

Abstract
OBJECTIVE
Mothers of children at risk for type 1 diabetes report engaging in preventive behaviors. The purpose of this study is to further document these actions in an international, longitudinal sample and examine variables that predict whether mothers engage in these behaviors.
RESEARCH DESIGN AND METHODS
This study examined an international sample (from Finland, Germany, Sweden, and the U.S.) from the naturalistic, longitudinal The Environmental Determinants of Diabetes in the Young (TEDDY) study, which tracked children genetically at risk for type 1 diabetes from birth to age 15 years. Mothers of 7,613 infants aged 6 months and 6,503 infants aged 15 months completed questionnaires assessing psychosocial factors and actions intended to prevent diabetes.
RESULTS
Many mothers (29.9% at 6 months and 42.8% at 15 months) reported engaging in a behavior intended to prevent type 1 diabetes, with the largest percentages (20.9–29.2%) reporting making changes to their child’s diet (e.g., reducing the consumption of sweets and carbohydrates). Factors related to engaging in preventive behaviors include older maternal age; higher maternal education; minority status; having only one child; having a first-degree relative with type 1 diabetes; being from a country other than Sweden; having an accurate perception of the child’s increased risk for developing diabetes; having postpartum depression, maternal anxiety, and worry about the risk of diabetes; and believing that diabetes can be prevented.
CONCLUSIONS
The findings of this study suggest that many mothers engage in actions to prevent diabetes and highlight the importance of tracking these behaviors to ensure the validity of naturalistic observational studies.
Introduction
There is mixed evidence suggesting that individuals make behavior changes after being notified of their genetic risk for certain diseases. Behaviors such as smoking cessation, physical activity, and medication and vitamin usage have shown little or no change because of risk notification, whereas there is some evidence that individuals make dietary changes as a result (1). Screening behaviors do increase in patients notified of increased genetic risk for cancer (2). Furthermore, patients increase dietary supplement usage when informed of an increased risk for developing Alzheimer disease, despite the fact that these changes have not been shown to prevent or delay the condition (3). There currently is no means of preventing type 1 diabetes in children with genetic risk for the disease; despite this, many caregivers report engaging in preventive behaviors. In the Prospective Assessment in Newborns of Diabetes Autoimmunity (PANDA) study (4), an observational study following infants at genetic risk for type 1 diabetes, many mothers reported taking actions intended to prevent diabetes. In fact, when parents were provided with a list of possible prevention behaviors more than 3 years after study enrollment, 67% reported behaviors intended to prevent diabetes, which included behaviors to monitor for the development of diabetes. Studies examining a smaller subgroup of the Diabetes Prevention Trial–Type 1 (DPT-1) (5,6), which examined caregivers of children and adults with genetic risk of diabetes who were offered research interventions, found that 38–48% of parents reported initiating actions to prevent type 1 diabetes. In both studies, dietary changes were the most commonly reported type of preventive behavior. Both the PANDA and the DPT-1 studies supported the assertion that many caregivers engage in preventive behaviors; however, data were cross-sectional and based on relatively small sample sizes within the U.S. only.
The Environmental Determinants of Diabetes in the Young (TEDDY) study is an international, longitudinal, naturalistic study following more than 8,000 children in an effort to identify the environmental trigger(s) of type 1 diabetes in children who are genetically at risk for the disease. TEDDY participants were identified at birth and joined the study before 4.5 months of age (7). Since parents were informed of their baby’s risk for type 1 diabetes as part of the TEDDY recruitment process, monitoring parental efforts to prevent the disease in the child is critical to understanding the impact of TEDDY on children and families. Furthermore, although families were told there was nothing they could do to prevent diabetes, many parents may still engage in behavior changes, and these changes could affect the interpretation of the natural history data collected as part of TEDDY. The current study documents maternal reports of actions to prevent type 1 diabetes during the first year of the TEDDY study. This study also examined the characteristics of mothers who reported such preventive actions, including both sociodemographic and psychological variables.
Research Design and Methods
Participants in the TEDDY Study
TEDDY is a natural history study designed to identify environmental triggers of autoimmunity and the onset of type 1 diabetes in genetically at-risk children identified at three centers in the U.S. (in Colorado, Georgia/Florida, and Washington State) and three centers in Europe (in Finland, Germany, and Sweden). Infants are screened at birth using HLA genotyping and families of infants eligible for HLA testing are invited to participate. Families were recruited from both the general population and from a subset of families with a first-degree relative (FDR) affected by type 1 diabetes. As part of the study sampling design, the German site recruited a larger proportion of participants with an FDR with type 1 diabetes than other sites. Parents were fully informed of the infant’s increased genetic risk, and infants were enrolled in the study before 4.5 months of age. After enrollment, families participate in clinic visits every 3 months during the first 4 years of the child’s life and every 6 months thereafter up to the age of 15 years. A variety of data are collected during each study visit, including biological samples (e.g., blood and saliva), records of the child’s diet, illnesses, and life stressors as well as information about related psychosocial functioning of the caregiver and child, as reported by the caregiver.
This study focuses on the first year of families’ participation in the TEDDY study, which began when infants were between birth and 4.5 months of age. Data from the 6- and 15 month study visits were used and were current as of June 30, 2011. Of a total of 8,677 participants who joined the TEDDY study, 8,133 completed the 6- or 15-month study visits. (For an extensive discussion of the characteristics of participants who dropped out during the first year of TEDDY, see Johnson et al. [8].) Of these participants, questionnaire data used for this study were available for 7,613 participants at the 6-month visit and 6,503 participants at the 15-month visit; 6,303 completed questionnaires at both 6 and 15 months. Only mothers’ responses were used because mothers were most often identified as the primary caregiver.
Measures
Sociodemographic Variables
Child sociodemographic characteristics included sex (male/female); ethnic minority status (U.S.: the child’s mother’s first language is not English or the mother was not born in the U.S. or the child is a member of an ethnic minority group [yes/no]; Europe: the child’s mother’s first language or country of birth is other than that of the country in which the child resides [yes/no]); whether the child is an only child (yes/no); and whether the child has an FDR with type 1 diabetes (yes/no). Maternal sociodemographic characteristics included mother’s age (years); mother’s education (primary education or high school, trade school or some college, graduated from college); and marital status (married/living together vs. single parent). Household crowding was measured by the number of persons in the household divided by the number of rooms in the house. Because the crowding variable was skewed, it was rescored to normalize the distribution (1 = 0–0.49; 2 = 0.50–0.59; 3 = 0.60–0.75; 4 = 0.76–1.00; 5 = >1.00).
Maternal Anxiety About the Child’s Diabetes Risk
An abbreviated six-item version of the state component of the Spielberg State-Trait Anxiety Inventory (STAI) (9) was used to assess maternal anxiety about the child’s risk of developing type 1 diabetes. This abbreviated form showed excellent internal consistency (coefficient α of 0.901 and 0.904 at 6- and 15-month study visits, respectively). Mothers also were asked, “How often do you worry that your child will develop diabetes?”; this question was scored on a 5-point Likert scale (1 = never, 5 = very often).
Maternal Depression
Postpartum depression was measured at the 6-month study visit using the Edinburgh Postnatal Depression Scale (EPDS) (10,11) (coefficient α = 0.844). Because the EPDS total scores were skewed, they were rescored to normalize the distribution 0 = 0, 1 = 1–2, 2 = 3–5, 3 = 6–8, 4 = 12, 5 = 13–27. In addition, scores were coded as above or below the clinical cutoff for postpartum depression (≥13). At the 15-month visit, maternal depression was assessed using the 6-item depression scale from the Well-Being Questionnaire (WBQ) (12), which showed fair internal consistency (coefficient α = 0.664). The WBQ depression scale scores also were skewed, so they were recoded to normalize the distribution (0 = 0–1; 1 = 2–4; 3 = ≥5). The EDPS (6 months) and the WBQ (15 months) were correlated (r = 0.40; P < 0.001).
Maternal Perception of Diabetes Risk
Mothers were asked about their perception of their child’s risk for developing type 1 diabetes at the 6- and 15-month study visits, and their responses were coded as accurate (the child’s diabetes risk was higher or much higher than other children’s risk) or underestimated (the child’s diabetes risk was the same, somewhat lower, or much lower than other children’s risk).
Maternal Belief That Diabetes Risk Can Be Reduced
At the 6- and 15-month study visits, mothers were asked if they believe they can do something to reduce their child’s risk for developing type 1 diabetes. Responses were provided on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree).
Maternal Actions to Prevent Diabetes
At the 6- and 15-month study visits, mothers were asked the following in questionnaire format: “Sometimes people do things to try to stop their child from getting diabetes. Sometimes people do nothing special to try to prevent diabetes in the child. Have you done anything to try to stop or prevent your child from getting diabetes?” If the mother responded “yes,” she was asked to list the actions she had taken. Her response(s) were then coded into 105 possible actions. Each response was coded into only one action; however, if mothers provided more than one response, multiple actions were coded. For data analysis purposes, codes that represented similar themes were collapsed into eight categories: 1) breast-feeding (e.g., increasing duration of breast-feeding); 2) diet (e.g., decreased sweet consumption, avoided cow’s milk; dietary changes other than breast-feeding), 3) dietary supplements (e.g., gave probiotics, gave vitamin D); 4) illness prevention (e.g., protected child from germs by using antibacterial soap); 5) alternative medicine (e.g., child had acupuncture); 6) physical activity (e.g., encouraged exercise); 7) stress reduction (e.g., avoided stressful situations for child); and 8) other. Preventive actions were coded into only one category.
Statistical Analysis
McNemar test was used to determine whether the frequency of maternal reports of actions to prevent type 1 diabetes significantly changed from 6 to 15 months. Univariate analyses were initially conducted to examine sociodemographic and psychological characteristics of mothers who did and did not report actions to prevent diabetes in their child. Differences in the frequency of actions to prevent diabetes across sociodemographic variables, maternal psychological functioning, and diabetes-specific beliefs were performed using χ2 tests. Independent two-sample t tests examined for significant differences in continuous variables between children whose caregivers reported an action to prevent type 1 diabetes compared with other children. Hierarchical logistic regression was used to identify a best final model of those unique characteristics that best differentiated mothers who reported engaging in behaviors to prevent diabetes in the child from mothers who did not. A hierarchical modeling approach enters variables in logically connected blocks, with blocks and their order of entry selected on an a priori basis. In this way, the statistical examination of each successive block of variables represents the contribution of those variables over and above the preceding blocks. In the current hierarchical model, variables were entered beginning with the most general demographic variables, followed by variables hypothesized to be most related to the outcome. In particular, the following blocks were entered: 1) sociodemographic factors, 2) maternal psychological factors (anxiety about the child’s diabetes risk and depression), and 3) maternal diabetes-specific cognitive factors (diabetes risk perception and belief that diabetes risk can be reduced). P values <0.05 were considered statistically significant and were retained, whereas nonsignficant variables were removed from the regression. Only participants with complete data for all variables were retained in this analysis (7,108 at 6 months and 6,144 at 15 months). All analyses were performed using SAS 9.3.
Results
Frequency of Actions to Prevent Diabetes
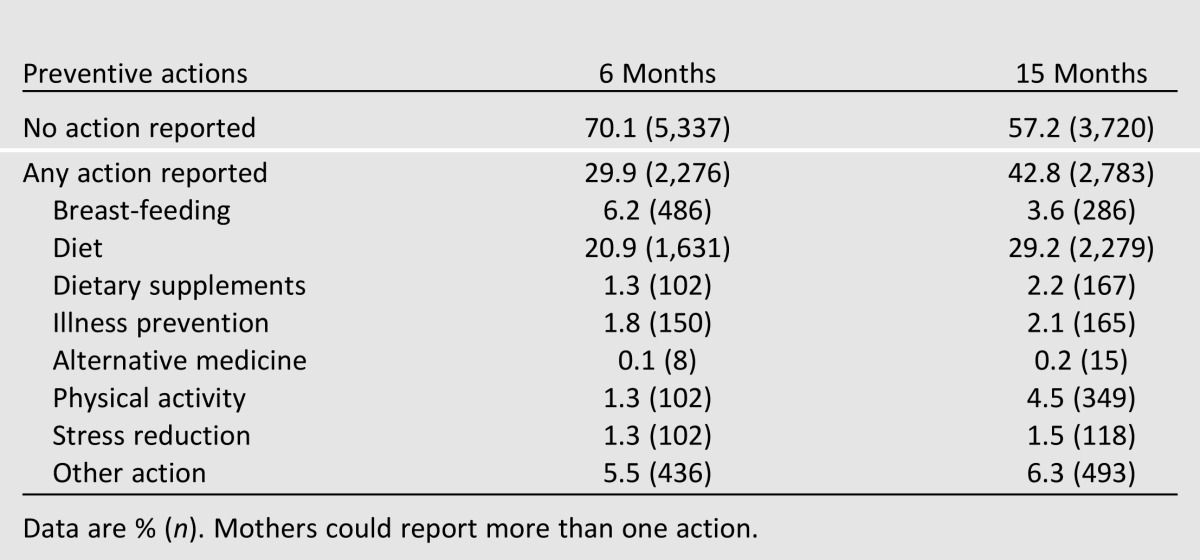
Overall, 29.9% of mothers reported at least one action to prevent type 1 diabetes at 6 months, and 42.7% reported at least one action at 15 months. Dietary changes were most commonly reported, followed by breast-feeding duration and increased physical activity (at 15 months) (Table 1). The specific type of dietary change reported most often was reduction of sweets/carbohydrates, with 31.5 and 46% of those reporting a dietary change specifying this type of action at 6 and 15 months, respectively (data not shown). To test the statistical significance of the increase in the percentage of mothers reporting actions to prevent type 1 diabetes at 6 and 15 months, the data were restricted to those who completed both the 6-month and 15-month study visits (n = 6,303). Seven percent of mothers who reported at least one action to prevent diabetes at 6 months did not report any action at 15 months. At 15 months, 19.8% of mothers reporting taking a preventive action had not reported an action at 6 months, whereas 22.6% reported an action at both 6 and 15 months. Thus, the significant increase at the 15-month visit compared with the 6-month visit (P < 0.001) was largely due to additional mothers reporting an action to prevent diabetes.
Table 1.
Actions to prevent type 1 diabetes by category
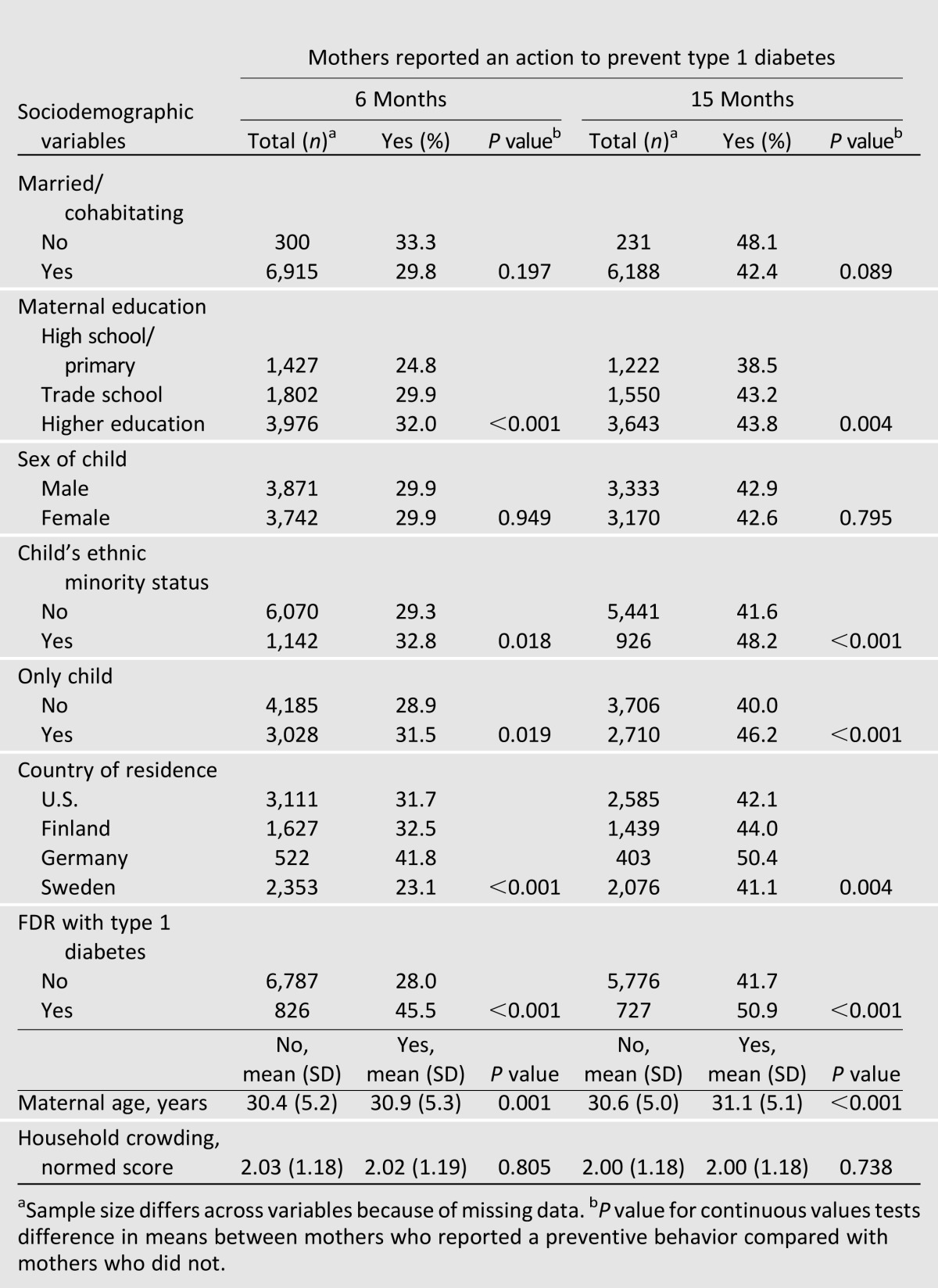
Univariate analyses showed significant differences in many of the sociodemographic variables between mothers who did and did not report actions to prevent diabetes at both the 6- and 15-month study visits (Table 2). At both study time points, the children of mothers who reported actions to prevent type 1 diabetes were more likely to be only children, be from an ethnic minority, and have an FDR with type 1 diabetes. These mothers were older and more educated. Compared with other countries, mothers from Sweden were less likely to report actions to prevent diabetes. Child sex and household crowding were unrelated to whether mothers reported actions to try to prevent type 1 diabetes. We found no statistical differences at 6 or 15 months in rates of preventive behaviors reported by mothers with type 1 diabetes or mothers from a family in which the father had type 1 diabetes.
Table 2.
Sociodemographic variables associated with actions to prevent diabetes
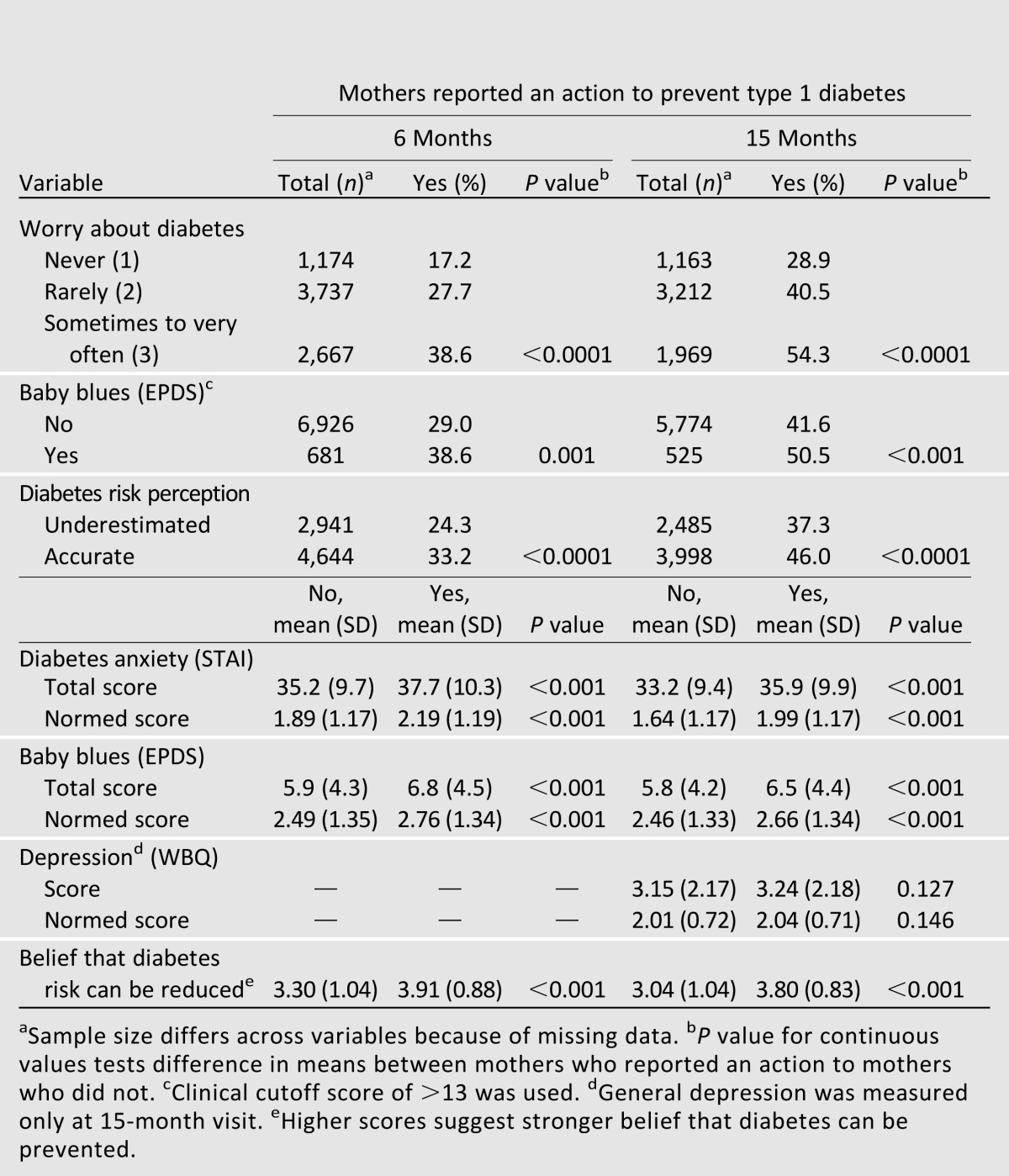
Except for the general depression measure (WBQ) administered at the 15-month study visit, all of the psychological and diabetes-specific cognitive variables were significantly associated with mothers’ report of actions to prevent type 1 diabetes in the univariate analyses (Table 3). Mothers who reported actions to prevent the disease were more anxious about their child’s risk of getting type 1 diabetes, more worried about diabetes, and more accurate in their risk perceptions; had higher postnatal depression scores; and believed more strongly that they could do something to prevent diabetes. The item assessing worry about diabetes also was excluded from the regression modeling because of high multicollinearity (data not shown) with the anxiety (STAI) items.
Table 3.
Caregiver psychosocial variables associated with actions to prevent diabetes
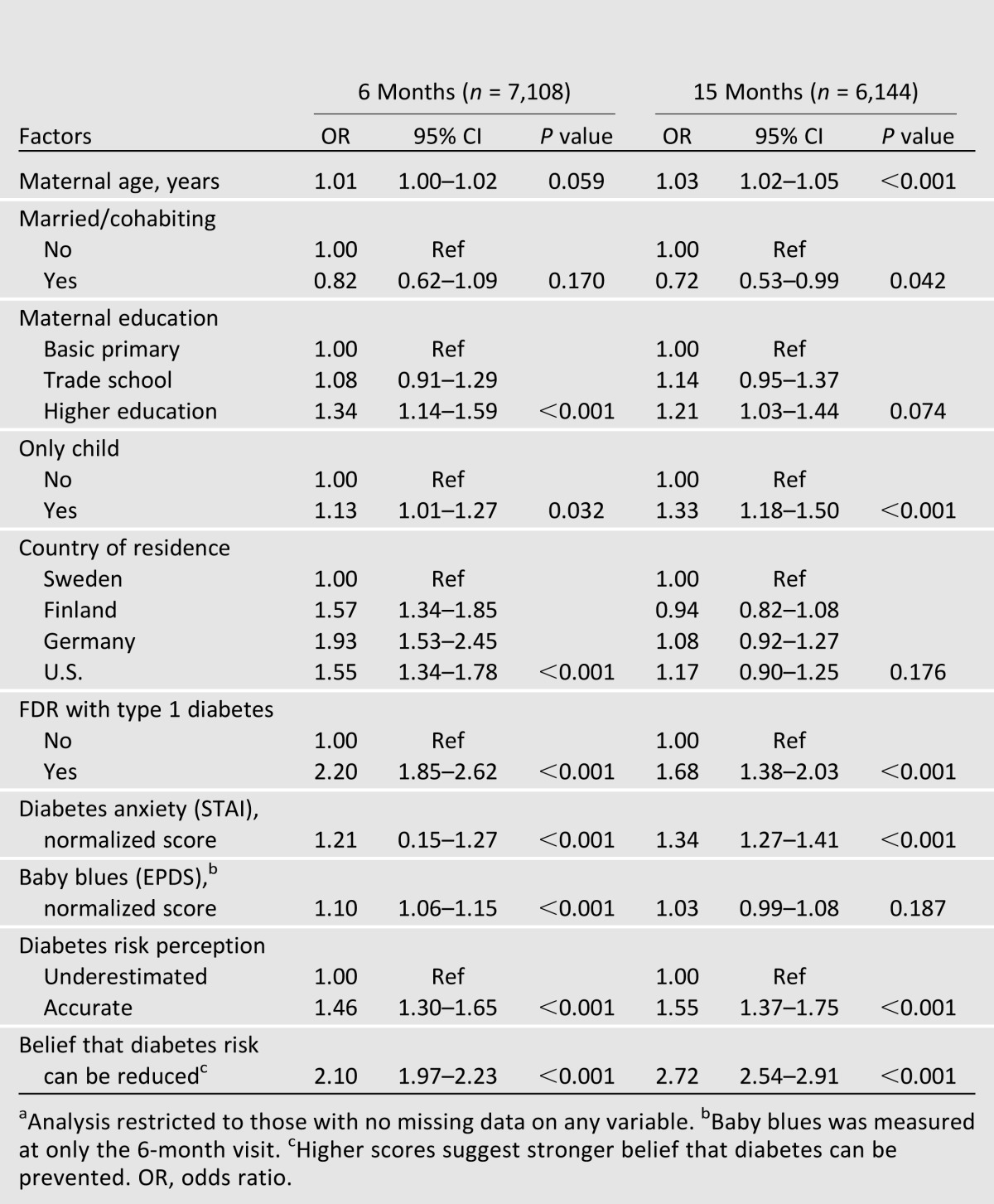
Hierarchical logistical regression was used to identify those variables that uniquely discriminated between mothers who did and did not report actions to prevent type 1 diabetes at both the 6- and 15-month visits. Each successive block of the regression controlled for the preceding variables in the model (see the final model in Table 4). In the first block of the regression, including sociodemographic variables, mothers from Sweden were significantly less likely to report actions to prevent type 1 diabetes than mothers from other countries at 6 months; however, this was no longer the case at 15 months. Only child status, minority group membership, and having an FDR with type 1 diabetes also were predictive of mothers reporting an action to prevent type 1 diabetes at both 6 and 15 months. Older maternal age and higher levels of maternal education were predictive of mothers reporting engaging in preventive behaviors in the multivariate analysis at both the 6-month and 15-month visit. In the second block of the regression, higher maternal anxiety (STAI) and higher baby blues (EPDS) were predictive of actions to prevent diabetes at both the 6- and 15-month visits. Baby blues (EPDS) scores also predicted actions to prevent diabetes at both study visits. With the addition of the anxiety score (STAI), ethnic minority was no longer a significant predictor of actions to prevent diabetes. In the final block of the regression, both an accurate perception of diabetes risk and higher maternal belief that diabetes can be prevented were predictive of actions to prevent diabetes at both time points when controlling for demographic and psychological variables. With the addition of these two diabetes-specific cognitive variables, baby blues and maternal education were no longer significant predictors at the 15-month visit.
Table 4.
Final block of multiple logistic regression analysis of factors associated with mothers reporting preventive behavior at 6 and 15 monthsa
Conclusions
Findings of this study suggest that a large proportion (29.9–42.8%) of mothers in the first year of the TEDDY study reported engaging in actions intended to prevent type 1 diabetes. Dietary changes, such as reducing the child’s sugar or carbohydrate intake, were the most common category of behavior reported by caregivers, with 20.9 and 29.2% of those engaging in any preventive behavior reporting this type at 6 and 15 months, respectively. It is notable that even with infants and toddlers who generally eat a somewhat limited variety of foods because of their developmental level, mothers are endorsing dietary changes as a behavior intended to reduce the risk of type 1 diabetes. In addition to dietary behaviors, mothers also frequently reported increasing physical activity and increasing the duration of breast-feeding to prevent type 1 diabetes. Data from this study do not provide information about why caregivers engage in certain types of preventive behaviors. Caregivers may access studies focusing on the etiology of type 1 diabetes and that often examine dietary factors, in particular breast milk, as potential contributing factors. Given that carbohydrate reduction and physical activity are common preventive behaviors, families may adopt behaviors used to prevent type 2 diabetes. Perhaps families glean health information from popular press sources, which tend to focus on the prevention of type 2 diabetes. Overall, rates and types of preventive behaviors found in the TEDDY study reiterate findings from the PANDA and DPT-1 studies, which also showed that preventive actions were common among parents of children at risk for type 1 diabetes (4–6). However, the current study replicates these findings within a much larger prospective sample and provides data on the occurrence of these preventive behaviors over time.
There were important international differences in this phenomenon as well, with mothers from Germany being most likely to report preventive behaviors and mothers from Sweden being least likely to report these behaviors. It may be that mothers from different countries receive different health-related information (e.g., more emphasis on extended breast-feeding, increased focus on dietary supplements such as vitamin D). Furthermore, the higher frequency of preventive actions reported by German mothers may be related to the fact that more participants with an FDR with type 1 diabetes were recruited from Germany compared with other TEDDY sites, and positive FDR status was significantly related to increased frequency of actions to prevent type 1 diabetes. It is somewhat surprising that mothers of children with an FDR with type 1 diabetes are more likely to engage in preventive behaviors given that they likely have more knowledge about the condition and potential influencing factors (i.e., the lack of evidence that behaviors prevent type 1 diabetes). However, it may be that these mothers are more invested in preventing their child from developing type 1 diabetes given their personal family experience with the condition. Regardless of whether a child’s mother or father has diabetes, rates of preventive behaviors do not change significantly and continue to be higher than that of families in the general population. This suggests that any firsthand experience with type 1 diabetes is related to more preventive behaviors. Overall, the frequency of behaviors intended to prevent type 1 diabetes increased over time, which suggests that mothers continue to believe it is important to make attempts to prevent type 1 diabetes as their child grows older. This increase may in part be due to more opportunities for mothers to change behaviors as their child ages. For example, although it is difficult to increase the physical activity of a young infant, as children become mobile mothers can more easily encourage additional activity if they choose.
In our examination, a number of demographic and psychosocial variables were related to actions to prevent type 1 diabetes reported by caregivers. At both time points, older mothers, those with more education, those with an FDR with type 1 diabetes, mothers from countries other than Sweden, mothers of an child in an ethnic minority, and mothers with only one child were more likely to report engaging in a preventive action. In addition, most psychological variables—type 1 diabetes risk perception, belief in the ability to prevent type 1 diabetes, caregiver anxiety, and postpartum depression—were related to the report of actions to prevent type 1 diabetes at both time points. General depression measured at 15 months was not related to actions to prevent type 1 diabetes, although postpartum depression was related to these actions. This may suggest that general depression is not a correlate of preventive behaviors, or it may be that a measure of depression on a general well-being scale is not sensitive enough to relate to this phenomenon.
Findings from the hierarchical regression models suggest that psychological variables accounted for some of the differences in reports of preventive behaviors among various sociodemographic groups. For example, ethnic minority status was not a significant predictor with the addition of the maternal anxiety about diabetes measure (block 2 of the regression; data not shown). This suggests that ethnic minority status affects actions to prevent diabetes because of mothers’ increased anxiety. Furthermore, caregiver education, marital status, country of residence, and baby blues were no longer significantly related to actions to prevent diabetes at 15 months when diabetes-specific cognitive variables were included in the final block of the model. This indicates that differences in beliefs about the ability to prevent type 1 diabetes account for the differences seen previously between groups based on these sociodemographic and psychological variables. Overall, findings suggest that the most important factors related to preventive behaviors are 1) having an FDR with type 1 diabetes, 2) having an accurate perception of the child’s risk of type 1 diabetes, and 3) believing that diabetes risk can be reduced. The belief that type 1 diabetes risk can be reduced was the strongest predictor of whether mothers engaged in preventive behaviors. This is not surprising given that beliefs about the outcome of a behavior strongly predict whether a person will engage in that behavior, as hypothesized by the Health Belief Model (13,14).
Future research should determine whether mothers who report engaging in actions intended to prevent type 1 diabetes do in fact make these changes. For example, it is unclear whether children of mothers who report reducing carbohydrate or sugar intake actually consume less of these nutrients than children whose mothers do not report this change. Although subjective caregiver reports of behavioral change are important to document, objective measures of behavior change are needed to confirm the validity of these reports. In addition, over the course of the study some children developed type 1 diabetes–related autoantibodies, which further increased their risk of developing the disease. At the time of seroconversion, families are notified of their child’s increased risk, and this may affect their attempts to prevent type 1 diabetes. Furthermore, results of this study raise questions about how participation in a longitudinal observational trial may influence behaviors that are of interest to researchers. It will be important to examine rates of actions intended to prevent type 1 diabetes vis-à-vis the development of autoantibody positivity and type 1 diabetes over time. Given the relatively high rate of preventive behaviors found in this study, it is important for researchers to be cognizant of this phenomenon and to measure these behaviors in future observational studies.
Supplementary Material
Article Information
Funding. This study was funded by DK-63829, 63861, 63821, 63865, 63863, 63836, and 63790; UC4DK095300; and Contract No. HHSN267200700014C from the National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Allergy and Infectious Diseases, National Institute of Child Health and Human Development, National Institute of Environmental Health Sciences, Juvenile Diabetes Research Foundation, and the Centers for Disease Control and Prevention.
Duality of Interest. No potential conflicts of interest relevant to this article were reported.
Author Contributions. L.B.S. formulated the research questions, researched data, and wrote the manuscript. K.F.L. conducted the analyses, contributed to the discussion, and wrote the manuscript. J.B. and T.S. reviewed and edited the manuscript. B.L. and R.R. contributed to the discussion and reviewed and edited the manuscript. S.B.J. developed and formulated the research questions, contributed to the discussion, and reviewed and edited the manuscript. L.B.S. and K.F.L. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Prior Presentation. Portions of this study were presented in poster form at the 72nd Scientific Sessions of the American Diabetes Association, Philadelphia, PA, 8–12 June 2012.
Footnotes
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc13-0449/-/DC1.
A complete list of the members of the TEDDY Study Group can be found in the Supplementary Data online.
References
- 1.Marteau TM, French DP, Griffin SJ, et al. Effects of communicating DNA-based disease risk estimates on risk-reducing behaviours. Cochrane Database Syst Rev 2010;10:CD007275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Heshka JT, Palleschi C, Howley H, Wilson B, Wells PS. A systematic review of perceived risks, psychological and behavioral impacts of genetic testing. Genet Med 2008;10:19–32 [DOI] [PubMed] [Google Scholar]
- 3.Vernarelli JA, Roberts JS, Hiraki S, Chen CA, Cupples LA, Green RC. Effect of Alzheimer disease genetic risk disclosure on dietary supplement use. Am J Clin Nutr 2010;91:1402–1407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Baughcum AE, Johnson SB, Carmichael SK, Lewin AB, She JX, Schatz DA. Maternal efforts to prevent type 1 diabetes in at-risk children. Diabetes Care 2005;28:916–921 [DOI] [PubMed] [Google Scholar]
- 5.Johnson SB, Baughcum AE, Hood K, Rafkin-Mervis LE, Schatz DA, DPT-1 Study Group Participant and parent experiences in the parenteral insulin arm of the diabetes prevention trial for type 1 diabetes. Diabetes Care 2007;30:2193–2198 [DOI] [PubMed] [Google Scholar]
- 6.Johnson SB, Baughcum AE, Rafkin-Mervis LE, Schatz DA, DPT-1 Study Group Participant and parent experiences in the oral insulin study of the Diabetes Prevention Trial for Type 1 Diabetes. Pediatr Diabetes 2009;10:177–183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.TEDDY Study Group The Environmental Determinants of Diabetes in the Young (TEDDY) study: study design. Pediatr Diabetes 2007;8:286–298 [DOI] [PubMed] [Google Scholar]
- 8.Johnson SB, Lee HS, Baxter J, Lernmark B, Roth R, Simell T, TEDDY Study Group The Environmental Determinants of Diabetes in the Young (TEDDY) study: predictors of early study withdrawal among participants with no family history of type 1 diabetes. Pediatr Diabetes 2011;12:165–171 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Spielberger CD, Gorsuch RL, Lushene R. Test Manual for the State-Trait Anxiety Inventory. Palo Alto, CA, Consulting Psychologists Press, 1970 [Google Scholar]
- 10.Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry 1987;150:782–786 [DOI] [PubMed] [Google Scholar]
- 11.Wisner KL, Parry BL, Piontek CM. Clinical practice. Postpartum depression. N Engl J Med 2002;347:194–199 [DOI] [PubMed] [Google Scholar]
- 12.Bradley C. The well-being questionnaire. In: Handbook of Psychology and Diabetes: A Guide to Psychological Measurement in Diabetes Research and Practice. Bradley C, Ed. London, U.K., Routledge, 1994, p. 89–109 [Google Scholar]
- 13.Rosenstock IM. Why people use health services. Milbank Mem Fund Q 1966;44:94–127 [PubMed] [Google Scholar]
- 14.Roth R. Psychological and ethical aspects of prevention trials. J Pediatr Endocrinol Metab 2001;14(Suppl. 1):669–674 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.