

Abstract
Background
During orthopedic operations, such as total hip replacement or total knee replacement, there is a lot of bone debris from bone cutting and reaming that commonly causes surgical suction devices to occlude many times, which can prolong the operative time and increase the amount of bleeding for the patient.
Materials and methods
We developed a surgical filter suction system that we call the VY suction tube. The suction tube assembly consists of a tube filter within a housing assembly. The filter pore size was designed to prevent tissue or bone debris from passing through the filter, though it allows fluid to pass through. A simulated total hip replacement operation was performed to test the efficacy of this new suction device when compared with two other types of tube suction devices.
Results
The VY suction tube showed that the mean duration to remove all fluid from a simulated field was significantly shorter than the Pool suction tube (P=0.0009) and Frazier suction tube (P=0.0012). The study also showed that the VY suction tube has a lower rate of occlusion when compared with the Pool suction tube (P≤0.0001) and Frazier suction tube (P≤0.0001).
Conclusion
Our new suction tube design shows good efficacy when removing fluid and debris from a simulated operative field. However, further studies in real clinical settings are needed.
Keywords: total hip replacement, filter suction, occlusion
Introduction
Surgical site infection is a devastating complication that commonly occurs postoperatively.1 A prolonged operative time is a risk factor of surgical site infection.2–8 One problem that surgeons face during an operation is occlusion of the surgical suction system due to tissue or bone debris, especially in orthopedic operations such as total hip replacement and total knee replacement. There is usually a lot of bone debris from bone cutting and reaming that frequently causes occlusion of the surgical suction equipment during an operation. In this study, we describe a filter suction system that was developed in our institute to solve the suction system occlusion problem. We also show the preliminary testing results of this filter suction.
Materials and methods
Design
The design concept was discussed between the physician and a design engineer before creating the three-dimensional models (Figure 1). The main concept was to decrease the occlusion rate of the suction system during operations. We developed a surgical filter suction tube that we call the VY suction tube. The suction assembly consists of a tube filter that is within the outer housing body, and that has inner and outer threads. The filter pore size is small enough to prevent tissue or bone debris from going through the filter pores, but there are a sufficient number of pores that allow blood and body fluids to pass through without plugging the tube filter. The inner filter can be removed from the outer housing to clean tissue or bone debris from the filter. At the end of the inner filter there is a handle that is designed to grasp and easily remove the filter (Figure 2).
Figure 1.
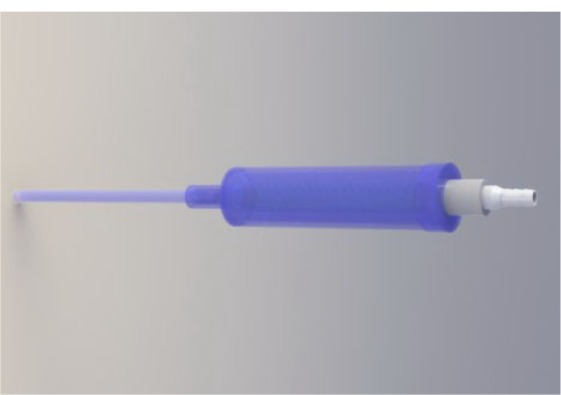
VY suction tube prototype three-dimensional model.
Figure 2.
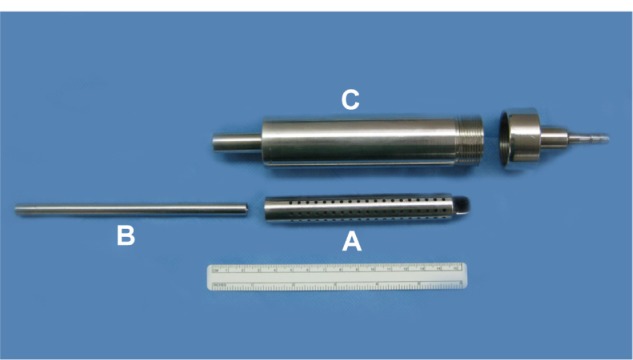
VY suction components.
Notes: (A), inner filter; (B), suction tip; (C), outer housing body.
Simulated operation suction testing
This study was approved by the Ethics Committee and Institutional Review Board of the Faculty of Medicine at Prince of Songkla University (Songkhla, Thailand). Suction efficacy was tested by suction of bone debris and fluid from a simulated acetabular reaming procedure in total hip replacement. The acetabulum was harvested from a porcine cadaver for the simulated operation (Figure 3). The acetabulum was reamed with an acetabular reamer (Quickset® Graters; DePuy, Warsaw, IN, USA) and a pneumatic hand piece (PowerPro® 6150; ConMed Corporation, Utica, NY, USA) that started from sizes of 41–43 mm. The bone debris was collected for the next testing step. Fifteen grams of bone debris were placed in a 100 mL stainless steel bowl and mixed with 10 mL of sterile water. Bleeding was simulated by adding sterile water into the bowl at a rate of 1 mL/second by infusion pumps (Terufusion®; Terumo Corporation, Tokyo, Japan) for a total of 90 mL (Figure 4).
Figure 3.

Porcine acetabulum and a reamer.
Note: Quickset® Graters; DePuy, Warsaw, IN, USA.
Figure 4.
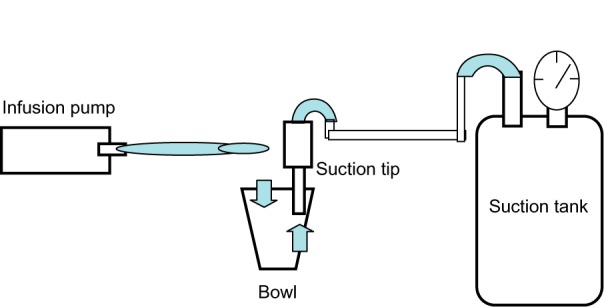
Suction testing system.
Notes: Suction pressure: 140 mmHg; infusion pump rate: 1 mL/second.
Five orthopedic surgeons tested and assessed the efficacy of the VY suction tube and compared it with the Pool suction tube (GF 862C; Aesculap, Tuttlingen, Germany) and the Frazier suction tube (GF 925C; Aesculap) (Figure 5). Each of the suction tips was connected to a silicone tube (6.35 × 1.6 mm) and a vacuum suction bottle and vacuum regulator (Ohmeda® Medical Surgical/Free-Flow Vacuum Regulator; Ohmeda Medical, Laurel, MD, USA). The suction pressure was set at 140 mmHg. All assessors used each suction tip two times separately to remove fluid in the simulated field. The suction tube’s efficacy was evaluated by the amount of time required to remove all fluid from the simulated field and the number of occlusions observed while the surgeons used the suction tubes from start to finish. The level of satisfaction for each suction device after testing was evaluated by a visual analog scale score.
Figure 5.
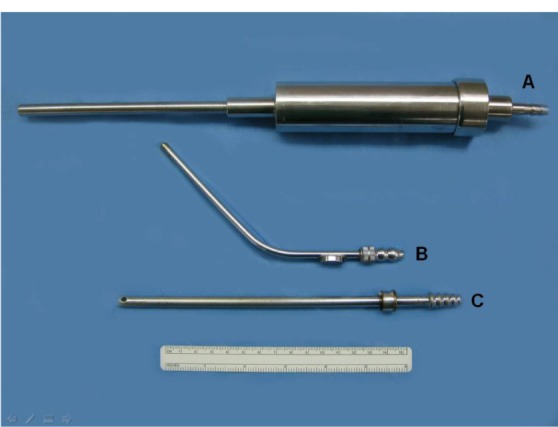
VY suction tube (A), Frazier suction tube (B), and Pool suction tube (C).
Statistical analysis
Statistical analysis was performed using R software (version 2.14.0; The Comprehensive R Archive Network, Institute for Statistics and Mathematics, Vienna, Austria). The continuous data were analyzed to detect differences using the Kruskal–Wallis rank sum test. The Wilcoxon rank sum test was used to analyze differences between groups.
Results
The suction test results from the five assessors (all assessors tested each type of suction twice) showed that the median amount of time required to remove all of the fluid from the simulated field with the VY suction tube was 92 seconds (range: 91–100 seconds; mean: 93 seconds; standard deviation [SD]: 2.63 seconds), which is significantly shorter than the amount of time required for the Pool suction tube (median: 119 seconds; range: 92–151 seconds; mean: 118.6 seconds; SD: 16.87 seconds; P=0.0009) and the Frazier suction tube (median: 117 seconds; range: 92–145 seconds; mean: 116.5 seconds; SD: 16.73 seconds; P=0.0012), but there was no difference between the Pool suction tube and the Frazier suction tube (P=0.85). The results of the test that evaluated and compared the occlusion rates between the VY, Pool, and Frazier suction tubes showed that the VY suction tube had a significantly lower rate of occlusion (median: 0; range: 0–1; mean: 0.1; SD: 0.32) when compared with the Pool suction tube (median: 6; range: 5–7; mean: 5.9; SD: 0.74; P≤0.0001) and the Frazier suction tube (median: 5; range: 3–10; mean: 5.1; SD: 2.03; P≤0.0001). There was no significant difference in the occlusion rate of the Pool suction tube when compared with the Frazier suction tube (P=0.06) (Table 1).
Table 1.
Time duration to remove all fluid from a simulated field and the number of occlusions (median) based on testing among five assessors (two times for each assessor)
| Suction tube types | VY suction | Pool suction | Frazier suction | P-value |
|---|---|---|---|---|
| Suction duration (seconds) | 92 (91–100) | 119 (92–151) | 117 (92–145) | <0.05 |
| Number of occlusions | 0 (0–1) | 6 (5–7) | 5 (3–10) | <0.05 |
The level of satisfaction associated with the use of each type of suction tip was evaluated by a Visual Analog Scale score, and the results showed a mean level of satisfaction score of 9.4 (SD: 0.55) for the VY suction tube. The satisfaction scores for the Pool and Frazier suction tubes were 6.6 (SD: 0.55) and 6.4 (SD: 1.14), respectively.
Discussion
Occlusion of suction while performing an operation is a common problem in orthopedic surgery, especially for total joint replacement surgery because there is a lot of bone debris in the operative field. Occlusion of the suction system causes inadequate suction capacity, which might increase the operative time due to poor operative field visualization – which may arise because of bleeding – and wasted time required to remove debris from the suction tube system. In addition, there is an increased amount of blood loss from the operation.
Prolonged surgical time is one factor that increases the risk of perioperative and postoperative complications. In a study by Peersman et al,9 the duration of the total knee replacement procedure is one of the risk factors associated with postoperative infection. Another conclusion was drawn by Kessler et al.10 In their study, the duration of the operation in revision total hip arthroplasty is a predictive parameter for perioperative morbidity.
Our VY suction tube showed that the occlusion rate and time to remove fluid in a simulated field is lower when compared to other suction tube systems. In this test, most of the assessors were satisfied with this new suction tube device. However, the simulated surgical field in this study had an exaggerated amount of bone debris when compared with an actual operation. The amount of bone removed through the suction devices might be more than in a real operation; therefore, conducting a study in a real operative field is necessary to prove the efficacy of this device.
One reason why our VY suction tube exhibited better performance and a higher satisfaction rate when compared with the other tubes could be that the tip diameter of our suction device is bigger than the others, but it is not so big as to obstruct the visual operative field. The other reason for this finding is that the filter in this suction device could trap bone debris inside the suction housing, so the bone debris does not travel through the suction tube and into the reservoir bottle where obstruction can also occur if some bone debris becomes deposited there. An additional benefit of this suction device is the fact that it is easy to clean because all parts are removable for resterilization. In this way, this device should work in a real operation because it has a low occlusion rate and it is easy to use and clean.
Conclusion
This suction prototype was designed for an operative field with a lot of bone debris. However, it may also be applied to an operative field with a lot of soft tissue debris. Therefore, further studies in a real clinical setting should be done.
Acknowledgment
We wish to thank Glenn Shingledecker for his assistance with the English proofreading of this report.
Author contributions
VY participated in the conception and design of the study, performed the data acquisition, participated in the statistical analysis, and drafted the manuscript. BT participated in the conception and design of the study, provided administrative support, carried out the critical revision of the manuscript, and supervised the study. TH and KI participated in the data acquisition and discussion of the results. All of the authors participated in drafting the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Namba RS, Inacio MC, Paxton EW. Risk factors associated with deep surgical site infections after primary total knee arthroplasty: an analysis of 56,216 knees. J Bone Joint Surg Am. 2013;95(9):775–782. doi: 10.2106/JBJS.L.00211. [DOI] [PubMed] [Google Scholar]
- 2.Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis MR, The Hospital Infection Control Practices Advisory Committee Guideline for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20(4):247–278. doi: 10.1086/501620. [DOI] [PubMed] [Google Scholar]
- 3.de Thomasson E, Guingand O, Terracher R, Mazel C. Perioperative complications after total hip revision surgery and their predictive factors. A series of 181 consecutive procedures. Rev Chir Orthop. Reparatrice Appar Mot. 2001;87(5):477–488. French. [PubMed] [Google Scholar]
- 4.Linam WM, Margolis PA, Staat MA, et al. Risk factors associated with surgical site infection after pediatric posterior spinal fusion procedure. Infect Control Hosp Epidemiol. 2009;30(2):109–116. doi: 10.1086/593952. [DOI] [PubMed] [Google Scholar]
- 5.Haridas M, Malangoni MA. Predictive factors for surgical site infection in general surgery. Surgery. 2008;144(4):496–501. doi: 10.1016/j.surg.2008.06.001. discussion 501–503. [DOI] [PubMed] [Google Scholar]
- 6.Culver DH, Horan TC, Gaynes RP, et al. Surgical wound infection rates by wound class, operative procedure, and patient risk index. National Nosocomial Infections Surveillance System. Am J Med. 1991;91(3B):152S–157S. doi: 10.1016/0002-9343(91)90361-z. [DOI] [PubMed] [Google Scholar]
- 7.Leong G, Wilson J, Charlett A. Duration of operation as a risk factor for surgical site infection: comparison of English and US data. J Hosp Infect. 2006;63(3):255–262. doi: 10.1016/j.jhin.2006.02.007. [DOI] [PubMed] [Google Scholar]
- 8.Peersman G, Laskin R, Davis J, Peterson MG, Richart T. Prolonged operative time correlates with increased infection rate after total knee arthroplasty. HSS J. 2006;2(1):70–72. doi: 10.1007/s11420-005-0130-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Peersman G, Laskin R, Davis J, Peterson M. Infection in total knee replacement: a retrospective review of 6489 total knee replacements. Clin Orthop Relat Res. 2001;(392):15–23. [PubMed] [Google Scholar]
- 10.Kessler S, Kinkel S, Käfer W, Puhl W, Schochat T. Influence of operation duration on perioperative morbidity in revision total hip arthroplasty. Acta Orthop Belg. 2003;69(4):328–333. [PubMed] [Google Scholar]