

Abstract
The reconstruction of full-thickness chest wall defects is a challenging problem for thoracic surgeons, particularly after a wide resection of the chest wall that includes the sternum. The location and the size of the defect play a major role when selecting the method of reconstruction, while acceptable cosmetic and functional results remain the primary goal. Improvements in preoperative imaging techniques and reconstruction materials have an important role when planning and performing a wide chest wall resection with a low morbidity rate. In this report, we describe the reconstruction of a wide anterior chest wall defect with a patient-specific custom-made titanium implant. An infected mammary tumour recurrence in a 62-year old female, located at the anterior chest wall including the sternum, was resected, followed by a large custom-made titanium implant. Latissimus dorsi flap and split-thickness graft were also used for covering the implant successfully. A titanium custom-made chest wall implant could be a viable alternative for patients who had large chest wall tumours.
Keywords: Chest wall resection, Reconstruction, Implant, Thoracic surgery
INTRODUCTION
Currently, wide resections of chest wall can be achieved with acceptable morbidity and mortality rates with the aid of improved surgical techniques, anaesthesia, intensive care and reconstruction materials. The most important functional steps in the reconstruction include covering the defect, protecting the underlying vital structures and preserving respiratory dynamics. In this study, we present a patient who underwent wide chest wall and partial sternal resection and reconstruction with a patient-specific titanium implant.
TECHNIQUE
A 62-year old female was admitted to the hospital with a mass located at the anterior chest wall associated with foul smelly drainage (Fig. 1A). She had a history of right radical mastectomy for breast cancer in 2010. The computerized tomography (CT) revealed a mass invading the manubrium, corpus sterni, bilateral clavicules, first three ribs on the left side and first four ribs on the right side. There was no invasion to the vascular structures of the mediastinum (Fig. 1B). The CT of the chest also revealed bilateral metastatic lung nodules. The PET-CT showed no distant metastasis other than bilateral lung parenchyma. The resection of the chest wall tumour was decided in order to avoid any septic complication and not for a curative purpose. Cranial magnetic resonance imaging was performed for metastatic work-up for the patient. The result was negative for metastasis.
Figure 1:

Preoperative view of the chest wall tumour. The mass involves the skin and anterior chest wall including manubrium sterni (A). The preoperative computed tomographic scan of the patient reveals no invasion to the vascular structures of the mediastinum. It also shows that most parts of the anterior chest wall bone structures were invaded by the mass (B). The resection plan was marked on the 3D reconstruction of the computed tomography scan (C).
Multislice CT Computed tomography (CT) images were obtained by using a 64 detector CT scanner (Aquilion 64, Toshiba Medical Systems, Otawara, Japan), while the patient was in the supine position. CT scan image outputs were dicom (.dcm) files. By software Materialise Mimics ver 16.0 (Materialise Medical Co, Leuven, Belgium) the dicom (.dcm) files were converted into .stl files. Then the implant model was digitally designed with softwares (3-matic 8.0, Magic RP 17.02, Materialise Medical Co, Leuven, Belgium) by a METUM specialist (investigator) in MEDMC (Medical Design and Manufacturing Center, GATA).
After approval by the surgical operator, the digital 3D implant model was transferred to selective metal Laser sintering (SLM) machine (M2 cusing, Concept Laser GmbH, Hoffman Grp., Lichtenfelds, Germany). The implant structure generated from powder Ti6Al4V ELI Grade 23 (Cl 41 Ti, Concept Laser GmbH, Hoffman Grp., Lichtenfelds, Germany) under %99.9 argon atmosphere according to the manufacturer's instructions. Then the implant was exposed to heat treatment by a special normalization owen (Proterm ACF 12/45, Alserteknik, Ankara, Turkey) also under 99.9% argon atmosphere according to the manufacturer's instructions for normalization.
After burnishing and polishing processes the implant structure was sandblasted with AlO particles (Korox, BEGO, Bremen, Germany) 250, 110, 50 micron particle size respectively. Then ultrasonic bath procedure was performed before the sterilization process for the surgical operation.
The size and shape of the implant were designed to reconstruct the chest wall after a wide resection which was 3 cm away from the tumour margins.
During the operation, a large circular incision with a diameter of 15 cm was made around the tumour mass. The clavicles, first three ribs on the left side and first four ribs on the right side, the manubrium sterni and two-third of the corpus sterni (Fig. 2a) were resected along with the pectoralis major and latissimus dorsi muscles. Frozen section analysis of margins confirmed the complete resection (i.e. all margins were tumour free). These margins were ∼1–2 cm away from the tumour because the mass was not the primary tumour of the sternum. The titanium implant was made in the same shape as the thoracic bony structure of the patient, according to the reconstructed images of the thorax CT of the patient and was 2–3 mm thick, weighed 160 g and included drainage holes on the surface. This implant was produced by Concept Laser M2 Cusing Machine (Hofmann Innovation Group, Germany) at our Medical Design and Production Center. The skeletal anatomy of the anterior chest wall was provided following the planned full thickness resection of the chest wall (Fig. 2B). The placement and fixation of the implant were straightforward and accomplished without a major difficulty. The securement of the implant was achieved with steel wire sutures to the remaining ribs and clavicles. The soft tissue reconstruction was performed with a latissimus dorsi musculocutaneous-rotated flap (Fig. 2C) and a free split-thickness cutaneous flap. The postoperative course of the patient was uneventful. She was discharged on the 12th postoperative day. The histopathological examination of the specimen revealed invasive ductal carcinoma and oestrogen receptor (−), progesterone receptor (−) and HER2 (−). She was referred to the Medical Oncology and Radiation Oncology Clinics. She has been doing well for 3 months; however, she developed additional bone metastases.
Figure 2:
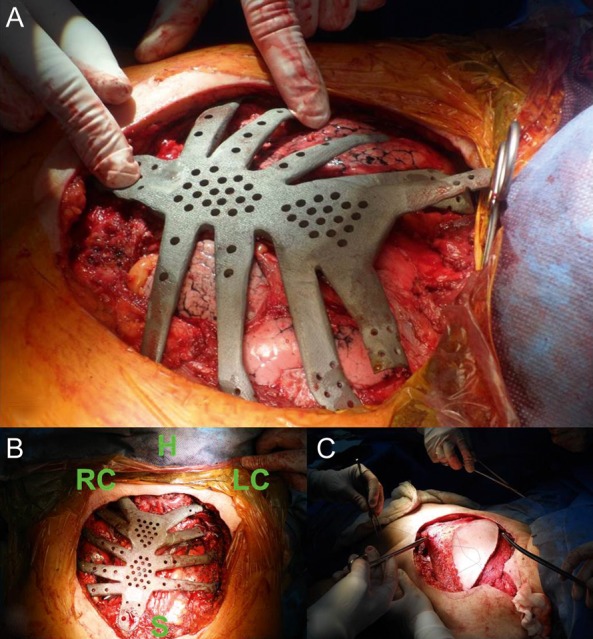
The patient specific titanium implant is compatible with the bony structures of the chest wall of patient. The angle between the clavicula and first rib can be seen clearly (A). The orientation view of the operative field. H: head of the patient, RC: right clavicula, LC: left clavicula, S: one-third distal part of the sternum ( B). The soft tissue coverage of titanium implant with latissimus dorsi musculocutaneous-rotated flap (C).
COMMENT
The most common complications after chest wall resection are respiratory in origin [1, 2]. Flail chest is the major leading factor for respiratory complication, and should be prevented. Bony skeletal reconstruction is the most important, but also most difficult, part of the chest wall resection and reconstruction surgery. However, an appropriate reconstruction remains the best way to avoid paradoxical motion of the chest wall. Weyant et al. [1] reported that there was no significant difference between large chest wall defects reconstructed with polypropylene mesh–methylmethacrylate composite and non-rigid reconstruction for small chest wall defects in terms of respiratory complications.
Methylmethacrylate sandwich graft is usually used for rigid reconstruction. However, this material has some disadvantages, including the inability to create a good chest wall concavity and non-permeability for fluid, which is the main cause of infection. Therefore, rigid reconstruction of the sternum with methylmethacrylate mesh should be limited after wide sternum resections because the major concern with using this material is the risk of infection [3].
Despite the aforementioned disadvantages, sternal resection without preservation of the manubrium requires an extensive and complex rigid stabilization that is usually achieved with methylmethacrylate [4]. However, the recent improvements in the reconstruction materials have an important impact on thoracic surgeons' choice of rigid reconstruction material for the sternum. Titanium plates, dual mesh [5] and the ‘rib-like’ technique [6] are prime examples of these new technologies. However, we thought that even these refinements are not sufficient for wide resections including bilateral clavicles, bilateral multiple ribs and sternum. In our case, we performed personalized reconstruction of extended chest wall defects with no complications. Our titanium ‘custom-made’ system was used successfully in a patient with a previous rib fracture.
Recently, the progression in 3D prototyping technology by selective laser sintering (SLS) technique has played an important role in producing complex, detailed and intricate models for both medical and dental applications. We used this technology in the thoracic surgery area, which minimized surgery failure and the duration of surgery, to the benefit of this patient.
This ‘en bloc’ custom-made implant provided quick, rigid, one-time reconstruction of the whole sternum, which is time-saving. Our inert titanium implant led to an excellent reconstruction.
CONCLUSION
From our experience, we conclude that this patient-specific titanium implant may be used safely and effectively. It is manufactured by one of the new technologies that can allow thoracic surgeons to perform a wide anterior chest wall resection including of the sternum. Despite the fact that the used titanium implant is novel and has not been used previously, the use of other types of titanium implants has been proved to be safe and effective [5, 6]. However, further studies are warranted in order to propose this method as a standard procedure.
Acknowledgements
This titanium material was designed and produced by Ali Osman Bengi, Kuntay Aktas, Murat Egri and Burcu Vardar at Gulhane Military Medical Academy, Medical Design and Production Center. The authors thank them for their significant contribution.
Conflict of interest: none declared.
REFERENCES
- 1.Weyant MJ, Bains MS, Venkatraman E, Downey RJ, Park BJ, Flores RM, et al. Results of chest wall resection and reconstruction with and without rigid prosthesis. Ann Thorac Surg. 2006;81:279–85. doi: 10.1016/j.athoracsur.2005.07.001. [DOI] [PubMed] [Google Scholar]
- 2.Mansour KA, Thourani VH, Losken A, Reeves JG, Miller JI, Jr, Carlson GW, et al. Chest wall resections and reconstruction: a 25-year experience. Ann Thorac Surg. 2002;73:1720–6. doi: 10.1016/s0003-4975(02)03527-0. [DOI] [PubMed] [Google Scholar]
- 3.Chapelier AR, Missana M, Couturaud B, Fadel E, Fabre D, Mussot S, et al. Sternal resection and reconstruction for primary malignant tumors. Ann Thorac Surg. 2004;77:1001–7. doi: 10.1016/j.athoracsur.2003.08.053. [DOI] [PubMed] [Google Scholar]
- 4.Rocco G. Chest wall resection and reconstruction according to the principles of biomimesis. Semin Thorac Surg. 2011;23:307–13. doi: 10.1053/j.semtcvs.2012.01.011. [DOI] [PubMed] [Google Scholar]
- 5.Berthet JP, Canaud L, D'Annoville T, Alric P, Marty-Ane C. Titanium plates and dualmesh: a modern combination for reconstructing very large chest wall defects. Ann Thorac Surg. 2011;91:1709–16. doi: 10.1016/j.athoracsur.2011.02.014. [DOI] [PubMed] [Google Scholar]
- 6.Girotti P, Leo F, Bravi F, Tavecchio L, Spano A, Cortinovis U, et al. The ‘rib-like’ technique for surgical treatment of sternal tumors: Lessons learned from 101consecutive cases. Ann Thorac Surg. 2011;92:1208–16. doi: 10.1016/j.athoracsur.2011.05.016. [DOI] [PubMed] [Google Scholar]