

Abstract
Background:
Soccer heading is using the head to directly contact the ball, often to advance the ball down the field or score. It is a skill fundamental to the game, yet it has come under scrutiny. Repeated subclinical effects of heading may compound over time, resulting in neurologic deficits. Greater head accelerations are linked to brain injury. Developing an understanding of how the neck muscles help stabilize and reduce head acceleration during impact may help prevent brain injury.
Hypothesis:
Neck strength imbalance correlates to increasing head acceleration during impact while heading a soccer ball.
Study Design:
Observational laboratory investigation.
Methods:
Sixteen Division I and II collegiate soccer players headed a ball in a controlled indoor laboratory setting while player motions were recorded by a 14-camera Vicon MX motion capture system. Neck flexor and extensor strength of each player was measured using a spring-type clinical dynamometer.
Results:
Players were served soccer balls by hand at a mean velocity of 4.29 m/s (±0.74 m/s). Players returned the ball to the server using a heading maneuver at a mean velocity of 5.48 m/s (±1.18 m/s). Mean neck strength difference was positively correlated with angular head acceleration (rho = 0.497; P = 0.05), with a trend toward significance for linear head acceleration (rho = 0.485; P = 0.057).
Conclusion:
This study suggests that symmetrical strength in neck flexors and extensors reduces head acceleration experienced during low-velocity heading in experienced collegiate players.
Clinical Relevance:
Balanced neck strength may reduce head acceleration cumulative subclinical injury. Since neck strength is a measureable and amenable strength training intervention, this may represent a modifiable intrinsic risk factor for injury.
Keywords: soccer, heading, biomechanics, acceleration, neck strength
Soccer is the world’s most popular sport, and participation varies from elite, professional play to recreational activity through the entire spectrum of the human life span. Heading the ball is a key component of the game and has come under much scrutiny in recent years.20,21,27-30,38 Heading is not associated with the highest risk of head injury (concussion) in experienced players.2,6,10,11,20,21,38,39
However, there remains a risk for the less experienced, novice population.18,22 In particular, children learning the game have a greater head-to–ball size ratio and lower neck strength, putting them at risk for head injury.40-42 This has led some organizations to prohibit heading until players are a certain age.36
When exploring the biomechanics of head and neck movement, evidence indicates that brain injury is associated with head acceleration.35,37 Acceleration can be measured many ways, including accelerometers and video.12,13,33,44,45 Motion analysis is a convenient way of recording the act with the advantage of permitting participants a less restricted movement with minimum equipment attached, closely mimicking actual game situations.19
Minimizing head acceleration has been a focus of recent research in many sports, including American football,9 rugby,31,32 lacrosse,25 and soccer.33,34 Protective headgear does not appear to be a valid solution for soccer players,4,34 hence other strategies have been explored.
Heading technique, neck muscle strength, and head size are potential intrinsic risk factors that have been investigated to date.1,7,26,46 Modeling of head and neck motion has identified the stiffening effect that neck muscles adopt when experienced players anticipate a head to ball contact.4,24,41 This stiffening is likely achieved by volitional eccentric contraction of the sternocleidomastoid muscles in the anterior cervical region as the ball makes contact with the head and the head moves backward. Concentric sternocleidomastoid muscle activity follows as the head moves forward and the ball rebounds from the head.1,4 The upper trapezius muscles are also involved in the heading motion. This muscle stiffening may absorb the kinetic energy of the ball by the head and torso rather than just the head, thus minimizing the acceleration that the head experiences by increasing the relative mass of the player and extending the time of contact with the ball.4,42,43 Neck musculature may also play a role in damping the flexion/extension oscillations that the head experiences during and after the act of heading.19,41 Damping is any effect that tends to reduce the amplitude of oscillations in an oscillatory system. In this case, neck muscle acts as a viscoelastic mechanism producing an effective shock absorber. Greater muscle stiffness may be a principal factor in lower head angular acceleration in head-neck stabilization.46 Further evidence exists in motor vehicle accident research23; awareness of impending impact may reduce the risk of injury through stiffening/damping. Investigations into vestibular reflexes17 during a sudden head drop have also highlighted the neck muscles’ ability to stabilize the head. In soccer, this neck muscle stabilizing effect may be particularly important during low ball velocity practice scenarios where the neck muscles are attempting to purposefully direct the ball rather than redirect the ball without effort. Such scenarios are commonplace in practices for novice players.
In this investigation, the authors sought to correlate head acceleration during heading to neck strength. While neck strength has not been correlated directly with head acceleration,26 it was hypothesized that the difference between neck flexion and neck extension strength may be a predictive factor of head acceleration. Achieving a balance between agonist and antagonist muscle activation has become an established means of preventing injury in other body parts.5 Previous comparison of novice and experienced soccer players19 suggests that differences in neck muscle coordination may be responsible for higher acceleration during heading by novices. Optimal damping of the ball’s kinetic energy would be expected in the setting of coordinated and balanced neck flexor (sternocleidomastoid) and neck extensor (trapezius) contraction to maximize the viscoelastic dashpot effect and diminish the head’s acceleration.
While heading coordination is a learned skill that all experienced players are expected to achieve, neck strength varies between populations.26,46 Greater muscle strength is expected to correlate with greater viscoelastic resistance, as both rely on a greater number of muscle filament cross-bridges.8 As with other body areas, the head-neck complex is expected to be stable, with symmetry in neck strength between flexors and extensors. This may be most important in practice situations at low incoming ball velocity because this necessitates greater voluntary effort and hence neck muscle activation.
Both male and female athletes were included in the study expecting there to be differences in mean neck strength between sexes. Thus, the study was designed to test the main hypothesis that neck extensor strength correlates with head acceleration.
Experimental Design and Methods
In this cross-sectional study, college-level soccer players were from Division I and II programs. Prior to enrollment, all subjects were informed of the risks and benefits of participating, and written informed consent was obtained. The Institutional Review Boards at both Albany Medical College and Rensselaer Polytechnic Institute approved this protocol. Furthermore, the variables used in this study were not available at the time of data collection, thus both the tester and the subjects were blinded to the values that were generated at time of testing.
Measuring Movement of Subject Head, Subject Body, and Ball During Heading
After providing demographic information (age, weight, height, and years of soccer experience), markers were attached by Velcro™ tape (VELCRO USA, Manchester, New Hampshire) to the subject in preparation for the motion capture experiment. The acceleration of the subject’s head during heading was measured using a 14-camera Vicon MX3 Motion Capture System (Vicon Motion Systems, Los Angeles, California). During preliminary testing, the motion capture system was able to record the position and movement of the subject marker set and the ball simultaneously at a rate of 450 Hz. Given that the impact between the ball and the player lasts approximately 20 milliseconds,19 this capture rate is sufficient to detect the peak acceleration of impact.47 A stationary marker set was used to estimate the sampling error at 450 Hz.
To record motion, 11 retro-reflective markers were attached to anatomic landmarks: the suprasternal notch (Clav) and the xyphoid (Strn), as well as the seventh cervical (C7) and tenth thoracic (T10) vertebrae (Figure 1). Torso markers were placed principally to facilitate kinematic analysis of heading technique. Both temples (left and right front of head; LFH, RFH) and along the parietal/occiput suture (left and right back of head; LBH, RBH) were marked and provided data for kinetic analysis of head acceleration. A minimum of 3 markers are required to determine an object’s rotational motion. However, redundant markers are often used in case 1 marker becomes obscured. Hip position was recorded by markers located at the first sacral vertebra (S1) and the anterior superior iliac spines (L/R ASIS) and was used by the Vicon software to identify the subject and differentiate subject markers from the ball markers. The soccer ball had 6 low profile soft markers attached, enabling simultaneous recording of ball speed and subject movement
Figure 1.
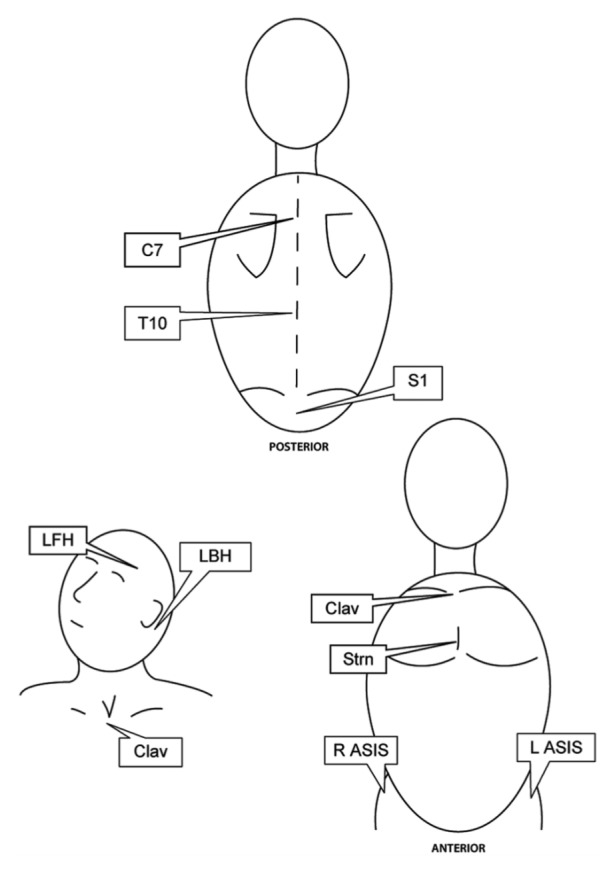
Retro-reflective marker set. Figure artwork courtesy of Kari Giordano. C7, seventh cervical vertebrae; T10, tenth thoracic vertebrae; S1, first sacral vertebra; LFH, left front of head; LBH, left back of head; Clav, suprasternal notch; Strn, xyphoid; R ASIS, right anterior superior iliac spine; L ASIS, left anterior superior iliac spine.
To record a single heading trial, soccer balls (450 g college-regulation Adidas inflated to 82.7 kPa) were served to the subjects by an investigator from 3 meters away mimicking a soccer practice scenario of low ball velocity. Subjects were asked to return the ball to the experimenter’s hands by executing a header. To be included, recordings had to contain all of the markers for the entirety of the heading maneuver. If a marker was not visible or the recording incomplete, the next suitable trial was used. Pilot testing showed 1 in 4 headers were of sufficient quality for further analysis, so approximately 20 headers were recorded for each subject to obtain 5 usable recordings. Five was chosen to minimize the effects of fatigue while obtaining a sample representative of the normal variation from header to header.
Calculation of Translational Head Acceleration
The translational acceleration of the subject’s head during the task was calculated by taking the numerical first derivative of each head marker. This provided velocity vectors in each direction (X’, Y’, and Z’). The numerical derivative of these velocity vectors was used to calculate component acceleration vectors for each marker. Because the skull is a rigid body, the component acceleration vectors were averaged to find a head acceleration vector.19 Commercial motion capture studios use similar techniques built around rigid body segments that combine to form full-body skeletons.48 Using multiple markers to calculate acceleration reduces intratrial error. Within each frame of data, the acceleration of the 4 head markers (RFH, LFH, RBH, LBH) was averaged for the subject’s mean head acceleration. The head acceleration throughout an entire trial was calculated by assuming that the greatest absolute head acceleration during the time of impact (when the ball first touches the subject’s head until when the ball leaves) was due to impact with the ball. The average of these values across each subject’s 5 trials was reported in the final analysis.
Calculation of Angular Head Acceleration
Head angular velocity was in the sagittal plane with the second numerical derivative of the angle defined between the head normal vector and the floor vector (the horizontal axis was used as a reference, as the ball was served parallel to this axis). The head normal was defined as a vector perpendicular to the plane of the 4 head markers (Figure 2).
Figure 2.
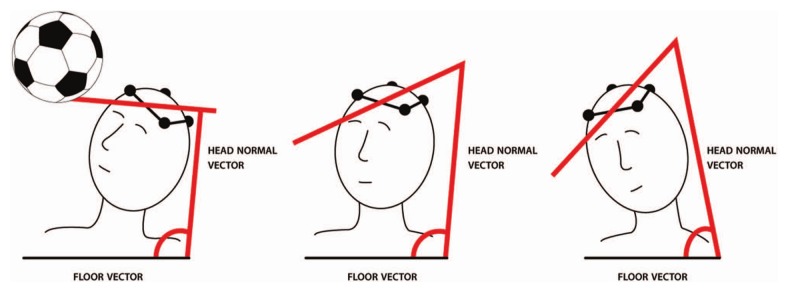
Calculation of angular head acceleration. Figure artwork courtesy of Kari Giordano.
Combinations of the head markers were used to create vectors, the cross-product of which was used to calculate an average head normal vector. The head-floor angle was defined as the angle between the head normal and the floor and was plotted as a function of time throughout the trial. The numerical second derivative of this angle was calculated to find the subject’s angular head acceleration. As with peak translational acceleration, the peak angular acceleration was identified as the highest value during the time of impact. The resulting peak angular acceleration values were averaged across each subject’s 5 trials and reported in radians per second squared.
Measuring Neck Strength
Neck strength measurements were taken using a spring-type clinical dynamometer (Baseline Push-Pull Dynamometer, Fabrication Enterprises Inc, White Plains, New York). The subject was seated facing the sensor and was restrained at the level of their shoulders to help isolate the neck muscles and reduce accessory movement (Figure 3).
Figure 3.
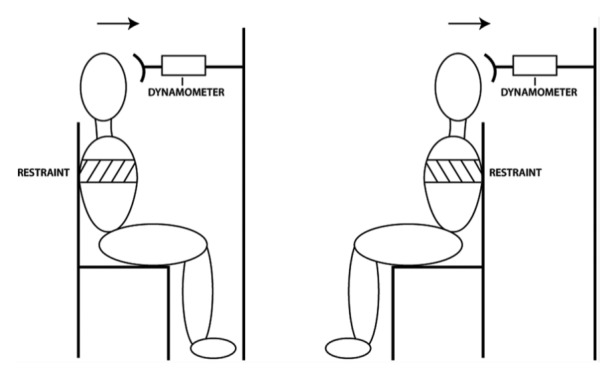
Neck strength apparatus. Figure artwork courtesy of Kari Giordano.
A special adapter allowed the sensor to be fit to the forehead. The sensor was horizontal and secured at the level of the subject’s forehead when the subject was seated upright. The dynamometer automatically digitally recorded the highest force generated during any 1 push. The subject attempted 5 isometric neck flexion movements at maximum voluntary exertion. The maximum force (in Newtons) generated by each attempt was recorded, with as much rest time as the subject desired between exertions. Subjects rested an average of 10 to 20 seconds between attempts. After completion of flexion, subjects then rotated 180° (facing away from the sensor) with the back of their head cradled by the sensor. Subjects then provided 5 isometric neck extensions, and the maximum force generated by each attempt was recorded by the dynamometer. Neck strength imbalance was defined as mean flexion strength minus mean extension strength.
Statistical Analysis
Independent samples t tests were used to compare differences in mean neck flexion strength, mean neck extension strength, and mean strength imbalance between sexes. Differences were considered statistically significant for P ≤ 0.05. When no sex-based differences were identified, data from all subjects were pooled (men and women) and correlations between:
mean flexion strength and mean head linear and angular acceleration
mean extension strength and mean head linear and angular acceleration
mean strength imbalance and mean head linear and angular acceleration
were tested using Spearman rho due to the sample size. Values were considered statistically significant if P ≤ 0.05. Correlations between mean flexion strength, mean extension strength, and mean strength imbalance and post-header ball velocity were also tested as a secondary outcome variable of interest. Ball velocity provided an indication of player voluntary effort in heading.
Results
Sixteen subjects, 8 men and 8 women, consisting of 6 forwards, 4 midfielders, 5 defenders, and 1 goal keeper, were tested.
The mean age was 20.5 years (±1.9 years). There were no significant differences between sexes in mean neck flexion (P = 0.201), extension strength (P = 0.130), or mean imbalance (P = 0.631), justifying the pooling of data (Table 1). The ball was pitched to subjects at a mean 4.29 m/s (±0.74 m/s) and subjects returned them at a mean velocity of 5.48 m/s (±1.18 m/s).
Table 1.
Comparison of male and female data
| Mean Value (± Standard Deviation) |
||||
|---|---|---|---|---|
| Men | Women | All Subjects | P value | |
| Flexion strength, N | 55.0 (±32.2) | 36.5 (±21.5) | 45.7 (±4.0) | >0.201 |
| Extension strength, N | 66.8 (±34.0) | 43.5 (±21.9) | 55.1 (±4.6) | >0.130 |
| Strength difference, N | −11.8 (±24.9) | −7.0 (±11.9) | −7.9 (±17.7) | >0.631 |
| Change in ball velocity, m/s | 9.38 (±1.671) | 9.31 (±6.30) | 9.34 (±1.49) | 0.648 |
| Translational acceleration, m/s2 | 101.70 (±34.3) | 101.75 (±64.92) | 101.73 (±51.68) | 0.997 |
| Angular acceleration, rad/s2 | 854.86 (±489.144) | 901 (±459.54) | 877.93 (±472.13) | 0.617 |
Figures 4, 5, and 6 depict a typical heading event. The dip in the ball velocity is due to the drop that occurs when the ball hits the player’s forehead (Figure 4). First, the head accelerates into the ball and then rapidly slows with impact (Figure 5). The head then speeds up as it launches the ball forward, going through a few flexion/extension oscillations. The remainder of the acceleration is negative as the player begins to decelerate his or her head and neck after accomplishing the heading task. Data indicate a maximum error in linear acceleration of the system of 2.19 m/s2.
Figure 4.
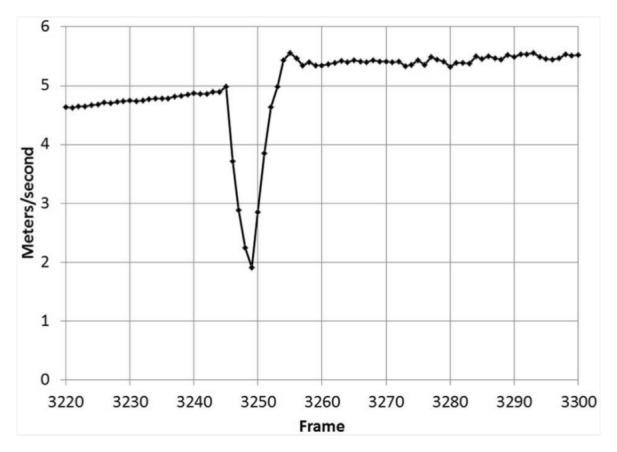
Ball velocity change versus time (subject 12, trial 7) during a 0.22-second window before and after impact with the subject’s head.
Figure 5.
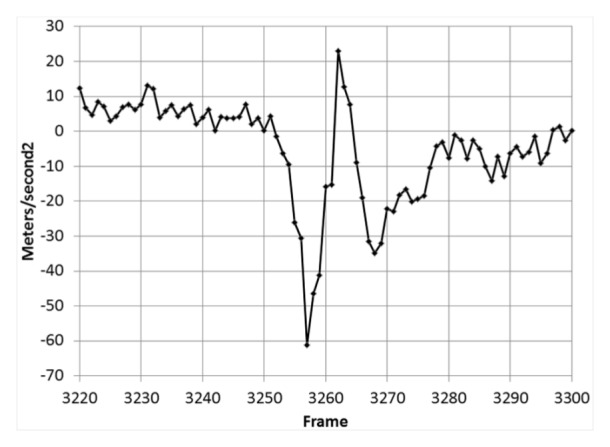
Head linear acceleration change versus time (subject 12, trial 7) during a 0.22-second window before and after a heading impact with the ball.
Figure 6.
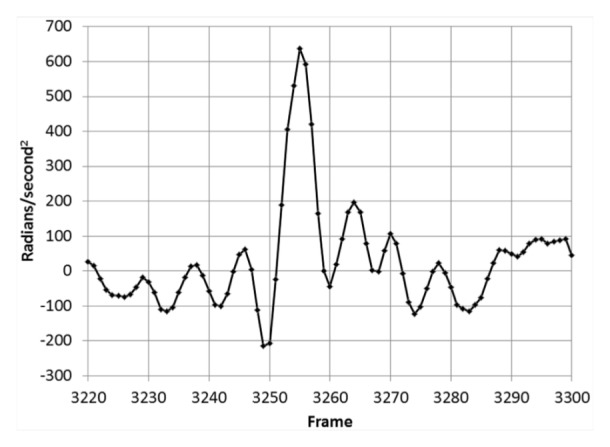
Head angular acceleration change versus time (subject 12, trial 7) during a 0.22-second window before and after a heading impact with the ball.
Angular acceleration is slightly negative prior to impact, as the head angularly accelerates into the ball (Figure 6). The angle between the head normal vector and the floor widens quickly as the head rocks back during impact, followed by damped oscillations.
Mean neck strength difference was positively correlated with angular head acceleration (rho = 0.497; P = 0.05), with a trend toward significance for linear head acceleration (rho = 0.485; P = 0.057). Correlation between mean flexion strength and head acceleration and mean extension strength and head acceleration were nonsignificant. Change in ball velocity did not correlate with either mean flexion strength (P > 0.05), mean extension strength (P > 0.05), or mean neck strength difference (P > 0.05).
Discussion
This study shows that symmetrical strength in neck flexors and extensors may reduce head acceleration of experienced collegiate players at low ball velocity. In contrast, previous investigations have been unable to correlate lower head acceleration with enhanced neck strengthening when neck flexor/extensor strength difference was not explored.26 It is not known if these results apply to a younger population, which may be at highest risk of head injury from repetitive heading.
Studies in movement science have used accelerometers to measure head acceleration because they afford a high sample rate.13,33 However, the necessary sensors, headgear, and wires often associated with accelerometers may impede natural motion. A 450 Hz capture rate satisfies the Nyquist criteria,47 and motion capture measures head acceleration naturally without the interference of wires and extra sensors. Realistic movement was captured at low ball velocities. These acceleration values are consistent with previous investigations.12,13,33,34,44,45
Achieving and maintaining a balance in neck strength may be a key preventive technique in limiting acceleration, hence limiting the potential risks of repetitive heading in soccer.6,11,21,22,27-30,38,39 Balancing agonist and antagonist muscle activation is an established injury prevention strategy for other areas such as the knee.5 Balancing muscles may be particularly beneficial for younger players learning the game and would perhaps be a more objective, quantitative parameter when deciding when to introduce heading relative to the abstract age limits currently in existence.36 Increasing ball velocities might magnify the relationship between head acceleration and neck strength.
Neck strength assessment could be used for pre-participation screening of soccer players to identify those most at risk and strengthening regimens employed during preseason conditioning to lower the risk of injury during soccer participation. Such strength and conditioning interventions have been successful in reducing incidence of anterior cruciate ligament injury in soccer.14-16
Because of the small cohort of subjects in this study and the lack of a power analysis, sex differences and player position or experience were inadequately investigated as predictive factors in head acceleration. There was a high standard deviation in mean flexion and mean extension strength in each sex. Therefore, no definitive conclusions can be made about the strength imbalance between sexes.
This study is further limited because the measurement of neck flexion and extension strength was not randomized. This may have biased the results toward greater flexion strength because it was always tested first.
Conclusion
This cross-sectional study of collegiate soccer players suggests a correlation between neck strength imbalance and angular head acceleration during heading. While the exact mechanism underlying this correlation is not clear, a balance of neck flexor/extensor strength may reduce head acceleration by increasing the relative mass of the head and neck and damping the flexion/extension oscillations that the head experiences during and after the act of heading.
Acknowledgments
The authors thank the Department of Medicine at Albany Medical College, whose kind support made this project possible, as well as Dr James Watt, who provided laboratory space and technical expertise. The authors also express their gratitude to Kari Giordano (sundaegraphics@gmail.com) who provided the artwork for Figures 1 through 3
Footnotes
The following authors declared potential conflicts of interest: Hamish A. Kerr, MD, MSc, FAAP, is employed as Team Physician at Siena College and received a grant from the American Medical Society for Sports Medicine.
References
- 1. Bauer JA, Thomas TS, Cauraugh JH, Kaminski TW, Hass CJ. Impact forces and neck muscle activity in heading by collegiate female soccer players. J Sports Sci. 2001;19:171-179 [DOI] [PubMed] [Google Scholar]
- 2. Broglio SP, Guskiewicz KM, Sell TC, Lephart SM. No acute changes in postural control after soccer heading. Br J Sports Med. 2004;38:561-567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Broglio SP, Ju YY, Broglio MD, Sell TC. The efficacy of soccer headgear. J Athl Train. 2003;38:220-224 [PMC free article] [PubMed] [Google Scholar]
- 4. Burslem I, Lees A. Quantification of impact accelerations of the head during the heading of a football. In: Reilly T, ed. Science and Football. London: E&FN SPON;1988:243-248 [Google Scholar]
- 5. Drez D. Delee & Drez’s Orthopaedic Sports Medicine. 3rd ed Philadelphia, PA: Saunders Elsevier; 2009 [Google Scholar]
- 6. Dvorak J, Junge A, McCrory P. Head injuries: do heading and head injuries in football lead to long term cognitive impairment? Br J Sports Med. 2005;39:i1-i2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Erkmen N. Evaluating the heading in professional soccer players by playing positions. J Strength Cond Res. 2009;23:1723-1728 [DOI] [PubMed] [Google Scholar]
- 8. Foster C, Faber MJ, Porcari JP. Basics of exercise physiology. In: McKeag DB, Moeller JL. eds. ACSM’s Primary Care Sports Medicine. Philadelphia, PA: Lippincott Williams & Wilkins; 2007: chapter 3 [Google Scholar]
- 9. Frechede B, McIntosh AS. Numerical reconstruction of real-life concussive football impacts. Med Sci Sports Exerc. 2009;41:390-398 [DOI] [PubMed] [Google Scholar]
- 10. Fuller CW, Junge A, Dvorak J. A six year prospective study of the incidence and causes of head and neck injuries in international football. Br J Sports Med. 2005;39:i3-i9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Guskiewicz KM, Marshall SW, Broglio SP, Cantu RC, Kirkendall DT. No evidence of impaired neurocognitive performance in collegiate soccer players. Am J Sports Med. 2002;30:157-162 [DOI] [PubMed] [Google Scholar]
- 12. Hanlon E, Bir C. Real-time head acceleration measurement in girls’ youth soccer [published online December 2, 2011]. Med Sci Sports Exerc. [DOI] [PubMed] [Google Scholar]
- 13. Hanlon E, Bir C. Validation of a wireless head acceleration measurement system for use in soccer play. J Appl Biomech. 2010;26:424-431 [DOI] [PubMed] [Google Scholar]
- 14. Hewett TE, Ford KR, Myer GD. Anterior cruciate ligament injuries in female athletes: part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am J Sports Med. 2006;34:490-498 [DOI] [PubMed] [Google Scholar]
- 15. Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: part 1, mechanisms and risk factors. Am J Sports Med. 2006;34:299-311 [DOI] [PubMed] [Google Scholar]
- 16. Hewett TE, Myer GD, Ford KR, Slauterbeck JR. Dynamic neuromuscular analysis training for preventing anterior cruciate ligament injury in female athletes. Instr Course Lect. 2007;56:397-406 [PubMed] [Google Scholar]
- 17. Ito Y, Corna S, von Brevern M, Bronstein A, Gresty M. The functional effectiveness of neck muscle reflexes for head-righting in response to sudden fall. Exp Brain Res. 1997;117:266-272 [DOI] [PubMed] [Google Scholar]
- 18. Janda DH, Bir CA, Cheney AL. An evaluation of the cumulative concussive effect of soccer heading in the youth population. Inj Control Saf Promot. 2002;9:25-31 [DOI] [PubMed] [Google Scholar]
- 19. Kerr H, Riches P. Distributions of peak head accelerations during soccer heading vary between novice and skilled females. Br J Sports Med. 2004;38:650-653 [Google Scholar]
- 20. Kirkendall DT, Garrett WE. Heading in soccer: integral skill or grounds for cognitive dysfunction? J Athl Train. 2001;36:328-333 [PMC free article] [PubMed] [Google Scholar]
- 21. Kirkendall DT, Jordan SE, Garrett WE. Heading and head injuries in soccer. Sports Med. 2001;31:369-386 [DOI] [PubMed] [Google Scholar]
- 22. Koutures CG, Gregory AJ. Injuries in youth soccer. Pediatrics. 2010;125:410-414 [DOI] [PubMed] [Google Scholar]
- 23. Kumar S, Narayan Y, Amell T. Role of awareness in head-neck acceleration in low velocity rear-end impacts. Accid Anal Prev. 2000;32:233-241 [DOI] [PubMed] [Google Scholar]
- 24. Lees A, Nolan L. The biomechanics of soccer: a review. J Sports Sci. 1998;16:211-234 [DOI] [PubMed] [Google Scholar]
- 25. Lincoln AE, Hinton RY, Almquist JL, Lager SL, Dick RW. Head, face, and eye injuries in scholastic and collegiate lacrosse: a 4-year prospective study. Am J Sports Med. 2007;35:207-215 [DOI] [PubMed] [Google Scholar]
- 26. Mansell J, Tierney RT, Sitler MR, Swanik KA, Stearne D. Resistance training and head-neck segment dynamic stabilization in male and female collegiate soccer players. J Athl Train. 2005;40:310-319 [PMC free article] [PubMed] [Google Scholar]
- 27. Matser EJ, Kessels AG, Jordan BD, Lezak MD, Troost J. Chronic traumatic brain injury in professional soccer players. Neurology. 1998;51:791-796 [DOI] [PubMed] [Google Scholar]
- 28. Matser EJ, Kessels AG, Lezak MD, Jordan BD, Troost J. Neuropsychological impairment in amateur soccer players. JAMA. 1999;282:971-973 [DOI] [PubMed] [Google Scholar]
- 29. Matser EJ, Kessels AG, Lezak MD, Troost J. A dose-response relation of headers and concussions with cognitive impairment in professional soccer players. J Clin Exp Neuropsychol. 2001;23:770-774 [DOI] [PubMed] [Google Scholar]
- 30. McCrory PR. Brain injury and heading in soccer. BMJ. 2003;327:351-352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. McIntosh AS, McCrory P. Effectiveness of headgear in a pilot study of under 15 rugby union football. Br J Sports Med. 2001;35:167-169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. McIntosh AS, McCrory P, Finch CF, Best JP, Chalmers DJ, Wolfe R. Does padded headgear prevent head injury in rugby union football? Med Sci Sports Exerc. 2009;41:306-313 [DOI] [PubMed] [Google Scholar]
- 33. Naunheim RS, Bayly PV, Standeven J, Neubauer JS, Lewis LM, Genin GM. Linear and angular head accelerations during heading of a soccer ball. Med Sci Sports Exerc. 2003;35:1406-1412 [DOI] [PubMed] [Google Scholar]
- 34. Naunheim RS, Ryden A, Standeven J, et al. Does soccer headgear attenuate the impact when heading a soccer ball? Acad Emerg Med. 2003;10:85-90 [DOI] [PubMed] [Google Scholar]
- 35. Ommaya AK, Gennarelli TA. Cerebral concussion and traumatic unconsciousness. Correlation of experimental and clinical observations of blunt head injuries. Brain. 1974;97:633-654 [DOI] [PubMed] [Google Scholar]
- 36.Ouellette J.Is heading safe? [Accessed July 28, 2011]. http://www.ayso.org/resources/safety/is_heading_safe.aspx
- 37. Prasad P, Mertz H. The position of the United States delegation to the ISO Working Group on the Use of HIC in the Automotive Environment. SAE Technical Paper 851246, 1985; 10.4271/851246 [DOI] [Google Scholar]
- 38. Putukian M. Heading in soccer: is it safe? Curr Sports Med Rep. 2004;3:9-14 [DOI] [PubMed] [Google Scholar]
- 39. Putukian M, Echemendia RJ, Mackin S. The acute neuropsychological effects of heading in soccer: a pilot study. Clin J Sport Med. 2000;10:104-109 [DOI] [PubMed] [Google Scholar]
- 40. Queen RM, Weinhold PS, Kirkendall DT, Yu B. Theoretical study of the effect of ball properties on impact force in soccer heading. Med Sci Sports Exerc. 2003;35:2069-2076 [DOI] [PubMed] [Google Scholar]
- 41. Riches P. A dynamic model of the head acceleration associated with heading a soccer ball. Sports Engin. 2005;9:39-47 [Google Scholar]
- 42. Schneider K, Zernicke RF. Computer simulation of head impact: estimation of head-injury risk during soccer heading. Int J Sport Biomech. 1988;4:358-371 [Google Scholar]
- 43. Shapiro I, Frankel VH. Biomechanics of the cervical spine. In: Nordin M, Frankel VA, eds. Basic Biomechanics of the Musculoskeletal System. Philadelphia, PA: Lea & Febiger; 1989:209-224 [Google Scholar]
- 44. Shewchenko N, Withnall C, Keown M, Gittens R, Dvorak J. Heading in football. Part 1: development of biomechanical methods to investigate head response. Br J Sports Med. 2005;39(suppl 1):i10-i25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Shewchenko N, Withnall C, Keown M, Gittens R, Dvorak J. Heading in football. Part 2: biomechanics of ball heading and head response. Br J Sports Med. 2005;39(suppl 1):i26-i32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Tierney RT, Higgins M, Caswell SV, et al. Sex differences in head acceleration during heading while wearing soccer headgear. J Athl Train. 2008;43:578-584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Winter D. Biomechanics and Motor Control of Human Movement. 4th ed. Hoboken, NJ: John Wiley & Sons; 2009 [Google Scholar]
- 48.Vicon Blade. [Accessed December 27, 2012]. http://www.vicon.com/products/blade.html