoff value of 2.5cm would partition subjects having orgasms in intercourse according to CUMD. Data for autosexual orgasms are provided for comparison. Using a 2.5cm cutoff, only the Bonaparte sample distributed the subjects experiencing orgasm in intercourse differently than would have been expected by chance given the distribution of subjects with CUMD measures greater than 2.5cm. The 2.5cm cutoff did not distribute women experiencing orgasm in intercourse in the Landis sample differently than chance, although there was a strong trend towards identifying such women (p=0.11). CUMD was no better than chance in predicting which women in the Bonaparte sample experienced orgasm during masturbation (p=0.65). These results support that knowing a woman's CUMD does not provide information allowing accurate prediction of whether or not she experiences autosexual orgasms, but can provide substantial information for predicting the occurrence of orgasms in intercourse.
Table 1.
Percentage of women experiencing orgasm in relation to whether their CUMD measurement is greater than or equal to 2.5cm, or less than 2.5cm. (For the Landis sample “orgasm” is those women experiencing orgasm in intercourse greater than 66% of the time.)
| CUMD >= 2.5cm | CUMD < 2.5CM | Chi-square | |
|---|---|---|---|
| Bonaparte Sample - Orgasm in intercourse | 88% | 0% | X2=9.3,df=1, p=0.002 |
| Landis Sample – Orgasm in intercourse | 73% | 33% | X2=2.6, df=1, p=0.11 |
| Bonaparte Sample -Autosexual orgasm | 75% | 89% | X2=0.2, df=1, p=0.65 |
Discriminant analysis
Lastly we asked whether CUMD could be used to accurately classify individuals into those who have orgasm in intercourse and those who do not. Because of the continuous nature of the orgasm measurement in the Landis sample we used the data on those women who experienced orgasm in intercourse 67% of the time or greater as women having orgasm in intercourse. When the discriminant function was generated using data from the Bonaparte sample a significant Eigenvalue of 1.37 (Wilks lambda = 0.42, X2=34.9, df=1, p<0.001) was generated, which indicated strong discrimination between the groups. Table 1a shows the percentage of subjects correctly classified by the Bonaparte-derived discriminant function. The function correctly classified 88% of the women in the Bonaparte sample which is significantly different from chance (Press's Q= 26.3, df=1, p<0.001). Similarly, 81% of the 16 women (Press's Q=6.25, df=1, P=0.025) in the Bonaparte sample who reported not having orgasm in intercourse and 93% of the 27 women (Press's Q= 19.6, df=1, p<0.001) who did were correctly classified. For the Landis sample, the Bonaparte-derived discriminant function correctly classified 90% of the 19 women (Press's Q= 11.8, df=1, p=0.001) who reported orgasm in intercourse less than 67% of the time, but only 44% of the women(Press's Q= 0.25, df=1, p=0.62) who reported having orgasm in intercourse 67% or more of the time. Thus for both samples the Bonaparte-derived discriminant function was successful in classifying those women who did not have orgasm in intercourse, but less successful, as least in the Landis sample, in classifying those women who had orgasm in intercourse more than 67% of the time.
When the discriminant function was generated using data from the Landis sample a smaller, but still significant Eigenvalue of 0.19 (Wilks lambda = 0.84, X2=5.6, df=1, p<0.036) was obtained indicating weaker discrimination between the groups than with the Bonaparte-derived function. The Landis-derived discriminant function correctly classified only 69% of the women in the Landis sample, which is not significantly different from chance (Press's Q= 4.8, df=1, p<0.056). The Landis-derived discriminant function did not classify better than chance women in the Landis sample who reported having orgasm in intercourse less than 67% of the time or women who reported having orgasm in intercourse more than 67% of the time (Table 1b). By contrast, the Landis-derived sample better classified the Bonaparte-sample women than it did the Landis-sample women, successfully classifying 86% of the women into the appropriate group (Press's Q= 22.3, df=1, p<0.001). In addition, the Landis-derived discriminant function correctly classified 100% of the Bonaparte-sample women who reported having orgasm in intercourse, but did not classify women who failed to experience orgasm in intercourse any better than chance (Table 1b, Press's Q=1, df=1, p=0.63).
These data show that CUMD can be used to accurately classify women according to the likelihood that they will have orgasms in intercourse. However, CUMD's power as a diagnostic tool is limited in these data. Both discriminant functions very accurately classified women in the Bonaparte sample who reported experiencing orgasm in intercourse, but did poorly in making the same classification in the Landis data. By contrast, both discriminant functions better classified women in the Landis sample who reported experiencing orgasm in intercourse less than 67% of the time. However, even in this case only the Bonaparte-derived discriminant function classified these women better than chance.
Discussion
Data from two independent samples, collected over 70 years ago and more than 15 years apart, support the notion that the distance between a woman's clitoris and her vagina influences the likelihood that she will regularly experience orgasm solely from intercourse. Women who reported more regularly experiencing orgasm had shorter CUMD measurements than did women who reported not experiencing or less regularly experiencing, orgasm in intercourse. When orgasms from masturbation were considered there was no meaningful relationship between CUMD and whether or not a woman experienced autosexual orgasms. Thus the influence of CUMD on women's orgasms is likely limited to orgasms solely from sexual intercourse. These results suggest that some of the variability in women experiencing orgasm from intercourse without concurrent clitoral stimulation reflects, as Bonaparte suggested in 1933, the consequences of embryological processes that determine the position of the clitoris relative to the vagina. Thus, some women may be anatomically predisposed to experience orgasm from intercourse, while the genital anatomy of other women makes such orgasms unlikely. While other factors, such as the sexual characteristics of a woman's partner, undoubtedly influence the likelihood of experiencing orgasm solely from intercourse, these data suggest that for some women their genital anatomy strongly influences the occurrence of orgasm in intercourse.
ROC and discriminant analysis revealed that CUMD can serve as a reliable and sensitive predictor of the likelihood that a woman will experience orgasm in intercourse. The two studies differed in the strength of this prediction with the Bonaparte sample providing better prediction and classification than does the Landis sample. This difference between the two studies may reflect how the genital measurements were obtained. If as we suspect, Bonaparte used the frenulum of the clitoris as her clitoral marker while Landis and colleagues used the tip of the clitoral glans, one would expect much more variation in CUMD between subjects using the Landis method because the clitoral glans is larger and more variable than is the frenulum (Verkauf, et al., 1992; Lloyd, et al., 2005). The frenulum is essentially a single point at the base of the clitoral glans, and thus would vary much less between subjects than would the clitoral glans. Thus the stronger relationship between CUMD and orgasm in intercourse in the Bonaparte study may simply reflect that she measured the same genital construct in all subjects, whereas the Landis technique may have had much greater inherent variance which reduced or obscured the magnitude of the relationship between CUMD and orgasm.
While the conclusion that a woman's genital configuration influences her likelihood of experiencing orgasm in intercourse has implications for women's sexual experience, caution in accepting this interpretation is warranted given possible bias in data collection. Although Bonaparte's data show a much stronger relationship between CUMD and orgasm than do the Landis data, Bonaparte apparently collected all of the data herself and she was certainly not blind to her hypothesis. In addition, Bonaparte was personally invested in finding that orgasm in intercourse was affected by clitoral location as she was looking for an explanation for her own inability to experience orgasm in intercourse. By contrast, although Landis and his colleagues were aware of Bonaparte's hypothesis, they were also aware of Dickinson's refutation of that hypothesis, citing both works in their book. It is thus unlikely that the Landis team had a particular bias in this aspect of their study. In addition, the Landis data were less easily biased since CUMD measures were collected by a doctor separate from the investigators collecting the interview data. In addition, the genital examination data and the interview data were recorded in separate documents and collected at different times. It is thus possible that the Landis data are more objective and less biased than the Bonaparte data, and that is why they also show a weaker relationship between CUMD and orgasm in intercourse. They do, however, show a statistically significant and relatively large relationship in the same direction as that found by Bonaparte. Thus we think it likely that the differences between the two studies in the strength of the relationship between CUMD and orgasm likely reflect genital measurement differences instead of biased data collection. Landis and colleagues replication of Bonaparte's finding 16 years later using a completely different research team in a completely different environment makes us more confident of the validity of the relationship between CUMD and orgasm despite the challenges these data present. Unresolved, however, is the different distribution of CUMD measurements in the two studies.
Bonaparte's women have CUMD measurements that average about 0.5cm shorter than those in the Landis sample and have a modal CUMD of 2cm compared to a modal CUMD of 3.0cm in the Landis sample. Thus the stronger relationship between CUMD and orgasm in the Bonaparte sample may not reflect bias, but simply that her sample had more women with shorter CUMDs. There is evidence that the Bonaparte and Landis CUMD measurements were likely collected using different methods and that the one that Landis likely used would produce both increased variability and a mean length difference of about 0.5cm, the length of the clitoral glans. However, given the limited information we have it is not possible to fully explain the differences between the two studies in the distributions of the CUMD measurements. Still, the consistent positive relationship between CUMD and orgasm in intercourse in both studies warrants further discussion, particularly what it implies about genital development how developmental differences might contribute to our understanding of variation in the ways in which women reach orgasm.
Neither of these studies address whether there is a “vaginal” orgasm triggered by vaginal stimulation, as opposed to a “clitoral” orgasm triggered by external clitoral stimulation. Similarly, these results do not resolve whether orgasm in intercourse for women with short CUMDs results from vaginal stimulation, from direct penile stimulation of the clitoral glans, from indirect clitoral stimulation though pelvic pressure, from stimulation of internal aspects of the clitoral complex, or from some combination of all of these. Any of these sources of stimulation could possibly produce the higher incidence of orgasm in intercourse found in women with shorter CUMD measurements.
One possibility, originally suggested by Bonaparte (Narjani, 1924), is that a shorter distance between the clitoris and the vagina facilitates direct clitoral-penile contact during sexual intercourse. This explanation is plausible given the configuration between penile shape and clitoral location as revealed in MRI or ultrasound images of men and women during coitus (Schultz, et al., 1999; Buisson, et al. 2010). However, without evidence of increased direct penile-clitoral contact during intercourse in women with shorter CUMD measurements it is not possible to conclude whether this is the mechanism through which CUMD affects orgasm in intercourse. Although the notion of pelvic or penile stimulation of the clitoral glans or shaft is intuitively appealing and is consistent with the data presented here, short CUMD, instead of being the actual mechanism increasing orgasm in intercourse, could be an external marker of other processes producing increased vaginal sensitivity that increases the likelihood of orgasm solely from sexual intercourse.
The clitoris consists of more than the shaft and clitoral glans. The majority of clitoral anatomy is internal, consisting primarily of two clitoral bodies and two clitoral bulbs that partially surround the vagina and form a vaulted structure above the anterior vaginal wall (O'Connell, et al., 1998; Suh, et al., 2003; O'Connell, Sanjeevan, and Hutson, 2005; Buisson, Foldes, and Paniel, 2008; Foldes and Buisson, 2009; O'Connell, et al., 2008). This small area appears to be erotically responsive as when Foldes and Buisson (2009) asked five women to “press with their fingers on their most pleasurable anterior vaginal area” during an ultrasound of their genitals, the ultrasound visualization of the pressing finger was near the double vaulted structure formed by the clitoral bulbs and bodies. Similarly, the internal clitoral structures are capable of participating in women's sexual arousal and orgasm as the anterior vaginal wall transmits penile force to these clitoral structures (Ingelman-Sundberg, 1997). In this regard, smaller CUMD may both represent a shorter distance between the clitoral glans and the vagina, but may also reflect that the bulbs and bodies of the clitoris are packed into a smaller volume pressing closer to the vagina. This compact spatial arrangement could result, for example, in more direct contact between the anterior vaginal wall and the erotically sensitive bulbs or bodies of the clitoris. This more direct contact between the vagina and portions of the clitoris distal to the shaft and glans produces increased vaginal sensitivity that is unlikely or impossible if these clitoral structures are distributed through out a larger volume. Thus shorter CUMD would not directly affect external clitoral stimulation, but would be a proxy for increased vaginal sensitivity and an increased likelihood that vaginal stimulation can produce orgasm even if there is no increased penile stimulation of the clitoral glans or shaft during sexual intercourse.
The possibility that vaginal stimulation acts on deep clitoral structures offers an interesting counterpoint to Freud's conceptualization of “vaginal” and “clitoral” orgasms and would support Sherfey's (1972) contention that all women's orgasms are the result of clitoral stimulation. However, this view would not support Master's and Johnson's (1966) contention that all women's orgasms during intercourse result from penile traction on the woman's labia minora pulling them across the clitoral glans to produce clitoral stimulation during intercourse. Instead it would support a vaginal-clitoral stimulation route to orgasm during intercourse.
Freud's (1905) theory of women's sexual development focused on the type of genital stimulation producing female orgasm. Freud contrasted orgasms from vaginal responsiveness with clitorally-induced orgasms, by which he meant orgasms resulting from stimulation of the external aspects of the clitoris. Ironically, Freud's distinction between vaginally- and clitorally-triggered orgasms may actually reflect a natural typology of women's orgasm induction. This typology has nothing to do with psychological maturity as Freud argued, but instead contrasts women who reach orgasm through vaginal stimulation of deep clitoral structures with women who reach orgasm through stimulation of external clitoral structures of the shaft or glans. However, Freud, by valuing vaginal induction of orgasm over external clitoral induction has likely negatively affected many women and impeded investigation of the sources of this natural variation in women's sexual arousal and orgasm. The results of the studies analyzed here suggest that these two different forms of orgasm induction might reflect which anatomical aspects of the clitoris have primary erotic sensitivity.
Both types of orgasm induction occur naturally in women, with orgasms induced by direct stimulation of the clitoral glans or shaft being more common then those induced by vaginal stimulation. Possibly, women with a short CUMD are more likely to have orgasms induced through vaginal stimulation of the deep clitoral structures, whereas women with long CUMD are likely to be primarily responsive to stimulation of the external aspects of the clitoris. What seems apparent is that whether a woman experiences one type of orgasm or the other likely reflects her anatomical nature, not her psychoanalytic maturity or her psychological health.
The source of anatomical variation in clitoral placement was speculated on by Bonaparte and the notion that the differences in CUMD result from embryological processes particularly intrigued her (Narjani, 1924). She noted that the range of variation in the distance of the clitoris from the vagina in women exceeded that seen in other species, such as the cow and the dog, and even in nonhuman primates, where the clitoris was located quite near the vagina. Only in humans, she argued, was there great variation in the separation between the two genital structures (Narjani, 1924). Interestingly, Bonaparte suggested that this variation resulted from embryological events, and she was aware that the genital tubercle migrates rostrally in men during prenatal development. She noted that the genitals of girls are similar to those of boyd around the 9th or 10th week of gestation before the genital tubercle has migrated very far rostrally leaving it in a more caudal location (Narjani, 1924). She argued further that women with long CUMD measurements, téléclitoridiennes in her terminology, had their clitoral migration arrested later in embryological development, resulting in the location of their genital tubercle a bit more like that of a male even though their urinary meatus remained in its female-typical location (Narjani, 1924). It is unclear how Bonaparte developed this very modern theory of prenatal genital development, but today we would find her conclusions consistent with the notion that women with longer CUMD measures have been exposed to higher levels of prenatal androgens than have women with smaller distances.
Bonaparte suggested that variation in CUMD likely reflects the timing of the cessation of rostral migration of the woman's genital tubercle during prenatal life. This migration is necessary in males to produce the much more rostral location of the penis necessary for successful sexual intercourse. Genital tubercle migration occurs in mammalian males and studies in animals show that prenatal androgens control this migration. Females, in a variety of species, treated with male-like levels of androgen develop male-like external genitalia with a rostrally-located penis (summarized in Wallen, and Baum, 2002). In rhesus monkeys low levels of testosterone administered to pregnant females when the genitals are differentiating (gestational days 35-70) resulted in their daughters having clearly female genitalia, but with an increased clitoris to vagina distance compared to females from untreated mothers (Herman, Jones, Mann, and Wallen, 2000). It seems likely that small endogenous variations in prenatal androgens produce variation in CUMD and that longer CUMD reflects greater exposure to prenatal androgen and thus greater rostral migration of the genital tubercle.
While there is no direct evidence for the relationship between CUMD and natural variation in prenatal androgens in women there is such evidence in rats. Anogenital distance (AGD), the distance from the genital tubercle to the anus, a measure analogous to CUMD, is longer in female rats located in utero between or downstream from sibling males and thus exposed to the male's endogenously secreted testosterone (Clemens, Gladue, and Coniglio, 1978; Meisel and Ward, 1981). Such females have a longer AGD (i.e., more male-like) than do females not gestating near a male sibling (Clemens, Gladue, and Coniglio, 1978). In addition, prenatal treatment of pregnant female rats with flutamide, a nonsteroidal anti-androgen, eliminated the effects on AGD of a female gestating near a male sibling (Clemens, Gladue, and Coniglio, 1978), supporting the notion that small differences in endogenous prenatal androgen exposure affect AGD. Interestingly, natural variation in female rat AGD predicts better adult reproductive function and earlier (e.g. more feminine) pubertal onset with shorter AGD measures, presumably reflecting lower exposure to endogenous prenatal androgens (Zehr, Gans, and McClintock, 2001). Thus data from rats support the notion that AGD serves as a proxy for the degree of prenatal exposure to androgens. If CUMD is similarly affected by endogenous prenatal androgen variation, it may be an external indicator of a woman's exposure to prenatal androgens. If true, this suggests that women exposed to lower levels of prenatal androgens are more likely to achieve orgasm solely through intercourse than are women exposed to higher levels of prenatal androgens.
Variation in exposure to prenatal androgens may explain why clitoral size is much more variable in women than is penis size in men (Wallen, and Lloyd, 2008), suggesting that women are exposed to a wider range of androgen levels than are men. Particularly intriguing is the notion that orgasm solely from sexual intercourse seems most likely to occur in women who may have been exposed to the lowest levels of prenatal androgens. Exposure to higher levels of androgens does not preclude orgasm, but may result in easier orgasm from direct stimulation of the clitoral shaft or glans, than from stimulation of the vagina or internal clitoral structures in close proximity to the vaginal walls. Thus the clitoral and vaginal eroticism that Freud invested with substantial psychoanalytic importance, may exist, but simply reflect the extent to which a woman was prenatally exposed to androgens. Possibly variation in prenatal androgens produces other genital changes, in addition to rostral migration of the genital tubercle, that influence the type of stimulation a women requires for reaching orgasm.
In males the genital tubercle differentiates into the penis under the influence of prenatal androgens. In this process the primary erogenous areas of the penis become the underside of the glans penis, where the frenulum connects the foreskin to the glans penis and, to a much lesser extent, the penile shaft. Thus, although the penis enlarges substantially under the influence of androgens the parts which contribute to sexual sensations remain, or become, quite small. In females the genital tubercle, without the strong influence of androgens, migrates much less than in males and differentiates into the clitoris possibly with a more diffuse distribution of erotic sensitivity such that the clitoral bulbs and bodies as well as the shaft and glans are erotically responsive. Women who are exposed to higher levels of prenatal androgens may not only have a more male-like rostral clitoral location, but also their clitoral eroticism may become more similar to that of the penis. Thus, increased prenatal androgen exposure may focus erotic sensitivity to the clitoral shaft and glans reducing or eliminating erotic sensitivity in the bulbs and bodies of the clitoris. In this view, all women possess erotic sensitivity in the clitoral shaft and glans, but only women exposed to lower levels of prenatal androgens retain significant erotic sensitivity in the internal clitoral structures. CUMD size, which likely reflects the extent of prenatal androgen exposure, might also be a proxy for the erotic sensitivity of internal clitoral structures, and thus the likelihood that women will experience orgasm solely from intercourse.
These findings support CUMD as a potential proxy for prenatal androgen exposure in women and suggest a number of studies. The first is that CUMD should be positively correlated with clitoral size, since in males the rostral migration of the genital tubercle is combined with an increase in genital tubercle size. A second study would combine CUMD measures with imaging studies allowing reconstruction of internal pelvic volumes to identify the relationship between internal clitoral anatomy and the vagonal walls (Gravina et al, 2008). Such a study could support the notion that short CUMD measurements are associated with the packing of internal clitoral anatomy into a smaller space leading to more intimate contact between internal clitoral structures and the vaginal walls. Hypotheses offered here could be directly tested by investigating women with atypical prenatal androgen exposure. For example, women with complete androgen insensitivity (CAIS) resulting from not having functional androgen receptors, would be expected to have very short CUMD, with their internal clitoral structures packed into a much smaller volume than would women with typical androgen exposure. Women with CAIS would also be expected to more reliably experience orgasm in intercourse than women exposed to androgens. However this last possibility is complicated by the fact that women with CAIS typically have shorter vaginas than do women without CAIS (Minto, et al., 2003). We do not know how this might affect the relationship between the vaginal walls and the internal aspects of the clitoris. Women with congenital adrenal hyperplasia (CAH) could contribute significantly to our understanding of genital anatomical development and orgasm. One would predict that women with CAH would have much longer CUMDs than women without CAH and that their incidence of orgasm solely from intercourse would be lower than in women without CAH. Studies of same and mixed sex twins could directly test the hypothesis that small differences in prenatal androgen exposure affect CUMD, with women with female co-twins having smaller CUMD measurements than would women with male co-twins. Lastly, the findings of Bonaparte and Landis need to be replicated using an assessment of orgasm that clearly distinguishes orgasms during intercourse without concurrent clitoral stimulation from those with concurrent clitoral stimulation. A standardized method of measuring CUMD needs to be developed, possibly one which measures actual clitoral-vaginal distances, though the size and flexibility of the vaginal opening make this challenging. Such studies might explain the great variation among women in the sexually arousing stimulation necessary for orgasm and why some women more easily experience orgasm in intercourse than do others. Ultimately such studies could establish the factors that cause the natural variation in women's orgasms and possibly why men and women differ so markedly in the likelihood that they will experience orgasm solely from sexual intercourse.
Acknowledgments
Dr. Rachel Maines is thanked for starting this project by tracking down Marie Bonaparte's 1924 article, published under the pseudonym A.E. Narjani. Liana Zhou and Shawn C. Wilson of the Kinsey Institute for Research in Sex, Gender and Reproduction library are thanked for discovering the original Landis data sheets. Cecile J. Click is thanked for transcribing the Landis raw data from the original records. Daniella Sanchez is thanked for blind coding of the Landis data. Dr. Nancy Bliwise is thanked for introducing Receiver Operating Characteristic curves as an analytical tool. Dr. Harold Gouzoules is thanked for advice on the use of discriminant analysis. This work was supported in part by the Center for Behavioral Neuroscience, a Science and Technology Center Program of the National Science Foundation under agreement IBN-9876754.
Footnotes
Narjani is a pseudonym for the psychoanalyst Marie Bonaparte whose idea it was that the distance between the clitoris and vagina affects the likelihood of woman experiencing orgasm in intercourse. It is unclear why Bonaparte used the pseudonym, which she revealed, without explanation, in her 1933 paper (Bonaparte, 1933).
Bonaparte used the urethral meatus in preference to the vaginal opening apparently because she thought it to have a consistent distance from the vaginal opening and, being much smaller and less flexible than the vagina, it was easier to consistently measure. Her assumption that the urinary meatus was a constant distance from the vagina was likely incorrect as the urethra in women can be completely separate from the vagina or within the vaginal opening itself (Dickinson, 1933). However, CUMD has been used in all subsequent studies and there appears to be no study in which actual clitoral-vaginal distance has been measured.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Kim Wallen, Department of Psychology, Emory University, 36 Eagle Row, Atlanta, GA 30322
Elisabeth A. Lloyd, History and Philosophy of Science, Indiana University, Bloomington, IN
References
- Alzate H. Vaginal eroticism: a replication study. Arch Sex Behav. 1985;14:529–37. doi: 10.1007/BF01541753. [DOI] [PubMed] [Google Scholar]
- Bonaparte M. Les deux frigidités de la femme. Bulletin de la Société de Sexologie. 1933;5:161–170. [Google Scholar]
- Brody S, Costa RM. Vaginal orgasm is associated with less use of immature psychological defense mechanisms. J Sex Med. 2008;5:1167–76. doi: 10.1111/j.1743-6109.2008.00786.x. [DOI] [PubMed] [Google Scholar]
- Buisson O, Foldes P, Jannini E, Mimoun S. Coitus as Revealed by Ultrasound in One Volunteer Couple. J Sex Med. 2010 doi: 10.1111/j.1743-6109.2010.01892.x. epub ahead of print. [DOI] [PubMed] [Google Scholar]
- Buisson O, Foldes P, Paniel BJ. Sonography of the clitoris. J Sex Med. 2008;5:413–7. doi: 10.1111/j.1743-6109.2007.00699.x. [DOI] [PubMed] [Google Scholar]
- Chan C. Biostatistics 303. Discriminant analysis. Singapore Med J. 2005;46:54–61. [PubMed] [Google Scholar]
- Clemens LG, Gladue BA, Coniglio LP. Prenatal endogenous androgenic influences on masculine sexual behavior and genital morphology in male and female rats. Horm Behav. 1978;10:40–53. doi: 10.1016/0018-506x(78)90023-5. [DOI] [PubMed] [Google Scholar]
- Cohen J. A power primer. Psychological Bulletin. 1992;112:155–159. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- Dickinson R. Atlas of Human Sexual Anatomy. Williams and Wilkins; Baltimore, MD: 1933. [Google Scholar]
- Fisher S. The Female Orgasm: Psychology, Physiology, Fantasy. Basic Books; New York: 1973. [Google Scholar]
- Foldes P, Buisson O. The clitoral complex: a dynamic sonographic study. J Sex Med. 2009;6:1223–31. doi: 10.1111/j.1743-6109.2009.01231.x. [DOI] [PubMed] [Google Scholar]
- Freud S. Three essays on the theory of sexuality/Sigmund Freud; with a foreword by Nancy J Chodorow; with an introductory essay by Steven Marcus; translated and edited by James Strachey. Basic Books; New York: 1905. [Google Scholar]
- Goldfoot DA, Westerborg-van Loon H, Groeneveld W, Slob AK. Behavioral and physiological evidence of sexual climax in the female stump-tailed macaque (Macaca arctoides) Science. 1980;208:1477–9. doi: 10.1126/science.7384791. [DOI] [PubMed] [Google Scholar]
- Gravina GL, et al. Measurement of the thickness of the urethrovaginal space in women with or without vaginal orgasm. J Sex Med. 2008;5:610–8. doi: 10.1111/j.1743-6109.2007.00739.x. [DOI] [PubMed] [Google Scholar]
- Griner PF, Mayewski RJ, Mushlin AI, Greenland P. Selection and interpretation of diagnostic tests and procedures. Principles and applications. Ann Intern Med. 1981;94:557–92. [PubMed] [Google Scholar]
- Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36. doi: 10.1148/radiology.143.1.7063747. [DOI] [PubMed] [Google Scholar]
- Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148:839–43. doi: 10.1148/radiology.148.3.6878708. [DOI] [PubMed] [Google Scholar]
- Herman RA, Jones B, Mann DR, Wallen K. Timing of prenatal androgen exposure: anatomical and endocrine effects on juvenile male and female rhesus monkeys. Horm Behav. 2000;38:52–66. doi: 10.1006/hbeh.2000.1608. [DOI] [PubMed] [Google Scholar]
- Hite S. The Hite Report. Macmillan; New York: 1976. [Google Scholar]
- Ingelman-Sundberg A. The anterior vaginal wall as an organ for the transmission of active forces to the urethra and the clitoris. Int Urogynecol J Pelvic Floor Dysfunct. 1997;8:50–1. doi: 10.1007/BF01920294. [DOI] [PubMed] [Google Scholar]
- Kinsey A, Pomeroy W, Martin C. Sexual Behavior in the Human Male. WB Saunders; Philadelphia: 1948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kinsey A, Pomeroy W, Martin C, Gebhard P. Sexual Behavior in the Human Female. WB Saunders; Philadelphia: 1953. [Google Scholar]
- Kline-Graber G, Graber B. Woman's Orgasm. Bobs-Merrill Company, Inc.; New York: 1975. [Google Scholar]
- Komisaruk BR, Beyer-Flores C, Whipple B. The Science of Orgasm. The Johns Hopkins University Press; Baltimore, MD: 2006. [Google Scholar]
- Landis C, Landis A, Bowles M. Sex in Development. P.B. Hoeber Inc.; New York: 1940. [Google Scholar]
- Lloyd E. The Case of the Female Orgasm: Bias in the Science of Evolution. Harvard University Press; Cambridge, MA: 2005. [Google Scholar]
- Lloyd J, Crouch NS, Minto CL, Liao LM, Creighton SM. Female genital appearance: “normality” unfolds. BJOG. 2005;112:643–6. doi: 10.1111/j.1471-0528.2004.00517.x. [DOI] [PubMed] [Google Scholar]
- Marmor J. Some considerations concerning orgasm in the female. Psychosom Med. 1954;16:240–5. doi: 10.1097/00006842-195405000-00006. [DOI] [PubMed] [Google Scholar]
- Masters WH, Johnson VE. Human Sexual Response. Little Brown; Boston: 1966. [Google Scholar]
- Meisel RL, Ward IL. Fetal female rats are masculinized by male littermates located caudally in the uterus. Science. 1981;213:239–42. doi: 10.1126/science.7244634. [DOI] [PubMed] [Google Scholar]
- Meisel RL, Camp DM, Robinson TE. A microdialysis study of ventral striatal dopamine during sexual behavior in female Syrian hamsters. Behav Brain Res. 1993;55:151–7. doi: 10.1016/0166-4328(93)90111-3. [DOI] [PubMed] [Google Scholar]
- Meston CM, et al. Women's orgasm. Annu Rev Sex Res. 2004;15:173–257. [PubMed] [Google Scholar]
- Minto CL, Liao KL, Conway GS, Creighton SM. Sexual function in women with complete androgen insensitivity syndrome. Fertil Steril. 2003;80:157–64. doi: 10.1016/s0015-0282(03)00501-6. [DOI] [PubMed] [Google Scholar]
- Narjani A. Considerations sur les causes anatomiques de frigidite chez la femme. Bruxelles-Medical. 1924;27:768–778. [Google Scholar]
- O'Connell HE, Sanjeevan KV, Hutson JM. Anatomy of the clitoris. J Urol. 2005;174:1189–95. doi: 10.1097/01.ju.0000173639.38898.cd. [DOI] [PubMed] [Google Scholar]
- O'Connell HE, Eizenberg N, Rahman M, Cleeve J. The anatomy of the distal vagina: towards unity. J Sex Med. 2008;5:1883–91. doi: 10.1111/j.1743-6109.2008.00875.x. [DOI] [PubMed] [Google Scholar]
- O'Connell HE, Hutson JM, Anderson CR, Plenter RJ. Anatomical relationship between urethra and clitoris. J Urol. 1998;159:1892–7. doi: 10.1016/S0022-5347(01)63188-4. [DOI] [PubMed] [Google Scholar]
- Schultz WW, van Andel P, Sabelis I, Mooyaart E. Magnetic resonance imaging of male and female genitals during coitus and female sexual arousal. BMJ. 1999;319:1596–600. doi: 10.1136/bmj.319.7225.1596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sherfey MJ. The Nature and Evolution of Female Sexuality. Vintage Books; New York: 1972. [Google Scholar]
- Stone H, Stone A. A Marriage Manual. Simon and Shuster; New York: 1935. [Google Scholar]
- Suh DD, Yang CC, Cao Y, Garland PA, Maravilla KR. Magnetic resonance imaging anatomy of the female genitalia in premenopausal and postmenopausal women. J Urol. 2003;170:138–44. doi: 10.1097/01.ju.0000071880.15741.5f. [DOI] [PubMed] [Google Scholar]
- Thompson NL. Marie Bonaparte's theory of female sexuality:Fantasy and Biology. American Imago. 2003;60:343–378. [Google Scholar]
- van de Velde T. Ideal Marriage. Random House; New York: 1930. [Google Scholar]
- van de Velde T. Ideal Marriage. Random House; New York: 1965. [Google Scholar]
- Verkauf BS, Von Thron J, O'Brien WF. Clitoral size in normal women. Obstet Gynecol. 1992;80:41–4. [PubMed] [Google Scholar]
- Wallen K, Baum MJ. Masculinization and defeminization in altricial and precocial mammals: comparative aspects of steroid hormone action. In: Pfaff D, Arnold A, Etgen A, Fahrbach S, Rubin R, editors. Hormones, Brain, and Behavior. four. Elsevier; 2002. pp. 385–423. [Google Scholar]
- Wallen K, Lloyd EA. Clitoral variability compared with penile variability supports nonadaptation of female orgasm. Evol Dev. 2008;10:1–2. doi: 10.1111/j.1525-142X.2007.00207.x. [DOI] [PubMed] [Google Scholar]
- Zehr JL, Gans SE, McClintock MK. Variation in reproductive traits is associated with short anogenital distance in female rats. Dev Psychobiol. 2001;38:229–38. doi: 10.1002/dev.1017. [DOI] [PubMed] [Google Scholar]
- Zweig MH, Campbell G. Receiver-operating characteristic (ROC) plots: a fundamental evaluation tool in clinical medicine. Clin Chem. 1993;39:561–77. [PubMed] [Google Scholar]