

This summer marked the 10th anniversary of the creation of the President’s Emergency Plan for AIDS Relief (PEPFAR), widely considered the most ambitious and successful global public health program since smallpox eradication. Over the past decade, PEPFAR has funded HIV–AIDS treatment for more than 5 million people in resource-limited settings in sub-Saharan Africa. Now, the U.S. government has reached a turning point in its emergency response and has decided to reduce funding to many of these countries, including South Africa, recipient of the most PEPFAR dollars. In August 2012, the U.S. government announced it would cut South Africa’s PEPFAR budget in half by 2017, making South Africa the first PEPFAR-funded country to transition to full ownership of — and financial responsibility for — its HIV program. Many observers laud the move as a step toward South African independence from global donors, but others warn that it may jeopardize the health of 1.7 million South Africans who are being treated for HIV–AIDS.
South Africa receives more than $500 million annually from PEPFAR but is also the only PEPFAR-funded country that has underwritten most of its own HIV budget for the past 5 years. As the government transitions to independence, it has begun closing many of the specialized HIV-treatment centers created by PEPFAR, moving patients into government-run, community-based health care centers, where long waiting times and medication shortages are common. Some observers worry that this shift will threaten the tremendous gains PEPFAR has brought. “We are working closely with the government of South Africa to decide how we can successfully shift many of the services that PEPFAR provided and decide what is essential for HIV care,” said the U.S. Global AIDS Coordinator, Ambassador Eric Goosby. “The tension is determining how to continue to provide state-of-the art treatment and care at affordable prices.”
When PEPFAR was started in 2003, President George W. Bush declared that the United States would provide $15 billion of “emergency funding” over 5 years to fight HIV in the 15 countries with the greatest global burden of disease. At the time, 34 million people worldwide were living with HIV, 20 million of them in sub-Saharan Africa, where highly active antiretroviral therapy was largely unavailable. Although some people bristled at the unilateral action that reflected the Bush administration’s approach to foreign policy, PEPFAR was welcomed by South African researchers and activists who had been fighting to get life-saving treatment to HIV-infected patients. As a very large international health initiative that was founded to combat a single disease, PEPFAR stands out because of its commitment to providing lifelong treatment for millions of people who would have died without it. (See bar graph for anti-retroviral coverage rates in 2010.)
When PEPFAR was founded, the idea of South African government-sponsored HIV care was unimaginable. South Africa’s HIV epidemic was exploding, and 20% of adults were infected. But President Thabo Mbeki and Minister of Health Manto Tshabalala-Msimang refused to believe that HIV caused AIDS and refused to work with PEPFAR. A later study estimated that more than 3.8 million person-years were lost because of the Mbeki administration’s obstruction of the provision of lifesaving treatment.1 The international community watched in horror as the epidemic raged in city after city, township after township throughout South Africa. “We projected what the worst-case scenario could look like if nothing was done, and then it came true,” said Mitchell Warren, executive director of the AIDS Vaccine Advocacy Coalition.
In this environment, HIV researchers and advocates were called on to provide treatment outside the existing government-run system of public health centers. “PEPFAR arrived in a big way, building HIV prevention, treatment, and care services,” said Goosby. “That support has helped give more than 1.7 million people access to state-of-the art care and treatment.” Indeed, HIV researchers and advocates in South Africa transformed their agendas overnight, adding treatment programs to their portfolio of work. “We were given a week to ramp up services and get our pharmacies ready to go,” said Francois Venter, deputy executive director of the Wits Reproductive Health and HIV Institute. “At the time, we had 500 patients on treatment, but within a decade we brought 40,000 more into care, literally pulling these people back from the edge.”
By 2012, the U.S. government had provided more than $44 billion in aid under PEPFAR and the Global Fund to Fight AIDS, Tuberculosis, and Malaria. The first 5 years of funding led to a 10.5% reduction in HIV-related mortality and an increase in overall life expectancy in the 15 countries supported by the initiative.2,3 As the United States faced its own economic recession, however, some observers questioned the program’s sustainability. “There is increasing pressure to transition away from an emergency response towards an integration of services and capacity building within countries,” noted Robert Black, professor of international health at Johns Hopkins Bloomberg School of Public Health and chair of the Institute of Medicine committee that conducted an evaluation of PEPFAR. “What this means at the individual level is transitioning away from ‘vertical programs’ which specialize in HIV care exclusively and entering community-based health centers which provide a range of care.”
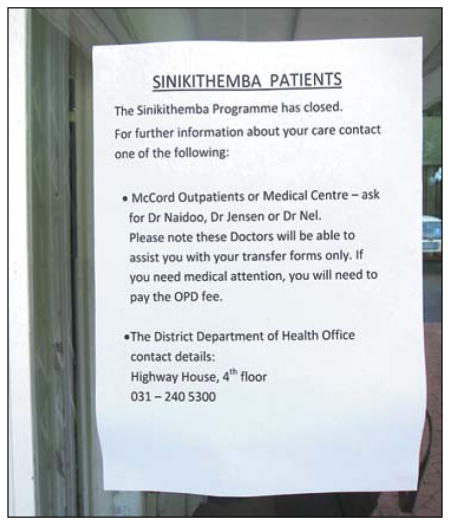
On the ground, this transition means that each PEPFAR-funded site has had to determine how to safely transfer patients to multiple local clinics. Many have made the transition without further funding for assessing whether patients seek follow-up care. At present, only a few studies are being performed independently to monitor the effects of “down-referral.” One such study at Mc-Cord Hospital in Durban, South Africa, tracked 4000 patients assigned to community health centers after budget cuts closed the treatment center. Preliminary results showed that 70 to 90% of these patients successfully transitioned to a new clinic, offering some evidence that patients are managing to navigate the early stages of the transition.4
One caveat, however, is that these findings address only the first visit to a transfer clinic, not rates of retention in care, adherence to medication, or ongoing virologic suppression — the outcome measures needed to fully evaluate the effects of the transfer process. Many patients have expressed fear of being recognized by family or friends at local clinics; some have sought care at private clinics to ensure confidentiality and avoid being stigmatized. Others express frustration about the lack of access to physicians at local community clinics, less-attentive care, and lost time; long lines often make obtaining medication a day-long procedure. Senior officials acknowledge that medication stock-outs at government-run clinics are common, which may threaten medication adherence. Beyond concerns about long-term retention in care, some wonder whether the transition will deter new patients from starting treatment, since prior research suggests that treatment refusal may be common even when PEPFAR-funded clinics exist.5
As PEPFAR changes course, two central questions remain: How can the South African government provide comparable care with fewer resources? And what is the United States’ responsibility for the nearly 2 million South African patients currently receiving treatment? As South Africa transitions away from PEPFAR’s model of HIV care, dedicated resources will be required to assess rates of treatment initiation, retention, medication adherence, and virologic suppression. Ideally, the transition would involve efforts to strengthen the health system that are measurable and the introduction of a centrally monitored reporting system to provide data on all patients receiving care. In addition, support is necessary to retain health care workers trained in PEPFAR programs so that they can provide supervision and mentorship, since community-based clinicians often have limited training in HIV care. PEPFAR should continue to collaborate with the South African government to fund research evaluating innovative methods for retaining patients in care.
Ultimately, PEPFAR’s legacy will rest on what happens at this juncture. “There are real patients whose lives are literally hanging in the balance right now,” argues Charles Holmes, former chief medical officer of the Office of the U.S. Global AIDS Coordinator. “It is extraordinarily important that we get this right.”
Antiretroviral Therapy Coverage in Sub-Saharan African Countries, 2010.

Coverage estimates are based on 2010 World Health Organization guidelines. No data for Ethiopia are available from this source. In Malawi, estimated coverage was reported as a range of 49 to 57%. DRC denotes Democratic Republic of Congo. Data are from WHO/UNAIDS/UNICEF Global HIV Response 2011.
Footnotes
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
References
- 1.Chigwedere P, Seage GR, III, Gruskin S, Lee TH, Essex M. Estimating the lost benefits of antiretroviral drug use in South Africa. J Acquir Immune Defic Syndr. 2008;49:410–5. doi: 10.1097/qai.0b013e31818a6cd5. [DOI] [PubMed] [Google Scholar]
- 2.Bendavid E, Holmes CB, Bhattacharya J, Miller G. HIV development assistance and adult mortality in Africa. JAMA. 2012;307:2060–7. doi: 10.1001/jama.2012.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bor J, Herbst AJ, Newell ML, Bärnighausen T. Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treatment. Science. 2013;339:961–5. doi: 10.1126/science.1230413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bassett Large scale, rapid transfer of HIV-infected patients from hospital-based to primary health clinics in South Africa: an assessment of self-reported linkage to care. Presented at the 8th International Conference on HIV Treatment and Prevention Adherence; Miami. June 2–4, 2013. [Google Scholar]
- 5.Katz IT, Essien T, Marinda ET, et al. Anti-retroviral therapy refusal among newly diagnosed HIV-infected adults. AIDS. 2011;25:2177–81. doi: 10.1097/QAD.0b013e32834b6464. [DOI] [PMC free article] [PubMed] [Google Scholar]