

Abstract
OBJECTIVE
To test the hypothesis that high levels of plasminogen-activating inhibitor (PAI)-1 and fibrinogen at baseline were associated with the onset or progression of diabetic retinopathy (DR) during the Veterans Affairs Diabetes Trial (VADT).
RESEARCH DESIGN AND METHODS
The VADT was an open-label, prospective, randomized controlled trial to test the effect of standard glycemic control (STD) compared with intensive control (INT) on cardiovascular events in patients with advanced type 2 diabetes mellitus (T2DM). Diabetic retinopathy (DR) outcomes were also collected. Incidence and progression of DR were assessed by grading seven-field stereoscopic fundus photographs at baseline and 5 years later taken in 858 of a total of 1,791 participants who completed both eye examinations.
RESULTS
Assignment to INT was not independently associated with decreased risk of onset of DR. However, after adjustment for multiple covariates, baseline level of PAI-1 was an independent risk factor for the onset of DR. The risk for incidence of DR increased by 12% for each 10 ng/dL increase in baseline PAI-1 concentration (odds ratio [OR] 1.012 [95% CI 1.00–1.024], P = 0.042). Assignment to INT was not independently associated with decreased risk of progression of DR. However, there was an interaction between glycemic treatment assignment and fibrinogen level at baseline. INT was associated with decreased progression of retinopathy in those with fibrinogen <296 mg/dL (OR 0.55 [95% CI 0.31–1.00], P = 0.03).
CONCLUSIONS
The results require confirmation but are consistent with greater hypercoagulabilty and inflammation, as measured by higher levels of PAI-1 and fibrinogen, being related to DR and responsiveness to INT.
Introduction
The prevalence of type 2 diabetes mellitus (T2DM) has increased to epidemic proportions in recent decades. Worldwide, the number of patients with T2DM is estimated to rise from 220 million in 2010 to 366 million in 2030 (1). The overall prevalence of any diabetic retinopathy (DR) in a large meta-analysis was 34.6% (2). Twenty-one percent of patients have retinopathy at the time of diagnosis of T2DM (3), and the incidence of retinopathy rises to 60% within the next two decades after diagnosis (4). Glycemic control remains the foundation for diabetes mellitus (DM), and it was shown to reduce the progression of retinopathy in both type 1 DM and newly diagnosed T2DM (5,6).
Hemostatic and inflammatory markers, such as serum fibrinogen (7) and plasminogen-activating inhibitor (PAI)-1 (8,9), have an established relationship with macrovascular disorders in subjects with and without DM. However, their association with microvascular disorders is somewhat controversial. It is plausible that high levels of these hemostatic factors might be associated with DR, since these factors lead to microvascular inflammation and occlusion, which participate in the genesis of DR. Our objective was to test the hypothesis that high baseline levels of PAI-1 and fibrinogen were associated with the onset or progression of DR and to determine whether there was an interaction between intensive glycemic control (INT) and these hemostatic factors with regard to onset or progression of DR, using data from the Veterans Affairs Diabetes Trial (VADT).
Research Design and Methods
VADT was an open-label prospective, randomized controlled trial targeting patients with inadequately controlled T2DM, and the details of study design have previously been reported (10,11). Briefly, 1,791 patients with T2DM with inadequate response to maximal doses of oral agents or insulin therapy were included and randomized to either a standard glycemic-management arm (STD) in which an HbA1c of 8.4% was achieved or an INT in which an HbA1c of 6.9% was achieved. Of 1,791, 865 individuals completed seven-field stereo fundus photographs at baseline and 5 years later. Of these, 7 individuals had some necessary baseline data missing, so this report uses data from the remaining 858 patients.
Fibrinogen and PAI-1 Assays
Fibrinogen was assessed by using thrombin to convert fibrinogen to fibrin. The coefficient of variation was 1.2% with the replicate samples, 2.8% in sequential studies of a single purified bovine fibrinogen pool, and 4.7% for lyophilized commercial plasma (12). An ELISA was used to assess PAI-1 level. The lower sensitivity of the assay was 2 ng/mL. The intra-assay, interassay, and interdilution coefficients of variation were 5.2%, 8.0%, and 7.1%, respectively (13). The assay is 12-fold more sensitive to detect free PAI-1 compared with the PAI-1/tPA. In platelet-poor plasma, a linear correlation (r = 0.80) was present between PAI-1 activity and PAI-1 antigen.
Assessment of Eye Complications
Seven-field stereoscopic color photographs of the retina were obtained at baseline and at 5 years by certified photographers in participating hospitals (14,15). The fundus photographs were centrally assessed by trained personnel at the Department of Ophthalmology and Visual Sciences, University of Wisconsin, Madison. The readers were blinded to subject attributes, including glycemic treatment assignment. The 23-level Early Treatment Diabetic Retinopathy Study (ETDRS) DR severity scale was used to define the incidence and progression of DR (3). Each eye was graded for retinopathy lesions individually, independent of the grading of the other eye. Incidence of DR was defined in subjects who had ETDRS severity 10 (absence of microaneurysms and other characteristics of DR) at baseline and who developed three or more retinal microaneurysms in one or both eyes or who developed level 31 or worse on the ETDRS scale at the 5-year follow-up visit. Progression of DR was defined as a two-step change in ETDRS severity in either eye between baseline and the 5-year follow-up visit.
Statistical Analysis
We first assessed the relationship of onset and progression of DR with a large number of baseline variables in a single logistic analysis for each variable. The variables included assignment to intensive treatment, age at onset of DM, duration of DM, sex, ethnicity, BMI, insulin treatment at baseline, blood pressure, lipid profile, glycemic control as measured by HbA1c, pancreatic reserve as measured by C-peptide, fibrinogen, PAI-1, prior cardiovascular events, presence of baseline DR, history of photocoagulation, history of vitrectomy, history of cataract surgery, presence of clinically significant macular edema, albuminuria, and estimated glomerular filtration rate (eGFR) (Table 1).
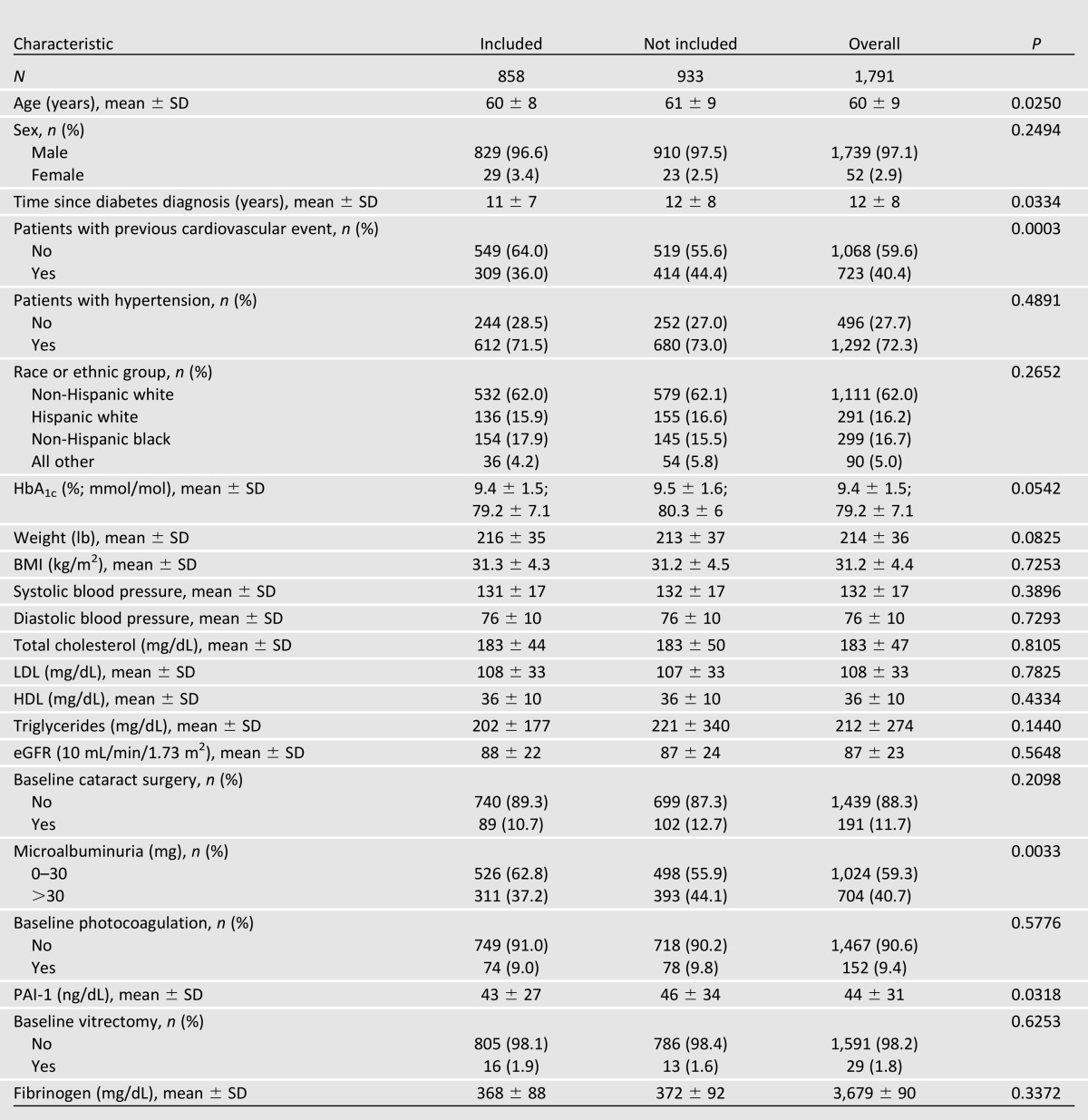
Table 1.
Baseline demographics and clinical characteristics of those included and not included in this study
Among these baseline risk factors, the most relevant variables to the outcome variables, the onset and progression of DR, were selected for following. For both progression and incidence, a multiple logistic regression model was used to determine baseline predictors of on-study retinopathy. The model selection procedure was as follows: After univariate analyses were performed on each outcome of interest using logistic regression, each covariate with treatment interactions was tested separately in logistic regression. The predictor variables and the treatment interactions with P value ≤0.2 were selected as candidates in the multiple logistic regression models, and backward elimination was performed with a cutoff P value of <0.07. According to the hypothesis, this paper focused on two hemostatic and inflammatory factors, PAI-1 and fibrinogen, adjusting for other covariates in the final model. No interaction effect between covariates was allowed to enter the model without the corresponding main treatment effects. The data analysis was generated using version 9.2 of the SAS system for Windows (Cary, NC).
Results
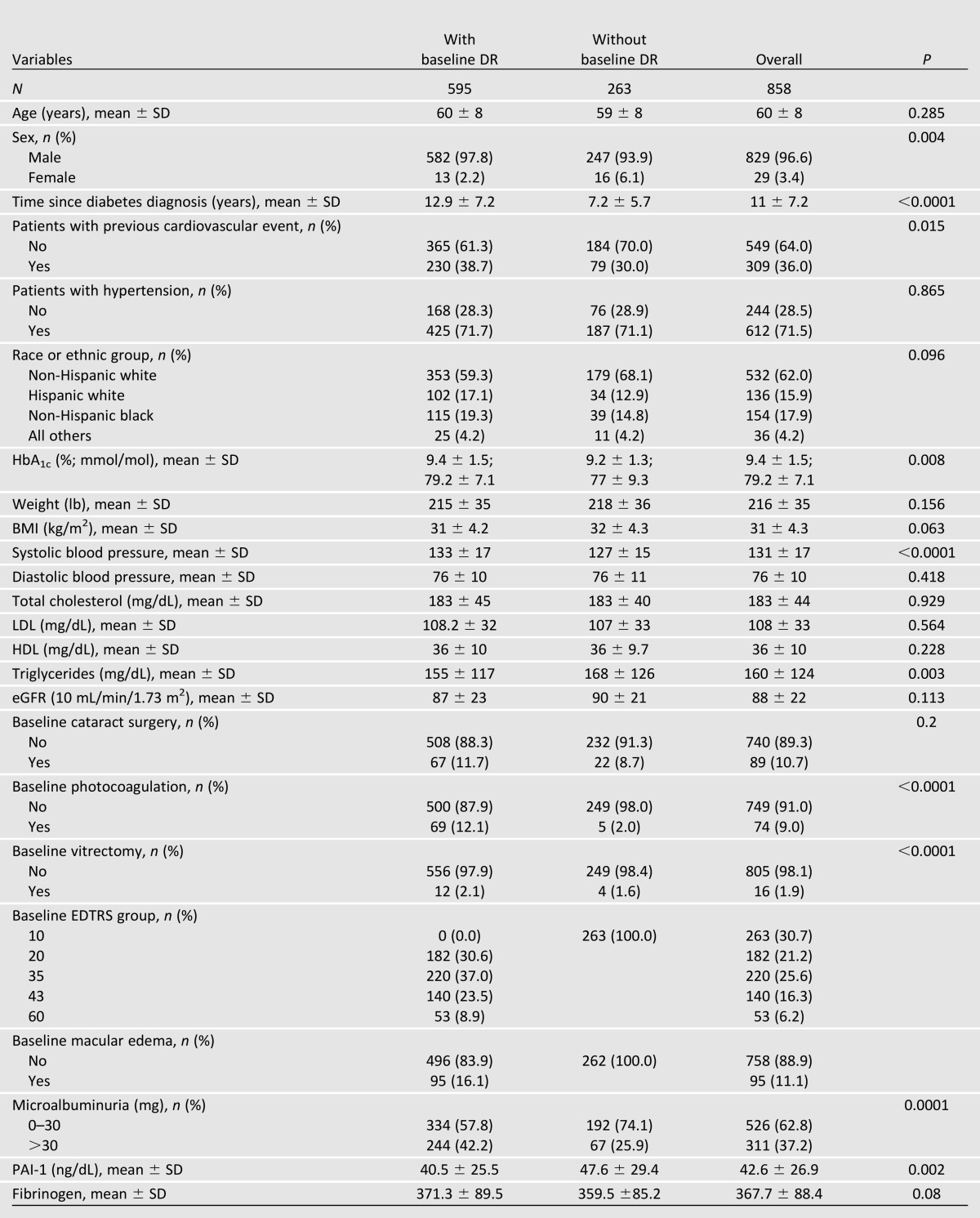
Table 1 shows that the individuals whose fundi were photographed and gradable for DR at baseline and 5 years were largely representative of the VADT cohort as a whole. Statistically significant differences between those included in this analysis and those excluded were relatively small and not likely of clinical significance. Table 2 compares the characteristics of those with and without DR at baseline. Not surprisingly, those with baseline DR had longer duration of DM, more macrovascular disease, higher systolic blood pressure, and slightly higher HbA1c. They had lower triglycerides and lower PAI-1.
Table 2.
Baseline demographics and clinical characteristics of those with and without baseline DR
Onset of DR During the Study
Of the 858 evaluable patients, 263 were free from DR at the onset of the study. Of these 263, 202 had all available data and were used for this analysis. Over the 5 years between photographs, 96 patients developed DR.
Assignment to INT was not independently associated with decreased risk of onset of DR. However, after adjustment for covariates, baseline level of PAI-1 was an independent risk factor for the incidence of DR. The risk for incidence of DR increased by 12% for each 10 ng/dL increase in baseline PAI-1 concentration (odds ratio [OR] 1.012 [95% CI 1.000–1.024], P = 0.0417) after controlling for other variables. This analysis was adjusted for age, LDL cholesterol, HDL cholesterol, albuminuria, and C-peptide.
Progression of DR During the Study
Of the 595 evaluable patients who had DR at baseline, 536 had all the data and were included in the analysis. During the 5-year observation period, 106 had progression of DR.
Neither PAI-1 nor fibrinogen was a significant predictor of progression of DR. Assignment to INT was also not independently associated with decreased risk for progression of DR. However, there was an interaction between glycemic treatment assignment and fibrinogen level at baseline. As shown in Fig. 1, INT was associated with decreased progression of retinopathy in those with fibrinogen <296 mg/dL (OR 0.55 [95% CI 0.31–1.00], P = 0.0347) after adjustment for other covariates. This analysis was adjusted for HbA1c, C-peptide, history of cataract surgery, and total cholesterol.
Figure 1.

The solid line represents the point estimate of the treatment ORs at various levels along the x-axis that ranges from the minimum to the maximum observed value, while the dotted lines represent the 95% CIs. INT was associated with decreased progression of retinopathy in those with fibrinogen <296 mg/dL (OR 0.55 [95% CI 0.31–1], P = 0.0347).
Conclusions
An altered coagulation pathway and high plasma levels of coagulation and fibrinolytic factors are accepted as important risk factors for the occurrence of coronary heart disease in individuals with or without DM (7–9). Plasminogen activator inhibitor-1 participates in the regulation of fibrinolysis. It has been shown that PAI-1 is a predictor of incidence of coronary heart disease (8,9,16), is an independent predictor of incidence of DM (17), and is associated with insulin resistance (18).
In addition to its association with macrovascular disease, there are data linking PAI-1 with microvascular disease as well. A number of prior studies had examined the cross-sectional association between circulating levels of PAI-1 and DR with inconsistent findings (rev. in 19). However, Brazionis et al. (19) found that a higher level of PAI-1was independently associated with a lower risk for DR, while it was positively correlated with a higher incidence of coronary artery disease. In light of most, but not all, studies, our data are not surprising. PAI-1 activity directly measured in retinal tissue was significantly higher in DM subjects compared with those of a control group (20). Furthermore, the same authors observed a positive correlation between expression of PAI-1 in the retina and the intensity of DR in a DM rabbit model (20). Erem et al. (21) reported a significantly higher level of plasma PAI-1 in DM subjects with DR compared with those without DR. We found that a high level of PAI-1 at baseline was an independent risk factor for the onset of DR during the VADT, even after adjustment for other relevant predictors including age, LDL cholesterol, HDL cholesterol, albuminuria, and C-peptide. This finding allows speculation that a propensity to hypercoagulabilty and probably increased inflammation, evidenced by higher PAI-1, may have a deleterious effect on the retinal vasculature in people with DM.
Fibrinogen is another coagulation factor that is involved in diabetic vascular disease. Fibrinogen has multiple roles in the pathogenesis of arteriosclerosis. Hyperfibrinogenemia enhances coagulation activity, and it is associated with blood hyperviscosity. Fibrinogen is a cofactor in the platelet activation process, and it may be directly involved in plaque formation where fibrinogen is converted to fibrin and fibrinogen degradation product. Hyperfibrinogenemia is also an indicator of inflammatory changes, which result in endothelial dysfunction (22–24). In addition, hyperfibrinogenemia may also be an indirect marker of an unstable vascular lesion with subintimal hemorrhage. Moreover, high levels of inflammatory markers such as fibrinogen and its independent association with cardiac mortality and morbidity have been reported in the past (25,26).
In addition to its implications in macrovascular disease, fibrinogen may also participate in the genesis of microvascular complications in DM. Data from Japan in subjects with T2DM demonstrated an independent association between serum fibrinogen and DR after adjustment with various covariates (27). A multiethnic study of atherosclerosis in DM subjects (type not stated) found a significant correlation between retinopathy and serum fibrinogen level after adjustment of the data for all the conventional markers of atherosclerosis except serum creatinine; however, addition of serum creatinine to the other markers weakened the correlation (28). The relationship between fibrinogen and retinopathy may not hold true in people with type 1 DM (8,29). To our knowledge, ours is the first study showing that INT in subjects with T2DM and lower fibrinogen was associated with a decrease in the progression of DR but not in DM individuals with higher fibrinogen level who presumably had a higher propensity to abnormal coagulation and inflammation (Fig. 1).
The limitations of this study are that it is a post hoc analysis of a cohort consisting mainly of males with advanced T2DM. Therefore, the findings may not be generalizable to a broader population of people with DM.
In summary, we found that a high baseline level of PAI-1 was an independent risk factor for the onset of DR. While INT was not associated with decreased risk of onset or progression of DR in the VADT cohort as a whole, there was a heretofore unrecognized interaction between INT and fibrinogen levels at baseline in that INT was associated with a beneficial effect on progression of DR in those with lower fibrinogen levels. Our data support the idea that patients with a high propensity for coagulation and vascular inflammation, demonstrated by elevated levels of PAI-1, are more likely to develop DR. Furthermore, there may be a differential retinal response to INT depending on the intensity of hypercoagulability and inflammation manifested by circulating fibrinogen concentration.
Article Information
Funding. This study was sponsored by the Cooperative Studies Program of the Department of Veterans Affairs Office of Research and Development. This study also received generous support from the National Eye Institute.
Duality of Interest. Medications and financial support were provided by Sanofi, GlaxoSmithKline, Novo Nordisk, Roche, Kos Pharmaceuticals, Merck, and Amylin. No other potential conflicts of interest relevant to this article were reported.
These companies had no role in the design of the study, in the accrual or analysis of the data, or in the preparation or approval of the manuscript.
Author Contributions. N.A., L.A., and N.V.E. researched data and wrote the manuscript. R.K. reviewed and edited the manuscript. G.D.B. conducted the statistical analysis. M.M. contributed to the initial design of the study. P.R. and R.H. reviewed and edited the manuscript. W.D. codesigned the study and reviewed data. N.A. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Clinical trial reg. no. NCT00032487, clinicaltrials.gov.
References
- 1.National Estimates and General Information on Diabetes and Prediabetes in the U.S., 2011 Atlanta, GA, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011
- 2.Yau JW, Rogers SL, Kawasaki R, et al. Meta-Analysis for Eye Disease (META-EYE) Study Group Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012;35:556–564 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Klein R, Klein BEK. Vision disorders in diabetes. In Diabetes in America Hamman R, Harris MWH, Eds. Bethesda, MD, U.S. Health Service NIH Publications, 1983, p. 1–36 [Google Scholar]
- 4.Fong DS, Aiello L, Gardner TW, et al. American Diabetes Association Diabetic retinopathy. Diabetes Care 2003;26:226–229 [DOI] [PubMed] [Google Scholar]
- 5.The Diabetes Control and Complications Trial Research Group The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977–986 [DOI] [PubMed] [Google Scholar]
- 6.UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837–853 [PubMed] [Google Scholar]
- 7.Klein RL, Hunter SJ, Jenkins AJ, et al. DCCT/ECIC STUDY GROUP Fibrinogen is a marker for nephropathy and peripheral vascular disease in type 1 diabetes: studies of plasma fibrinogen and fibrinogen gene polymorphism in the DCCT/EDIC cohort. Diabetes Care 2003;26:1439–1448 [DOI] [PubMed] [Google Scholar]
- 8.Agirbasli M. Pivotal role of plasminogen-activator inhibitor 1 in vascular disease. Int J Clin Pract 2005;59:102–106 [DOI] [PubMed] [Google Scholar]
- 9.Schneider DJ, Sobel BE. PAI-1 and diabetes: a journey from the bench to the bedside. Diabetes Care 2012;35:1961–1967 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Duckworth W, Abraira C, Moritz T, et al. VADT Investigators Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 2009;360:129–139 [DOI] [PubMed] [Google Scholar]
- 11.Abraira C, Duckworth W, McCarren M, et al. VA Cooperative Study of Glycemic Control and Complications in Diabetes Mellitus Type 2 Design of the cooperative study on glycemic control and complications in diabetes mellitus type 2: Veterans Affairs Diabetes Trial. J Diabetes Complications 2003;17:314–322 [DOI] [PubMed] [Google Scholar]
- 12.Swaim WR, Feders MB. Fibrinogen assay. Clin Chem 1967;13:1026–1028 [PubMed]
- 13.Declerck PJ, Alessi MC, Verstreken M, Kruithof EK, Juhan-Vague I, Collen D. Measurement of plasminogen activator inhibitor 1 in biologic fluids with a murine monoclonal antibody-based enzyme-linked immunosorbent assay. Blood 1988;71:220–225 [PubMed]
- 14.Emanuele N, Moritz T, Klein R, et al. Veterans Affairs Diabetes Trial Study Group Ethnicity, race, and clinically significant macular edema in the Veterans Affairs Diabetes Trial (VADT). Diabetes Res Clin Pract 2009;86:104–110 [DOI] [PubMed] [Google Scholar]
- 15.Emanuele N, Klein R, Mortiz M. Comparison of dilated fundus examination by ophthalmologists, with 7-field stereo photographs in the VADT. J Diabetes Complications 2009;23:323–329 [DOI] [PubMed] [Google Scholar]
- 16.Trost S, Pratley RE, Sobel BE. Impaired fibrinolysis and risk for cardiovascular disease in the metabolic syndrome and type 2 diabetes. Curr Diab Rep 2006;6:47–54 [DOI] [PubMed] [Google Scholar]
- 17.Meigs JB, O’donnell CJ, Tofler GH, et al. Hemostatic markers of endothelial dysfunction and risk of incident type 2 diabetes: the Framingham Offspring Study. Diabetes 2006;55:530–537 [DOI] [PubMed] [Google Scholar]
- 18.Stoney RM, O’Dea K, Herbert HE, et al. Insulin resistance as a major determinant of increased coronary heart disease risk in postmenopausal womwn with type 2 diabetes mellitus. Diabet Med 2001;18:476–482 [DOI] [PubMed] [Google Scholar]
- 19.Brazionis L, Rowley K, Jenkins A, Itsiopoulos C, O’Dea K. Plasminogen activator inhibitor-1 activity in type 2 diabetes: a different relationship with coronary heart disease and diabetic retinopathy. Arterioscler Thromb Vasc Biol 2008;28:786–791 [DOI] [PubMed] [Google Scholar]
- 20.Grant MB, Ellis EA, Caballero S, Mames RN. Plasminogen activator inhibitor-1 over expression in nonproliferative diabetic retinopathy. Exp Eye Res 1996;63:233–244 [DOI] [PubMed]
- 21.Erem C, Hacihasanoğlu A, Celik S, et al. Coagulation and fibrinolysis parameters in type 2 diabetic patients with and without diabetic vascular complications. Med Princ Pract 2005;14:22–30 [DOI] [PubMed] [Google Scholar]
- 22.Stec JJ, Silbershatz H, Tofler GH, et al. Association of fibrinogen with cardiovascular risk factors and cardiovascular disease in the Framingham Offspring Population. Circulation 2000;102:1634–1638 [DOI] [PubMed] [Google Scholar]
- 23.Mendall MA, Patel P, Ballam L, Strachan D, Northfield TC. C reactive protein and its relation to cardiovascular risk factors: a population based cross sectional study. BMJ 1996;312:1061–1065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Low GD, Rumley A. Fibrinogen and its degradation products as thrombotic risk factors. Ann N Y Acad Sci 1997;2:115–125 [DOI] [PubMed] [Google Scholar]
- 25.Saito I, Folsom AR, Brancati FL, Duncan BB, Chambless LE, McGovern PG. Nontraditional risk factors for coronary heart disease incidence among persons with diabetes: the Atherosclerosis Risk in Communities (ARIC) Study. Ann Intern Med 2000;133:81–91 [DOI] [PubMed] [Google Scholar]
- 26.Jager A, van Hinsbergh VW, Kostense PJ, et al. Increased levels of soluble vascular cell adhesion molecule 1 are associated with risk of cardiovascular mortality in type 2 diabetes: the Hoorn study. Diabetes 2000;49:485–491 [DOI] [PubMed] [Google Scholar]
- 27.Fujisawa T, Ikegami H, Yamato E, et al. Association of plasma fibrinogen level and blood pressure with diabetic retinopathy, and renal complications associated with proliferative diabetic retinopathy, in Type 2 diabetes mellitus. Diabet Med 1999;16:522–526 [DOI] [PubMed] [Google Scholar]
- 28.Nguyen TT, Alibrahim E, Islam FM, et al. Inflammatory, hemostatic, and other novel biomarkers for diabetic retinopathy: the multi-ethnic study of atherosclerosis. Diabetes Care 2009;32:1704–1709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Soedamah-Muthu SS, Chaturvedi N, Pickup JC, Fuller JH, EURODIAB Prospective Complications Study Group. The EURODIAB Prospective Complications Study (PCS) Relationship between plasma sialic acid and fibrinogen concentration and incident micro- and macrovascular complications in type 1 diabetes. Diabetologia 2008;51:493–501 [DOI] [PMC free article] [PubMed] [Google Scholar]