

Abstract
Purpose
In recent years, laser surgery has been widely used to treat benign prostatic hyperplasia (BPH). A thulium:yttrium-aluminium-garnet (Tm:YAG) laser was recently introduced for BPH surgery. We compared the effectiveness and safety of Tm:YAG laser vaporesection of the prostate (ThuVaRP) with that of bipolar transurethral resection of the prostate (TURP).
Materials and Methods
From January 2010 to December 2012, 86 patients underwent surgical treatment for symptomatic BPH by a single surgeon. We retrospectively analyzed and compared the medical records of 43 patients who underwent ThuVaRP and 43 patients who underwent bipolar TURP. All patients were assessed by using the International Prostate Symptom Score, transrectal ultrasonography, the serum prostate-specific antigen (PSA) level, uroflowmetry, and postvoid residual volume before and 1 month after surgery. All complications were compared between the two groups.
Results
ThuVaRP was superior to TURP in catheterization time (p<0.001) and length of hospital stay (p<0.001). However, operation time was longer with ThuVaRP than with TURP (p<0.001). In patients with a large prostate (>50 g), operation time was much longer with ThuVaRP. One month after surgery, the decrease in PSA was greater (p=0.045) with ThuVaRP than with TURP, and the increase in maximal urine flow rate was greater (p<0.001) with ThuVaRP than with TURP. The postoperative complication transient urinary incontinence was significantly different between the ThuVaRP group (nine cases, 20.9%) and the TURP group (two cases, 4.7%). Other complications were comparable between groups.
Conclusions
The effectiveness and safety of ThuVaRP and TURP were comparable. ThuVaRP is a promising alternative surgical technique to TURP for BPH.
Keywords: Prostatic hyperplasia, Thulium, Transurethral resection of the prostate
INTRODUCTION
Benign prostatic hyperplasia (BPH) is one of the most common causes of urinary obstruction, which occurs in 50% to 60% of men aged 60 years or older [1]. Because of the increasing aged population and advancements in diagnostic tools, the incidence and importance of BPH have increased. BPH can be treated with pharmacotherapies and with surgery [2,3]. Transurethral resection of the prostate (TURP) has been recognized as the standard treatment for BPH [4]. Advancements in medical technology have resulted in the availability of a variety of laser therapies for the treatment of BPH, and it will not be long before they replace TURP as the standard treatment [5]. In many studies, holmium: yttrium-aluminium-garnet (YAG) laser enucleation of the prostate (HoLEP) or GreenLight laser photo selective vaporization (PVP) were proved to be safe and effective surgical procedures comparable with TURP. However, the ideal laser must have the effectiveness of the holmium:YAG laser plus the handling and safety properties of the GreenLight laser [6].
The recently developed thulium:YAG (Tm:YAG) laser has been found to be superior to the holmium:YAG laser in spatial beam quality and tissue incision precision and because of its ability to operate in continuous-wave pulsed modes [7]. Another advantage of the thulium laser is that it is based on vaporesection, which allows it to resect small pieces of prostate tissue without morcellation. European and Chinese groups have conducted many studies of Tm:YAG laser prostate surgery [8-12]. Two comparative studies of Tm:YAG laser vaporesection of the prostate (ThuVaRP) and monopolar TURP have been conducted, but no comparison of ThuVaRP with bipolar TURP has been conducted. In Korea, no study of Tm:YAG laser prostate surgery has been undertaken.
In this study, we assessed the effectiveness and safety of ThuVaRP in comparison with those of bipolar TURP.
MATERIALS AND METHODS
1. Subjects
This study was conducted in 86 patients who underwent operations to treat BPH at Daegu Fatima Hospital between January 2010 and December 2012; the patients' medical records were retrospectively analyzed. All operations were performed by a single surgeon. The subjects were limited to patients who satisfied the following conditions: a maximal urine flow rate (Qmax) of less than 15 mL/s or acute repeated urinary retention and an International Prostate Symptom Score (IPSS) greater than 7. This study excluded patients aged 85 or older, whose prostate weighted 100 g or more (on transrectal ultrasonography [TRUS]), whose BPH was accompanied by neurogenic bladder, or who had a history of prostate, bladder neck, or urethral surgery. Of the 86 patients, 43 underwent ThuVaRP and the remaining 43 underwent bipolar TURP.
Before surgery, the participants underwent a medical history, a physical examination, a digital rectal examination, routine laboratory tests, IPSS determination, TRUS, prostate-specific antigen (PSA) measurement, and uroflowmetry with postvoid residual volume (PVR) measurement. IPSS, TRUS, PSA, and uroflowmetry with PVR were reassessed 1 month after surgery for comparison with the preoperative data.
For patients whose PSA values were 4 or greater or who had any other risk factor (e.g., nodule on the digital rectal examination or hypoechoic lesion on TRUS), a prostate biopsy sample was collected before surgery to rule out cancer. The histopathologic analysis of the specimens showed BPH in all cases.
2. Instruments and surgical techniques
All operations were performed while patients were in the lithotomy position, most of whom were under spinal anesthesia. General anesthesia was limited to patients who could not receive spinal anesthesia. ThuVaRP was performed with a 70-W continuous-wave Tm:YAG laser (Revolix, LISA Laser Products OHG, Katlenburg-Lindau, Germany) and a 26-French continuous flow resectoscope (Richard Wolf Medical Instruments, Vernon Hills, IL, USA). Saline irrigation was used in all cases. A Tm:YAG laser was delivered through a 550-µm end-firing RigiFib-SU fiber.
At the beginning of the operation, an inverted U-shape incision distal to the resection border was made around the verumontanum. After an additional linear incision was made at 5 and 7 o'clock, the median lobe was vaporesected. Then, both lateral lobes were also vaporesected until the prostate capsule was identified. During vaporesection, it was important that the prostate tissue was cut into pieces small enough to pass through the resectoscope.
Bipolar TURP was performed in the traditional manner with the use of a bipolar electrical current generator and a wire loop (Gyrus Medical GMBH, Tuttligen, Germany) and a 24-French resectoscope (Karl Storz Endoscope, Tuttlingen, Germany). Saline irrigation was used in all cases. The cutting power and coagulating power were within 160 and 80 W, respectively. After surgery, a 20-French three-way silicone urethral catheter was placed in all patients to maintain continuous saline irrigation until the resolution of hematuria. A biopsy sample from each tissue was collected.
3. Assessments
An analytical between-group comparison was made of operation time, volume of resected tissue, remaining volume of the prostate (%), postoperative hemoglobin level, period of urethral catheterization (the catheter was removed when hematuria could not be visually observed anymore), days of hospitalization, and preoperative and postoperative data (collected 1 month after surgery) on IPSS, TRUS, serum PSA level, uroflowmetry with PVR, and, by extension, perioperative complications such as bleeding (required blood transfusion), temporary urinary retention (treated with recatheterization), urinary irritative symptoms such as dysuria, and temporary incontinence.
4. Verification
In this study, the unpaired Student t-test, the paired Student t-test, and the chi-square test were applied to the verification of findings. The unpaired Student t-test was used to verify the homogeneity and difference of continuous variables, the paired Student t-test was used to verify postoperative changes, and the chi-square test was used to verify the difference between groups in postoperative complications. The significance level was defined as a p-value <0.05.
RESULTS
All 86 patients underwent surgical treatment for symptomatic BPH, and each of the two groups included 43 patients. Prostate volume was somewhat greater in the ThuVaRP than in the TURP group, but the difference was not significant. The other parameters were also similar between groups (Table 1). The mean operation time was significantly longer in the ThuVaRP group than in the TURP group (113.6±44.4 minutes compared with 76.7±32.0 minutes, p<0.001). However, catheterization time (3.5±1.4 days compared with 5.4±1.8 days, p<0.001) and length of hospital stay (4.6±1.8 days compared with 6.4±1.8 days, p <0.001) were significantly shorter in the ThuVaRP group (Table 2). In the ThuVaRP group, the mean operation time was steadily or slightly greater in patients with a small prostate volume (≤50 g). However, the mean operation time was sharply greater in patients with a large prostate volume (>50 g) (Fig. 1). In each group, the changes in all parameters were significant 1 month after surgery. In the ThuVaRP group, IPSS declined by 57.2%, the PSA level fell by 82.7%, TRUS volume decreased by 66.7%, Qmax increased by 102.0%, and PVR decreased by 64.2% (Table 3). In the TURP group, IPSS declined by 51.6%, the PSA level fell by 65.2%, TRUS volume decreased by 60.9%, Qmax increased by 51.2%, and the PVR decreased by 51.7% (Table 4).
TABLE 1.
Baseline characteristics
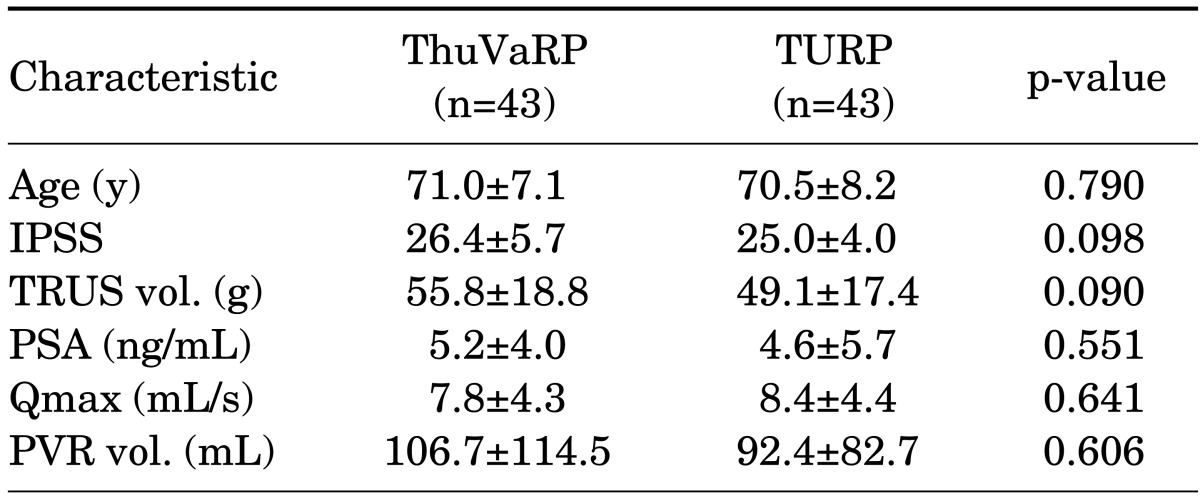
Values are presented as mean±standard deviation.
ThuVaRP, thulium laser vaporesection of the prostate; TURP, transurethral resection of the prostate; IPSS, International Prostate Symptom Score; TRUS, transrectal ultrasound; vol., volume; PSA, prostate-specific antigen; Qmax, maximum flow rate; PVR, postvoid residual.
TABLE 2.
Perioperative data
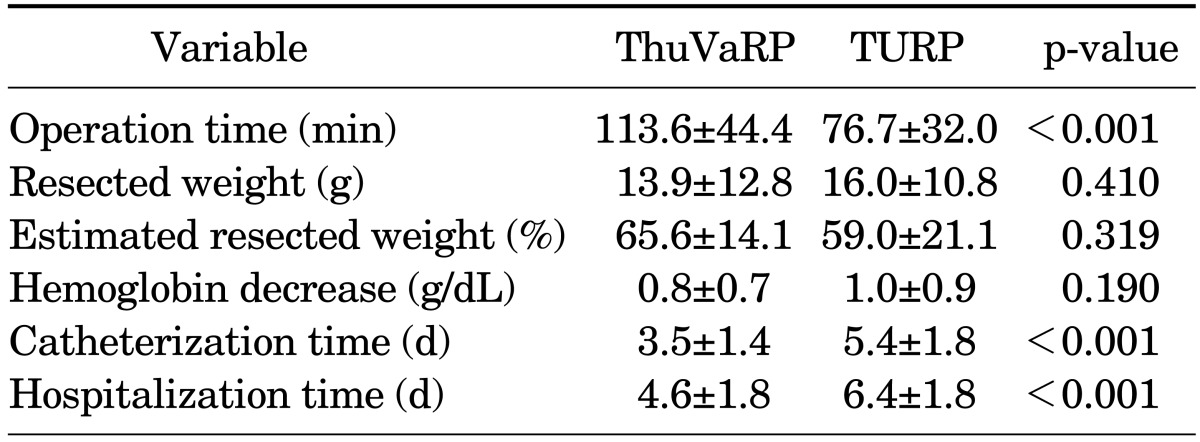
Values are presented as mean±standard deviation.
ThuVaRP, thulium laser vaporesection of the prostate; TURP, transurethral resection of the prostate.
FIG. 1.
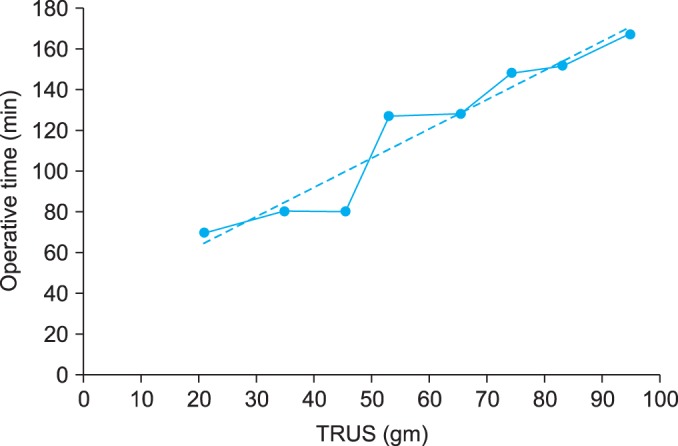
The mean operation time of the thulium laser vaporesection of the prostate. TRUS, transrectal ultrasound.
TABLE 3.
Changes in clinical parameters after ThuVaRP
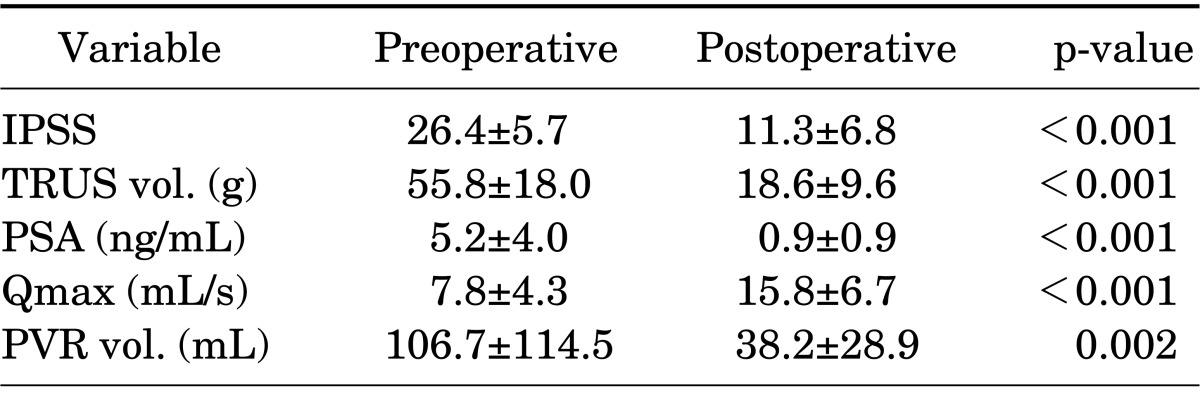
Values are presented as mean±standard deviation.
ThuVaRP, thulium laser vaporesection of the prostate; IPSS, International Prostate Symptom Score; TRUS, transrectal ultrasound; vol., volume; PSA, prostate-specfic antigen; Qmax, maximum flow rate; PVR, postvoid residual.
TABLE 4.
Changes in clinical parameters after TURP
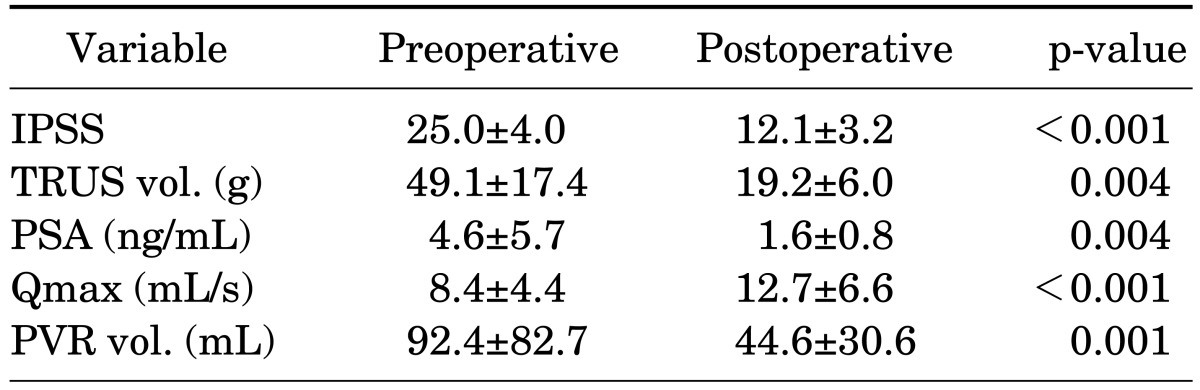
Values are presented as mean±standard deviation.
TURP, transurethral resection of the prostate; IPSS, International Prostate Symptom Score; TRUS, transrectal ultrasound; vol., volume; PSA, prostate-specfic antigen; Qmax, maximum flow rate; PVR, postvoid residual.
In the intergroup analysis, no significant differences between the ThuVaRP and TURP groups, respectively, were found for the changes in IPSS (15.4±9.8 compared with 13.2±4.7, p=0.357), TRUS volume (37.2±16.2 mL compared with 31.1±15.3 mL, p=0.387), and the PVR (85.4±109.4 mL compared with 65.4±58.9 mL, p=0.414). However, the numerical value was slightly higher in the ThuVaRP group. The decrease in PSA was greater in the ThuVaRP group than in the TURP group (4.3±3.6 ng/dL compared with 2.0±1.3 ng/dL, p=0.045). The increase in Qmax was also much greater (8.9±6.3 mL/s compared with 4.1±2.9 mL/s, p<0.001) in the ThuVaRP group (Table 5). Postoperative complications were checked for, such as bleeding requiring transfusion, temporary urinary retention, urinary irritative symptoms such as dysuria, and temporary incontinence. Blood transfusions were given to one patient (2.3%) and two patients (4.7%) in the ThuVaRP and TURP groups, respectively. Temporary urinary retention occurred in six patients (14.0%) and nine patients (20.9%), respectively. All patients improved after Foley catheterization for 3 to 4 days. Dysuria occurred in seven patients (16.3%) and three patients (7.0%) without significant intergroup differences. There was no febrile urinary tract infection and no culture-positive urinary tract infection, respectively. Temporary incontinence occurred in nine patients (20.9%; stress urinary incontinence in five patients, urge incontinence in three patients, and mixed incontinence in one patient) and two patients (4.7%; stress urinary incontinence in all cases), and the intergroup differences were significant; however, this condition changed for the better 4 weeks afterward (Table 6).
TABLE 5.
Comparison of perioperative data between ThuVaRP and TURP
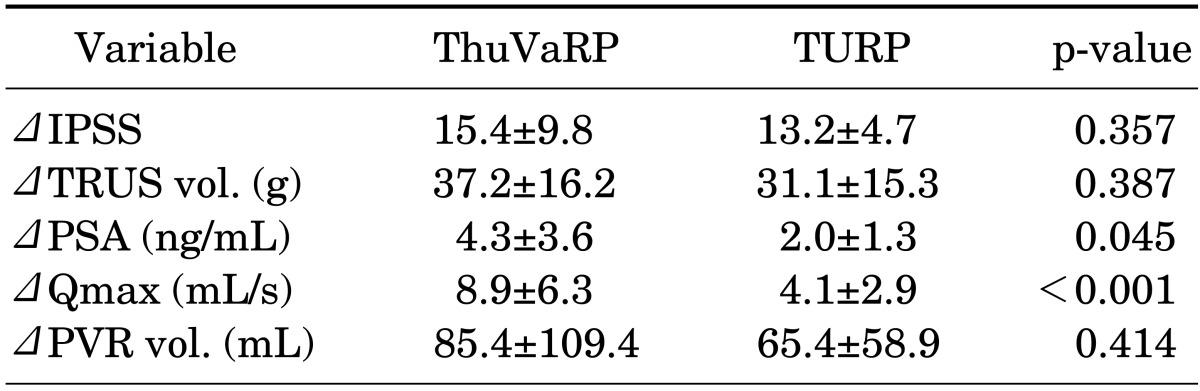
Values are presented as mean±standard deviation.
ThuVaRP, thulium laser vaporesection of the prostate; TURP, transurethral resection of the prostate; IPSS, International Prostate Symptom Score; TRUS, transrectal ultrasound; vol., volume; PSA, prostate-specfic antigen; Qmax, maximum flow rate; PVR, postvoid residual.
TABLE 6.
Postoperative complications
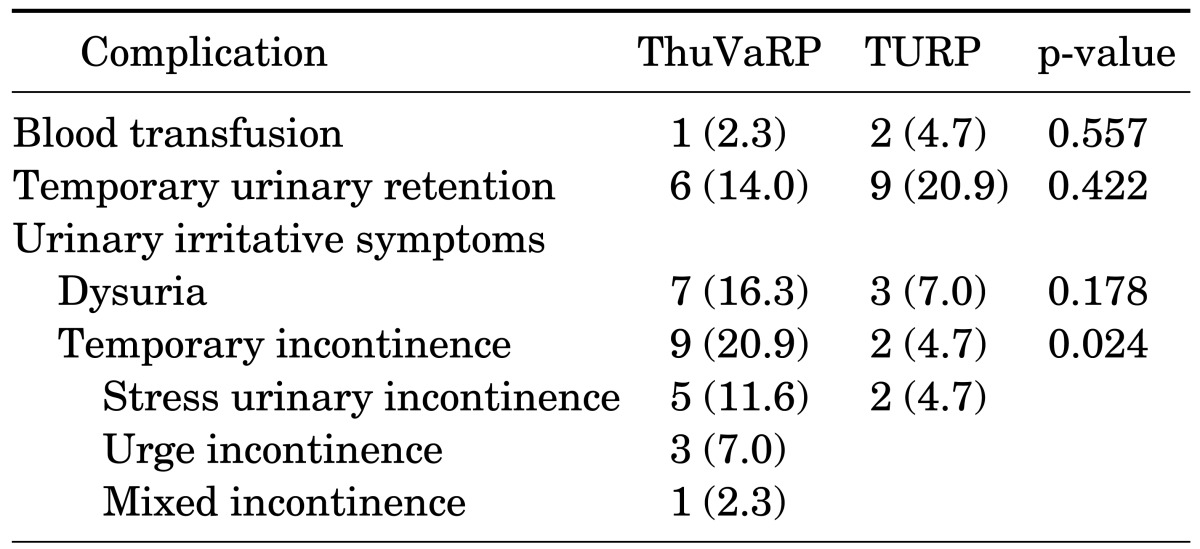
Values are presented as no. of cases (%).
ThuVaRP, thulium laser vaporesection of the prostate; TURP, transurethral resection of the prostate.
DISCUSSION
Currently, a variety of laser therapies are available for prostate surgery to treat BPH and have good results; thus, they are expected to replace TURP (the standard prostate surgery technique for BPH) before long. There have been many studies of PVP and HoLEP, which are widely recognized as substitutes for TURP or open prostatectomy [13]. Both of these procedures have had good results, even in high-risk patients or patients with large prostatic adenomas [14-16]. In particular, HoLEP is drawing attention as an alternative treatment for bladder outlet obstruction [9]. According to previous studies, HoLEP enables the endoscopic removal of prostatic adenoma regardless of its size and is as effective as open prostatectomy; moreover, it can decrease the severity of complications [16,17]. Despite good clinical results, both of these procedures have limitations. For HoLEP, the steep learning curve and longer operation time seem to be the major drawbacks and limit its widespread clinical application [18]. For PVP, no tissue specimen is provided for histologic evaluation, and the speed of tissue ablation is significantly slower [19].
The recently developed Tm:YAG laser works with a wavelength of 2013 nm, which can be easily absorbed into water, especially interstitial water. Its waves are more continuous than those of other lasers and therefore provide more effective hemostasis. In addition, it provides accurate resection with sufficient vaporization, and the moving laser probe maximizes vaporization but reduces the heat applied to tissue [10].
In 2005, Xia et al. [20] published the initial clinical report on Tm:YAG laser prostate surgery. They performed Tm:YAG laser resection with the prostate-tangerine technique on 30 patients and reported its safety and efficacy. Bach et al. [10] reported 1-y follow-up data on ThuVaRP, which showed a significant improvement in voiding symptoms and patients' quality of life.
Thus far, two studies have compared the efficacy and safety of ThuVaRP and monopolar TURP [6,11]. Fu et al. [6] compared the results of a prospective nonrandomized trial with 1-year follow-up between 58 patients who underwent ThuVaRP and 42 patients who underwent monopolar TURP. They concluded that ThuVaRP had favorable perioperative safety, had the same therapeutic effect as TURP, and had the advantage of significantly less blood loss, shorter length of hospital stay, and shorter catheter indwelling time compared with monopolar TURP. However, the mean operation time was slightly longer in the ThuVaRP group. Xia et al. [11] performed a prospective randomized trial comparing 52 patients who underwent ThuVaRP with 48 patients who underwent monopolar TURP. They reported that ThuVaRP was significantly superior to TURP in terms of catheterization time, length of hospital stay, and decrease in hemoglobin, although it required an equivalent time to perform. In their report, ThuVaRP was as efficacious as TURP after 1 year of follow-up.
In the current study, ThuVaRP was associated with a shorter catheterization time and a shorter hospital stay compared with TURP. However, unlike the two abovementioned studies, the improvement in Qmax was much greater. We thought that this might have resulted from the greater resection volume with prostate adenoma. Although the resection volume of prostate tissue was smaller with ThuVaRP than with TURP, the decrease in TRUS volume was much greater than that with TURP. Also, the reduction in PSA value, which might be a proxy indicator of prostate tissue removal, is much greater with ThuVaRP. The strong vaporization ability of the thulium laser might have contributed to this result.
The results for ThuVaRP were equivalent or superior to those for TURP in the short term. However, the operation time was longer with ThuVaRP than with TURP, for two possible reasons. First, TURP has been the standard surgery used to treat BPH, and surgeons have become experienced with this procedure. In contrast, ThuVaRP is a newer procedure and, although the technique is similar to that of TURP and is easy to learn, surgeons need to overcome the learning curve. Second, as the prostate volume increased, the operation time increased much more than the increase in prostate volume. Thus, ThuVaRP is a more suitable surgical technique for relatively smaller prostates [10,11].
Postoperative complications such as bleeding requiring transfusion, temporary urinary retention, and dysuria were not significantly different between the treatment groups. However, temporary incontinence occurred more frequently in the ThuVaRP group (nine patients) than in the TURP group (two patients), possibly because of technical problems associated with the manipulation of the resectoscope and laser fiber around the external urethral sphincter area, because two previous comparative studies reported no difference in temporary incontinence [6,11].
ThuVaRP met functional outcome and safety expectations; however, it did not meet efficacy expectations in patients with a large prostate because of the prolonged operation time in this group. This could be interpreted as a potential disadvantage of Tm:YAG laser prostatectomy compared with the previously introduced HoLEP. Bach et al. [12] introduced the technique of Tm:YAG laser vapoenucleation of the prostate (ThuVEP) to identify the efficacy of Tm:YAG laser prostatectomy in patients with a larger prostate. They concluded that the functional outcome of ThuVEP was comparable with that of HoLEP. Also, there was no limitation in prostate size. Herrmann et al. [21] published a modified ThuVEP technique, i.e., blunt enucleation of prostate adenoma with laser support. They called this technique Tm:YAG laser enucleation of the prostate (ThuLEP). As the number of institutes equipped with Tm:YAG lasers has increased, more studies of Tm:YAG laser surgery for BPH have been investigated. The results are promising, but more long-term data and well-designed comparative studies with TURP and other laser technique are needed.
The limitations of this study were its nonrandomized design and its short follow-up period. More cases and long-term data are needed to clarify the usefulness of ThuVaRP. We believe that ThuVaRP is a promising technique for the effective surgical management of BPH.
CONCLUSIONS
ThuVaRP, a new laser therapy, has shown results equivalent or superior to those of TURP in terms of effectiveness and safety. Although further well-designed comparative studies and long-term data are needed, we suggest that ThuVaRP can be an alternative to TURP for the surgical management of BPH.
Footnotes
The authors have nothing to disclose.
References
- 1.Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132:474–479. doi: 10.1016/s0022-5347(17)49698-4. [DOI] [PubMed] [Google Scholar]
- 2.McNeal J. Pathology of benign prostatic hyperplasia. Insight into etiology. Urol Clin North Am. 1990;17:477–486. [PubMed] [Google Scholar]
- 3.Hwang EC, Joo JS, Min KD, Oh BR, Kang TW, Kwon DD, et al. A short-term comparative study on efficacy and safety of standard transurethral resection and high power (80W) potassium-titanyl-phosphate laser vaporization of the prostate. Korean J Urol. 2005;46:1251–1255. [Google Scholar]
- 4.Wasson JH, Reda DJ, Bruskewitz RC, Elinson J, Keller AM, Henderson WG. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. The Veterans Affairs Cooperative Study Group on Transurethral Resection of the Prostate. N Engl J Med. 1995;332:75–79. doi: 10.1056/NEJM199501123320202. [DOI] [PubMed] [Google Scholar]
- 5.de la Rosette J, Alivizatos G. Lasers for the treatment of bladder outlet obstruction: are they challenging conventional treatment modalities? Eur Urol. 2006;50:418–420. doi: 10.1016/j.eururo.2006.04.013. [DOI] [PubMed] [Google Scholar]
- 6.Fu WJ, Zhang X, Yang Y, Hong BF, Gao JP, Cai W, et al. Comparison of 2-microm continuous wave laser vaporesection of the prostate and transurethral resection of the prostate: a prospective nonrandomized trial with 1-year follow-up. Urology. 2010;75:194–199. doi: 10.1016/j.urology.2009.07.1266. [DOI] [PubMed] [Google Scholar]
- 7.Fried NM, Murray KE. High-power thulium fiber laser ablation of urinary tissues at 1.94 microm. J Endourol. 2005;19:25–31. doi: 10.1089/end.2005.19.25. [DOI] [PubMed] [Google Scholar]
- 8.Szlauer R, Gotschl R, Razmaria A, Paras L, Schmeller NT. Endoscopic vaporesection of the prostate using the continuous-wave 2-microm thulium laser: outcome and demonstration of the surgical technique. Eur Urol. 2009;55:368–375. doi: 10.1016/j.eururo.2008.10.034. [DOI] [PubMed] [Google Scholar]
- 9.Elzayat EA, Habib EI, Elhilali MM. Holmium laser enucleation of the prostate: a size-independent new "gold standard". Urology. 2005;66(5 Suppl):108–113. doi: 10.1016/j.urology.2005.06.006. [DOI] [PubMed] [Google Scholar]
- 10.Bach T, Herrmann TR, Ganzer R, Burchardt M, Gross AJ. RevoLix vaporesection of the prostate: initial results of 54 patients with a 1-year follow-up. World J Urol. 2007;25:257–262. doi: 10.1007/s00345-007-0171-x. [DOI] [PubMed] [Google Scholar]
- 11.Xia SJ, Zhuo J, Sun XW, Han BM, Shao Y, Zhang YN. Thulium laser versus standard transurethral resection of the prostate: a randomized prospective trial. Eur Urol. 2008;53:382–389. doi: 10.1016/j.eururo.2007.05.019. [DOI] [PubMed] [Google Scholar]
- 12.Bach T, Wendt-Nordahl G, Michel MS, Herrmann TR, Gross AJ. Feasibility and efficacy of Thulium:YAG laser enucleation (VapoEnucleation) of the prostate. World J Urol. 2009;27:541–545. doi: 10.1007/s00345-008-0370-0. [DOI] [PubMed] [Google Scholar]
- 13.Bach T, Netsch C, Haecker A, Michel MS, Herrmann TR, Gross AJ. Thulium:YAG laser enucleation (VapoEnucleation) of the prostate: safety and durability during intermediate-term follow-up. World J Urol. 2010;28:39–43. doi: 10.1007/s00345-009-0461-6. [DOI] [PubMed] [Google Scholar]
- 14.Ruszat R, Wyler S, Forster T, Reich O, Stief CG, Gasser TC, et al. Safety and effectiveness of photoselective vaporization of the prostate (PVP) in patients on ongoing oral anticoagulation. Eur Urol. 2007;51:1031–1038. doi: 10.1016/j.eururo.2006.08.006. [DOI] [PubMed] [Google Scholar]
- 15.Rajbabu K, Chandrasekara SK, Barber NJ, Walsh K, Muir GH. Photoselective vaporization of the prostate with the potassium-titanyl-phosphate laser in men with prostates of >100 mL. BJU Int. 2007;100:593–598. doi: 10.1111/j.1464-410X.2007.06985.x. [DOI] [PubMed] [Google Scholar]
- 16.Elzayat EA, Elhilali MM. Holmium laser enucleation of the prostate (HoLEP): the endourologic alternative to open prostatectomy. Eur Urol. 2006;49:87–91. doi: 10.1016/j.eururo.2005.08.015. [DOI] [PubMed] [Google Scholar]
- 17.Hwang JC, Park SM, Lee JB. Holmium laser enucleation of the prostate for benign prostatic hyperplasia: effectiveness, safety, and overcoming of the learning curve. Korean J Urol. 2010;51:619–624. doi: 10.4111/kju.2010.51.9.619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Elzayat EA, Elhilali MM. Holmium laser enucleation of the prostate (HoLEP): long-term results, reoperation rate, and possible impact of the learning curve. Eur Urol. 2007;52:1465–1471. doi: 10.1016/j.eururo.2007.04.074. [DOI] [PubMed] [Google Scholar]
- 19.Ruszat R, Seitz M, Wyler SF, Abe C, Rieken M, Reich O, et al. GreenLight laser vaporization of the prostate: single-center experience and long-term results after 500 procedures. Eur Urol. 2008;54:893–901. doi: 10.1016/j.eururo.2008.04.053. [DOI] [PubMed] [Google Scholar]
- 20.Xia SJ, Zhang YN, Lu J, Sun XW, Zhang J, Zhu YY, et al. Thulium laser resection of prostate-tangerine technique in treatment of benign prostate hyperplasia. Zhonghua Yi Xue Za Zhi. 2005;85:3225–3228. [PubMed] [Google Scholar]
- 21.Herrmann TR, Bach T, Imkamp F, Georgiou A, Burchardt M, Oelke M, et al. Thulium laser enucleation of the prostate (ThuLEP): transurethral anatomical prostatectomy with laser support. Introduction of a novel technique for the treatment of benign prostatic obstruction. World J Urol. 2010;28:45–51. doi: 10.1007/s00345-009-0503-0. [DOI] [PubMed] [Google Scholar]