

Abstract
The anaerobic threshold (AT) has been defined as the theoretical highest exercise level that can be maintained for prolonged periods. It is of practical importance to the competitive endurance athlete to measure progress and plan training programs. The primary objective of this study was to assess the reliability and validity of breakpoint in the respiratory rate (RR) during incremental exercise as a marker for the AT. Secondary objectives were 1) to assess the reliability of the ventilatory threshold (VE) and ventilatory equivalent (VE/VO2) breakpoint, and 2) to assess differences in these 3 methods for their potential to measure change in fitness, as measured by standard error of measurement (SEM), coefficient of variability (CV), and correlation coefficient (R). Fifteen competitive male cyclists (5 category II, 6 category III, 1 category IV, 3 category V United States Cycling Federation) completed 2 maximal oxygen consumption tests within one week on an electronically braked cycle ergometer. A repeated measures Analysis of Variance using 2x3 design (test and methods) resulted in no significant differences (F = 0.02, p = 0.978), indicating that 1)all 3 methods are reproducible, and 2) RR, when compared to VE and VE/VO2, is a valid method of assessing the anaerobic threshold. The lowest SEM, lowest CV and highest R were obtained with the VE method (SEM = 19.4 watts, CV = 6.7%, R = 0.872), compared to VE/VO2 (SEM = 21.5 watts, CV = 7.4%, R=.811) and RR (SEM = 35.3 watts, CV = 12.2%, R = 0.800). From the results of this study, it is concluded that the RR method is a valid and reliable method for detecting AT. However, due to the relatively high SEM and CV, and low R, when compared to VE and VE/VO2, its insensitivity to small changes seen in highly fit athletes would preclude its use in measuring changes in AT. It appears that either VE or VE/VO2 would be appropriate for measuring AT changes in highly fit athletes.
Key Points.
Respiratory rate is a valid and reliable marker of the anaerobic threshold.
Due to a relatively high standard error of measurement and coefficient of variability for the respiratory rate method, use of ventilation (VE) and ventilatory equivalent for oxygen (VE/VO2 is preferred when assessing changes in anaerobic threshold.
When assessing changes in maximal aerobic capacity, maximal watts has a lower standard error of measurement and coefficient of variability and is preferred over changes in maximal oxygen consumption.
Key Words: Reliability, validity, standard error of measurement, coefficient of variation
Introduction
The use of the anaerobic threshold (AT) for assessing fitness, measuring training progress, and predicting performance is well-documented. While maximal lactate steady state (MLSS) is considered the “gold standard ”in AT assessment (Aunola and Rusko, 1992), several ventilatory parameters, such as ventilation (VE) (Yamamoto et al., 1991), ventilatory equivalent for oxygen (VE/VO2) (Amann et al., 2004; Caiozzo et al., 1982; Hoogeveen et al., 1999), respiratory exchange ratio (RER) (Santos and Gianella-Neto, 2004; Solberg et al., 2005), and a non-linear increase in the VCO2/VO2 ratio (V-slope method) (Hoogeveen et al., 1999) have shown excellent agreement with either MLSS or performance field tests.
All of these methods require sophisticated laboratory equipment, tester expertise or both for their assessment. For these reasons, a practical method that is accessible, reliable and valid is needed. If it can be determined that respiratory rate breakpoint (non-linear increase in respiratory rate during incremental exercise) can be shown to be a valid and reproducible marker for AT, a possibility exists for the creation of a respiratory rate monitor (similar to heart rate monitors) that could be used for both AT assessment and monitoring training intensity (personal communication, Department of Engineering, University of St. Thomas, 2004). A field test was developed by Conconi et al. (1982) that could supposedly detect AT by a breakpoint in linearity of heart rate during incremental exercise. Given the popularity of heart rate monitors with competitive endurance athletes, this application could have great value for both testing and training. However, the validity of this procedure has been challenged (Carey et al., 2002; 2005).
Previous research has supported the validity of the RR breakpoint in assessing AT. This author (Carey et al., 2005) found no significant differences in any pairwise comparisons for RR, VE, and VE/VO2 (F = 2.81, p = 0.067) breakpoints in 26 fit male cyclists. James et al (1989) compared RR and VE/VO2 breakpoints and found no difference in these methods of AT assessment. Neary (Neary et al., 1995) reported a significant correlation(R = 0.89, p < 0.05) for RR and VE breakpoints during incremental exercise. However, RR breakpoint was significantly less than RR during a 40-kilometer time trial, indicating that RR at breakpoint and RR at steady state, high intensity exercise are different.
Objectives of this study are to 1) assess the reliability and validity of the RR breakpoint in determining AT 2) establish SEM and CV values for the 3 methods of AT assessment as related to fitness changes in the individual athlete.
Methods
Approval to conduct this study was granted by the Institutional review Board (IRB) of the University of St. Thomas. Subjects were recruited through an advertisement placed on the Minnesota Cycling Federation (MCF) website. Requirements for participation included a current United States Cycling Federation (USCF) category and age 18 to 50. Descriptive characteristics of fifteen competitive male cyclists (5 category II, 6 category III, 1 category IV, 3 category V United States Cycling Federation) were: mean age 34.0 ± 5.3 years, mean height 1.81 ± 0.05 meters, and mean weight 77.8 ± 6.4 kilograms. Subjects read and signed consent forms and completed a brief medical history prior to the first maximal oxygen consumption (VO2 max) test. Both VO2 max tests were completed within one week and were performed at the same time of day for each subject. Every effort was made to standardize conditions on test days, including eating and sleeping habits, pre-test exercise, and testing environment. All tests were performed on an electrically-braked cycle ergometer (Lode Excalibur Sport, Lode, Netherlands) that was adjusted for seat height and distance and handlebar height and distance. Metabolic measurements were performed by the Medical Graphics VO2000 Metabolic Measurement System (Medical Graphics, St. Paul, Minnesota) utilizing breath-by- breath analysis. This system was calibrated for temperature, barometric pressure, oxygen and carbon dioxide concentrations immediately prior to each test. Heart rate was measured using a Polar Vantage XL (Polar Electro, Woodbury, New York) and was recorded each minute and at test termination. Exercise began at 25 watts and increased 25 watts per minute. Subjects were instructed to maintain a cadence of 90-95 rpm throughout the test. The test was terminated when the subjects could no longer maintain a cadence of 50 revolutions per minute. VO2 max was assessed by averaging the VO2 for the final 10 seconds of the test.
Respiratory rate (RR), Ventilation (VE), and ventilatory equivalent (VE/VO2) breakpoints in linearity were assessed using a Minitab macro software program designed to assess the fit of the data by a smallest residual sum of squares (Quantitative Methods and Computer Science Department, University of St. Thomas). VE/VO2 data for the first minute of exercise was omitted due to the rapid decrease seen in this measurement at the onset of exercise and the effect this would have on the computer-assessed breakpoint. All data points for VE and RR were included in the computer assessment (see Figure 1. accompanying scatter plot for computer-assessed breakpoint).
Figure 1.
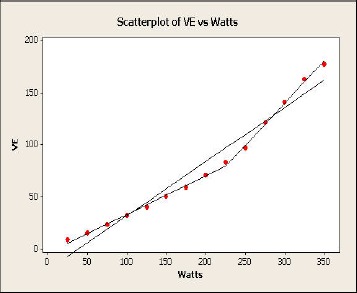
Scatterplot of VE vs. Watts.
Analysis of Variance (ANOVA) using a 2X3 repeated measures design identified differences between methods and tests. The standard error of measurement (SEM) may be considered a standard deviation of repeat testing in the same individual. Alternatively, it may be calculated by performing 2 tests on multiple individuals, calculating the standard deviation of the difference scores, and dividing this standard deviation by the square root of 2 (Hopkins, 2004). This was the method of SEM measurement used in this study. Coefficient of variation (CV) was calculated by dividing SEM by the mean. Pearson correlation coefficients were used to assess relationships between variables Data are presented as mean ± SD.
Results
Table 1 contains descriptive data on all variables measured in this study. All subjects met at least 2 of the following 3 criteria for attainment of VO2 max: 1) >95% age-predicted maximum heart rate 2) plateauing of VO2 (less than 250 ml·min-1 increase over final 2 stages of the test) 3) respiratory quotient of 1.1 or greater. Maximal respiratory quotient was 1.19 ± 0.04 for test 1 and 1.18 ± 0.06 for test 2.
Table 1.
Descriptive data of the subjects (n = 15). Values are means (±SD).
| Power (Watt) |
VO2 (ml·kg-1·min-1) |
Heart Rate (bpm) |
||||
|---|---|---|---|---|---|---|
| Test 1 | Test 2 | Test 1 | Test 2 | Test 1 | Test 2 | |
| VEVT | 305 (37) | 302 (26) | 43.1 (6.8) | 43.9 (6.1) | 164 (13) | 165 (9) |
| VE/VO2VT | 296 (30) | 307 (20) | 43.8 (6.7) | 45.1 (8.2) | 164 (11) | 164 (9) |
| RRVT | 325 (30) | 323 (33) | 43.0 (11.1) | 44.5 (9.2) | 161 (18) | 163 (15) |
| Maximal | 389 (35) | 392 (21) | 65.7 (5.1) | 67.4 (4.6) | 184 (7) | 183 (7) |
VEVT = ventilation at the ventilatory threshold, VE/VO2VT = ventilatory equivalent at the ventilatory threshold, RRVT = respiratory rate at the ventilatory threshold.
Repeated measures 2 X 3 ANOVA for the 2 repeat tests and 3 methods of AT assessment resulted in no significant differences for any comparisons (F = 0.02, p = 0.978), indicating that RR is a reliable and valid method for AT assessment when compared to the accepted methods of VE and VE/VO2.
When these same comparisons were performed using oxygen consumption (ml·kg-1·min-1), no significant differences were found between tests and methods (F = 0.13, p = 0.984). Very small mean differences between tests 1 and 2 (1.18 ml·kg-1·min-1) and small differences between methods (average difference = 0.62 ml·kg-1·min-1) would indicate excellent reproducibility and validity.
Table 2 contains correlation coefficients (r), standard error of measurement (SEM) and coefficient of variation (CV) for the 3 methods of AT assessment. Small mean differences in AT watts (VE = 1.0 watts, VE/VO2 = 4.0 watts, RR = 10.0 watts), relatively good correlation coefficients and non- significant P-values would indicate that all 3 methods are reproducible. However, SEM and CV for RR appear to be significantly greater than that of VE and VE/VO2. When AT was expressed in ml·kg-1·min-1 instead of watts, similar results were obtained. SEM and CV for VE (2.64 ml·kg-1·min-1 and 6.1%) and VE/VO2 (3.72 ml·kg-1·min-1 and 8.4%) were substantially smaller than that of RR (5.71 ml·kg-1·min-1 and 13.1%).
Table 2.
Reproducibility of the 3 methods of anaerobic threshold (AT) assessment. Values are means (±SD).
| Method | Test | Watts at AT | CC (r) | T-value | p | SEM | CV (%) |
|---|---|---|---|---|---|---|---|
| VE | 1 | 292 (57) | .872 | .11 | .910 | 19.4 | 6.7 |
| 2 | 291 (48) | ||||||
| VE/VO2 | 1 | 290 (46) | .811 | -.52 | .609 | 21.5 | 7.4 |
| 2 | 294 (52) | ||||||
| RR | 1 | 284 (82) | .800 | -.73 | .479 | 35.3 | 12.2 |
| 2 | 294 (73) |
VE = ventilation, VE/VO2 = ventilatory equivalent, RR = respiratory rate, CC = correlation coefficients, SEM = standard error of measurement (watt), CV = coefficient of variation.
Table 3 demonstrates the reproducibility of maximal values for VO2, heart rate and watts. Small mean differences, relatively high correlation coefficients, and low SEM and CV would indicate that these maximal measurements are highly reproducible.
Table 3.
Reproducibility of maximal values. Values are means (±SD).
| Measurement | Test | Values | CC (r) | T-value | p | SEM | CV (%) |
|---|---|---|---|---|---|---|---|
| VO2 max | 1 | 65.9 (7.1) | .845 | -1.01 | .329 | 2.7 | 4.1 |
| (ml·kg-1·min-1) | 2 | 66.9 (6.8) | |||||
| Heart rate | 1 | 183 (7) | .809 | -.21 | .836 | 3.5 | 1.9 |
| (bpm) | 2 | 184 (8) | |||||
| Power | 1 | 385 (45) | .958 | -.53 | .606 | 9.9 | 2.6 |
| (Watts) | 2 | 387 (38) |
CC = correlation coefficients, SEM = standard error of measurement (ml·kg-1·min-1), CV = coefficient of variation.
Discussion
The validity of RR as a method for AT assessment is supported by the results of this study. The only other studies to examine RR as a method of detecting AT have all supported these results (Carey et al., 2005; James et al., 1989; Neary et al., 1995). James et al. (1989) compared RR breakpoint to VE/VO2 breakpoint and found no significant difference between the 2 methods. This author (Carey et al., 2005) has previously compared RR, VE, and VE/VO2 and found no differences in any pairwise comparisons (F = 2.81, p = 0.067). Neary et al. (1995) also reported a significant correlation (0.89, p < 0.05) between RR and ventilatory threshold (VE). However, RR at threshold was significantly less then mean RR in a 40-kilometer time trial in trained cyclists, indicating that RR at threshold cannot be used as a method of identifying intensity of exercise during competition. In contrast, others have found that VE and VE/VO2 thresholds (Amann et al., 2004; Hoogeveen et al., 1999; Urhausen et al., 1993; Yamamoto et al., 1991) obtained during incremental exercise testing coincided with maximal lactate steady state (MLSS) and should be indicative of intensity during competition. The use of AT during incremental exercise as the intensity that could be maintained during endurance competition is controversial. Groslambert et al. (2004) reported that triathletes could maintain power outputs and physiological measurements during competition that are significantly greater than similar measurements obtained during incremental testing. This is in direct contrast to the results obtained by others (Amann et al., 2004; Hoogeveen et al., 1999; Urhausen et al., 1993; Yamamoto et al., 1991), indicating that VE/VO2 breakpoint coincided with either MLSS or mean power output during continuous high intensity exercise. These differences may be explained by variations in time of endurance performance, with endurance time at MLSS determined to be approximately 1 hour (Billat, 1996).
Small differences in SEM and CV for VE and VE/VO2 would indicate that both are equally reliable in identifying AT. However, others (Caiozzo et al, 1982) have reported that the validity of VE/VO2 in predicting MLSS is greater than that of VE and should be the method of choice in identifying AT. Still others have contended that there are 2 separate breakpoints that can be identified during incremental exercise (Bhambhani and Singh, 1985) and that they occur during different stages of the test. The first breakpoint is identified as that point at which VE/VO2 achieves a minimum value, with increasing intensities resulting in a hyperventilation with respect to VO2 (respiratory compensation point, or RCP, for VO2). The second point which occurs at higher intensities is identified when VCO2 reaches a minimal value, with increasing intensity resulting in a hyperventilation with respect to CO2 and an increase in VE/VCO2 (RCP for CO2). The former has been identified as that point when lactate concentration increases significantly above baseline, while the latter breakpoint represents a non-linear increase in blood lactate. These authors associate VE/VO2 with the first breakpoint and VE with the second breakpoint, which is in direct contrast to our results indicating no significant difference in VE and VE/VO2 breakpoints. Differences in these results may be explained by 1) Bhambhani and Singh used visual rather than computer-assessed breakpoints, 2) our computer-assessed breakpoints represented a change in linearity during incremental exercise, while examination of the Bhambhani and Singh graphs indicate that point when VE/VO2 and VE/VCO2 first reach a minimal value, not when these measurements began to rise, 3) subjects were only described as “38 healthy male volunteers”. Indeed the identification of their 2 breakpoints (60 watts and 120 watts, respectively) were less than one-half the AT watts achieved by our subjects (280-295 watts), indicating large differences in fitness status).
The reproducibility of methods of AT assessment is extremely important when assessing changes in fitness. Large variations in repeat testing make it statistically impossible to separate random error from true change. Statistical methods for assessing this change each have their strengths and weaknesses. Mean differences can detect systematic change (i.e., the 1st test is larger than the 2nd test), but cannot measure random error in testing. In contrast, the correlation coefficient suffers from the opposite effect - it cannot detect systematic change from test to test. In addition, the correlation coefficient is highly affected by the homogeneity of the sample, with greater homogeneity resulting in a smaller correlation coefficient. Subjects in this study would be considered homogeneous, with relatively small ranges for both AT values and maximal exercise values.
While the results of this study statistically support the reproducibility of RR, comparison of RR to both VE and VE/VO2 indicates the latter 2 methods have substantially lower SEM’s (19.4 and 21.5 watts, respectively) and CV’s (6.7% and 7.4%, respectively), when compared to RR SEM (35.3 watts) and RR CV(12.2%).
Atkinson and Nevill (1998) supports what he calls the “limits of agreement ”as a method of distinguishing true change from random error. To calculate the “limits of agreement”, he recommends multiplying 1.96 X √2 X SEM. Applying the “limits of agreement ”to the results of this study, the amount of improvement in AT watts needed to determine that a true improvement has been made are:
VE method = 12.2 watts
VE/VO2 method = 12.9 watts
RR method = 16.5 watts
This information may be valuable to the exercise scientist who re-tests athletes to measure improvement. However, while the above wattage needed to determine that improvement has been made appears relatively small, this may be greater than the small changes made by athletes who 1)have attained a high level of fitness, and 2) have been training for many years.
Hopkins (2000) contends that the “limits of agreement ”are too stringent and supports the use of half the “limits of agreement”, since this will still give 84% confidence of a true change, as opposed to the 95% confidence of the “limits of agreement”. This may be the preferred method when testing highly fit athletes.
Few studies have reported CV in watts. The 10.1% reported by Earnest et al. (2005) is considerably greater than the CV for AT watts of 6.7% and 7.4% for VE and VEVO2, respectively, found in this study. When AT is expressed in ml·kg-1·min-1, our CV for VE (6.1%) is very comparable to the 5.6% to 6. 4% obtained in other studies (Caiozzo et al., 1982). Our CV for VE/VO2 (8.4%) is only slightly greater than results from these previous studies. However, our CV for RR (13.1%) is significantly greater than that obtained by other methods of AT assessment and seems to preclude its use in measuring fitness changes.
In measuring improvement in VO2 max, using the limits of agreement ”as above, the following increase would need to be made to separate true change from random error:
VO2 max = 7.6 ml·kg-1·min-1
Max watts = 8.7 watts
The smaller CV for watts (2.6%) compared to VO2 max (4.1%) would indicate that just monitoring for change in maximal watts may be a better method for assessing improvement than VO2 max changes. The practical application here is the use of testing on any reproducible ergometer without the need for expensive gas analysis equipment.
The lower CV for max watts, when compared to VO2 max (ml·kg-1·min-1), is supported by others (Bagger et al., 2003, Earnest et al., 2005). Bagger et al. (2003) reported a CV less than 5% for maximum watts, while CV for VO2 max was reported as “less than 10%. ”Earnest et al. (2005) obtained CV’s of 6.3% and 7.1% for maximum watts and VO2 max (ml·kg-1·min-1), respectively. While Shephard et al. (2004) and Katch et al. (1982) did not compare CV for maximum watts and CV for VO2 max, their CV’s for VO2 max (5.0% and 5.6%) are slightly greater than the 4.1% observed in this study.
The finding of no significant differences between test 1 and test 2 would argue against habituation and a “learning effect”. Hopkins et al. (2001) reported relatively large CV values between tests 1 and 2 but smaller, non-significant differences in subsequent tests. A possible explanation for different results in this study may be explained by 1) the testing ergometer could very closely simulate the subject’s road cycle seat and handlebar positions 2) these cyclists were familiar with maximal exertion 3) many of the subjects had been tested in this lab previously.
Conclusions
It is concluded that: 1) Respiratory rate is a reliable and valid method of assessing the anaerobic threshold, when compared to the currently accepted methods of ventilation (VE) and ventilatory equivalent (VE/VO2). 2) A relatively high standard error of measurement (SEM) and coefficient of variation (CV) for the respiratory rate method, when compared to the VE and VE/VO2 methods would preclude its use in measuring the relatively small improvement seen in highly conditioned athletes. 3) The relatively smaller CV and SEM seen in maximum watts, when compared to VO2 max (ml·kg-1·min-1) would seem to indicate that the former would be more sensitive to the relatively small changes in maximal capacity seen in highly fit athletes.
Biographies

Daniel G. CAREY
Employment
Ass. Prof. in the Depart. of Health and Human Performance at the Univ.of St. Thomas in St. Paul, Minnesota, USA.
Degree
PhD
Research interests
Anaerobic threshold and body composition assessment. Metabolic changes associated with weight loss.
E-mail: dgcarey@stthomas.edu
Leslie A. SCHWARZ
Employment
student.
Degree
Bachelor of science candidate
Research interests
Sport and exercise physiology.
E-mail: GJPliego@stthomas.edu
German J. PLIEGO
Employment
Prof. of statistics in the Quantitative Methods and Computer Science Depart. of the Univ. of St. Thomas in St. Paul, Minnesota, USA.
Degree
Ph.D
Research interests
Applied statistics, regression analysis.
E-mail: GJPliego@stthomas.edu
Robert L. RAYMOND
Employment
Prof. of statistics in the Quantitative Methods and Computer Science Depart. of the Univ. of St. Thomas in St. Paul, Minnesota, USA.
Degree
PhD
E-mail: RLRaymond@StThomas.edu
References
- Amann M., Subudhi A., Walker J., Eisenman P., Shultz B., Foster C. (2004) An evaluation of the predictive validity and reliability of ventilatory threshold. Medicine and Science in Sports and Exercise 36, 1716-1722 [DOI] [PubMed] [Google Scholar]
- Atkinson G., Nevill A. (1998) Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Medicine 26, 217-238 [DOI] [PubMed] [Google Scholar]
- Aunola S., Rusko H. (1984) Reproducibility of aerobic and anaerobic thresholds in 20-50 year old men. European Journal of Applied Physiology 53, 260-266 [DOI] [PubMed] [Google Scholar]
- Aunola S., Rusko H. (1992) Does anaerobic threshold correlate with maximal lactate steady state? Journal of Sport Science 10, 309-323 [DOI] [PubMed] [Google Scholar]
- Bagger M., Petersen P., Pedersen P. (2003) Biological variation in variables associated with exercise training. International Journal of Sports Medicine 24, 433-440 [DOI] [PubMed] [Google Scholar]
- Bhambhani Y., Singh M. (1985) Ventilatory thresholds during a graded exercise test. Respiration 47, 120-128 [DOI] [PubMed] [Google Scholar]
- Billat V. (1996) Use of blood lactate measurements for prediction of exercise performance and for control of training. Sports Medicine 22, 157-175 [DOI] [PubMed] [Google Scholar]
- Caiozzo V., Davis J., Ellis J., Azus J., Vandagriff R., Prietto C., McMaster W. (1982) A comparison of gas exchange indices used to detect the anaerobic threshold. Journal of Applied Physiology: Respiratory and Environmental Exercise Physiology 53, 1184-1189 [DOI] [PubMed] [Google Scholar]
- Carey D., Duoos B., Raymond R. (2002) Intra- and Inter-observer reliability of the heart rate deflection point during incremental exercise: comparison to computer-generated deflection point. Journal of Sports Science and Medicine 4, 115-122 [PMC free article] [PubMed] [Google Scholar]
- Carey D., Hughes J., Raymond R., Pliego G. (2005) The respiratory rate as a marker for the ventilatory threshold: comparison to other ventilatory parameters. Journal of Exercise Physiology 8(2), 30-38 [Google Scholar]
- Conconi F., Ferrari M., Ziglio M., Droghetti P., Codeca L. (1982) determination of the anaerobic threshold by a non-invasive field test in runners. Journal of Applied Physiology 52, 869-873 [DOI] [PubMed] [Google Scholar]
- Earnest C., Wharton R., Church T., Lucia A. (2005) Reliability of the Lode Execalibur Sport Ergometer and applicability to Computrainer electromag-netically braked cycling training device. Journal of Strength and Conditioning Research 19, 344-348 [DOI] [PubMed] [Google Scholar]
- Groslambert A., Grappe F., Bertucci W., Perrey S., Girard A., Rouillon J. (2004). A perceptive individual time trial performed by triathletes to estimate the anaerobic threshold. Journal of Sports Medicine and Physical Fitness 44, 147-156 [PubMed] [Google Scholar]
- Hoogeveen A., Schep G., Hoogsteen J. (1999) The ventilatory threshold, heart rate, and endurance performance: relationships in elite cyclists. International Journal of Sports Medicine 20, 114-117 [DOI] [PubMed] [Google Scholar]
- Hopkins W. (2000) Measures of reliability in sports medicine and science. Sports Medicine 30, 1-15 [DOI] [PubMed] [Google Scholar]
- Hopkins W., Schabort E., Hawley J. (2001) Reliability of power in physical performance tests. Sports Medicine 31, 211-234 [DOI] [PubMed] [Google Scholar]
- Hopkins W. (2004) How to interpret changes in an athletic performance test. Sportscience 8, 1-7 [Google Scholar]
- James N., Adams G., Wilson A. (1989) Determination of te anaerobic threshold by ventilatory frequency. International Journal of Sports Medicine 10, 192-196 [DOI] [PubMed] [Google Scholar]
- Katch V., Sady S., Freedson P. (1982) Biological variability in maximum aerobic power. Medicine and Science in Sports and Exercise 14, 21-25 [DOI] [PubMed] [Google Scholar]
- Lucia A., Carvajal A., Calderon F., Alfonso A., Chicharro J. (1999) Breathing pattern in highly competitive cyclists during incremental exercise. European Journal of Applied Physiology 79, 512-521 [DOI] [PubMed] [Google Scholar]
- Neary J., Bhambhani Y., Quinney H. (1995) Validity of breathing frequency to monitor exercise intensity in trained cyclists. International Journal of Sports Medicine 16, 255-259 [DOI] [PubMed] [Google Scholar]
- Orr G., Green H., Hughson R., Bennett G. (1982) A computer linear regression model to determine ventilatory anaerobic threshold. Journal of Applied Physiology: Environmental and Exercise Physiology 52, 1349-1352 [DOI] [PubMed] [Google Scholar]
- Santos E., Giannella-Neto A. (2004) Comparison of computerized methods for detecting the ventilatory thresholds. European Journal of Applied Physiology 93, 315-324 [DOI] [PubMed] [Google Scholar]
- Shephard R., Rankinen T., Bouchard C. (2004) Test-retest errors and the apparent heterogeneity of training response. European Journal of Applied Physiology 91, 199-203 [DOI] [PubMed] [Google Scholar]
- Solberg G., Robstad B., Sjjonsberg O., Borchsenius F. (2005) Respiratory gas exchange indices for estimating the anaerobic threshold. Journal of Sports Science and Medicine 4, 29-36 [PMC free article] [PubMed] [Google Scholar]
- Urhausen A., Coen B., Weiler B., Kindermann W. (1993) Individual anaerobic threshold and maximum lactate steady state. International Journal of Sports Medicine 14, 134-139 [DOI] [PubMed] [Google Scholar]
- Yamamoto Y., Miyashita M., Hughson R., Tamura S., Shinohara M., Mutoh Y. (1991) The ventilatory threshold gives maximal lactate steady state. European Journal of Applied Physiology 63, 55-59 [DOI] [PubMed] [Google Scholar]