

Abstract
Background:
Prevention of diseases in gynecology can be improved by better understanding of health promotion and management of diseases. Management is “the art of performing jobs by or with other people” Mary Parker Follet.
Methods:
A descriptive analysis was performed on scientific studies in several published articles in medical journals and books.
Results:
There are five primary functions of management as: Anticipate and plan, organize, command, coordinate and control. If we introduce the following definition in the sense of medical science and apply it to the medical practice that would mean way of recognizing, managing and resolving issues of diagnosis and therapy of diseases (in this case gynecology diseases) according to certain guidelines and treatment algorithms. Treatment of family doctors is an important aspect in the quality-of-life of women and their reproductive health as well as a significant issue in public, environmental and social problems.
Conclusions:
It is very important to deal with it on the primary care level and in addition to promote the primary and secondary prevention of diseases, which is sometimes more important than the curative procedures. The primary prevention involves regular gynecological examinations and screening. The doctors have also a duty to educate women about the risk factors for malignant diseases, as well as proposing some of the qualitative preventive measures.
Keywords: Diseases, gynecology, malignancies, prevention
INTRODUCTION
Management is “the art of performing jobs by or with other people” Mary Parker Follet [Figure 1]. This is one of the many definitions of management, but apart from these definitions, it is very important to mention one of the general management theory postulates that gave Henry Fayol and which proposed the five primary functions of management as: Anticipate and plan, organize, command, coordinate and control.
Figure 1.

Mary Parker Follet
In the few last decades, papilloma and herpes viruses gets more importance in the development of epithelial dysplasia, neoplasia and cervix cancer. Cervix cancer has the second place in mortality from gynecology diseases with the incidence of 350,000 new cases diagnosed each year.
In countries where screening is well-developed, such as England, the number of women suffering and dying from cervix cancer has been reduced by 80%. Breast cancer is the most common cancer among women (about 32% of all cancers) and the most common cause of death in the age of 45-55 years. In the world, about 1 million new cases are registered each year. In developed countries, mortality was significantly reduced to about 25%, thanks to the early detection and modern therapy. The incidence of the polycystic ovary syndrome (PCOS) is 15-25% in the population of women in the reproductive age according to the European criteria. It is more common in adolescents with 25%. Luckily, after the age of 40 it is relieved by hyperandrogenemia spontaneously so that in this age the incidence is about 15% and in perimenopausal period the incidence is 10%.
Diagnosis is made by medical history (general, gynecologic, family), clinical examination (general condition of the patient-performance status and gynecological speculum examination, bimanual and rectal), by taking the smear by Papanicolaou method and histological examination after biopsy. Papanicolaou test is the standard test for cervix cancer detection and like some results of several studies shows this cytological test reduces the incidence of cervix cancer in many countries.
Numerous studies have shown that the rate of incidence and mortality are significantly reduced where there is organized screening. The general practitioners has an important role to make sure that most of the women are attending regular, systematic gynecological examinations according to recommendation that exist in the national guide for the prevention of malignant diseases.
In terms of medical science and practice this imply: How to identify, lead and resolve, also treat the diseases according to certain guidelines and treatment algorithms. Furthermore, disease management and compliance means algorithms and the adoption of certain postulates by family doctors in the health care centers as they represent the first line of meeting and solving certain diseases and conditions in patients.
Management of gynecological diseases represents the application in the field of gynecological diseases. Gynecological diseases are diseases of the female genital organs and within it we can talk about sexually transmitted diseases and obstetrics.[1,2,3,4,5] Their diagnosis and treatment is an important aspect of the quality-of-life of women and their reproductive health because these diseases are public health and social problem and is very important to deal with them at the level of primary health-care (PHC), so in this context to promote both primary and secondary prevention.[6,7] Sometimes, this is more important than curative procedures. First of all, it is important to promote a healthy life-style and conscious entering the sexual activity by young girls. Primary prevention involves regular gynecological examinations and screening. Screening involves preventive examinations, which test apparently healthy population with a preventive goal in order to identify as early as possible those who show early signs of disease or are at risk for the development of a disease. In addition to primary prevention and screening it is important to emphasize education of patients about the importance of a healthy life-style and explaining hygienic and diet measures for certain diseases. Thus, achieves the effect that patients understand the importance of the early of the prevention of gynecological diseases and the application of regular screening for their early detection in order to eradicate the disease.
Here, we will specify the definition and epidemiology of the most frequent gynecological diseases and their risk factors: Cervical cancer, breast cancer, PCOS, irregular bleedings from the uterus and vulvovaginitis.
In recent decades, to papilloma and herpes viruses is attributed the growing importance in the emergence of epithelial dysplasia, neoplasia and cervical cancer. It is believed that the influence of these viruses that penetrate the epithelium around the outer cervix at the place of metaplasia of the layered stratified epithelium in the cylinder caused changes in epithelial cells that lead to dysplasia. Cervical cancer primarily affects women from 45 to 50 years of age; approximately 37% of patients are younger than 35 years. Women over 65 make up 10% of patients and this age group usually dies from the disease, which is related to progression of the disease at the time of diagnosis.
Among gynecological malignancies cervical cancer ranks second both in incidence and mortality among women in almost all developed countries, diagnosed each year. Although in recent years their incidence declined, there are still areas of high incidence of mortality among women of low socio-economic status, which is a consequence of the lack or absence of regular and irregular screening. In countries where screening is well-developed, such as England, the number of women suffering and dying from cervical cancer has been reduced by 80%. At 5-year survival for patients with early clinical stage varies from 50% to 90% according to various prognostic factors. Local recurrence is a significant cause of mortality. Scientific evidences support the link between human papilloma virus (HPV) infections which is present in 93% of cases of cervical neoplasia. The risk of malignant transformation in the cervix increases with the presence of high-risk genital HPV subtypes. Among more than 70 so far detected HPV virus types, most probable role in oncogenesis have subtypes 16, 18, 31, 33 and 35. The disease often affects persons from lower socio-economic class, with a lower possibility of regular health-care. Early onset of sexual life and a greater number of sexual partners, also favors the development of the disease. Specifically, the transformation zone in the younger age is more sensitive to oncogenic agents. Smoking is also a significant risk factor. The role of oral contraceptives to date remains controversial. Opinions are divided, but higher incidence of abnormal histological types of cervical cancer is observed in women who have for a longer period of time used these contraceptives.
Breast cancer occurs and develops from the milk ducts (duct epithelium) and lobule, so the most common types are ductal (80%) and lobular (10%) breast cancer. It can be in invasive and non-invasive form (ductal carcinoma in situ) and (lobular carcinoma in situ). Breast cancer is the most common cancer in women (about 32% of all malignancies) and the most common cause of death at the age of 45-55 years. In the world are registered each year about 1 million new cases. In developed countries, mortality was significantly reduced to about 25%, thanks to early detection and modern therapy. Survival is slightly lower in women younger than 40 years (82%), 40-74 years of age (88%) and at age of 75 years and over (89%). Screening is the examination of women who have no symptoms of the disease, with the purpose of early detection of cancer. At these examinations, the women are called for a review, which is repeated at certain intervals. It is not known exactly what causes the appearance of breast cancer, but it is known that there are several risk factors, some of which are already known from before; others are yet to be explored. The frequency (incidence) of breast cancer increases with age, about 80% occurs after menopause. It is extremely rare before age of 20 years of age and is also unusual before age of 35 years.
Women who were previously treated for breast cancer have 2 times greater risk of developing cancer in the other breast. Among hereditary factors often are mentioned the two breast cancer genes: BRCA1 and BRCA2.
Few women in the course of their lives, especially in the age of sexual maturity, did not have an acute infection, subacute or chronic, at the level of the external genitalia. Whether it comes to an acute infection, recurrent from inactive focal points or repeated infection (reinfection) is very often health, family and social problem, as they often have to be for long and persistently treated and that the conservative and surgical therapy eliminates its consequences or complications.
Vaginitis is an inflammation of the lining of the vagina. Vulvitis is an inflammation of the vulva. Vulvovaginitis is an inflammation of the vulva and vagina. In these situations there is inflammation of the tissues, which sometimes leads to vaginal discharge. The causes are infection (Streptococcus, Staphylococcus, Escheria coli, Neisseria gonorhea, Chlamydia trachomatis, Trichomas vaginalis, Mycoplasma hominis, also HPV, Cytomegalovirus, etc.). Possible causes are also irritants in the form of substances or objects, tumors or other abnormal buildup of tissue, irradiation therapy, medications and hormonal changes. Poor personal hygiene can contribute to the proliferation of bacteria and fungi and cause irritation. The feces can enter the vagina through the abnormal connection with the guts (fistula), which can lead to inflammation of the vagina.
PCOS is the most common reproductive and metabolic disorder in women of childbearing age, which is characterized by chronic anovulation/oligomenorrhea, hyperandrogenism and the appearance of polycystic ovaries. Often is associated with obesity, hyperlipidemia, insulin resistance (IR) and type II diabetes. The incidence of the syndrome is 15-25% of the female population childbearing age according to the European criteria for diagnosis. It is somewhat more common in adolescents and amounts to 25%. It is the lucky circumstance that after the age of 40 it is spontaneously relieved by hyperandrogenaemia and ovulation are more common, so in this age its incidence is around 15% and perimenopausal incidence is 10%. Because of the many preceding pathophysiology changes of PCOS it seems to affects very heterogeneous group of patients. Despite the extensive literature data on the etiology of PCOS, no uniform position on the nomenclature and criteria used in the definition of the syndrome exist. In 2003, it needed two of the three criteria for the diagnosis of PCOS: Oligo/anovulation, clinical or biochemical signs of elevated androgens and polycystic ovaries demonstrated by ultrasound (US). Furthermore, for the diagnosis of PCOS it is necessary to exclude a number of conditions and diseases related to similar changes in the appearance of ovarian US image. Just the appearance as polycystic ovaries is not sufficient for the diagnosis of this syndrome. Diseases and conditions that should be by differential diagnosis excluded are hyperprolactinemia, gonadotropin, congenital adrenal hyperplasia, Cushing's syndrome, virilizing tumors, hypothalamic amenorrhea, acromegaly, hipertecosis, glucocorticoid and IR and the effect of some medications. Childhood obesity, especially in adolescence is the most important trigger for the development and worsening of PCOS. It was found that adolescent obesity independently contributes to disorders at childbearing age, as well as premature menarche, later infertility, infertility, abnormal pregnancies and IR.
Any bleeding from the uterus that is not regular menstruation is considered as abnormal (metrorrhagia). Menorrhagia may result from anatomical (visible pathological changes in some of the genital organs) and functional reasons. They may differ, not only in the time of occurrence, duration, amount of the lost blood, but also at intervals. It may be encountered during the entire period of fertile age of the women. However, it is significantly often seen at puberty and menopause, as well as juvenile and menopausal bleeding (explained by a disturbed balance in those ages between the ovaries and other endocrine glands).
Causes of primary dysmenorrhea and mechanism of pain occurrence in it are not known today. It is believed that a substantial influence have psychological factors, due to the threshold of sensitivity of different people. More frequent occurrence of dysmenorrhea is in underdeveloped and physically weak parsons, who are suffering from anemia, diabetes, tuberculosis and other exhaustive diseases. For them to achieve good therapeutic results it is necessary the healing and repair of the general health condition. Among etiological factors great attention is paid to the factors that may lead to partial or complete temporary obstruction. It is believed that the main cause is hormonal imbalance between estrogen and progesterone. The fact that dysmenorrhea does not occur during anovulatory cycle, when the endometrium is affected mainly by estrogen.
GOALS
The goals of this study were:
To understand the role of the health system in early diagnosis of gynecological diseases
Emphasize the importance of prevention through the management of gynecological diseases
Highlight the role of family doctors in educating women about the importance of regular gynecological examinations.
METHODS
Made is a descriptive analysis of experience of gynecological and obstetric diseases management described in the articles published in indexed journals retrieved from biomedical databases: PubMed Central, ScopeMed, Google Scholar, etc., The authors of articles are mostly from the former Yugoslavia. Emphasis is placed on the Guidelines for gynecological diseases because they are basic landmark that doctors should respect and use in the management of any disease and also gynecological. These are guides to whom physicians should adhere and stick to them and their algorithms in the course of their work. Within this set are: Basic symptoms, how to identify and diagnose and therapy protocols for the most common gynecological diseases, as parameters to procedures in managing gynecological and obstetric diseases.
MANAGEMENT OF COMMON GYNECOLOGICAL DISEASES
For cervical cancer there are no early symptoms, which will prompt the patients to contact a doctor for review. Symptoms usually occur at a later stage when it came to the erosion that accompanies contact bleeding (bleeding is usually sparse and occurs after intercourse, irrigation or gynecological exam). They can be frequent and persistent, resistant to therapy with concomitant blood secretion and in advanced stage also with severe pain.
Diagnostic procedure includes: History (general, gynecological, family, targeted family), clinical examination (general patient state, physical examination and gynecological speculum examination, bimanual and rectal examination) and swab by Papanicolaou method. The standard Papanicolaou test for detection of cervical cancer as the results of several studies indicated is cytological test, which reduces the incidence of cervical cancer in many countries. Papanicolaou test has limitations such as low sensitivity and poor reproducibility. Cytomorphologicall examination of cervicovaginal smear is performed by “The Bethesda system” classification: Atypical squamous cell of undetermined sigificance (ASCUS), atypical glandular cell of undetermined significance (AGUS), low-grade squamous intraepithelial lesions (LSIL) and high-grade squamous intraepithelial lesions (HGSIL) and histopathological examination of the biopsies of the cervix and cervical canal abrasion.
Additional tests, which are needed to determine the stage of the disease, are: Cystoscopy, rectoscopy, intravenous pyelography and chest X-ray. US, computed tomography, magnetic resonance imaging (MRI) and abdominal lymphangiography and possible laparoscopy may not be used to determine the clinical stage of disease according to International Federation of Gynecology and Obstetrics (FIGO), but are important in planning treatment. The clinical stage of the disease is determined by using the FIGO classification, which is also called morphological classification because it is based on tumor size and histological data for the early stages and the spreading of pelvic masses with disease progression [Figure 2].
Figure 2.
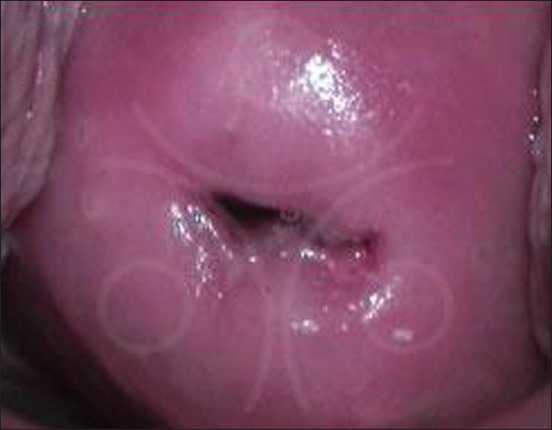
Colposcopy finding of the cervix cancer
Stage 0 - Changes within the epithelium, or preinvasive cancer (stroma intact).
Stage I - The cancer is affected only cervix without spreading to the body of the uterus.
Ia1 - Stromal invasion between 1 and 3 mm with horizontal spread of up to 7 mm
Ia2 - Invasion into the stroma of 3-5 mm from the horizontal spread of up to 7 mm
Ib1 - Clinically evident cervical lesions up to 4 cm in size
Ib2 - Clinical cervical lesions greater than 4 cm.
Stage II - Expansion at the upper and middle third of the vagina or parametrium (does not reach the bone).
IIa1 - Initial expansion into fornix
IIa2 - Spreading into the upper and middle third of the vagina
IIb1 - Initial infiltration of parametrium
IIb2 - Parametrium infiltration, but not reaching the bone.
Stage III - Spread to the pelvic wall or lower third of the vagina and/or hydronephrosis and/or kidney dysfunction.
IIIa - Infiltration into lower third of the vagina
IIIb - Tumor spread to the pelvic wall and/or kidney hydronephrosis and/or kidney dysfunction.
Stage IV - Spreading outside of pelvis
IVa - Spread into surrounding organs (bladder or colon)
IVb - Distant metastases.
After classification, according to the FIGO classification and staging of disease, the decision and the sequence of therapeutic procedures for each patient individually, is made by a multidisciplinary team of radiologists, pathologists, gynecologists, radiation oncologists and medical oncologists. Only a multidisciplinary approach to treatment may result in properly and successfully treatment and result in an overall improvement of survival. Surgical therapy should be carried out in institutions that have requirements for specified diagnostic and multidisciplinary treatment planning. It should aim to total removal of a diseased organ and lymphadenectomy (minimum of 10 lymph nodes from the chain of iliac blood vessels, both sides). Adjuvant therapy should begin within a period of 3-6 weeks after surgery or with advanced disease immediately after the diagnosis and staging of the disease. Concomitant chemo and radiotherapy should be conducted in an institution that has the technology for high voltage radiotherapy and intra-cavitary radiotherapy.
Self-examination includes periodic examination that the woman herself done by watching and feeling the texture of the breast and axillary lodge. For this review she should be taught by a doctor or nurse of family medicine. Self-examination should begin at the age of 20 years. Previously advised monthly self-examination is abandoned in many developed countries and is left to women to choose whether to use it and in what interval and then follows clinical examination. This includes physical examination by a physician. Doctor carefully observe the breast, their environment and with palpation explores possible changes in the breast and adjacent lymph nodes. Clinical examination should be conducted at least once every three years for all women who do not belong to a risk group, aged 20-40 years.
From the age of 40 a woman should once a year have clinical examination and then to perform the initial (basic) mammographs. It is best that clinical examination precedes mammography. If there is a screening program, it in some countries starting with the age of 40, in some at age of 45 or 50 years, to age of 65 or 70 years, depending upon the incidence of cancer, the available resources and the level of population health culture. Mammography is the “gold standard” of breast cancer diagnosis and the most important screening method.
Mammography is a radiological imaging method for breast that uses minimal radiation dose and allows you to see the internal structure of the breast. It is very important that the doctor discussed with the woman and advise her about the best time for her regular mammogram control in accordance with the existing guide for screening, so it does not happened that in the meantime the tumor that was not visible progresses. Mammography as a diagnostic tool has a much lower value (reliability) in younger (premenopausal) women due to developed glandular breast tissue that makes it radiologically “dens” or poorly visible for interpretation. In these cases, necessary are additional methods, US and where possible, MRI.
US is an additional (complementary) method for diagnosis using US waves, without ionizing radiation, it is completely harmless and can be used indefinitely even in pregnant women. It is used in finding tumors in the dens breasts, for example in young premenopausal women. MRI is a modern, complementary method. Not a method for mass screening, but in recent years can be used for the diagnosis of tumors in genetically predisposed women, where the screening normally begins in early premenopausal period, then in case of more dense breast tissue. When the radiologist in the mammography images finds a change that raises doubts on cancer, or is not able to declare it a benign, it is necessary to take a small sample of cells from the area for cytological examination and setting cytological diagnosis. Before treatment the set diagnosis of cancer, allows the duly treatment plan, selection of the best method for treatment (for example, type of surgery) in consultation between the patient and team of specialists who will treat. Although breast cancer is a very serious disease, it can be successfully treated if detected at an early stage, when it is not invasive and when tumor cells do not have the ability for displacement-metastasizing. This treatment can be successful if it is carried out by an expert team of specialists comprising of: A surgeon, radiation oncologist, internist-medical oncologist, radiologist, pathologist, oncology nurse, social worker and others as needed. This expert team examines the patient at one place, within joint review and makes decisions on any additional diagnostic tests, treatment method and sequence of methods.
In this way, each patient gets the best possible treatment. If the cancer has not metastasized and if not locally advanced, treatment usually begins with the surgical procedure. If the tumor is small, only the tumor can be removed and part of the surrounding healthy breast tissue (sparing surgery) so that the breast is not removed. At the same time will be removed a number of lymph nodes from the armpit. In some cases, it will be necessary to perform radical surgery. After radical surgery plastic reconstructive surgery may follow to make a new breast, immediately during breast removal, or when all other therapies are completed. After this surgery irradiation treatment is carried out. Irradiation therapy last for about 6 weeks and usually does not cause special problems.
With the presence of a vulvitis of any etiology, the patient complains of itching and burning sensation and burning of the skin around the vulva and vaginal introitus. On examination the vulvar skin is bright red, easily swollen, painful and warmer than surrounding tissue. First signs of infection are redness and smaller island of the affected areas of skin. Symptoms include a feeling of itching, burning or light pain. Condyloma are warty growths that occur as a consequence of infection by Papova virus (from a group of HPV type 6 and type 11), first individually around vaginal introitus, usually at first in the area of the perineum and later spread to most of the vulvar skin, mucous membrane of the vagina and cervix. Usually transmitted by sexual intercourse and formed over a period of few days to months after infection. Individual condyloma is bright red colors on the stalk or tapered at the top. Later, they can multiply to form a broad plate of compressed and joined individual warts.
Diagnosis is made based on history (general, gynecological, family, targeted family), clinical examination (general condition of the patient, physical examination and gynecological speculum examination, bimanual and rectal examination) as well as histological examination of taken biopsy material. If the cause is the infection, the treatment consists of antibiotic, anti-fungal or antiviral medications, depending on the agent.
If the infection is cured, to maintain the improved condition can be used for a short time rinsing of the vagina by exact ratio of vinegar and water. Frequent washing and use of medical type detergents is not advisable because it increases the risk of developing pelvic inflammatory disease. With antibiotics, treatment of bacterial infections may include propionic acid gel that makes more acidic vaginal mucus, which hinders the growth of bacteria. In case of STDs both partners must be treated simultaneously to prevent re-infection.
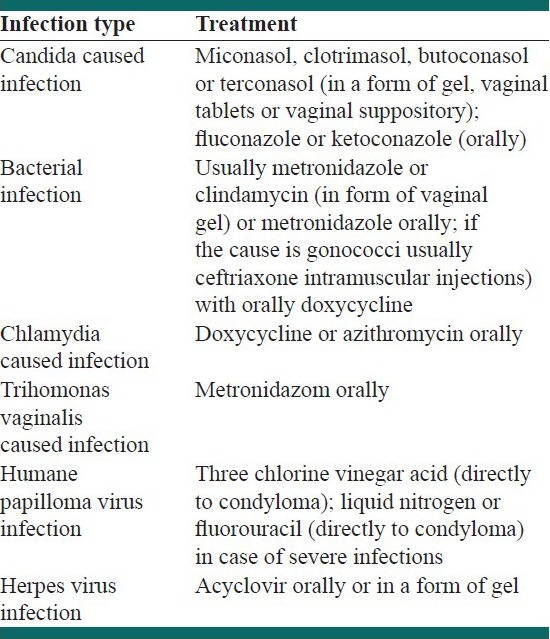
Thinning of the lining of the vagina after menopause is treated with estrogen supplements. Estrogen can be administered orally or by skin patch, or it can be applied directly to the vulva and vagina. Additional procedures include wearing comfortable and absorbent lingerie that allows air to circulate, such as cotton or cotton padded panties and maintaining the hygiene of the vulva. It is needed to use glycerin soap because other soaps can irritate this area. Sometimes, putting ice on the vagina, sitting in cold baths or cold compresses can ease sensitivity and itching. Itching that is not caused by infection can be mitigated by corticosteroid creams and ointments, such as those that contain hydrocortisone, as well as antihistamines taken orally. If chronic vulvitis is caused by poor personal hygiene, the first to be given is instructions on proper hygiene. Following are some guidelines for the treatment of vulvovaginitis caused by different agents [Table 1].
Table 1.
The usual treatment of infection of the vagina and vulva
The diagnosis of PCOS is based on the case history and physical examination, biochemical tests and US examination of the ovaries.
There are a number of data from medical history and physical findings that help in the diagnosis of PCOS.
In the family history are important diabetes, hyperandrogenaemia and clinical signs of hyperandrogenism, subfertility. In personal history is important birth weight, rapid weight gain in infancy, rapid growth and early adrenarhe, obesity in childhood and adolescence, menarche, menstrual cycle characteristics, weight changes, symptoms of hyperandrogenism, infertility and miscarriages. Physical examination includes determination of body mass index, the ratio of waist and hip circumferences, blood pressure measurement and evaluation of hyperandrogenism. Signs of hyperandrogenaemia and hyperandrogenism, which involves increased activity of androgens, are seborrhea, oily skin and hair, acne, hirsutism, alopecia and virilization. Hirsutism should be distinguished from hypertrichosis in which there is no male-type hair distribution and is not dependent on androgens.
However, the most common disorder in PCOS is anovulation in more than 90% of women, which is primarily linked with oligomenorrhea and rarely amenorrhea. Anovulation is often associated with irregular dysfunctional uterine bleeding.
US examination of the ovaries is unavoidable and simplest method in the diagnosis of PCOS. Criteria for declaring polycystic ovary according to the latest classification are 12 or more follicles with a diameter of 2-9 mm and ovarian volume greater than 10 ml and it is enough that only one ovary have these characteristics. It is important to emphasize that in puberty and adolescence US PCOS is not specific.
Biochemical analysis includes determining hormonal status: Follicle-stimulating hormone, luteinizing hormone, E2, total testosterone, SHBG, free testosterone, dehydroepiandrostendion sulfate, 17-hydroxyprogesterone androstenedione, the determination of IR (glucose tolerance test), fasting glucose, IR and some dynamic tests are performed exceptionally for the differential diagnosis of PCOS with other endocrine disorders. However, biochemical tests are necessary for girls who are overweight, with pronounced hirsutism or acne resistant to treatment. Furthermore, to adolescents that in the first two years after menarche have amenorrhea/oligomenorrhea or repeated dysfunctional uterine bleeding is necessary to determine the biochemical status. Regardless of that, women with PCOS should be treated and monitored continuously. Treatment of PCOS depends on the patient's age, symptoms and signs of this syndrome and reproductive desires. For this purpose, the hormonal preparations, insulin-sensitizing medicines and surgical treatments are performed.
In adolescents with PCOS treatment is aimed at controlling irregular bleeding, reduce acne and hirsutism and reduction of obesity and IR (risk of endometrial cancer in these women is three times increased). The strongest effect of anti-androgens has oral hormonal contraceptives. From other hormone therapy for PCOS should be noted neandrogene progestogens that are given because of their opposed action to estrogens primarily to protect the endometrium. Surgical treatment of PCOS is laparoscopic ovarian electrocoagulation (drilling), which destroys fat ovarian stroma.
Diagnosis is based on the history of irregular bleeding and more abundant bleeding, the existence of secondary anemia that accompanies it and normal palpation findings of patient's genital organs, but if this is the result of anatomical changes, then we cannot talk about these types of bleeding. Therefore, it is essential that before diagnosis are excluded other possible causes of irregular bleeding, which is usually done by combined rectal-vaginal examination. Also, examination of peripheral blood and bone marrow needle aspiration is needed to exclude blood diseases. Diagnostic curettage is performed in the extreme conditions and can be therapeutic and most often the material is sent for histological evaluation. Treatment of juvenile bleeding should first stop the bleeding, compensate for lost blood and fluid and improve the general condition. Among drugs are given uterotonic agents and preparations of the anterior pituitary lobe or synthetic preparations with identical actions, together with calcium, vitamin K and nicotinic acid amide.
Treatment of metrorrhagia in the generative period is implemented by giving progesterone at a dose of 25 mg and in the second half of treatment, during the 3 months. If the therapy begins at the stage of irregular bleeding, then progesterone provides 2 or 3 days to regulate the bleeding. Patients with atrophic endometrium and demonstrated lack of estrogen are treated by alternately application of estrogen and progesterone in 3-4 cycles.
DISCUSSION
Quality and successful management of gynecological diseases cannot be ensured without following certain guidelines recommended by experts in this field. Good clinical practice concept that is applied in the world puts in front: (a) Patient education, (b) counseling patients about healthy life-style, (c) conducting screening. Necessary and advisable is to follow proper quality parameters of provided gynecological care at certain levels of its organization in the health system given in the documents of the World Health Organization and the comparable results (incidence, morbidity, mortality) in the countries that did so in relation to the countries that were not able to implement it. Reasons for the latter may be low socioeconomic status, lack of education of patients by their physicians about the importance of regular gynecological examinations, etc.
Although in recent years, the incidence of cervical cancer has decreased there is still a high incidence and high mortality among women with low socio-economic status, which is the result of a lack of screening or irregular screening.
Numerous studies have shown that the rate of morbidity and mortality are significantly reduced where there is organized screening. Selected family doctor plays an important role in regular referring of woman to systematic gynecological examinations according to the recommendations that are in the National Guide for the prevention of malignant diseases. Furthermore, he/she has a duty to educate women about the risk factors for malignant diseases, as well as preventive measures to prevent their occurrence. In developed countries where screening is regularly conducted the number of women suffering and dying from cervical cancer has been reduced by 80%. The disease often affects women from lower socio-economic class, with a lower possibility of regular health care. In developed countries, mortality was significantly reduced to about 25%, thanks to early detection and modern therapy.
Hence, it is very important to perform comparisons on the basis of the results obtained from the rich countries to the results from poor countries because the incidence of diseases and mortality rates are significantly higher in poor countries than in rich ones. Poorer countries due to lack of funds do not have good technological methods for screening that will allow the disease detection at an early stage and thus prevent complications, which does not even have close PHC centers and specialist consultation services in their place of residence. Not only the financial aspect is cited as an important factor in health for an increase of morbidity and mortality in a group of gynecological diseases, but there are also important other factors, such as: (Un) healthy environment, lack of clean drinking water, inhumane living conditions, which may lead to the occurrence of a number of infections than in rich countries with higher gross national income of the population in which they can provide a means for personal hygiene. Richer countries have the resources to invest in a variety of methods of prevention, such as the development of educational advertisements, posters and brochures for health promotion and education of the population at all levels: Local communities, schools, companies, medical facilities, etc.
It is also very important to stress the importance of sexual education, especially in schools, which can contribute to reduced incidence of sexually transmitted diseases, especially human immunodeficiency virus (HIV) and the HPV which is considered as important in the development of dysplasia with consequential occurrence of cervical cancer.
Because of the high incidence of cervical cancer it is necessary to organize a screening examination of women. Numerous studies have shown that the rate of morbidity and mortality significantly reduced where there is organized screening. Selected family doctor has a very important role in referring to regular systematic gynecological examinations according to the recommendations that are in the National Guide for the prevention of malignant diseases. Furthermore, the physician has a duty to educate women about the risk factors for malignant diseases, as well as preventive measures. Cervical cancer is an ideal disease for screening because it typically has a long preclinical phase, which allows early detection. Taking a cervical smear and staining by method of Papanikolaou is the best method available to reduce the morbidity and mortality of invasive cancer of the uterus cervix. According to the recommendations the screening should begin as early as at the age of 18 years (or from the moment of sexual relations start) because the age of this disease occurrence moves toward the younger generations. Control Papa test should be done once a year and if two consecutive findings are negative then is recommended control every 2 years. Any patient with persistent or progressive cervical intraepithelial neoplasia regardless of age, according to new studies and each patient aged over 30 years should do HPV deoxyribonucleic acid screening test. Regular and proper implementation of the screening program is also the best way to prevent the appearance of clinical symptoms.
Outside the organized screening program, women should be advised on the following:
It is necessary to improve information and increase awareness about the importance of women about the possibilities and the importance of preventive measures and examinations
Mammography is recommended to start at age of 40 year and continue each year until a woman is in good health
Clinical breast examination as part of a periodic health examination every 3 years for women aged 20-40 years, then every year
Women should know how their breasts look normal and that any changes immediately and without delay leads them to the doctor. Self-examination is an option (according to the will of women) and it should begin at the age of 20 years
Women at increased risk (family history, genetic predisposition, previous cancer in the other breast) should talk with their doctor about the possible consequences of the irregular examinations.
Screening as an organized program of secondary prevention for breast cancer usually starts at the age of 45 in women who do not belong to the risk group of the first category and in high-risk even earlier, i.e. 40 years.
It is needed to raise self-awareness of women by education from physicians and polyvalent nurses.
It is necessary to create awareness among medical staff in PHC, particularly family doctor about the possibilities, needs and the importance of early detection of breast cancer.
It is necessary to provide human and material resources to carry out the screening, especially mammography machines, radiology technicians and radiologists trained to perform quality interpretation of the findings.
Establish centers at the secondary or tertiary health-care level for the setting of explicit diagnosis and treatment of breast cancer.
Create conditions for exact and timely histopathological examination of biopsy material at the secondary or tertiary health-care level.
A particular problem is the issue of taboo in our society about sexuality, which is of a systemic character and it should be a deal with by the multi-disciplinary teams in health care and education (educators at all levels of education, teachers, psychologists, sociologists, family doctors, gynecologists, sexologists etc.). Our society is patriarchal and this issue is becoming a burning issue. The system should ensure the introduction of the health education in primary and secondary schools in the framework of which the students, as age-appropriate, are informed about sexually transmitted diseases, their prevention, diagnosis, treatment. The particular attention should be paid to the prevention of teenage pregnancies and abortions, which is increasingly prevalent among younger people with a tendency to move toward even younger ages. Of course, the parents had to be maximally involved in the work of these teams. A particular problem is the social network that indiscriminately provides information to young people about sexuality, very often wrong and non-selective, even to say in an inappropriate way that should be banned by the relevant institutions. Unwanted pregnancy, HIV infection, genital organs, especially sexually transmitted disease are difficult to manage, especially their early discovering and then treatment, which has resulted in increasing incidence of unwanted pregnancies, abortions and infertility in women, or in women of childbearing age. Family doctors and gynecologists here can play a key role, especially in the field of health promotion.
CONCLUSION
Prevention of diseases in gynecology can be improved by better understanding of health promotion and management of diseases. The importance of family medicine physicians and their team is remarkable in the prevention of gynecological diseases. Girls and women in their office should find advice and a create way to educate them about the importance of personal hygiene, life-style, diet and of course, sexual behavior and the use of antibiotics that lead to the disruption of normal vaginal flora and fungal infections. They need to provide sufficient information, either orally or by educational brochures about the origin, prevention and the ultimate treatment of these infections. To girls and women should be emphasized that by unprotected sex can infection can be transmitted. Essential is also the education of those people who do not have permanent sexual partner in the proper use of condoms and before this would be better the importance of highlighting the hazards of promiscuity.
In the existing clinical guidelines for PCOS is emphasized the need for early detection of the syndrome. During compulsory education all school children are available for preventive activities and medical examinations, which provide great opportunities for early detection and improving the health of children and young people and in the long-term of the whole population. It is not negligible also the economic effect. School medicine has prepared guidelines with instructions and set of activities and measures. Very often from the school, doctor and nurse while working on counseling the students and their parents seeking clarification on the recommended procedures and treatment.
However, the first measure is a healthy life-style and weight reduction of obese patients. Thus, the weight loss in combination with other therapeutic procedures achieves optimal therapeutic effects, prevents long-term adverse and harmful effects and provides high-quality life. Early detection and timely treatment can, not only reduce and eliminate these symptoms and clinical manifestations, but also prevent the development of diabetes and cardiovascular diseases and some form of cancers later in life.
Family doctor in the health-care system should be oriented to a number of measures and activities in order to adequately and well manage gynecological disease in practice as follows:
Know that the regular and proper implementation of screening programs at the same time is the best prevention of the occurrence of clinical forms of the disease
Emphasize that the increase in the number of patients in the early stages of the disease (based on records and hospital records) is very important
Encourage the improvement of treatment (based on hospital records and records of mortality)
Highlight the importance of self-examination, to the extent that the woman be aware of her breasts and to think of them, to be properly informed
Insist on teaching women, as well as the professional staff in primary and family health-care, that breast cancer is very serious disease, that early detection is important for successful treatment and that the methods by which breast cancer is detected is simple and painless
Counseling, education and guidance to women through a PHC about the importance of keeping proper daily personal hygiene should be the primary task of the family medicine teams
Counseling and education of women, especially young women of the dangers from frequent change of sexual partners and condom use should be encouraged by doctors
Infection control, because they are a serious social and public health problem, especially in women who plan their families and pregnant women, should also be stimulated
Education of women about healthy life-style and proper nutrition, with weight reduction in obese patients is one of the main tasks of the family medicine teams
Emphasize the need for all school children to undergo preventive activities and medical examinations, which provides great opportunities for early detection and improving the health of children and young people and in the long-term of the whole population
Emphasize the need for the development of guidelines with instructions and procedures for the management of gynecological diseases.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Mladenović D, Mladenović-Bogdanović Z, Mladenović-Mihailović A. Ginaecology and Obstretics. Belgrade, Serbia: Zavod za Udzbenike Beograd/Book's Publishing; 2008. [Google Scholar]
- 2.Šimunić V. Gineaecology. Zagreb, Croatia: Naklada Ljevak; 2001. i sar. [Google Scholar]
- 3.Ćorušić A, Babić D, Šamija M, Šobat H. Ginaecological Oncology. Zagreb, Croatia: Medicinska Naklada; 2005. [Google Scholar]
- 4.Basic E, Kozaric H, Kozaric M, Suko A. Ovarial cancer incidence and surgical approach to treatment at clinic for ginaecology and obstretics of clinical center of University of Sarajevo in 2009. Mater Sociomed. 2010;22:101–4. [Google Scholar]
- 5.Basic E, Kozaric H, Kozaric M, Suko A. Conization as treatment of choice for precancerous changes and university cervical cancer at the Department of Obstetrics and Gynecology of Clinical Center of Sarajevo University in 2009. Med Arh. 2010;64:171–4. [PubMed] [Google Scholar]
- 6.Kurjak A, Predojevic M, Stanojevic M, Salihagic Kadic A, Miskovic B, Badrelden A, et al. Intrauterine growth restriction and cerebral palsy. Acta Inform Med. 2010;18:64–82. doi: 10.5455/aim.2010.18.64-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Fejdic J, Djurovic D, Gotovac N, Hrgovic Z. Criteria and procedures for breast cancerring surgery. Acta Inform Med. 2011;19:114–7. doi: 10.5455/AIM.2013.21.16-19. [DOI] [PMC free article] [PubMed] [Google Scholar]