

Abstract
Emotion knowledge in childhood has been shown to predict social functioning and psychological well-being, but relatively little is known about parental factors that influence its development in early childhood. There is some evidence that both parenting behavior and maternal depression are associated with emotion recognition, but previous research has only examined these factors independently. The current study assessed auditory and visual emotion recognition ability among a large sample of preschool children to examine typical emotion recognition skills in children of this age, as well as the independent and interactive effects of maternal and paternal depression and negative parenting (i.e., hostility and intrusiveness). Results indicated that children were most accurate at identifying happy emotional expressions, followed by other basic emotions. The lowest accuracy was observed for neutral expressions. A significant interaction was found between maternal depression and negative parenting behavior, such that children with a maternal history of depression were particularly sensitive to the negative effects of maladaptive parenting behavior on emotion recognition ability. No significant effects were found for paternal depression. These results highlight the importance of examining the effects of multiple interacting factors on children’s emotional development, and provide suggestions for identifying children for targeted preventive interventions.
Keywords: emotion recognition, emotion knowledge, preschool, depression, parenting
The development of emotion knowledge, including the ability to recognize and understand emotions portrayed in facial expressions and non-verbal cues, is essential to the development of socioemotional competence (Izard, 2001). Poor emotion knowledge in childhood and adolescence has been shown to be associated with a number of problematic outcomes, including poor social functioning, attention problems in school, poor academic performance and both internalizing and externalizing symptoms (Denham et al., 2003; Ensor, Spencer, & Hughes, 2011; Fine, Izard, Mostow, Trentacosta, & Ackerman, 2003; Izard et al., 2001; Leppänen & Hietanen, 2001; Trentacosta & Fine, 2010; Trentacosta, Izard, Mostow, & Fine, 2006).
There is evidence that neural systems for processing emotional information are already established at birth, and the ability to discriminate expressions begins to develop in infancy, with continual influence by environmental experiences (Leppänen & Nelson, 2009). Even as early as seven months, infants appear to be able to differentiate some types of emotions and show physiological evidence of discrimination between fearful and happy faces (Caron, Caron, & Myers, 1982; Peltola, Leppänen, & Hietanen, 2011). The identification of affective expressions through combined auditory and visual stimuli may begin to develop even earlier, with four-month-old infants displaying evidence of discrimination of emotion expression in audiovisual stimuli, followed by the ability to discriminate purely auditory expressions at five months (Flom & Bahrick, 2007).
Despite very early discrimination of emotional expressions, the ability to accurately label emotions continues to develop throughout childhood and adolescence, with recognition of some types of emotional expressions developing earlier than others. A study of five-, seven-, nine-, and eleven-year-old children and adults indicated that the ability to recognize emotional faces improves with age, though accuracy for specific types of faces varies in the rate of development. For example, happy and sad expressions were recognized at age five with similar accuracy to adults, but recognition of fear, anger, disgust and neutral faces appeared to develop more slowly (Durand, Gallay, Seigneuric, Robichon, & Baudouin, 2007). Other studies also suggest that recognition of happiness develops early, followed by other relatively basic emotions (e.g., sadness, anger) and then more complex emotions (e.g., surprise, shame, contempt) (Ale, Chorney, Brice, & Morris, 2010; Broeren, Muris, Bouwmeester, Field, & Voerman, 2011; MacDonald, Kirkpatrick, & Sullivan, 1996). In addition, in a free labeling task, Widen and Russell (2003) found that around the age of three, children tend to use one or two labels to broadly describe expressions, with the use of happy developing first followed by angry and sad. The use of labels such as scared, surprised and disgusted developed closer to age five and appeared to be less accessible to children than other emotion expressions. Taken together, previous research suggests that although emotion recognition continues to develop throughout childhood and adolescence, by preschool age, children are able to recognize and label at least some types of emotional expressions.
Though the development of emotion knowledge is clearly important in predicting child outcomes (e.g., Denham et al., 2003; Ensor et al., 2011; Fine et al., 2003; Izard et al., 2001; Leppänen & Hietanen, 2001; Trentacosta & Fine, 2010; Trentacosta et al., 2006), relatively little is known about factors that predict the development of emotion recognition skills in early childhood. There is some evidence that parenting has a significant effect on the development of emotion knowledge. A number of studies indicate that child maltreatment influences emotion understanding, with physically abused children showing enhanced recognition of angry faces and neglected children showing increased difficulty distinguishing emotional faces compared to both controls and physically abused children (Pollak, Cicchetti, Hornung, & Reed, 2000; Pollak, Messner, Kistler, & Cohn, 2009; Pollak & Sinha, 2002). In addition, children who were institutionalized at birth and consequently experienced early emotional neglect, perform poorer on tasks involving recognizing emotional faces and matching emotions to situations (Fries & Pollak, 2004). Less extreme parenting behavior also may influence the development of emotion understanding. For example, parents’ supportive reactions to children’s negative emotions appear to be positively related to emotion understanding in children (McElwain, Halberstadt, & Volling, 2007). In addition, cross-sectional and longitudinal research suggests that more discussion of feelings and mental states by parents during early childhood predicts increased emotion understanding in children (Doan & Wang, 2010; Dunn, Brown, & Beardsall, 1991; Taumoepeau & Ruffman, 2006, 2008).
In addition, some previous research has linked parental depression to impairments in emotion recognition skills in offspring. For example, one study using a task in which faces morphed from neutral to emotional expressions found that girls of mothers with a history of depression required greater intensities of sadness to correctly identify sad faces and made more errors when identifying angry faces compared to girls with no maternal history of depression (Joormann, Gilbert, & Gotlib, 2010). There is some evidence that adults with depression perform poorer than controls on tasks requiring the identification of facial emotion expressions (Feinberg, Rifkin, Schaffer, & Walker, 1986; Persad & Polivy, 1993; Rubinow & Post, 1992), thus it is possible that these impairments influence depressed parents ability to teach these skills to their children or that genetic factors predispose children of depressed parents to similar impairments. In addition, there is evidence that compared to nondepressed mothers, depressed mothers display abnormal affective behavior in interacting with their infants and that infants as young as three months old are able to detect changes in the affect cues of their mothers (Cohn & Tronick, 1983; Downey & Coyne, 1990; Weinberg & Tronick, 1998). Importantly, not all depressed mothers display significant impairments in their interactions with their infants; some show relatively typical, positive interactions (Weinberg & Tronick, 1998). This suggests that depression in parents may increase risk of abnormal emotional development in children, but does not necessarily predict such outcomes on its own. Consistent with this possibility, a recent study found that maternal depression predicted emotion recognition deficits only in combination with genetic risk. Jacobs et al. (2011) found an interaction between 5HTTLPR genotype and maternal depression, such that adolescents of depressed mothers with the low expressing genotype made the greatest number of errors when classifying emotional faces.
It is possible that the link between negative parenting and emotion recognition deficits in offspring may be moderated by parental depression. That is, the effects of negative parenting may be particularly strong among children who are at risk for emotion recognition deficits due to a parental history of depression. We are aware of only one study that examined the effects of both maternal depressive symptoms and maladaptive parenting on emotion knowledge in children. In a sample of four-year-olds, Bennett, Bendersky, and Lewis (2005) reported that neither variable exhibited a significant unique association. However, this study did not examine the interaction between maternal depression and parenting; hence, it is unclear if these variables have synergistic effects on children’s emotion knowledge.
Studies of emotion recognition among offspring of depressed parents have focused on maternal depression; thus, the ways in which paternal depression may influence emotion recognition in early childhood remain unclear. Maternal depression may have stronger effects on some offspring outcomes, compared to paternal depression. For example, the association between paternal depression and offspring psychopathology in childhood is weaker than the association with maternal depression (Connell & Goodman, 2002). Consistent with this, previous research indicates that children of depressed mothers, but not depressed fathers, show reduced neural reactivity to emotional faces (Kujawa, Hajcak, Torpey, Kim, & Klein, 2012). Nonetheless, it is possible that paternal depression also influences development of emotion knowledge.
The current study examined emotion recognition ability as measured by three tasks (one auditory, two visual) among a large sample of three-year-old children. The first objective was to describe typical emotion recognition abilities in three-year-old children by assessing accuracy across tasks and type of emotional expression. The second objective was to examine the effects of maternal and paternal histories of depression and negative parenting behavior (i.e., parental hostility and intrusiveness) on emotion recognition. We first examined associations between child characteristics and emotion recognition to determine whether parental depression and negative parenting predict these skills beyond child characteristics that have been previously established. We hypothesized that maternal depression and negative parenting would interact such that the detrimental effect of negative parenting would be particularly strong among children with a history of maternal depression. As little work has examined effects of paternal depression on emotion recognition, these analyses were exploratory, though we hypothesized that a similar interaction between paternal depression and negative parenting may be observed. We also examined whether effects were specific to parental depression by controlling for parental anxiety and substance use disorders.
Methods
Participants
Participants were part of a larger study (N = 559) of children recruited through commercial mailing lists. Three-year-old children with no significant medical problems or developmental disabilities and at least one English-speaking biological parent were eligible. A total of 511 children participated in the emotion recognition battery; however, data from 35 children were unusable because the child failed to respond to at least one item on each task. In most of these cases, the child refused to continue to participate; however, in some cases the experimenter discontinued testing because the child was unable to complete the task (e.g., one child showed noticeable speech delays that limited verbal responses). Thus, data from 476 children were included in the overall analyses. For analyses of child and parent characteristics, data from 458 children were included. Measures of child internalizing and externalizing symptoms were missing for three children, three children were missing data on receptive vocabulary (see below), parental diagnostic data were unavailable for eight children, and four children were excluded for parental history of bipolar disorder.
The mean age of the children included in the overall analysis was 3.66 (SD = 0.29) years. With regard to racial/ethnic distribution, 86.3% of participants were Caucasian, 1.2% were African American, 9.5% were Hispanic, 1.9% were Asian American, and 1.1% were from other ethnic backgrounds. The majority of children (95.8%) lived with both biological parents. The sample was primarily middle-class, with 109 families falling into social class I, 207 in class II, 127 in class III, 28 in class IV and 5 in class V according to Hollingshead’s Four Factor Index of Social Status (Hollinghead, 1975).
Measures
Emotional Listening Task
To assess ability to identify affect in vocal tone, an affect listening task based on the Florida Affect Battery was administered (Bowers, Blonder, & Heilman, 1991). A set of three happy, sad, and neutral schematic faces were placed in front of the children. The experimenter informed the child that the task would be to choose which picture looks like the way the adult male or female voice on the tape sounds. Participants first completed six practice trials before beginning the nine trials that made up the task. For each trial, the experimenter played a single sentence on the tape and then asked the child whether the voice was happy, okay or sad, while pointing to the respective schematic faces. The practice block consisted of two happy sentences, two neutral sentences, and two sad sentences. Each sentence was congruent, as the content of the sentence corresponded to voice tone (e.g., “I won a prize” in a happy tone). After each response, the experimenter told the child the correct response and provided an explanation. For the test block, the child was again asked to respond to how the voice sounded, but no feedback was given regarding whether or not the response was correct. This block consisted of three happy trials, three sad trials, and three neutral trials. All sentences had neutral content (e.g., “His shoes are in the closet”), requiring the child to derive the answer from the tone of the voice rather than the content.
Emotion Labeling Task
The picture labeling task was based on the Emotion Labeling Task of the Facial Affect Comprehension Evaluation developed for preschoolers by Mrakotsky (2001). A total of 18 pictures of adult and child faces with different expressions were used for the task: three pictures depicted happy expressions, four sad, two angry, three scared, two surprised, two disgusted and two ashamed. The experimenter verbally provided the child with a list of possible feelings (happy, sad, mad, scared, surprised, yucky, ashamed/guilty) and described the meaning of each (e.g., “Ashamed is when you did something wrong and your mommy yells at you, you feel ashamed”). Each picture was then presented to the child and he/she was asked to label each one with an emotion word. After each set of 6 pictures, the experimenter repeated the response options, though the meaning of each word was not repeated. No feedback on incorrect trials was provided for this task.
Emotion Learning Task
A second picture labeling task was administered to evaluate whether children are able to identify affect when corrective feedback is provided. This task required participants to label emotional expressions for one child. Images of two children were available (one male, one female) with fearful, surprised, sad, happy, angry and neutral expressions for each (Camras et al., 1990). Each participant viewed only the set of images that corresponded to his/her own gender. The task was administered in three blocks. At the start of the first block, all six emotional pictures for a single actor were placed in front of the child. The experimenter pointed to the images one at a time and asked “How do you think he/she is feeling here?” During the first trial, correct responses were confirmed (e.g., “Yes! She is feeling angry”), and incorrect responses were corrected along with an explanation (e.g., “I think she is angry here. See how her mouth looks. She looks mad. Maybe she is mad because she was playing with a toy and another child took it way.”). Following completion of the first trial, the same set of pictures was shuffled and organized in front of the child. Again, the experimenter pointed to each image and asked the child how the actor was feeling. For the second trial, incorrect responses were corrected but without an explanation (e.g., “I think she is feeling angry”). For the third trial, the same set of pictures was shuffled and placed in front of the child. The experimenter pointed to each image and asked how the actor was feeling, but no correction was offered for incorrect trials. Average scores on all three trials were included in analyses. Due to the open-ended nature of the prompts for this task, guidelines were developed to determine acceptable responses and when the experimenter should query the response. For example, acceptable responses to fearful faces included “scared,” “nervous,” and “worried,” while responses of “bad” or “not good” were queried for an acceptable response. For neutral faces, responses of “okay,” “nothing,” “normal” or “neutral” were acceptable.
Receptive Vocabulary
To control for variability in children’s verbal ability, the Peabody Picture Vocabulary Test-III (PPVT; L. Dunn & Dunn, 1997) was administered. The PPVT is a widely used measure of receptive verbal ability. It is highly reliable, with an internal consistency of .95 and test-retest reliability of .92, and is highly correlated with a number of other measures of verbal ability (Dunn & Dunn, 1997). Standardized PPVT scores were used for all analyses.
Child Internalizing & Externalizing Symptoms
To control for child symptoms of psychopathology, the Child Behavior Checklist 1½–5 (CBCL; Achenbach & Recorla, 2000) was administered to one parent. The CBCL is a 99-item parent-report checklist assessing emotional and behavioral problems in 1½ to 5-year-old children. The CBCL was completed by 434 mothers and 24 fathers. Analyses focused on the internalizing problem scale, which includes 36 symptoms of internalizing disorders, and the externalizing problem scale, which includes 24 symptoms of externalizing disorders.
Parental Depression
Biological mothers and fathers were interviewed using the Structured Clinical Interview for DSM-IV non-patient version (First, Spitzer, Gibbon, & Williams, 1996). The SCID is the most widely used semi-structured diagnostic interview and has acceptable levels of interrater reliability and procedural validity (Williams, Gibbon, First, & Spitzer, 1992). Interviews were conducted by telephone, which generally yields comparable results to face-to-face interviews (Rohde, Lewinsohn, & Seeley, 1997; Sobin, Weissman, Goldstein, & Adams, 1993). Two Masters-level raters conducted the diagnostic interviews. A second rater derived independent diagnoses based on audiotapes of 30 interviews. The interrater reliability (Kappa) for lifetime depressive disorder was 0.93. When one parent was not available to complete the SCID, diagnostic information was obtained from the other parent using a family history interview (Andreasen, Endicott, Spitzer, & Winokur, 1977). Data from 69 fathers and one mother were obtained from family history methods. Because maternal and paternal depression may differentially influence children’s emotional processing (e.g., Kujawa, et al., 2012), maternal and paternal depression were examined as separate variables. Of the 458 children, 148 (32.3%) had mothers, and 74 (16.2%) had fathers with a lifetime history of major depressive disorder (MDD) or dysthymic disorder.
Parenting Behavior
Negative parenting was measured using a lightly modified version of the Teaching Tasks battery (Egeland et al., 1995). One biological parent and the child completed six standardized tasks designed to elicit parent and child behaviors while the interaction was videotaped. The child’s primary caregiver was asked to accompany the child to the lab and complete the battery. For almost all families (93.0%), the biological mother was the parent who participated in the interaction. For the remaining 7.0% of families, the biological father participated instead. The battery began with a book reading task, followed by four teaching tasks that required the parent to prompt the child to complete a goal: naming objects with wheels, putting blocks together to form a bigger block, matching shapes and colors, and completing a maze using a mechanical drawing toy. Lastly, the parent presented a gift to the child. Trained coders reviewed the tapes for parental hostility, which captures a parent’s expression of anger, frustration, and criticism toward the child, and intrusiveness, which captures a parent’s failure to recognize child’s efforts to gain autonomy, or inappropriate interference with the child’s needs, interests or behaviors. Both variables were rated on 5-point scales (1–5) for each task, and ratings were averaged across tasks. Coders were unaware of the data on parental psychopathology and child emotion recognition. The internal consistency (α = .76, .61) and interrater reliability (ICC = .83, .70, n = 55) of the hostility and intrusiveness scales, respectively, were acceptable, though the internal consistency of the intrusiveness scale was in the marginal range. Because the hostility scores were highly skewed, a square root transformation was applied. As parental hostility and intrusiveness were moderately correlated (r = .37), the two variables were combined. Standard scores were calculated for the transformed hostility average and the intrusiveness average and the two variables were summed to form a negative parenting composite variable. The internal consistency (α = .70) and interrater reliability (ICC = .83) of the composite variable were acceptable.
Procedure
As the current study is part of a larger study involving a number of assessments, data used in this study were collected across two laboratory visits. Written informed consent was obtained from all parents. As part of the initial visit, children completed the PPVT and parents completed the CBCL. The SCID was completed with both parents over the phone between the first and second visits. At the second visit, participants first completed the emotion listening task, followed by the teaching tasks battery, and then the two affect labeling tasks. The two visits were scheduled as close as possible with an average of 47.87 days between visits (SD = 51.32).
Data Analysis
For all emotion recognition tasks, average accuracy rates were determined by calculating the percentage of correct responses out of total trials for each task and the percentage of correct responses for each emotion type within each task. To examine overall accuracy across tasks and emotional stimuli, repeated-measures ANOVAs were computed. Greenhouse-Geisser corrections were used for violations of sphericity and Bonferroni corrections were applied to control for multiple comparisons. Multiple regression analyses were computed to examine predictors of emotion recognition. Separate analyses were computed for average accuracy on each task as well as an emotion recognition composite, which was calculated by summing standard scores on each task.
Results
First, we evaluated characteristics of the sample and maternal and paternal depression group differences on demographic variables. Next, we examined typical emotion recognition abilities among preschool children by comparing accuracy across each of the emotion recognition tasks and specific types of emotional stimuli. In order to control for effects of child characteristics on emotion recognition skills, we then evaluated whether child age, sex, PPVT, or internalizing and externalizing symptoms predicted scores on any of the emotion recognition tasks or the emotion recognition composite. Lastly, our main analyses focus on the effects of negative parenting and parental depression on emotion recognition while controlling for relevant child characteristics.
Participant Characteristics
Child age, gender, race, PPVT scores, and CBCL internalizing/externalizing scores and parent education, and history of anxiety and substance use disorders as a function of both maternal and paternal history of depression are presented in Table 1. There were no significant associations between maternal or paternal depression and child age, gender, race, or parent education. There was a significant link between paternal depression and PPVT scores, such that a history of paternal depression was associated with lower PPVT scores, t(456) = 2.54, p < .05; however, both groups had mean PPVT scores in the average range. There was no significant association between maternal depression and PPVT scores. Children of mothers with a history of depression had higher CBCL internalizing scores than those of mothers with no history of depression, t(456) = −2.65, p < .05, but no significant differences were found for CBCL externalizing symptoms and there were no significant associations between paternal depression and CBCL scores. Mothers with a history of depressive disorders were more likely than those without such a history to also have a history of anxiety disorders, χ2(1) = 35.66, p < .001, and substance use disorders, χ2(1) = 9.65, p < .01. Likewise, fathers with a history of depressive disorders were more likely to have a history of anxiety disorders, χ2(1) = 44.85, p < .001, and substance use disorders, χ2(1) = 4.26, p < .05.
Table 1.
Participant characteristics by parental depression group.
| No maternal depression (n = 310) | Maternal history of depression (n = 148) | |
|---|---|---|
| Mean child age (months) | 43.77 (SD = 3.34) | 44.05 (SD = 3.69) |
| Sex (% female) | 44.5% | 52.0% |
| Race (% Caucasian) | 85.5% | 87.8% |
| Child PPVT | 102.82 (SD = 13.68) | 104.03 (SD = 12.31) |
| Child CBCL Internalizing Symptoms | 8.59 (SD = 5.78)* | 10.23 (SD = 7.05)* |
| Child CBCL Externalizing Symptoms | 12.44 (SD = 7.27) | 13.39 (SD = 7.43) |
| Mother obtained college degree (%) | 55.7% | 60.3% |
| Maternal lifetime history of anxiety disorder | 24.5%*** | 52.7%*** |
| Maternal lifetime history of substance use disorder | 18.7%** | 31.8%** |
| No paternal depression (n = 384) | Paternal history of depression (n = 74) | |
| Mean child age (months) | 43.95 (SD = 3.40) | 43.41 (SD = 3.73) |
| Sex (% female) | 45.3% | 55.4% |
| Race (% Caucasian) | 86.5% | 85.1% |
| Child PPVT | 103.90 (SD = 13.13)* | 99.65 (SD = 13.38)* |
| Child CBCL Internalizing Symptoms | 8.92 (SD = 5.92) | 10.15 (SD = 7.72) |
| Child CBCL Externalizing Symptoms | 12.54 (SD = 7.28) | 13.79 (SD = 7.54) |
| Father obtained college degree (%) | 49.3% | 41.7% |
| Paternal lifetime history of anxiety disorder | 14.6%*** | 48.6%*** |
| Parental lifetime history of substance use disorder | 35.9%* | 48.6%* |
p < .001;
p < .01;
p < .05
Emotion Recognition in Preschool Children
Comparison of emotion recognition tasks
Means and standard deviations of accuracy rates across tasks and emotional stimuli are presented in Table 2. Accuracy rates on each task were significantly correlated with accuracy on all other tasks (Table 3). A repeated-measures ANOVA was computed to examine the effect of task type on overall accuracy. There was a significant effect of task on accuracy, F(2, 950) = 152.87, p < .001, and paired-samples t-tests indicated that accuracy was higher for Emotion Learning than for both Emotion Labeling, t(476) = 21.59, p < .001 and Emotional Listening, t(475) = 12.55, p < .001. No significant differences were found between accuracy on Emotion Labeling and Emotional Listening.
Table 2.
Mean (Standard Deviation) accuracy for each emotion recognition task overall and emotion type within each task.
| Emotional Listening | Emotion Labeling | Emotion Learning | |||
|---|---|---|---|---|---|
| Overall Accuracy | .44(.22) | Overall Accuracy | .43(.16) | Overall Accuracy | .59(.21) |
| Happy Tones | .54(.35) | Happy Faces | .81(.32) | Happy Faces | .86(.29) |
| Sad Tones | .42(.36) | Angry Faces | .71(.38) | Angry Faces | .76(.34) |
| Neutral Tones | .36(.34) | Sad Faces | .49(.34) | Sad Faces | .74(.32) |
| Disgust Faces | .35(.35) | Scared Faces | .51(.34) | ||
| Scared Faces | .23(.26) | Surprised Faces | .50(.37) | ||
| Ashamed Faces | .14(.26) | Neutral Faces | .18(.28) | ||
| Surprised Faces | .13(.28) |
Table 3.
Correlations, means, and standard deviations for affect battery scores and predictors.
| Variable | Mean(SD)/% | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. PPVT | 103.21(13.25) | - | ||||||||||
| 2. Age (months) | 43.86(3.45) | .17*** | - | |||||||||
| 3. Sex (female) | 46.9% | .06 | .00 | - | ||||||||
| 4. Child Internalizing | 9.12(6.26) | −.09 | .04 | .01 | - | |||||||
| 5. Child Externalizing | 12.74(7.33) | −.09 | .01 | −.03 | .55*** | - | ||||||
| 6. Negative Parenting | .00(1.65) | −.22*** | −.04 | .00 | .02 | .06 | - | |||||
| 7. Maternal Depression | 32.3% | .04 | .04 | .07 | .12** | .06 | −.01 | - | ||||
| 8. Paternal Depression | 16.2% | −.12* | −.06 | .07 | .07 | .06 | .04 | .12* | - | |||
| 9. Emotion Recognition Composite | .00(2.26) | .49*** | .38*** | .05 | −.11* | −.03 | −.20*** | .05 | −.05 | - | ||
| 10. Listening Task | .44(.22) | .24*** | .18*** | .01 | −.02 | .04 | −.11* | .06 | .03 | .63*** | - | |
| 11. Labeling Task | .43(.16) | .41*** | .32*** | .14** | −.13** | −.04 | −.16** | .01 | −.03 | .81*** | .21*** | - |
| 12. Learning Task | .59(.21) | .46*** | .35*** | −.03 | −.10* | −.08 | −.18*** | .05 | −.10* | .81*** | .22*** | .62*** |
p < .001;
p < .01;
p < .05
Comparison of emotion types
Repeated-measures ANOVAs were then conducted to examine the effect of type of emotional stimuli on accuracy within each task. Means and standard deviations for each emotion type are presented in Table 2. For the Emotional Listening task, the main effect of stimulus type was significant, F(2, 950) = 36.63, p < .001, and paired-samples t-tests indicated that after applying Bonferroni corrections, accuracy rates for all affect types differed from one another (all ps < .01). For Emotion Labeling, there was a significant effect of stimulus type, F(6, 2850) = 381.55, p < .001. Paired-samples t-tests indicated that accuracy for all face types significantly differed from each other, even with Bonferroni corrections (all ps < .001), with the exception of the ashamed vs. surprised comparison, t(475) = −.31, p > .05. For Emotion Learning, there was a significant effect of stimulus type, F(5, 2375) = 372.43, p < .001. Paired samples t-tests indicated that accuracy for all face types significantly differed from all other face types even with Bonferroni corrections (all ps < .001), with the exception of the angry vs. sad, t(475) = 1.34, p > .05, and surprised vs. scared comparisons, t(475) = −.46, p > .05.
Consistent with Widen and Russell (2003), the results indicated that three-year-old children are more accurate in identifying happy voices and faces than all other types of affect. Accuracy rates are higher for sad and angry face recognition compared to surprised, afraid, disgusted and ashamed. Neutral stimuli appear to be the most difficult for young children to identify.
Effects of Child Characteristics
Regression analyses were conducted to examine child variables that may predict emotion recognition. Accuracy for each emotion recognition task and the sum of standard scores for all tasks combined were the dependent variables. Criterion variables were age in months, sex, PPVT scores and CBCL internalizing and externalizing symptom scores. Means and standard deviations and intercorrelations for all variables are presented in Table 3. Table 4 presents the standardized and unstandardized regression coefficients, as well as the total model R2, for the prediction of each emotion task and the composite score. PPVT and age in months significantly predicted emotion recognition across all dependent variables. Sex was not consistently related to emotion recognition. Significant effects were observed only for the Emotion Labeling task t(452) = 3.04, p < .01, which girls performed better than boys. Greater internalizing symptoms were associated with poorer accuracy on both the emotion recognition composite, t(452) = −2.76, p < .01, and Emotion Labeling task, t(452) = −3.08, p < .01, but no significant effects were observed for child externalizing symptoms on any of the dependent measures.
Table 4.
Multiple regression analyses with PPVT, age, sex, child internalizing symptoms and child externalizing symptoms predicting accuracy on each emotion recognition task and a composite of all tasks.
| Emotion Recognition Composite | Listening Task | Emotion Labeling Task | Emotion Learning Task | |||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Predictor | b(SE) | β | b(SE) | β | b(SE) | β | b(SE) | β |
| PPVT | .07(.01) | .43*** | .004(.00) | .22*** | .004(.00) | .36*** | .01(.00) | .41*** |
| Age (months) | .20(.03) | .31*** | .01(.00) | .15** | .01(.00) | .27*** | .02(.00) | .28*** |
| Sex (female) | .13(.17) | .03 | .00(.02) | −.00 | .04(.01) | .12** | −.02(.02) | −.06 |
| Child Internalizing | −.05(.02) | −.13** | .00(.00) | −.06 | −.004(.00) | −.15** | .00(.00) | −.08 |
| Child Externalizing | .02(.01) | .08 | .00(.00) | .09 | .00(.00) | .08 | .00(.00) | .00 |
| Total model R2 = .34 | Total model R2 =.08 | Total model R2 =.27 | Total model R2 =.30 | |||||
p < .001;
p < .01;
p < .05
Effects of Negative Parenting and Parental Depression
Hierarchical regression analyses were conducted to examine parental predictors of child emotion recognition. Accuracy for each emotion recognition task and the sum of standard scores for all tasks combined were the dependent variables. The negative parenting variable was centered. Because child age, PPVT scores, and internalizing symptoms were shown to relate to emotion recognition abilities, these variables were added to the model first to evaluate whether parenting and parental depression contribute unique variance beyond these factors1. In Step 1, we entered child age in months, PPVT scores and internalizing symptoms, followed by maternal and paternal depression history and negative parenting in Step 2, and the interactions between parenting and parental depression in Step 3.
Means, standard deviations, and intercorrelations for all variables are presented in Table 3. Table 5 presents the standardized and unstandardized regression coefficients, as well as the total model R2, for the prediction of each emotion task and the composite score. Again, PPVT and age in months significantly predicted emotion recognition across all dependent variables, and child internalizing symptoms significantly predicted scores on the emotion recognition composite, Emotion Labeling task, and Emotion Learning task. Negative parenting contributed additional variance in predicting performance on the emotion recognition composite and Emotion Learning task. Maternal and paternal depression did not uniquely predict emotion recognition on any of the measures. However, the interaction between maternal depression and negative parenting was significant for the emotion recognition composite, t(449) = −2.25, p < .05, and Emotion Learning2, t(449) = −2.30, p < .05, and approached significance for Emotional Listening, t(449) = −1.85, p = .065. The interaction between paternal depression and negative parenting was not significant for any of the dependent variables3. To interpret the significant maternal depression X negative parenting interaction (Figure 1), hierarchical regression analyses were calculated at each level of maternal depression with emotion recognition composite scores as the dependent variable. For children with a maternal history of depression, more negative parenting was associated with poorer accuracy, β = −.24; t(142) = −3.71, p < .001. For children with no maternal history of depression, the effect of negative parenting was not significant, β = −.03; t(304) = −.60, p > .05. The pattern of results was the same for Emotion Learning, with a significant effect of negative parenting among children with a maternal history of depression, β = −.23; t(142) = −3.25, p < .01, but no significant effect of negative parenting for children with no maternal history of depression, β = −.01; t(304) = .28, p > .05.
Table 5.
Hierarchical regression with PPVT, age, child internalizing symptoms, maternal & paternal depression, negative parenting, and interactions between parenting and parental depression on each emotion recognition task and a composite of all tasks.
| Emotion Recognition Composite | Listening Task | Emotion Labeling Task | Emotion Learning Task | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Predictor | b(SE) | Entry β | Final β | b(SE) | Entry β | Final β | b(SE) | Entry β | Final β | b(SE) | Entry β | Final β |
| 1. Child Characteristics | ||||||||||||
|
| ||||||||||||
| PPVT | .07(.01) | .43*** | .42*** | .004(.00) | .21*** | .21*** | .00(.00) | .36*** | .35*** | .01(.00) | .40*** | .39*** |
| Age (months) | .20(.03) | .31*** | .30*** | .01(.00) | .15** | .15** | .01(.00) | .27*** | .26*** | .02(.00) | .28*** | .28*** |
| Child Internalizing | −.03(.01) | −.09* | −.09* | .00(.00) | −.01 | −.02 | .00(.00) | −.10* | −.11* | .00(.00) | −.08 | −.08* |
|
| ||||||||||||
| 2. Parental Variables | ||||||||||||
|
| ||||||||||||
| Paternal Depression | .17(.24) | .03 | .03 | .03(.03) | .06 | .07 | .01(.02) | .03 | .03 | −.02(.02) | −.03 | −.02 |
| Maternal Depression | .14(.19) | .03 | .03 | .02(.02) | .04 | .04 | .00(.01) | .00 | .00 | .01(.02) | .03 | .03 |
| Negative Parenting | −.14(.05) | −.10* | −.02 | −.01(.01) | −.06 | .03 | −.01(.00) | −.07 | −.07 | −.01(.01) | −.09* | −.02 |
|
| ||||||||||||
| 3. Interactions | ||||||||||||
|
| ||||||||||||
| Paternal Depression X Negative Parenting | −.11(.14) | −.03 | −.03 | −.03(.02) | −.08 | −.08 | .01(.01) | .02 | .02 | −.00(.01) | −.01 | −.01 |
| Maternal Depression X Negative Parenting | −.25(.11) | −.11* | −.11* | −.02(.01) | −.10 | −.10 | −.00(.01) | −.02 | −.02 | −.02(.01) | −.11* | −.11* |
| Total model R2 = .36 | Total model R2 =.10 | Total model R2 =.25 | Total model R2 =.31 | |||||||||
p < .001;
p < .01;
p < .05
Figure 1.
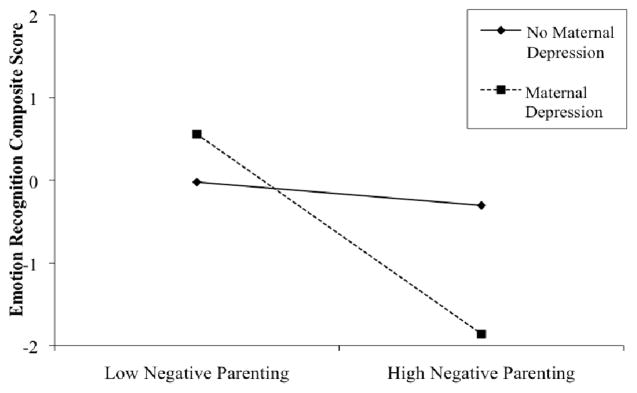
Interaction between maternal depression and negative parenting in predicting emotion recognition composite scores. Low and high negative parenting represent the lowest and highest scores obtained in the sample.
Because of the overlap between parental depression and anxiety and substance use disorders, an additional multiple regression analysis was calculated to control for the effects of parental anxiety or substance use disorders on the emotion recognition composite variable. The model was identical to the overall analyses, with the addition of maternal and paternal anxiety and substance use disorder histories to Step 1. The maternal depression X negative parenting interaction remained significant, β = −.10; t(445) = −2.14, p < .05, suggesting that anxiety and substance use disorders do not fully account for the effect of the interaction.
Lastly, additional analyses were computed to examine whether maternal depression timing or chronicity influence the results. Only children with a maternal history of depression were included in these analyses in order to compare subtypes of depression. Child characteristics were again entered in Step 1. In Step 2, current (i.e., past month; n = 17) vs. lifetime (n = 131) depression or maternal chronic (n = 55) vs. acute (n = 92) depression was entered along with negative parenting. Chronicity data were missing for one mother. The interaction between the subtype of depression and parenting was entered in Step 3. The main effect of current vs. lifetime depression, β = .02; t(141) = .35, p > .05, and interaction between timing of depression and negative parenting, β = −.11; t(141) = 1.65, p = .10, were not significant. In addition, the main effect of chronic vs. acute, β = .00; t(140) = .07, p > .05, and interaction between chronicity and negative parenting were not significant, β = .02; t(140) = .19, p > .05.
Discussion
Consistent with previous work (Ale, et al., 2010; Broeren, et al., 2011; MacDonald, et al., 1996; Widen & Russell, 2003), the current study provides further evidence that young children are most accurate in identifying happy faces and tones, followed by other basic emotions (e.g., sad and angry) and then more complex emotions (e.g., shame, surprise). Interestingly, neutral faces and vocalizations were the most difficult for children to accurately identify, even in tasks in which incorrect responses were initially corrected. Thus, failure to identify neutral images in early childhood cannot be entirely attributed to lack of vocabulary to describe the images, and may relate instead to the ambiguous nature of neutral facial expressions and vocalizations.
Also consistent with previous work (Bennett, et al., 2005), the current findings suggest that a measure of intellectual functioning (i.e., the PPVT in the current study) is a moderate predictor of emotion recognition in early childhood. In addition, child age was also a moderate predictor of emotion recognition ability, despite the fact that the current study only included children within a very narrow age range. While previous research has suggested that emotion recognition continues to develop across childhood and adolescence (Ale, et al., 2010; Broeren, et al., 2011; Durand, et al., 2007), the current study suggests there is a substantial increase in emotion recognition between ages three and four. In addition, consistent with previous research (e.g., Fine et al., 2003; Trentacosta & Fine, 2010), greater child internalizing symptoms were associated with poorer emotion recognition in the current study. Interestingly, the current findings suggest that this association is already present in early childhood, but the combined effects of negative parenting and maternal depression continue to predict emotion recognition skills even when controlling for child symptoms.
The current results suggest that negative parenting behavior, consisting of hostility and intrusiveness, is associated with poorer performance on emotion recognition tasks, and that maternal depression only has an effect on child emotion recognition skills in combination with negative parenting. Parental anger and criticism in combination with interference with the child’s need for autonomy may limit the child’s experiences with a wide range of social and affective cues, which could impair the development of emotion recognition skills. In addition, this effect appears to be moderated by maternal history of depression. Mothers with a history of depression may also show deficits in emotion recognition (e.g., Feinberg et al., 1986; Persad & Polivy, 1993; Rubinow & Post, 1992), which could be transmitted to offspring through genetic processes or limited exposure to opportunities to learn these skills Relatedly, mothers with a history of depression may show widespread abnormalities in the affect cues used to communicate with their children, including flat speech, lower rates of affective facial expression, and delayed responding (for reviews, Downey & Coyne, 1990; Weinberg & Tronick, 1998). Exposure to abnormal affect behavior from parents may interfere with children’s ability to learn affect cues and may intensify the maladaptive effects of negative parenting on emotion knowledge. That is, the affective characteristics of depressed mothers may enhance the impact of negative parenting style on the development of emotion recognition deficits.
Importantly, the current results suggest that maternal depression alone may not predispose children to poorer emotion understanding in preschool. Instead, children of mothers with a history of depression but less negative parenting styles show typical development of emotion recognition at least in early childhood. This finding is somewhat consistent with previous studies that have failed to find effects of maternal depressive symptoms on emotion recognition (Bennett, et al., 2005) or have observed effects of maternal depression only in combination with other risk factors (Jacobs, et al., 2011). It is important to note, however, that most of the mothers in our study were not currently depressed, and many mothers had only experienced depression prior to the child’s birth. Though we did not find a significant effect for current vs. lifetime depression, our analysis was limited by the small number of mothers currently in a depressive episode. It is possible that current maternal depression may have more pervasive effects on the development of children’s emotion knowledge even in the absence of negative parenting.
Given the importance of emotion recognition in predicting child outcomes, there has been growing interest in the integration of emotion theory in interventions. For example, a recent study examined the effects of an emotion-focused intervention for parents of children with behavior problems and found improvements both in the children’s emotion knowledge and behavior (Havighurst, Wilson, Harley, Keho, Efron, & Prior, 2012). Emotion research can also be used to drive the development of preventive interventions (Izard, 2002) and attempts have been made to identify children at increased risk for emotion knowledge difficulties to target for interventions. For example, children from low-income families are at a high risk for emotion knowledge deficits, and research suggests that emotion-based prevention programs can be helpful for improving emotion knowledge as well as symptoms of internalizing and externalizing problems among children attending Head Start (Izard et al., 2008). The results of the current study provide further insight into identifying children who may be appropriate targets for preventive interventions by suggesting that it may be important to examine both parental psychopathology and parenting behavior in combination to identify children at greatest risk.
Though bivariate correlations suggest that a paternal history of depression is associated with poorer accuracy on the Emotion Learning task, no significant main or interactive effects of paternal depression were found in regression analyses. While these results are consistent with a stronger impact of maternal than paternal depression on offspring functioning in childhood (Connell & Goodman, 2002) and previous evidence of emotional processing deficits among children of depressed mothers, but not fathers (Kujawa et al., 2012), it is important to note that the parenting variable used in the current study primarily reflected maternal parenting behavior. Thus, while paternal depression does not appear to interact with parenting to predict emotion recognition, it is possible that including observational measures of both maternal and paternal parenting would strengthen these results.
There are a number of strengths to the current study, including the large sample size and inclusion of observational measures of parenting behavior. In addition, this is among the first studies to examine interactive effects of parental variables in predicting child emotion recognition. Nonetheless, there are several limitations. First, low accuracy rates, particularly on the Emotion Listening and Emotion Labeling tasks, suggest that these tasks may have been too difficult for children of this age. Other tasks developed to specifically assess emotion understanding in preschool children, such as the Affective Knowledge Test (Denham, 1986) or Emotion Matching Task (Izard, Haskins, Schultz, Trentacosta, & King, 2003), may be more sensitive in this age group. Though it was developed for young children, the Emotion Labeling task in the current study may have been particularly challenging, as it required the children to remember the possible response options and included emotional concepts (e.g., shame) that may have been less familiar to the children than other emotions. While significant interactive effects of depression and parenting were found for the emotion composite score and Emotion Learning task, with effects for the Emotion Listening task approaching significance, no significant effects were found for the Emotion Labeling task. Nonetheless, child internalizing symptoms did significantly predict performance on the Emotion Labeling task, suggesting that it has some validity in tapping individual differences in early emotion recognition skills. It is also possible that the Emotion Labeling task assesses somewhat different aspects of emotional processing compared to the Emotional Listening or Emotion Learning tasks. The ability to freely label emotional expressions may be more closely linked to child internalizing problems, while the ability to identify affective vocal tones and to learn to identify emotions across time may be more strongly linked to parenting factors.
The current findings emphasize the importance of examining multiple factors in understanding the development of emotion knowledge in childhood. Maternal depression alone does not appear to be related to poorer emotion recognition among offspring in early childhood but does seem to moderate the association between negative parenting and emotion recognition. Future research is needed to determine whether similar effects are apparent in other developmental periods.
Acknowledgments
This work was supported by the following grants: National Institute of Mental Health Grants RO1 MH069942 to Daniel N. Klein and F31 MH09530701 to Autumn Kujawa, and GCRC Grant M01-RR10710 to Stony Brook University from the National Center for Research Resources.
Footnotes
As sex significantly predicted accuracy on the Emotion Labeling task, we also evaluated the model for Emotion Labeling with the addition of sex to Step 1. The results were the same as the model excluding sex (Table 5).
To determine whether feedback across trials influenced effects for Emotion Learning, a repeated-measures ANCOVA was computed with the three trials as the repeated-measures variables and all other variables as covariates. Accuracy increased across trials, F(2, 898) = 100.85, p < .001, but no significant interactions were found between trial and maternal/paternal depression, negative parenting, or the interactions between maternal or paternal depression and negative parenting (all Fs < 1, p > .05). Thus, all analyses focus on average accuracy across trials.
Because 93% of parents in the observational parenting assessment were biological mothers, the overall model was calculated to examine predictors of the emotion recognition composite excluding cases in which the biological father completed the Teaching Tasks (n = 32). The maternal depression X parenting interaction remained significant, β = −.11; t(417) = −2.17, p < .05.
References
- Achenbach TM, Rescorla LA. Manual for ASEBA preschool forms & profiles. Burlington, VT: University of Vermont, Reseach Center for Children, Youth, & Families; 2000. [Google Scholar]
- Ale CM, Chorney DB, Brice CS, Morris TL. Facial affect recognition and social anxiety in preschool children. Early Child Development and Care. 2010;180(10):1349–1359. doi: 10.1080/03004430903059318. [DOI] [Google Scholar]
- Andreasen NC, Endicott J, Spitzer RL, Winokur G. The family history method using diagnostic criteria: Reliability and validity. Archives of General Psychiatry. 1977;34(10):1229–1235. doi: 10.1001/archpsyc.1977.01770220111013. [DOI] [PubMed] [Google Scholar]
- Bennett DS, Bendersky M, Lewis M. Antecedents of emotion knowledge: Predictors of individual differences in young children. Cognition and Emotion. 2005;19(3):375–396. doi: 10.1080/02699930441000201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowers D, Blonder LX, Heilman KM. The Florida Affect Battery. Cognitive Neuroscience Laboratory, University of Florida; 1991. [Google Scholar]
- Broeren S, Muris P, Bouwmeester S, Field AP, Voerman JS. Processing biases for emotional faces in 4- to 12-year-old non-clinical children: An exploratory study of developmental patterns and relationships with social anxiety and behavioral inhibition. Journal of Experimental Psychopathology. 2011;2(4):454–474. doi: 10.5127/jep.016611. [DOI] [Google Scholar]
- Camras LA, Ribordy S, Hill J, Martino S, Sachs V, Spaccarelli S, Stefani R. Maternal facial behavior and the recognition and production of emotional expression by matreated and nonmaltreated children. Developmental Psychology. 1990;26:304–312. [Google Scholar]
- Caron RF, Caron AJ, Myers RS. Abstraction of invariant face expressions in infancy. Child Development. 1982;53(4):1008–1015. doi: 10.2307/1129141. [DOI] [PubMed] [Google Scholar]
- Cohn JF, Tronick EZ. Three-month-old infants’ reaction to simulated maternal depression. Child Development. 1983;54(1):185–193. doi: 10.2307/1129876. [DOI] [PubMed] [Google Scholar]
- Connell AM, Goodman SH. The association between psychopathology in fathers versus mothers and children’s internalizing and externalizing behavior problems: A meta-analysis. Psychological Bulletin. 2002;128(5):746–773. doi: 10.1037/0033-2909.128.5.746. [DOI] [PubMed] [Google Scholar]
- Denham SA. Social cognition, prosocial behavior, and emotion in preschoolers: Contextual validation. Child Development. 1986;57(1):194–201. doi: 10.2307/1130651. [DOI] [Google Scholar]
- Denham SA, Blair KA, DeMulder E, Levitas J, Sawyer K, Auerbach-Major S, Queenan P. Preschool emotional competence: Pathway to social competence. Child Development. 2003;74(1):238–256. doi: 10.1111/1467-8624.00533. [DOI] [PubMed] [Google Scholar]
- Doan SN, Wang Q. Maternal discussions of mental states and behaviors: Relations to emotion situation knowledge in European American and immigrant Chinese children. Child Development. 2010;81(5):1490–1503. doi: 10.1111/j.1467-8624.2010.01487.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Downey G, Coyne JC. Children of depressed parents: An integrative review. Psychological Bulletin. 1990;108(1):50–76. doi: 10.1037/0033-2909.108.1.50. [DOI] [PubMed] [Google Scholar]
- Dunn J, Brown J, Beardsall L. Family talk about feeling states and children’s later understanding of others’ emotions. Developmental Psychology. 1991;27(3):448–455. doi: 10.1037/0012-1649.27.3.448. [DOI] [Google Scholar]
- Dunn LM, Dunn LM. Peabody Picture Vocabulary Test-III. Circle Pines, MN: American Guidance Service; 1997. [Google Scholar]
- Durand K, Gallay M, Seigneuric A, Robichon F, Baudouin J-Y. The development of facial emotion recognition: The role of configural information. Journal of Experimental Child Psychology. 2007;97(1):14–27. doi: 10.1016/j.jecp.2006.12.001. [DOI] [PubMed] [Google Scholar]
- Egeland B, Weinfield NS, Heiester M, Lawrence C, Pierce S, Chippendale K, Powell K. Unpublished Manuscript. Institute of Child Development, University of Minnesota; 1995. Teaching tasks administration and scoring manual. [Google Scholar]
- Ensor R, Spencer D, Hughes C. ‘You feel sad?’ emotion understanding mediates effects of verbal ability and mother-child mutuality on prosocial behaviors: Findings from 2 years to 4 years. Social Development. 2011;20(1):93–110. doi: 10.1111/j.1467-9507.2009.00572.x. [DOI] [Google Scholar]
- Feinberg TE, Rifkin A, Schaffer C, Walker E. Facial discrimination and emotional recognition in schizophrenia and affective disorders. Archives of General Psychiatry. 1986;43(3):276–279. doi: 10.1001/archpsyc.1986.01800030094010. [DOI] [PubMed] [Google Scholar]
- Fine SE, Izard CE, Mostow AJ, Trentacosta CJ, Ackerman BP. First grade emotion knowledge as a predictor of fifth grade self-reported internalizing behaviors in children from economically disadvantaged families. Development and Psychopathology. 2003;15(2):331–342. doi: 10.1017/s095457940300018x. [DOI] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams JBW. The Structured Clinical Interview for DSM-IV Axis I Disorders - Non-patient editions. New York: Biometrics Research Department, New York State Psychiatric Institute; 1996. [Google Scholar]
- Flom R, Bahrick LE. The development of infant discrimination of affect in multimodal and unimodal stimulation: The role of intersensory redundancy. Developmental Psychology. 2007;43(1):238–252. doi: 10.1037/0012-1649.43.1.238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fries ABW, Pollak SD. Emotion understanding in postinstitutionalized Eastern European children. Development and Psychopathology. 2004;16(2):355–369. doi: 10.1017/s0954579404044554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Havighurst S, Wilson K, Harley A, Kehoe C, Efron D, Prior M. “Tuning into Kids”: Reducing young children’s behavior problems using an emotion coaching parenting program. Child Psychiatry & Human Development. 2012 doi: 10.1007/s10578-012-0322-1. [DOI] [PubMed] [Google Scholar]
- Hollingshead AB. Unpublished manuscript. Yale University; New Haven, CT: 1975. Four factor index of social status. [Google Scholar]
- Izard C. Emotional intelligence or adaptive emotions? Emotion. 2001;1(3):249–257. doi: 10.1037/1528-3542.1.3.249. [DOI] [PubMed] [Google Scholar]
- Izard C. Translating emotion theory and research into preventive interventions. Psychological Bulletin. 2002;128(5):796–824. doi: 10.1037/0033-2909.128.5.796. [DOI] [PubMed] [Google Scholar]
- Izard C, Fine S, Schultz D, Mostow A, Ackerman B, Youngstrom E. Emotion knowledge as a predictor of social behavior and academic competence in children at risk. Psychological Science. 2001;12(1):18–23. doi: 10.1111/1467-9280.00304. [DOI] [PubMed] [Google Scholar]
- Izard CE, Haskins FW, Schultz D, Trentacosta CJ, King KA. Emotion Matching Task. Unpublished test (Contains 182 standardized color photos of children’s emotion expressions) Newark, DE: University of Delaware; 2003. [Google Scholar]
- Izard CE, King KA, Trentacosta CJ, Morgan JK, Laurenceau J-P, Krauthamer-Ewing ES, Finlon KJ. Accelerating the development of emotion competence in Head Start children: Effects on adaptive and maladaptive behavior. Development and Psychopathology. 2008;20(01):369–397. doi: 10.1017/S0954579408000175. [DOI] [PubMed] [Google Scholar]
- Jacobs RH, Pine DS, Schoeny ME, Henry DB, Gollan JK, Moy G, Wakschlag LS. Maternal depressive history, teen 5HTTLPR genotype, and the processing of emotional faces: Exploring mechanisms of risk. [doi: 10.1016/j.brat.2010.10.004] Behaviour Research and Therapy. 2011;49(1):80–84. doi: 10.1016/j.brat.2010.10.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joormann J, Gilbert K, Gotlib IH. Emotion identification in girls at high risk for depression. Journal of Child Psychology & Psychiatry. 2010;51(5):575–582. doi: 10.1111/j.1469-7610.2009.02175.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kujawa A, Hajcak G, Torpey D, Kim J, Klein DN. Electrocortical reactivity to emotional faces in young children and associations with maternal and paternal depression. Journal of Child Psychology and Psychiatry. 2012;53(2):207–215. doi: 10.1111/j.1469-7610.2011.02461.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leppänen JM, Hietanen JK. Emotion recognition and social adjustment in school-aged girls and boys. Scandinavian Journal of Psychology. 2001;42(5):429–435. doi: 10.1111/1467-9450.00255. [DOI] [PubMed] [Google Scholar]
- Leppänen JM, Nelson CA. Tuning the developing brain to social signals of emotions. Nature Reviews Neuroscience. 2009;10(1):37–47. doi: 10.1038/nrn2554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacDonald PM, Kirkpatrick SW, Sullivan LA. Schematic drawings of facial expressions for emotion recognition and interpretation by preschool-aged children. Genetic, Social, and General Psychology Monographs. 1996;122(4):373–388. [PubMed] [Google Scholar]
- McElwain NL, Halberstadt AG, Volling BL. Mother- and father-reported reactions to children’s negative emotions: Relations to young children’s emotional understanding and friendship quality. Child Development. 2007;78(5):1407–1425. doi: 10.1111/j.1467-8624.2007.01074.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mrakotsky C. dissertation manuscript. Austrian National Library; Vienna: 2001. Spatial cognition, face perception, and affect recognition in preschool depressive syndromes: A neuropsychological framework of information processing. [Google Scholar]
- Peltola MJ, Leppänen JM, Hietanen JK. Enhanced cardiac and attentional responding to fearful faces in 7-month-old infants. Psychophysiology. 2011;48(9):1291–1298. doi: 10.1111/j.1469-8986.2011.01188.x. [DOI] [PubMed] [Google Scholar]
- Persad SM, Polivy J. Differences between depressed and nondepressed individuals in the recognition of and response to facial emotional cues. Journal of Abnormal Psychology. 1993;102(3):358–368. doi: 10.1037//0021-843x.102.3.358. [DOI] [PubMed] [Google Scholar]
- Pollak SD, Cicchetti D, Hornung K, Reed A. Recognizing emotion in faces: Developmental effects of child abuse and neglect. Developmental Psychology. 2000;36(5):679–688. doi: 10.1037/0012-1649.36.5.679. [DOI] [PubMed] [Google Scholar]
- Pollak SD, Messner M, Kistler DJ, Cohn JF. Development of perceptual expertise in emotion recognition. Cognition. 2009;110(2):242–247. doi: 10.1016/j.cognition.2008.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollak SD, Sinha P. Effects of early experience on children’s recognition of facial displays of emotion. Developmental Psychology. 2002;38(5):784–791. doi: 10.1037/0012-1649.38.5.784. [DOI] [PubMed] [Google Scholar]
- Rohde P, Lewinsohn PM, Seeley JR. Comparability of telephone and face-to-face interviews in assessing axis I and II disorders. American Journal of Psychiatry. 1997;154(11):1593–1598. doi: 10.1176/ajp.154.11.1593. [DOI] [PubMed] [Google Scholar]
- Rubinow DR, Post RM. Impaired recognition of affect in facial expression in depressed patients. Biological Psychiatry. 1992;31(9):947–953. doi: 10.1016/0006-3223(92)90120-o. [DOI] [PubMed] [Google Scholar]
- Sobin C, Weissman MM, Goldstein RB, Adams P. Diagnostic interviewing for family studies: Comparing telephone and face-to-face methods for the diagnosis of lifetime psychiatric disorders. Psychiatric Genetics. 1993;3(4):227–233. [Google Scholar]
- Taumoepeau M, Ruffman T. Mother and infant talk about mental states relates to desire language and emotion understanding. Child Development. 2006;77(2):465–481. doi: 10.1111/j.1467-8624.2006.00882.x. [DOI] [PubMed] [Google Scholar]
- Taumoepeau M, Ruffman T. Stepping stones to others’ minds: Maternal talk relates to child mental state language and emotion understanding at 15, 24, and 33 months. Child Development. 2008;79(2):284–302. doi: 10.1111/j.1467-8624.2007.01126.x. [DOI] [PubMed] [Google Scholar]
- Trentacosta CJ, Fine SE. Emotion knowledge, social competence, and behavior problems in childhood and adolescence: A meta-analytic review. Social Development. 2010;19(1):1–29. doi: 10.1111/j.1467-9507.2009.00543.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trentacosta CJ, Izard CE, Mostow AJ, Fine SE. Children’s emotional competence and attentional competence in early elementary school. School Psychology Quarterly. 2006;21(2):148–170. doi: 10.1521/scpq.2006.21.2.148. [DOI] [Google Scholar]
- Weinberg MK, Tronick EZ. Emotional characteristics of infants associated with maternal depression and anxiety. Pediatrics. 1998;102(Supplement E1):1298–1304. [PubMed] [Google Scholar]
- Widen SC, Russell JA. A closer look at preschoolers’ freely produced labels for facial expressions. Developmental Psychology. 2003;39(1):114–128. doi: 10.1037/0012-1649.39.1.114. [DOI] [PubMed] [Google Scholar]
- Williams JB, Gibbon M, First MB, Spitzer RL. The Structured Clinical Interview for DSM-III-R (SCID): II. Multisite test-retest reliability. Archives of General Psychiatry. 1992;49(8):630–636. doi: 10.1001/archpsyc.1992.01820080038006. [DOI] [PubMed] [Google Scholar]