

Abstract
Renal injury can occur during sports activity. Although it is, generally, associated with contact trauma, it is known that the renal injury can be developed during training without a direct trauma. The diagnosis of renal injuries should not be based solely on urine analysis. Computed tomography scan is necessary diagnose possible renal injuries.
Key Points.
Renal injuries may develop during sporting activities without a direct trauma.
CT scan is necessary in order to diagnose possible renal injuries and to grade accurately the degree of injury.
Key Words: Renal injury, exercise, computed tomography
Introduction
Although kidneys are well protected organs in the body, their relative mobility could lead to injury by contusion, such as a fractured rib or a sudden decelerating force. The exact incidence of renal trauma during exercise is not clear. Many sports, however, have been identified as generating renal trauma (e.g., football, soccer, rugby, horseback riding, diving, ice skating, hockey, and lacrosse). Those renal injuries are classified according to their anatomical location and pathophysiological severity, namely: renal contusions, caliceal lacerations, and renal fracture and vascular pedicle injuries (Amaral, 1997; Cainflocco AJ, 1992). This report describes a renal injury occurred without a direct trauma.
Case Report
A 45- years-old sedentary man, complained about left costolomber pain and dizziness after lifting a heavy dumbbell at sitting position during first training session of body building exercise. In the emergency room, blood pressure was determined 80/60 mmHg, and pulse was 112 beat per minute. On the admission, there was no history of contact trauma and hemoglobin and hematocrit levels, and urinalysis were all normal. He complained of lumbar pain on the left lumbar region by blunt percussion. He and his family had no history of any disease.
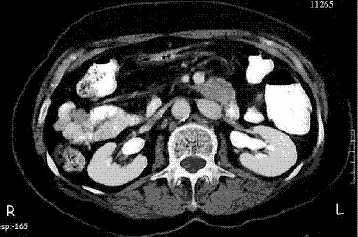
There was no abnormality in the direct radiography and the ultrasonography of abdominal region was also normal. However, the patient was also screened for any possible intraabdominal lesion by contrast computed tomography (CT) scan, and a left subcapsular renal haematoma (Figure 1) was found subsequently. Intravenous analgesia and normal saline were administrated to alleviate the patient’s pain. On the second day, the pain was receded and systolic blood pressure was increased to 120 mmHg. Repeated hemoglobin and hematocrit measurements were not different compared to previous results, and urinalysis and blood tests were also normal. The patient was discharged on the third day and was recommended only to have bed rest. After 3 months of monitoring, control CT scan has demonstrated complete recovery (Figure 2).
Figure 1.

Left subcapsular renal hematoma (arrow).
Figure 2.
Control abdominal computed tomography shows complete recovery.
Discussion
This case report presents a renal injury occurred by an indirect trauma during a sportive activity. Only positive finding was lumbar pain. We hypothesized that the renal injury was developed due to increased intra-abdominal and retro-peritoneal pressure during weight lifting.
Although, there was no abnormality in urinalysis and blood tests, the subject was suffering from mild flank pain. Since, as high as 25% of renal injuries and 60% of renal pedicle injuries may present no hematuria, the absence of hematuria is not conclusive for renal injuries. Renal contusion can occur with hematuria or mild gross hematuria (Amaral, 1997). Although major haemorrhage was not developed, serious hypotension was found on the admission of the patient. We speculated that vasovagal effect due to abdominal pain could have been responsible for that hypotension.
Abdominal ultrasonography is recommended as a first choice to screen renal injuries, since it is cheaper and easier to use than computed tomography scan. On the other hand, however, its sensitivity, specifity and accuracy for staging in those cases are less reliable than the latter (Healy et al., 1995). With or without hematuria, spiral contrast CT scan should be carried out. Abdominal CT is the preferred diagnostic modality in stable patients, because it better delineates renal parenchymal injury, detects extravasations, assesses nonviable tissue, and detects associated injuries (Carpio and Morey, 1999).
Decisions about patient’s treatment are based on the subjective clinical status of him and guided by objective evidence regarding the injury severity. In general, radiographic imaging by CT scan allows accurate grading using the Organ Injury Scaling Committee Guidelines on a scale of grade 1 to 5 (grade 1, microscopic or gross hematuria with only subcapsular haematoma or no abnormality on imaging; grade 2, perirenal haematoma or renal cortical laceration less than 1 cm in depth with no urinary extravasations; grade 3, renal cortical laceration greater than 1 cm in depth with no urinary extravasations; grade 4, renal cortical laceration extending into the collecting system as evidenced by urinary extravasations, renal arterial or venous injury with a contained haematoma, or segmental renal vascular injury; and grade 5, completely shattered kidney or avulsion of the renal hilum) (Moore et al., 1989).
The decision for renal imaging in diagnosing and grading the renal injuries should not be based on urine analysis solely. The patient’s clinical status, history, and injury mechanism should also be considered. Although the vast majority of renal injuries do not require surgical intervention, their accurate grading prompts treatment with surveillance, bed rest, and close in-hospital monitoring (Matthews et al., 1997; Moore et al., 2002).
Conclusions
It can be assumed that renal injuries may develop during sporting activities without a direct trauma. We believe that a CT scan is necessary in order to diagnose possible renal injuries and to grade accurately the degree of those injuries.
Biographies
Erdem KASIKCIOGLU
Employment
Physician, Istanbul Univ., Istanbul Medical School, Department of Sports Medicine, Istanbul, Turkey.
Degrees
MD
E-mail: erkasikci@yahoo.ca
Abidin KAYSERILIOGLU
Employment
Prof., Istanbul Univ., Istanbul Medical School, Department of Sports Medicine, Istanbul, Turkey.
Degrees
MD, Prof.
Ates KADIOGLU
Employment
Prof., Istanbul Univ., Istanbul Medical School, Department of Urology, Istanbul, Turkey.
Degrees
MD, Prof.
References
- Amaral J.F. (1997) Thoracoabdominal injuries in the athlete. Clinical Sports Medicine 16, 739-753 [DOI] [PubMed] [Google Scholar]
- Cainflocco A.J. (1992) Renal complication of exercise. Clinical Sports Medicine 11, 437-451 [PubMed] [Google Scholar]
- Carpio F., Morey A.F. (1999) Radiographic staging of renal injuries. World Journal of Urology 17, 66-70 [DOI] [PubMed] [Google Scholar]
- Healy M.A., Simons R.K., Winchell R.J., Gosink B.B., Casola G., Steele J.T., Potenza B.M., Hoyt D.B. (1996) A prospective evaluation of abdominal ultrasound in blunt trauma: is it useful?. Journal of Trauma 40, 875-883 [DOI] [PubMed] [Google Scholar]
- Matthews L.A., Smith E.M., Spirnak J.P. (1997) Nonoperative treatment of major blunt renal lacerations with urinary extravasation. Urology 15, 2056-2058 [PubMed] [Google Scholar]
- Moore E.E., Shackford S.R., Pachter H.L., McAninch J.W., Browner B.D., Champion H.R., Flint L.M., Gennarelli T.A., Malangoni M.A., Ramenofsky M.L. (1989) Organ injury scaling: spleen, liver, and kidney. Journal of Trauma 29, 1664-1666 [PubMed] [Google Scholar]
- Moore E.E, Shackford S.R., Nguyen M.M., Das S. (2002) Pediatric renal trauma. Urology 59, 762-766 [DOI] [PubMed] [Google Scholar]