

Abstract
Objective:
To ascertain the current status of global health training and humanitarian relief opportunities in US and Canadian postgraduate neurology programs.
Background:
There is a growing interest among North American trainees to pursue medical electives in low- and middle-income countries. Such training opportunities provide many educational and humanitarian benefits but also pose several challenges related to organization, human resources, funding, and trainee and patient safety. The current support and engagement of neurology postgraduate training programs for trainees to pursue international rotations is unknown.
Methods:
A survey was distributed to all program directors in the United States and Canada (December 2012–February 2013) through the American Academy of Neurology to assess the training opportunities, institutional partnerships, and support available for international neurology electives.
Results:
Approximately half of responding programs (53%) allow residents to pursue global health–related electives, and 11% reported that at least 1 trainee participated in humanitarian relief during training (survey response rate 61%, 143/234 program directors). Canadian programs were more likely to allow residents to pursue international electives than US programs (10/11, 91% vs 65/129, 50%, p = 0.023). The number of trainees participating in international electives was low: 0%–9% of residents (55% of programs) and 10%–19% of residents (21% of programs). Lack of funding was the most commonly cited reason for residents not participating in global health electives. If funding was available, 93% of program directors stated there would be time for residents to participate. Most program directors (75%) were interested in further information on global health electives.
Conclusions:
In spite of high perceived interest, only half of US neurology training programs include international electives, mostly due to a reported lack of funding. By contrast, the majority of Canadian programs that responded allow international electives, likely due to clearer guidelines from the Royal College of Physicians and Surgeons of Canada compared to the Accreditation Council of Graduate Medical Education. However, the number of both Canadian and US neurology trainees venturing abroad remains a minority. Most program directors are interested in learning more information related to global health electives for neurology residents.
International health exchange programs have existed for several decades at various levels of medical training,1 but the interest to pursue overseas electives has dramatically increased in multiple medical specialties in the United States in recent years.2 International opportunities may be a major motivating reason for students to choose medicine as a career and pursue certain specialties or subspecialties. In 2010, 31% of graduating medical students reported participating in an international health elective and 43% of all students stated that their global health experiences in medical training were “inadequate.”3
Each year, an estimated 6,200 physicians graduate from more than 900 neurology training programs worldwide,4 making the potential workforce for global neurology exchanges high. Although international rotations are anecdotally popular among neurology trainees, most international experiences are without guidelines, curricular goals, formal structure, or preparation to ensure trainee and patient safety.5,6 Trainees who venture abroad may provide a range of benefits to the global health workforce. These include provision of humanitarian aid, a better-educated network of physicians that can prevent the international spread of disease, a wider understanding of the global burden of disease (particularly infectious diseases), enhanced institutional reputation, and a better understanding of cost-effectiveness and test selection.7 However, such experiences are not without risk and cost and may be a potential burden to human resources for teaching in low- and middle-income countries (LMIC). Given the increasing global mobility of neurologic trainees and the current range of opinions on international health electives in LMIC, we sought to assess the extent to which neurology trainees participate in international neurology rotations during residency.
METHODS
Standard protocol approvals, registrations, and patient consents.
This study was approved by the Johns Hopkins University Bloomberg School of Public Health Institutional Review Board.
Survey instrument.
The survey instrument was a 13-point questionnaire devised by the authors based on previously reported surveys8,9 assessing the status of international electives in various disciplines. Questions were in the form of multiple choice, yes/no, and fill-in-the-blank questions; some items were accompanied by free text comments or explanations (appendix e-1 on the Neurology® Web site at www.neurology.org). The survey was approved, with minor additions, by the American Academy of Neurology (AAN) Graduate Education Subcommittee and Member Research Subcommittee. The survey was made available via postal mail, fax, and an online link received via e-mail. Respondents were also given the opportunity to provide free text responses at the end of the survey with additional comments or concerns.
Survey distribution.
The AAN distributed the survey to each of the 234 neurology residency program directors in the United States and Canada on December 11, 2012. All surveys were in English only. In order to maximize access to program directors, respondents were not required to be members of the AAN. Participation was voluntary and confidential. Nonrespondents were sent a reminder e-mail on December 18, 2012, with a link to the online survey. Three additional reminders were sent to nonrespondents via postal mail or fax and e-mail approximately every 2 weeks until study completion on February 22, 2013.
RESULTS
Characteristics of survey respondents and nonrespondents.
A total of 143 of 234 possible program directors completed the survey, yielding a response rate of 61%. Response rate did not differ between Canada (12/26, 46%) and the United States (131/208, 63%) (p > 0.05). Geographically, 24% of responses came from the Northeast and Midwestern United States each, 29% from the South, and 15% from the West. An additional 8% of responses were from Canada. There were no significant differences in mean age or sex between survey respondents and nonrespondents (p > 0.05). The median number of residents per year at programs who responded was 3–4, ranging from 0 to 19 residents. The majority of respondents (75%) expressed interest in receiving further information on global health initiatives.
Survey results.
Just over half of programs (75/141, 53%) allow global health electives (table 1). The top reason for not allowing such rotations was lack of funding (figure 1A). Nearly all program directors (70/75, 93%) reported that their residents would have the academic time to participate in international electives if funding were not an issue. Among programs that do not allow global health electives (n = 65), 86% cited lack of funding, 55% stated there were no formal programs or partnerships with international sites, 40% cited no provisions for offsite electives in their program, and 31% perceived no interest by residents. Other impediments included hospital restriction of offsite electives, no overseas malpractice coverage, and loss of graduate medical education (GME) payments.
Table 1.
US and Canadian neurology training program allowance of and support information for international electives during residency
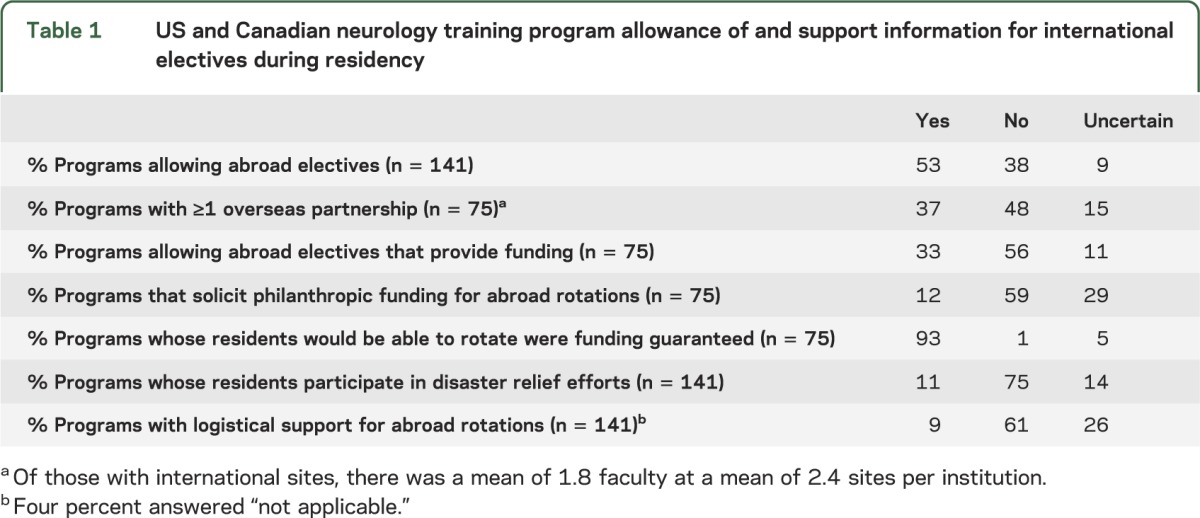
Figure 1. Reasons provided by survey respondents for nonparticipation in international electives among US and Canadian neurology residency trainees.

(A) Lack of funding was the principal reason selected for barring such experiences. (B) Percentage of residents who complete international rotations from programs shows more than half of programs have fewer than 10% of their residents rotate abroad.
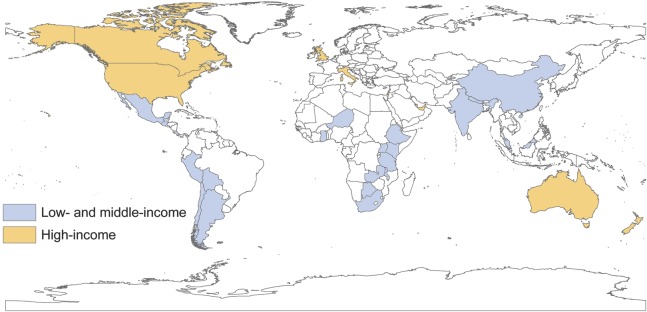
Table 2 lists selected representative comments relating to coverage for, funding of, and interest in international electives. Of the programs allowing global health rotations, the majority of program directors responded that fewer than 10% of program residents participate in such rotations prior to graduation (figure 1B). Destinations of global health electives in neurology are predominantly in South America and sub-Saharan Africa. Respondents also volunteered information regarding international electives to countries outside of the survey instrument's definition of “international” sites. These are depicted in figure 2.
Table 2.
Selected comments by program directors regarding global health in residency programs
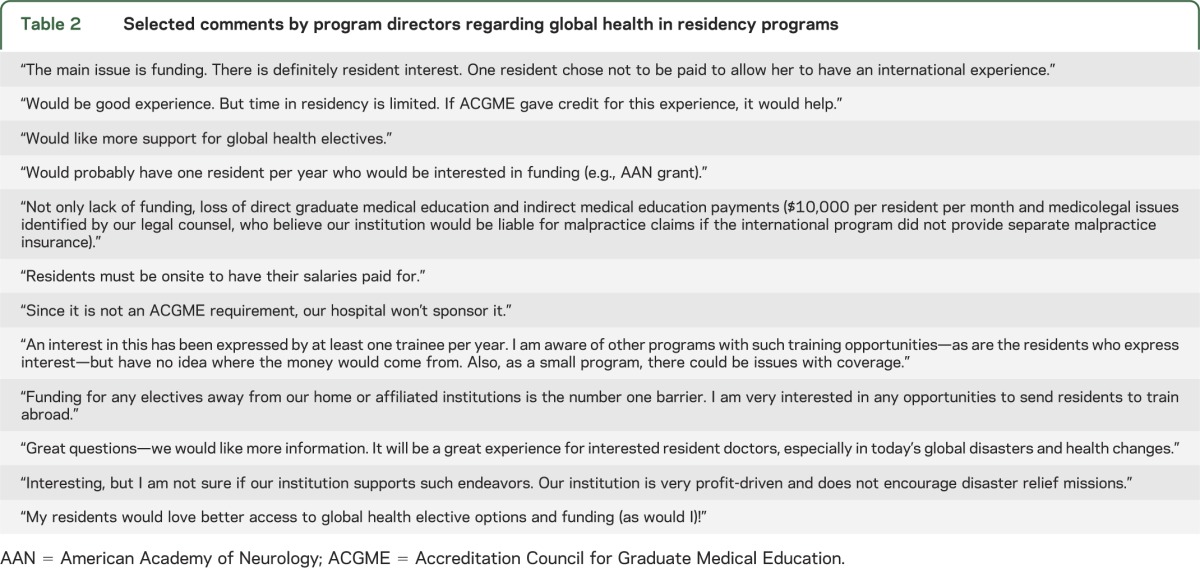
Figure 2. World map of international destinations for neurology trainees on elective as reported by neurology program directors.
Of the programs that allow for international electives, most (42/75, 56%) have no financial support available to participants. One-third of programs offer financial support (25/75, 33%) and some program directors were uncertain (8/75, 11%). Where funding is available, funding is derived mostly through formal university, hospital, or departmental programs. Philanthropic donations for funding international electives are rarely available, and only 12% (9/75) of programs solicit such donations.
The vast majority of respondents shared that their residents have not participated in humanitarian relief efforts or such participation is unknown (125/141, 89%). Among those who participated, most did so without formal institutional support. Very few residencies have support programs for predeparture training, psychosocial support, postexposure prophylactic medications, or debriefing for trainees who are involved in humanitarian aid activities (table 1). Those who have support available accessed it through global health offices on campus (n = 3), existing hospital-based programs (n = 2), residency program (n = 1), military resources (n = 1), attending physician on site (n = 1), or reported that there was support only for faculty and not residents (n = 1).
Canadian program directors were more likely to report that their programs allowed global health-related electives for residents (10/11, 91%) compared to US program directors (65/129, 50%) (p = 0.023), although there were relatively fewer Canadian programs in this survey. Lack of funding was the main reason for residents not participating in both Canada and the United States. No Canadian program director reported that more than 30% of residents participated in international electives, while 16% of US programs reported more than 30% of residents had already participated. Both Canadian (8/10) and US (62/65) respondents believed that residents would have time to participate in global health electives if funding was not an issue. Approximately 40% of both countries' respondents reported an office of global health at their institution, whether or not it was engaged for neurology rotations abroad (5/12, 42% programs in Canada vs 54/125, 43% in the United States). Interest in learning more about global health electives was high in both countries: 10/12, 83% of programs in Canada and 95/129, 74% of programs in the United States.
DISCUSSION
There is no consensus on the structure of international opportunities for neurology trainees in United States and Canadian residency programs. Some neurology training programs have well-established, long-term relationships with sites in low-income settings, whereas other programs do not allow residents to go off-site during the course of their entire postgraduate neurology training. In other cases, residents and fellows are permitted to make single visits to locations of their choice to explore neurologic practice, and occasionally neurologic research, in LMIC.10–17
Currently, most neurology trainees in the United States and Canada do not participate in international rotations in LMIC prior to program graduation, with the most significant barrier being limited to no funding for such initiatives. In addition to lack of financial support, several respondents noted loss of GME funds for off-site trainees as a barrier to such activities. However, the current lack of opportunities for neurology residents does not equate to a lack of interest in international electives. Our results disclosed perceived interest in rotations abroad and in obtaining further information on global health electives by 75% of program directors. A logical next step is to formally assess neurology residents' interest and availability for international electives. In other studies, the opportunity to treat patients of low socioeconomic status abroad was predictive of long-term participation in the medical care of disadvantaged populations domestically.18–20
Many residency programs in other specialties incorporate global health into GME, and this has translated into improved provider knowledge.19,21 Approaches to global health education in residency vary, ranging from independently motivated/funded connections with a remote site9,22 to institutionalized global health electives.9,23,24 Some residencies have developed, or are working toward, formal global health tracks.25–27 In neurology, the majority of trainees who engage in international electives visit via established institutional connections. It is difficult to assess the benefit of independent arrangements compared to institutionalized support.
Centralized support or program information through professional organizations such as the AAN could improve availability of global health exchanges.28 Other opportunities may include a registry of neurologists in LMIC sites who are willing to host neurology trainees in partnership with high-income sites that are in turn willing to provide similar opportunities for trainees from LMIC. The AAN in particular could be instrumental in developing online training modules for predeparture training of residents and fellows, establishing guidelines for safety and field training (e.g., postexposure prophylaxis in the setting of bloodborne pathogens), and recommendations to program directors for access of trainees to postelective debriefing and counseling as necessary. Working groups of the AAN could also help establish core competencies for international work in global health. This may include “global health competencies” as promoted by the American Society for Tropical Medicine and Hygiene Committee on Medical Education: 1) a basic understanding of burden of global diseases, 2) traveler's medicine, and 3) immigrant health.29 To these competencies, neurology-specific priorities such as treatment gaps, a more thorough understanding of vaccine-preventable and infectious neurologic disorders, cost-effectiveness, and neurologic diagnosis in low-resourced settings could be considered as important additions.
The Accreditation Council for Graduate Medical Education (ACGME), the organization responsible for “the accreditation of post-MD medical training programs within the United States,” has no official position on international electives during neurology training and has remained silent on this issue. While there is no official prohibition or disallowance of international training, there is also no statement of acceptance or how to facilitate such an opportunity. International electives thus remain at the discretion of the individual program or institution and can also be entertained at the ACGME on a case-by-case basis (personal communication, ACGME, August 8, 2013). The question of international electives does not appear on the frequently asked questions of the Neurology Review Committee for Neurology30 Web site because the question is not frequently asked (personal communication, ACGME, August 8, 2013). By contrast, there is an “international rotation application process review committee for neurologic surgery” at the ACGME that states that rotations overseas may be electives only, must be approved before departure, and no operative cases can be used in the ACGME Case Log System.31 By contrast, the Royal College of Physicians and Surgeons of Canada (RCPSC) has an updated policy that includes “electives taken in an unaccredited setting” (4.6.1, Policies and Procedures for Certification and Fellowship) that guides all specialty training in Canada.32 According to the RCPSC, in order to pursue an international elective at an unaccredited site, 1) the resident must be enrolled in a recognized program, 2) the elective must be less than 6 months in duration, 3) planning must occur between the resident and program director and approved by the program director, 4) there is a clearly defined elective supervisor, 5) there are clearly defined and understood educational objectives, and 6) there is a well-defined in-training evaluation system to include evaluation of the resident.32
Since the need for medical professionals during disaster relief efforts (in the United States or abroad) may present a unique opportunity for neurology trainees to engage in humanitarian efforts during residency, we also polled program directors on participation in such endeavors. Very few neurology trainees (approximately 10%) are reported to have participated in humanitarian relief efforts either domestically or abroad. Among those who participated, few had access to logistical or psychosocial support programs for management of illness or stresses borne out by such undertakings. This raises concern for the physical and emotional well-being of neurology residents who participate in challenging international opportunities. Increasing the support and access to care for trainees who choose to participate should be systematically strengthened.
This study has several limitations. First, the response rate was relatively low (61%) and may limit generalizability to all programs in the United States and Canada. It is possible that survey response bias occurred; programs that value international neurology electives or nontraditional educational opportunities may have been more likely to respond to this survey. If so, the results here would over-represent the interest and opportunities in the current climate for international health rotations. The differences between Canadian and US programs also deserve further exploration. Canadian residency training for adult neurology includes an additional year compared to US training, which may facilitate more offsite elective time. There are fewer residents per training year in most Canadian neurology residency programs compared to US programs. The guidelines for residents who wish to pursue elective time may be more stringent for Canadian trainees but are likely more clear for all those involved. Since there are relatively few Canadian training programs for neurology overall, statistical analyses comparing the countries may not convey important differences in the attitudes and acceptance of global health electives.
Also, not all trainee involvement in international electives and humanitarian relief efforts may be known to program directors responding to the survey. Since electives may be ad hoc and programs may have several residents offsite domestically, the range of electives being undertaken is likely under-reported. It is possible that program directors are unaware of the risks experienced by residents and are therefore unable to help mitigate potential problems. The high number of “uncertain” replies by program directors in this survey suggests that program directors may not all be fully aware of the opportunities, challenges, or scope of international involvement of their residents. Therefore, the exact number of residents traveling abroad may be impossible to estimate without a survey of residents themselves.
In spite of these limitations, our results provide a first assessment of the current depth and breadth of global health involvement by neurology trainees in US and Canadian residency programs. They suggest opportunities for core competency development, curricular approaches, decision-making, and best practices in the approach to international training opportunities for neurology electives. This may help meet what appears to be a growing demand and enthusiasm for international experiences by neurology residents, fellows, and faculty.
Supplementary Material
ACKNOWLEDGMENT
The authors thank Laura Lamberti, MHS, PhD candidate, Department of International Health, Bloomberg School of Public Health, the Johns Hopkins University, for assistance with creating figure 2.
GLOSSARY
- AAN
American Academy of Neurology
- ACGME
Accreditation Council for Graduate Medical Education
- GME
graduate medical education
- LMIC
low- and middle-income countries
- RCPSC
Royal College of Physicians and Surgeons of Canada
Footnotes
Editorial, page 100
Supplemental data at www.neurology.org
AUTHOR CONTRIBUTIONS
J.L.L. assisted in creating the survey instrument, analyzed and interpreted the results, wrote and edited the manuscript. M.C. assisted in creating the survey instrument, acquisition and interpretation of data, and editing the final manuscript. J.E. assisted in data interpretation and manuscript editing. F.J.M. designed the study, drafted the survey instrument, analyzed results, and contributed to writing and editing the manuscript.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
The authors report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Bissonette R, Route C. The educational effect of clinical rotations in nonindustrialized countries. Fam Med 1994;26:226–231 [PubMed] [Google Scholar]
- 2.Martiniuk AL, Manouchehrian M, Negin JA, Zwi AB. Brain Gains: a literature review of medical missions to low and middle-income countries. BMC Health Serv Res 2012;12:134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Global Health Learning Opportunities (GLHO) [online] Available at: www.aamc.org/services/glho. Accessed April 30, 2013.
- 4.Bergen DC, Good D. Neurology training programs worldwide: a world federation of neurology survey. J Neurol Sci 2006;246:59–64 [DOI] [PubMed] [Google Scholar]
- 5.Crump JA, Sugarman J. Ethics and best practice guidelines for training experiences in global health. Am J Trop Med Hyg 2010;83:1178–1182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sharafeldin E, Soonawala D, Vandenbroucke JP, Hack E, Visser LG. Health risks encountered by Dutch medical students during an elective in the tropics and the quality and comprehensiveness of pre-and post-travel care. BMC Med Educ 2010;10:89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kanter SL. International collaborations between medical schools: what are the benefits and risks? Acad Med 2010;85:1547–1548 [DOI] [PubMed] [Google Scholar]
- 8.Birnberg JM, Lypson M, Anderson RA, et al. Incoming resident interest in global health: occasional travel versus a future career abroad? J Grad Med Educ 2011;3:400–403 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Volsky PG, Sinacori JT. Global health initiatives of US otolaryngology residency programs: 2011 global health initiatives survey results. Laryngoscope 2012;122:2422–2427 [DOI] [PubMed] [Google Scholar]
- 10.Ambrose JB, Babu D. A neurology resident's reflections on an elective in Hyderabad. Ann Neurol 2011;69:1055–1059 [DOI] [PubMed] [Google Scholar]
- 11.Dahodwala N. Neurology education and global health: my rotation in Botswana. Neurology 2007;68:E15–E16 [DOI] [PubMed] [Google Scholar]
- 12.Laccheo I, Espinosa PS. International issues: neurology mission in the Ecuadorian Amazon rainforest. Neurology 2012;78:e60–62 [DOI] [PubMed] [Google Scholar]
- 13.Mateen FJ. International issues: neurology in Bangladesh. Neurology 2010;74:e5–e8 [DOI] [PubMed] [Google Scholar]
- 14.Porter A. International education issues: a perspective on the practice of neurology in northern Kenya. Neurology 2007;69:1719–1720 [DOI] [PubMed] [Google Scholar]
- 15.Sheikh SI. International issues: of saints and sickness: a neurology elective in India. Neurology 2009;72:e24–e26 [DOI] [PubMed] [Google Scholar]
- 16.Sheikh SI. International issues: tropical neurology in Vietnam. Neurology 2011;76:e102–e104 [DOI] [PubMed] [Google Scholar]
- 17.Siddiqi OK, Atadzhanov M. Neurological letter from Zambia. Pract Neurol 2013;13:281–285 [DOI] [PubMed] [Google Scholar]
- 18.Ramsey AH, Haq C, Gjerde CL, Rothenberg D. Career influence of an international health experience during medical school. Fam Med 2004;36:412–416 [PubMed] [Google Scholar]
- 19.Thompson MJ, Huntington MK, Hunt DD, Pinsky LE, Brodie JJ. Educational effects of international health electives on U.S. and Canadian medical students and residents: a literature review. Acad Med 2003;78:342–347 [DOI] [PubMed] [Google Scholar]
- 20.Drain PK, Holmes KK, Skeff KM, Hall TL, Gardner P. Global health training and international clinical rotations during residency: current status, needs, and opportunities. Acad Med 2009;84:320–325 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bjorklund AB, Cook BA, Hendel-Paterson BR, Walker PF, Stauffer WM, Boulware DR. Impact of global health residency training on medical knowledge of immigrant health. Am J Trop Med Hyg 2011;85:405–408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sekhar A, Eisenberg RL, Yablon CM. Enhancing the resident experience with global health electives. AJR Am J Roentgenol 2012;198:W118–W121 [DOI] [PubMed] [Google Scholar]
- 23.Leow JJ, Kingham TP, Casey KM, Kushner AL. Global surgery: thoughts on an emerging surgical subspecialty for students and residents. J Surg Educ 2010;67:143–148 [DOI] [PubMed] [Google Scholar]
- 24.Nelson BD, Lee AC, Newby PK, Chamberlin MR, Huang CC. Global health training in pediatric residency programs. Pediatrics 2008;122:28–33 [DOI] [PubMed] [Google Scholar]
- 25.Bazemore AW, Goldenhar LM, Lindsell CJ, Diller PM, Huntington MK. An international health track is associated with care for underserved US populations in subsequent clinical practice. J Grad Med Educ 2011;3:130–137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gladding S, Zink T, Howard C, Campagna A, Slusher T, John C. International electives at the university of Minnesota global pediatric residency program: opportunities for education in all Accreditation Council for Graduate Medical Education competencies. Acad Pediatr 2012;12:245–250 [DOI] [PubMed] [Google Scholar]
- 27.Calland JF, Petroze RT, Abelson J, Kraus E. Engaging academic surgery in global health: challenges and opportunities in the development of an academic track in global surgery. Surgery 2013;153:316–320 [DOI] [PubMed] [Google Scholar]
- 28.Siddiqi OK, Koralnik IJ, Atadzhanov M, Birbeck GL. Emerging subspecialties in neurology: global health. Neurology 2013;80:e78–80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Houpt ER, Pearson RD, Hall TL. Three domains of competency in global health education: recommendations for all medical students. Acad Med 2007;82:222–225 [DOI] [PubMed] [Google Scholar]
- 30.Review committee for neurology ACGME Frequently asked questions: Neurology. Available at: http://www.acgme.org/acgmeweb/Portals/0/PDFs/FAQ/180_Neurology_FAQs.pdf Last. Accessed August 12, 2013
- 31.International rotation application process review committee for neurological surgery. Accreditation Council for Graduate Medical Education (ACGME) Available at: http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramResources/160_International_Rotation_Application_Process.pdf Last. Accessed August 12, 2013.
- 32.Royal College of Physicians and Surgeons of Canada Policies and procedures for certification and fellowship. 2013. Available at: http://www.royalcollege.ca/portal/page/portal/rc/common/documents/credentials/policy_procedures_e.pdf Last. Accessed August 12, 2013
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.