

Abstract
Background:
Assessing growth is a useful tool for defining health and nutritional status of children. The objective of this study was to construct growth reference curves of Iranian infants and children (0-6 years old) and compare them with previous and international references.
Methods:
Weight, height or length of 2107 Iranian infants and children aged 0-6 years old were measured using a cross-sectional survey in Tehran in 2010. Standard smooth reference curves for Iranian population were constructed and compared to multinational World Health Organization 2006 reference standards as well as a previous study from two decades ago.
Results:
Growth index references for Iranian girls are increased in compare to data from two decades ago and are approximately close to the international references. In boys; however, the increment was considerably large as it passed the international references. Not only the values for indexes was changed during two decades, but also the age at adiposity rebound came near the age of 3, which is an important risk factor for later obesity.
Conclusions:
During two decades, growth indexes of Iranian children raised noticeable. Risk factors for later obesity are now apparent and demand immediate policy formulations. In addition, reference curves presented in this paper can be used as a diagnostic tool for monitoring growth of Iranian children.
Keywords: Body mass index, children, height, infant, weight
INTRODUCTION
Changes and trends in growth indexes have been researched and reported in many studies in the recent decades. Especially, a positive weight and height trend in Iranian children and adolescents 2-18 year old was shown in the last decade of 20th century by Hosseini et al.[1] However, the latest nationwide survey assessed the growth indexes percentiles of 2-18 year old Iranian children, has been conducted in 1997.[2] Since then, although several studies have been conducted in Iran, all of them were regional representative and did not stand for the whole nation.
In the year of 2000, Center of Disease Control (CDC) presented growth charts for the United States.[3,4] Six years later, in the year of 2006, World Health Organization (WHO) released the result of an international multi-center study, which was implemented between 1997 and 2003 as WHO child growth standards.[5] The WHO study data is gathered from six countries (United States, Norway, Brazil, India, Oman, and Ghana), which is claimed to be representative for the whole world children.[6] Prior to 2004, 99 (68%) countries adopted the pervious National Center for Health Statistics or WHO references and 25 (17%) used their local standards.[7] However, currently, WHO 2006 growth standards are the main references in many countries, including Iran, to assess the growth status of the children.
Under or over nutrition is diagnosed using the growth standards. This emphasizes the importance of growth references and makes the assessment of newly updated growth references crucial. Many studies in both developed[8,9] and developing[10,11,12,13] countries have compared the international references with their own local data and suggest the use of local growth reference rather than international references such as WHO 2006 or CDC 2000. In addition, two studies[14,15] have been recently conducted in two region of Iran, which showed the deviation of Iranian growth standards to the global ones.
Previous studies have shown that Iranian standard reference values of growth was lower than international references;[16] therefore, in this paper, in order to assess the present status of growth of Iranian infants and children, anthropometric indexes of Tehran's infants and children have been studied as it has been shown to be representative for the whole country.[17] Furthermore, to evaluate the efficiency of using such global standard references in Iranian population, the differences between current WHO growth standards and local charts have been addressed in this paper.
METHODS
Subjects
Weight and standing height or recumbent length of 2107 infants and children were measured using a cross-sectional study. All of these infants and children were younger than 6 years with healthy condition that was confirmed by trained physicians. Having chronic, growth, or malnutrition disorders were the exclusion criteria.
Sampling procedure
Infants (2 years old and younger) were sampled from health centers and children (older than 2 years) were sampled from kindergartens, using 2-stage cluster sampling method. Each municipality district of Tehran considered as a cluster for the first stage and for the second stage, kindergartens or health centers were referred as clusters. To assess the infants’ weight with 50 g precision, SECA baby scale model 725 (Hamburg, Germany), was used, and their recumbent length to the nearest mm was measured using SECA mobile measuring mat model 210, (Hamburg, Germany). Weight of children (older than 2 years old) was measured with 500 g precision using SECA scale model 760, (Hamburg, Germany), and to assess their standing height to the nearest mm, SECA mechanical measuring tape model 206 (Hamburg, Germany) was used.
Construction of growth standards
For constructing growth standards, a similar method to that applied by WHO was used in order to have comparable results. For constructing weight for age standards, a model was applied to the whole data. However, to construct height/length for age standards, at first 0.7 cm was added to the heights of children older than 2 years. Then a model fitted the data, and finally, 0.7 cm subtracted from fitted model for ages older than 2 years.
For constructing body mass index (BMI) for age standards, for ages equal to and younger than 2 years, first, the original data from 1 to 30 months were used by adding 0.7 cm to the height of children older than 2 years, and then a model applied to find a smooth curve and fitted values for ages from 1 to 24 months were held. Similarly, original data from 18 to 71 months were used by subtracting 0.7 from the height of infants and children with age equal to or younger than 2 years and after fitting a model, only fitted values for ages older than 2 years were recorded.
Statistical analysis
Data were entered into Stata version 11.0 (College Station, TX: Stata Corporation) software and analyzed using it. In order to construct models, fractional polynomial method[18] was used by means of fracpoly procedure. At first, all measurements were transformed logarithmic to follow a normal distribution and the mean value of transformed data for ages was modeled. In addition, age-specific standard deviations were estimated by another fractional polynomial model, which regressed absolute values of residuals in the first model. Predicted values of the second model were multiplied by the square root of π/2 and considered as the standard deviation for each age.[19] Finally, fitted means and age-specific standard deviations were used by back transformation to obtain smooth percentiles for measurements.
All models were sex specified. Goodness of fit for each model was estimated using grid χ2 tests criterion. As the weight were modeled once for the whole range, only one χ2 is reported for these model; however, two χ2 statistics were obtained for height and BMI models, which covers ages younger and older than 2 years. It is noteworthy to say that we did not have any subject for ages equal to 72 months and also there were no boys with age of 17 months in our model. Hence, the predicted values for these ages were estimated using interpolation or extrapolation.
RESULTS
Weight and height/length of 2107 infants and children aged 1 month to 6 years old were measured in 2010. Among, 1152 (54.7%) were male and 955 (45.3%) were female. Smooth standard references by age (years) and sex for weight, height or length, and BMI are given in Table 1. This table shows that the difference between girls and boys standards is more apparent for ages of 5 and 6 years and is slight for the first month of age. Grid tests for goodness of fit for the smooth weight (χ2girls = 0.2, P > 0.999; χ2boys = 0.4, P > 0.999), height (χ2girls, 0-2 years = 5.3, P = 0.627; χ2girls, 2-6 years = 5.1, P = 0.652; χ2boys, 0-2 years = 11.0, P = 0.140; χ2boys, 2-6 years = 10.9, P = 0.143), and BMI (χ2 girls, 0-2 years = 4.8, P = 0.688; χ2girls, 2-6 years = 7.0, P = 0.432; χ2boys, 0-2 years = 6.3, P = 0.507; χ2boys, 2-6 years = 6.7, P = 0.465) curves were not significant. It confirms the goodness of fit of all growth curves to the data.
Table 1.
Smooth standard reference values for weight, height, and BMI of Iranian children by age and sex
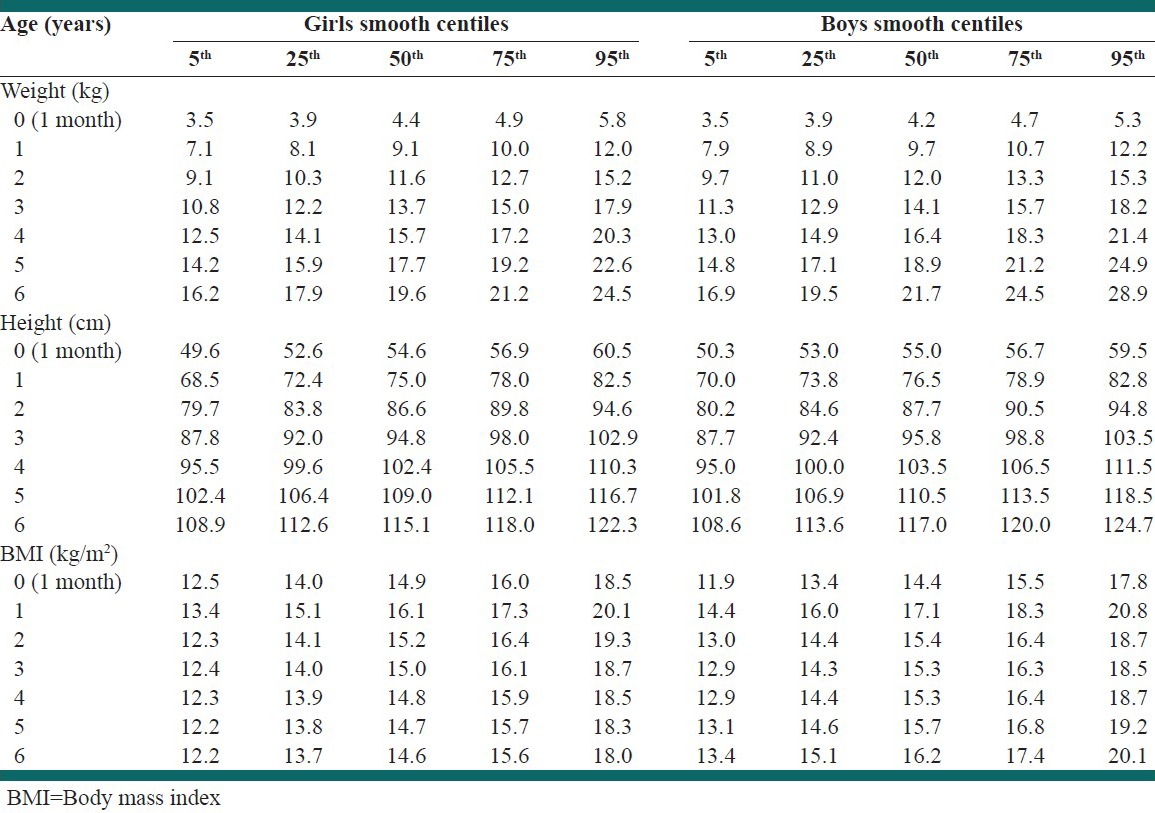
Figure 1 shows the standard values for weight of Iranian infants and children as well as the WHO standard references. Although, the lowest and median percentiles of weight for Iranian population seem to be close to WHO standards, higher centiles tend to diverge in boys for ages after 4 years. Annual increase of weight for Iranian girls and boys were on average 2.2 kg and 2.4 kg, respectively.
Figure 1.
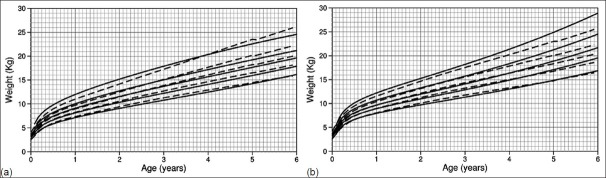
Weight centiles (5, 25, 50, 75, 95) of Iranian (a) girls and (b) boys (solid lines) compared to World Health Organization standards (dashed lines)
Standing height or recumbent length of Iranian infants and children is compared to WHO standards in Figure 2. A slight difference is apparent for 5th and 95th centiles between Iranian population and WHO curves; however, in total, it was not remarkable. For height, annual increment was 8.9 cm for both Iranian boys and girls.
Figure 2.
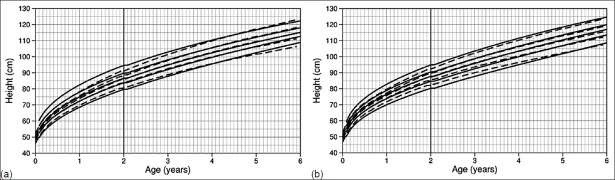
Height centiles (5, 25, 50, 75, 95) of Iranian (a) girls and (b) boys (solid lines) compared to World Health Organization standards (dashed lines)
A considerable difference between BMI of Iranian infants and children and WHO standards is shown in Figure 3. Furthermore, the shape of BMI curves for Iranian boys and girls were not similar. In addition, it is visible that Adiposity Rebound (ADR); increase point in BMI after reaching the lowest point) for Iranian girls occur after the 6 years, but, it happens about the 3rd year for boys.
Figure 3.
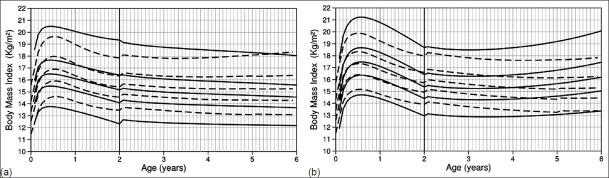
Body mass index centiles (5, 25, 50, 75, 95) of Iranian (a) girls and (b) boys (solid lines) compared to World Health Organization standards (dashed lines)
DISCUSSION
The most interesting and important result in our work was the age at adiposity rebound for Iranian boys. Early ADR is suggested to be and an important risk factor for the adulthood obesity.[20] Previous study[16] has shown that ADR for both girls and boys of Iranian population was occurred about the age of 6 years, about two decades ago. Though in our analysis the age of ADR for girls showed to be after the age of 6 years, for boys it was shown that it will occur about the age of 3 years old.
Some studies have compared the BMI pattern for obese children with reference populations. In these studies, mean age at ADR showed to be about 3 for obese children and about 6 for the reference population.[21] Their results along with ours emphasize the importance of growth monitoring for Iranian boys and formulating policies to take appropriate preventive measures.
Another interesting result of our study was the change of BMI levels for Iranian boys after a decade. Hosseini et al.[16] compared the BMI levels of Iranian children and adolescents (2-18 years) to US population reference about two decades ago. Based on their results, BMI levels of Iranian children were considerably lower than US population for both boys and girls. Although, they did not investigate the levels for children younger than 2 years and also it was not compared to WHO reference standards, comparing their results together with ours implies the increment of levels for both Iranian girls and boys, which tends to be close to international references for girls, and even passes the reference standards for boys.
Emdadi et al.[15] have conducted the only recent similar work in North East in Iran, which is in contrast with ours. Although this study is recently carried out and has more subjects than ours, the different methodology is resulted in different shape and values for BMI standard references. In their study, the data from infants and children younger than 2 years is not measured. The methodology for constructing BMI standards suggested by WHO,[6] uses the data from children aged 18 months and older to obtain reference values for children older than 2 years. Having these data will play an important role in forming the shape of BMI reference curves.
BMI over 30 and 25 is defined as obesity and overweight for adults, respectively. However, there are no such criteria for children. Therefore, the extreme age and sex-specific centiles of BMI of national or international references are considered for diagnosing obesity or overweight in children.[22] Hence, in addition to above results, the reported centiles for BMI can be used for monitoring the nutritional and growth status of Iranian children.
Findings of a recent school-based nationwide study[23] showed that 15.5% of Iranian girls and 19.9% of Iranian boys aged 10-18 years were overweight or obese. On this study, overweight and obese were defined as having age and sex-specific BMI greater than +1 and +2 z-score based on WHO growth curves, respectively. Since near 15.9% of children of a normal population that follows WHO growth standards are overweight or obese, this study is consistent with ours, which shows that growth of Iranian girl are similar to international standards and BMI of Iranian boys are higher than WHO growth references.
In view of the fact that the BMI of Iranian children have increased during the recent years and adulthood obesity risk factor is now apparent, it is suggested to take the preventive measures such as the United States Preventive Services Task Force recommendations since it is shown that the prevalence of high BMI did not increase among children in United States during the year 2003-2006.[24]
Many studies have reported the growth of school-aged children, however, up to now no research has conducted the growth indexes of Iranian infants and children younger than 2 years. Beside this advantage of this study, we tried to have similar methodology with WHO to have comparable results; However, our study lacks from having longitudinal data. In addition, finding breast-fed children similar to WHO subjects was not easy to consider as an inclusion criterion. However, we measured the weight and height of healthy children to have similar subjects.
CONCLUSIONS
During two decades, BMI levels of Iranian infants and children increased noticeably and even BMI levels of Iranian boys currently passes the international references. Furthermore, age at adiposity rebound for Iranian boys was about 3 years, which is an important risk factor for obesity for later ages. In addition, smoothed centiles presented in this paper can be used as a tool for diagnosing obese infants and children of Iranian population.
Footnotes
Source of Support: This work was supported by Tehran University of Medical Sciences and Health Services [17131]
Conflict of Interest: None declared
REFERENCES
- 1.Hosseini M, Taslimi Sh, Dinarvand P, Jones ME, Mohammad K. Trends in weights, heights, BMI and comparison of their differences in urban and rural areas for Iranian children and adolescents 2-18-year-old between 1990-1991 and 1999. Child Care Health Dev. 2010;36:858–67. doi: 10.1111/j.1365-2214.2010.01140.x. [DOI] [PubMed] [Google Scholar]
- 2.Hosseini M, Carpenter RG, Mohammad K. Growth charts for Iran. Ann Hum Biol. 1998;25:237–47. doi: 10.1080/03014469800005602. [DOI] [PubMed] [Google Scholar]
- 3.Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R, et al. CDC growth charts: United States. Adv Data. 2000;314:1–27. [PubMed] [Google Scholar]
- 4.Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R, et al. Centers for Disease Control and Prevention 2000 growth charts for the United States: Improvements to the 1977 National Center for Health Statistics version. Pediatrics. 2002;109:45–60. doi: 10.1542/peds.109.1.45. [DOI] [PubMed] [Google Scholar]
- 5.WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr Suppl. 2006;450:76–85. doi: 10.1111/j.1651-2227.2006.tb02378.x. [DOI] [PubMed] [Google Scholar]
- 6.Geneva: World Health Organization; 2006. [Accessed on 11 August 2011]. Group WMGRS. WHO child growth standards: length/height-for-age, weight-for-age, weight-forlength, weight-for-height, and bodymass index-for-age: methods and development. Available from: http://www.who.int/childgrowth/standards/technical_report/en . [Google Scholar]
- 7.de Onis M, Wijnhoven TM, Onyango AW. Worldwide practices in child growth monitoring. J Pediatr. 2004;144:461–5. doi: 10.1016/j.jpeds.2003.12.034. [DOI] [PubMed] [Google Scholar]
- 8.Rao S, Simmer K. World Health Organization growth charts for monitoring the growth of Australian children: Time to begin the debate. J Paediatr Child Health. 2011;48:84–90. doi: 10.1111/j.1440-1754.2011.02214.x. [DOI] [PubMed] [Google Scholar]
- 9.Rosario AS, Schienkiewitz A, Neuhauser H. German height references for children aged 0 to under 18 years compared to WHO and CDC growth charts. Ann Hum Biol. 2011;38:121–30. doi: 10.3109/03014460.2010.521193. [DOI] [PubMed] [Google Scholar]
- 10.Abdulrazzaq YM, Nagelkerke N, Moussa MA. UAE population reference standard charts for body mass index and skinfold thickness, at ages 0-18 years. Int J Food Sci Nutr. 2011;62:692–702. doi: 10.3109/09637486.2011.567978. [DOI] [PubMed] [Google Scholar]
- 11.El Mouzan MI, Foster PJ, Al Herbish AS, Al Salloum AA, Al Omar AA, Qurachi MM, et al. The implications of using the world health organization child growth standards in Saudi Arabia. Nutr Today. 2009;44:62. [Google Scholar]
- 12.Halisdemir N, Colak C, Camurdan AD, Ergocen S, Sahin F, Elhan AH. Body mass index percentile curves for predominantly breastfed children aged 0-2 years from Ankara, Turkey. Bratisl Lek Listy. 2011;112:517–20. [PubMed] [Google Scholar]
- 13.Soliman A, Eldabbagh M, Khalafallah H, Alali M, Elalaily RK. Longitudinal growth of infants in Qatar: Comparison with WHO and CDC growth standards. Indian Pediatr. 2011;48:791–6. doi: 10.1007/s13312-011-0123-9. [DOI] [PubMed] [Google Scholar]
- 14.Heydari ST. Infants’ growth charts in Jahrom, Iran. Iran J Pediatr. 2009;19:25–34. [Google Scholar]
- 15.Emdadi M, Safarian M, Doosti H. Standardized percentile curves of body mass index of northeast Iranian children aged 25 to 60 months. Iran J Pediatr. 2011;21:88–94. [PMC free article] [PubMed] [Google Scholar]
- 16.Hosseini M, Carpenter RG, Mohammad K, Jones ME. Standardized percentile curves of body mass index of Iranian children compared to the US population reference. Int J Obes Relat Metab Disord. 1999;23:783–6. doi: 10.1038/sj.ijo.0800924. [DOI] [PubMed] [Google Scholar]
- 17.Hosseini M, Carpenter RG, Mohammad K. Growth of children in Iran. Ann Hum Biol. 1998;25:249–61. doi: 10.1080/03014469800005612. [DOI] [PubMed] [Google Scholar]
- 18.Royston P, Altman DG. Regression using fractional polynomials of continuous covariates: Parsimonious parametric modelling. Appl Stat. 1994;43:429–67. [Google Scholar]
- 19.Altman DG. Construction of age-related reference centiles using absolute residuals. Stat Med. 1993;12:917–24. doi: 10.1002/sim.4780121003. [DOI] [PubMed] [Google Scholar]
- 20.Williams SM, Goulding A. Early adiposity rebound is an important predictor of later obesity. Obesity (Silver Spring) 2009;17:1310. doi: 10.1038/oby.2009.104. [DOI] [PubMed] [Google Scholar]
- 21.Rolland-Cachera MF, Deheeger M, Maillot M, Bellisle F. Early adiposity rebound: Causes and consequences for obesity in children and adults. Int J Obes (Lond) 2006;30:S11–7. doi: 10.1038/sj.ijo.0803514. [DOI] [PubMed] [Google Scholar]
- 22.Must A, Anderson SE. Body mass index in children and adolescents: Considerations for population-based applications. Int J Obes (Lond) 2006;30:590–4. doi: 10.1038/sj.ijo.0803300. [DOI] [PubMed] [Google Scholar]
- 23.Kelishadi R, Heshmat R, Motlagh ME, Majdzadeh R, Keramatian K, Qorbani M, et al. Methodology and early findings of the third survey of CASPIAN study: A national school-based surveillance of students’ high risk behaviors. Int J Prev Med. 2012;3:394–401. [PMC free article] [PubMed] [Google Scholar]
- 24.Schwandt P. Can we slow down the global increase of adiposity? Int J Prev Med. 2011;2:115–6. [PMC free article] [PubMed] [Google Scholar]