

According to the most recent National Health and Nutrition Examination Survey, an estimated 5.1 million adult Americans have heart failure (HF), and projections show that by the year 2030 the prevalence of HF in the U.S. will increase by 25%.1 Despite guideline-recommended therapy for patients with HF and reduced ejection fraction,2 the overall 5-year mortality remains around 50%, and the 1-year mortality in patients with New York Heart Association (NYHA) functional class III-IV heart failure on maximal medical therapy is 35-40%. Given the public health burden of HF, there is a clear need for improved medical therapies.
Oxidant Stress and Progression of Heart Failure
Reduced myocardial antioxidant activity and increased oxidant damage have been demonstrated in animal models of HF, and markers of oxidative stress are increased in HF patients.3 These data support the thesis that reactive oxygen species (ROS) may contribute to the progression of myocardial failure. Xanthine oxidase (XO) is among the potential stimuli of formation of ROS in HF, and may be an important target for therapy.4 Current evidence supports the hypothesis that HF is associated with an increase in the activity of XO, which in turn increases production of superoxide and uric acid (UA) during purine metabolism. The resulting nitroso-redox imbalance5 may be exacerbated by decreased activity of nitric oxide synthase (Figure 1). Significant hyperuricemia (i.e., serum UA ≥ 9.5 mg/dl) is present in about 25% of patients with HF and reduced ejection fraction.6,7 In addition to nitroso-redox imbalance, other contributors to hyperuricemia in HF include activation of pro-inflammatory cytokines, impaired vascular function and renal insufficiency, as well as loop diuretic therapy.8 In patients with HF, there is a strong relationship between elevated UA levels and worsening symptoms,9 impaired exercise tolerance,10 and increased mortality.6 Based on these findings, serum UA levels have been included in HF risk scores.11,12 Furthermore, observational studies in both chronic and acute HF patients with gout suggest that treatment with allopurinol, an XO inhibitor, is associated with improved survival.13-15
Figure 1.
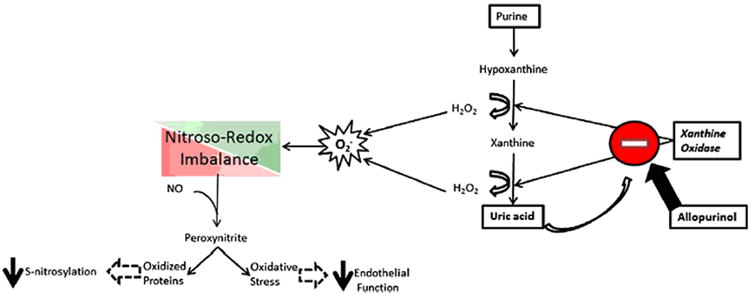
Nitroso-redox imbalance due to increased xanthine oxidase (XO) activity in HF. Purines are metabolized to hypoxanthine and xanthine by the action of xanthine oxidase leading to the production of uric acid. In the process, reactive oxygen species including hydrogen peroxide (H2O2) and superoxide anion (O2-) are produced. Increased ROS can lead to peroxynitrite formation and the oxidation of proteins blocking important post-translation nitrosylation modifications. Allopurinol is a potent inhibitor of xanthine oxidase. NO, nitric oxide. From Karantalis et al.,4 with permission.
Superoxide decreases nitric oxide signaling and also decreases myofilament sensitivity to calcium and contractility.16 Decreased contractility leads to hypoperfusion of the heart and other organs, increases anaerobic metabolism, and leads to depletion of ATP and the accumulation of hypoxanthine (the substrate of XO). Allopurinol is a potent XO inhibitor that can reverse these processes, ultimately increasing cardiac contractile efficiency and reducing myocardial oxygen consumption (MVO2). There are several lines of experimental and clinical data that support the use of XO inhibitors in HF.
Acute Xanthine Oxidase Inhibition in Heart Failure
HF is characterized by an imbalance between left ventricular (LV) performance and MVO2. Experimental models suggest that oxidant stress resulting from XO activation contributes to mechanoenergetic uncoupling, and that XO inhibition with allopurinol may improve LV efficiency.17 Cappola et al.18 instrumented patients with idiopathic dilated cardiomyopathy to assess MVO2, contractility (dP/dtmax and Ees) and efficiency (stroke work/MVO2) before and after intracoronary infusion of allopurinol. Allopurinol caused a significant decrease in MVO2 (-16 ± 5%, p<0.01) without a parallel decrease in dP/dtmax or Ees. The net result was a significant increase in myocardial efficiency (+40 ± 7%, p<0.05). More recently, Hirsh et al.19 used 31P magnetic resonance spectroscopy to determine myocardial concentrations of adenosine triphosphate (ATP) and the rate of ATP synthesis through creatine kinase flux in vivo. In 16 patients with non-ischemic cardiomyopathy, intravenous allopurinol acutely increased myocardial high-energy phosphates and ATP flux, thereby providing a mechanism for the improvement in mechanoenergetic coupling.
Chronic Xanthine Oxidase Inhibition in Heart Failure
Impaired endothelium-dependent relaxation contributes to symptoms and exercise intolerance in HF. An important mechanism underlying endothelial dysfunction is increased oxidative stress, due in part to vascular XO activity. To determine if chronic XO inhibition would improve endothelial function in HF, Farquharson et al.20 randomized 11 patients with mild-moderate HF in a double-blind, crossover study to receive allopurinol 300 mg once daily or placebo for one month. Allopurinol significantly improved endothelium-dependent vasodilation and reduced markers of oxidative stress. In a subsequent study, George et al.21 demonstrated a steep dose-response relationship between allopurinol and its effect on endothelial function. In 30 subjects with chronic HF, allopurinol 600 mg once daily increased forearm blood flow in response to acetylcholine compared to both allopurinol 300 mg once daily and placebo, and was well tolerated. Other short-term studies with allopurinol in patients with HF have demonstrated improvements in LV ejection fraction,22 diastolic function, and coronary flow reserve.23
Xanthine Oxidase Inhibition and Clinical Outcomes in Heart Failure
Oxypurinol is the primary metabolite of allopurinol, and therefore a potent XO inhibitor. Numerous studies have documented the potential benefits of oxypurinol in experimental and clinical conditions involving oxidative stress. The Oxypurinol Compared With Placebo for Class III-IV NYHA Congestive Heart Failure (OPT-CHF) Trial was designed to test whether oxypurinol produces clinical benefits in patients with moderate-severe HF due to systolic dysfunction receiving optimal medical therapy.24 In this study, 405 patients with a mean age of 65 years, LV ejection fraction of 26% and UA level of 8.1 mg/dl, who were well treated with angiotensin-converting enzyme inhibitor/angiotensin receptor blocker (96%) and beta-blocker (92%), were randomized to receive oxypurinol 600 mg once daily or placebo for 24 weeks. Efficacy was assessed using a composite end point comprising HF morbidity, mortality and quality of life.25 Oxypurinol reduced serum UA by ∼2 mg/dl (p<0.001), but did not improve clinical status in unselected patients with HF. In a hypothesis-generating subgroup analysis, patients with elevated UA levels (≥ 9.5 mg/dl, n = 108) responded favorably to oxypurinol, whereas patients with UA < 9.5 mg/dl exhibited a trend towards worsening. In addition, UA reduction to oxypurinol correlated with favorable clinical response.
Based on these findings, we hypothesize that in patients with symptomatic HF due to LV systolic dysfunction, who have elevated serum uric acid levels and are not receiving allopurinol for another indication such as gout, treatment with high-dose allopurinol for 24 weeks will improve clinical outcomes compared to treatment with placebo. We chose allopurinol over oxypurinol given its wide availability and known safety profile of higher doses.
Study Design and Patient Population
The Xanthine Oxidase Inhibition for Hyperuricemic Heart Failure Patients (EXACT-HF) study is a multi-center, randomized (1:1), double-blind, placebo-controlled, 24-week trial of allopurinol in patients with symptomatic HF due to LV systolic dysfunction (LVEF ≤ 40%) and elevated serum uric acid levels (UA ≥ 9.5 mg/dl). The study includes screening, study drug administration, and follow-up phases (Figure 2). A total of 250 patients meeting eligibility criteria (Table 1) will be enrolled in the study. In an effort to enroll a population with an adequate event rate to power a medium-size, proof-of-concept study, patients must have at least one additional marker of increased risk, including an acute HF event within 12 months, severe LV dysfunction (LVEF ≤ 25%) or an elevated natriuretic peptide level (BNP > 250 pg/ml or NT-proBNP > 1500 pg/ml).26,27
Figure 2.
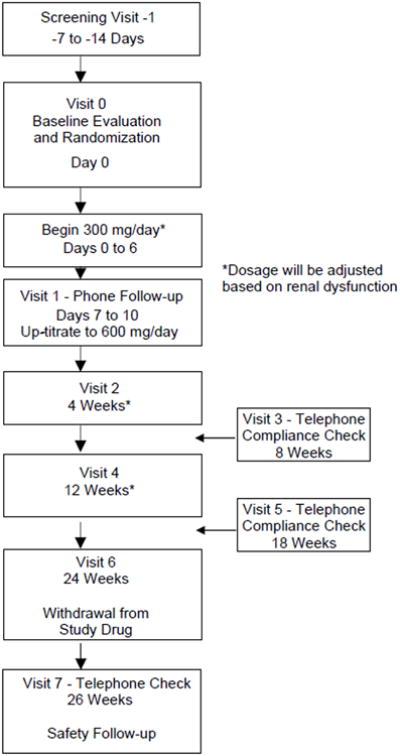
Flow diagram of the EXACT-HF study.
Table 1. EXACT-HF Inclusion and Selected Exclusion Criteria.
| Inclusion Criteria |
|
|
|
| Selected Exclusion Criteria |
|
ACE, angiotensin-converting enzyme; ALT, alanine aminotransferase; ARB, angiotensin receptor blocker; AST, aspartate aminotransferase BNP, B-type natriuretic peptide; CABG, coronary artery bypass grafting; DBP, diastolic blood pressure; ER, emergency room; GFR, glomerular filtration rate; HF, heart failure; IV, intravenous; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association; PAD, peripheral arterial disease; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; UA, uric acid; VAD, ventricular assist device.
Determined at or within 4 weeks of screening evaluation;
determined at the time of screening evaluation.
Active Drug Intervention and Dose Adjustment for Renal Dysfunction
For patients with gout, allopurinol is typically initiated at a dose of 100 mg once daily and may be titrated to a maximum dose of 800 mg depending on the severity of disease and the target uric acid level (usual goal < 6.0 mg/dl).28 The drug is metabolized in the liver to oxypurinol, and the latter is excreted in the urine. The elimination half-life of oxypurinol is 15-25 hours, and may be longer in renal failure.29 Recommendations first proposed in 1984 and maintained in the current allopurinol package insert28 call for a dose reduction to 200 mg if the estimated glomerular filtration rate (GFR) is 10-20 ml/min, and to 100 mg if < 10 ml/min. Importantly, EXACT-HF excludes subjects with an estimated GFR < 20 ml/min.
Based on this information, active therapy in EXACT-HF consists of allopurinol (target dose, 600 mg daily in divided doses), with dose adjustment for renal function (Table 2). Study drug is given for 24 weeks starting with 300 mg by mouth once daily for 1 week. If that dose is well tolerated, the dose is increased to 600 mg daily for the remaining 23 weeks of the study. Patients unable to tolerate the 600 mg dose are maintained on the 300 mg dose. Patients with a serum creatinine level > 2.0 mg/dl at screening are started on 100 mg daily, and titrated to 300 mg daily. Patients are instructed to take the study drug with food, and compliance is assessed by phone contact at multiple time points (Figure 2). The rationale for using relatively high doses of allopurinol is based on data reported by Struthers and colleagues showing that allopurinol has dose-dependent effects on both uric acid lowering and endothelium-dependent vasodilation in patients with HF, and is well tolerated (Table 3).21
Table 2. Dose Adjustment with Renal Dysfunction.
| Visit (Time) | SCr ≤ 2 mg/dl | SCr > 2, but ≤ 3 mg/dl | SCr > 3, but < 5 mg/dl | SCr ≥ 5 mg/dl |
|---|---|---|---|---|
| 0 (Baseline)* | 300 mg | 100 mg | Excluded | Excluded |
| 1 (7-10 Days)*† | 600 mg | 300 mg | --- | --- |
| 2 (4 Weeks)‡ | 600 mg | 300 mg | 100 mg | Discontinue |
| 4 (12 Weeks)‡ | 600 mg | 300 mg | 100 mg | Discontinue |
SCr, serum creatinine level.
Screening laboratories used to determine dosing at baseline and visit 1;
laboratories are not checked at this visit, which is a telephone call;
if renal function improves at visit 2 or 4, subjects remain at established dose (i.e., no up-titration).
Table 3. Rationale for High-dose Allopurinol in EXACT-HF.
| Oxypurinol | Allopurinol | Effect on UA levels21,24 | Effect on vascular function20,21 | Toxicity | Other |
|---|---|---|---|---|---|
| 600 mg | ≈81 mg* | ↓ 26% | Mildly improved | Well tolerated | Dose used in OPT-CHF24 (n=450) |
| 300 mg | ↓ 44% | Moderately improved | Well tolerated | Dose used in vascular study20 (n=11) | |
| 600 mg | ↓ 61% | Markedly improved | Unknown | Dose used in vascular study21 (n=30) |
UA, uric acid.
Dose equivalent of oxypurinol 600 mg.
Randomization, Stratification and Blinding
At the baseline visit, patients who qualify are randomized to treatment using a permuted block randomization scheme stratified by clinical site. Study drug or matching placebo is started within 12 hours of completing the baseline visit. Randomization is performed using an automated web-based system administered by the Data Coordinating Center. Blinding of the study is preserved by the use of matching placebo capsules. Investigators are requested not to measure serum UA levels during the study. Given the well-known safety profile of allopurinol and lack of a specific antidote, it is anticipated that there will be no need to un-blind study drug.
Concomitant HF Medication and Management of Gout
Patients should be receiving a stable treatment regimen for HF for at least 2 weeks prior to randomization, and in the case of beta-blockers for at least 3 months. Regular intermittent use of supplemental diuretic doses (oral or intravenous) is permitted if used as part of a regular diuretic treatment regimen at baseline. Patients are excluded if they are taking allopurinol (or oxypurinol) or have taken one of these agents within 30 days of randomization. Patients with a history of gout may enter the trial as long as they are not currently treated with these agents and are unlikely to require these agents during the study. However, it is anticipated that enrollment of hyperuricemic patients with HF will include those at risk for developing gout during the course of the trial. In addition, the initiation of allopurinol itself may precipitate a gout flare.30 If this occurs and the patient's physician recommends use of open-label allopurinol (or oxypurinol), study drug will be permanently discontinued and the subject will continue with study visits through 24 weeks.
Risks of Treatment with Allopurinol
Allopurinol is a commonly used, FDA-approved medication for the treatment of gout, and chronic treatment is generally safe. The dose being evaluated in this study (600 mg orally in divided doses) is within the current standard of care for patients with gout, although doses used in clinical practice are typically lower, and the side effect profile is well characterized.31,32 This dose has also been studied in patients with mild-moderate HF21 as well as in patients with coronary artery disease,33,34 and shown to be well tolerated. Uncommon side effects include pruritus (3%), rash (1.5%), nausea or vomiting (1.3%), and renal failure (1.2%). Rare, serious adverse effects (less than 1%) include Stevens-Johnson syndrome, agranulocytosis, anemia, myelosuppression, and hepatotoxicity.
The Allopurinol Hypersensitivity Syndrome (AHS), which involves progression of skin rash to exfoliative lesions, generalized vasculitis and/or irreversible hepatotoxicity, occurs in less than 0.5% of patients, with a case fatality rate of up to 25%.32 Risk factors for AHS include renal dysfunction, recent onset allopurinol use and use in asymptomatic hyperuricemia.35 The keys to prevention and treatment are early recognition, drug withdrawal and supportive care. In the event of a new rash, the protocol requires that study drug be held until clinical assessment is made.
Study Endpoints
Primary Endpoint
The primary endpoint of EXACT-HF is a composite clinical endpoint (CCE) that classifies the subject's clinical status as improved, worsened, or unchanged at 24 weeks (Table 4), similar to that reported by Packer,36 with a slight modification as previously described.25 The classification follows sequential rules based on the outcomes of the following items:
Death: All-cause mortality will be used in the composite analysis, and adjudicated as due to HF, other cardiac cause, or non-cardiac cause.
Hospitalization, emergency room (ER) visit or emergent clinic visit for worsening HF: These events will also be adjudicated as due to HF, other cardiac, or non-cardiac.
Medication change for worsening HF: The investigator must prescribe or concur with: a) the addition of a new drug class for worsening HF, or 2) an increase in diuretic dose or an increase or decrease in beta-blocker or renin-angiotensin system inhibitor dose by at least 50% for more than one week. A newly added drug class is defined as the addition of a new pharmacologic agent specifically for HF therapy, or generally recognized as effective in the management of HF within current treatment guidelines.2
Patient Global Assessment (PGA): The 7-point PGA tool asks patients to define their current status relative to baseline as markedly improved, moderately improved, mildly improved, no change, slightly worse, moderately worse and markedly worse. It will be evaluated at 4, 12 and 24 weeks.
Table 4. Composite Clinical Endpoint.
| Improved | Worsened | Unchanged |
|---|---|---|
| Patient Global Assessment moderate or markedly improved | Death | Neither improved or worsened |
| Hospitalization, ER visit or emergent clinic visit for worsening HF | ||
| Medication change for worsening HF | ||
| Patient Global Assessment moderate or markedly worse |
ER, emergency room; HF, heart failure.
Secondary Endpoints
The principal secondary efficacy criteria in this study include the change in quality of life (QOL) as assessed by the Kansas City Cardiomyopathy Questionnaire (KCCQ) and the change in submaximal exercise capacity as assessed by 6-minute walk test (6-MWT), both at 12 and 24 weeks. The KCCQ is a self-administered, 23-item questionnaire developed to provide a better description of health-related QOL in patients with HF.37 It quantifies physical limitation, symptoms, QOL, social interference and self-efficacy. A clinical summary score is calculated by combining the functional status with the QOL and social limitation domains.
Because usual daily activities generally require much less than maximal exertion, the measurement of submaximal exercise capacity may provide information that is complementary to that provided by maximal exercise testing.38 The 6-MWT is the most common of the fixed-time tests. It is moderately predictive of maximal oxygen consumption, and independently predicts morbidity and mortality in HF.39,40
Tertiary Endpoints
Additional parameters that will be assessed for efficacy include NYHA functional class, echocardiographic measures of LV remodeling (LV volumes, stroke volume, ejection fraction and mass), HF biomarkers (uric acid, NT-proBNP), measures of renal function (serum creatinine, cystatin C, estimated GFR), markers of oxidative stress (malondialdehyde, nitrotyrosine and allantoin), total number of hospitalizations and hospital days, time to first HF hospitalization and cardiovascular death. In addition, increased diuretic requirement (defined as an increase in outpatient diuretic dose by at least 50% for more than one week) will be tracked.
Statistical Considerations
All analyses will be conducted using the intention to treat (ITT) principle with the minor modification as described below. The ITT population includes all patients who are randomized. Analysis of the primary efficacy CCE will utilize the Cochran-Mantel-Haenszel row mean score test with modified ridit scores to compare the distributions. The study is designed to test whether allopurinol is significantly more effective than placebo in patients with NYHA class II-IV HF and LVEF ≤ 40% receiving standard background therapy for HF. The test for the superiority of allopurinol versus placebo will be based on a chi-square statistic which compares the two randomized arms with respect to differences in a linear trend in the proportions of patients that fall into the ordinal categories of the primary endpoint.41
Sample Size and Power Calculation
Based on previous data from the OPT-CHF study,24 which used the same composite endpoint, it is assumed that the placebo arm will have approximately the following response rates for the primary endpoint: 33% improved, 42% unchanged and 25% worsened. We hypothesize that the outcome of the allopurinol arm will be superior, with response rates of approximately 52% improved, 37% unchanged, and 11% worsened. To estimate the statistical power of these assumptions, we randomly generated data sets to simulate the clinical trial, computed the Cochran-Mantel-Haenszel row mean score test statistic in each data set, and compared the resulting P value to the 0.05 level of significance. Based on 2,000 replicate samples, we estimated that a sample size of 250 patients would provide 83% power to detect a statistically significant difference using the row mean score statistic under the assumptions above. Additional calculations confirmed that a sample size of 250 subjects will also provide adequate power for other endpoints.
Safety
Although interim data analysis for the primary efficacy endpoint will not be conducted, safety data will be frequently assessed by a Data Safety Monitoring Board (DSMB). Appointed by the NHLBI, this independent committee of individuals with expertise in HF clinical trials will advise the NHLBI regarding the continuing safety of current participants and those yet to be recruited, as well as the continuing validity and scientific merit of the trial. The DSMB will also perform interim reviews of all-cause mortality, using the Haybittle-Peto boundary for interpreting mortality differences between the treatment arms. Information on adverse event definitions and reporting is provided in the supplemental online material.
Other Targets for Therapy
Increasing recognition that nitroso-redox imbalance can affect cardiac structure and function has led investigators to target XO in other cardiovascular disease states.4 Rekhraj et al.34 randomized 66 patients with ischemic heart disease and left ventricular hypertrophy to receive allopurinol 600 mg daily or placebo for 9 months. Compared to placebo, allopurinol significantly reduced LV mass and volumes (as assessed by cardiac magnetic resonance imaging), improved flow-mediated dilation, and was well tolerated. Others have demonstrated benefits of high-dose XO inhibition on symptoms and exercise tolerance in patients with stable angina.42 Both of these studies suggest that reducing myocardial and vascular XO activity underlies the benefit of allopurinol. However, while a reduction in systemic markers of oxidative stress has been demonstrated, these changes have not uniformly correlated with structural and functional improvements. More work is needed to understand the underlying mechanisms and pathobiology of enhanced XO activity in heart disease.43 In addition to cardiovascular disorders, allopurinol is currently undergoing investigation in non-cardiovascular disease states as diverse as sleep apnea, chronic kidney disease, sarcopenia, and intrauterine growth retardation.44 Finally, we aim to explore the role of chronic XO inhibition in improving insulin sensitivity in an EXACT-HF substudy (see Supplemental Material).45
Conclusions
Accumulating evidence suggests the potential efficacy and safety of XO inhibition in cardiovascular disease states in general, and HF in particular. Furthermore, a sub-group of analysis of the OPT-CHF study demonstrated a signal of benefit of XO inhibition in patients with HF and elevated uric acid levels. Against this background, we designed the EXACT-HF study to test the hypothesis that in patients with symptomatic HF due to LV systolic dysfunction, who have elevated serum uric acid levels, treatment with high-dose allopurinol for 24 weeks will improve clinical outcomes compared to treatment with placebo.
Supplementary Material
Acknowledgments
Sources of Funding: The Heart Failure Clinical Research Network is supported by the NHLBI, National Institutes of Health (U10HL084904 for the coordinating center; and U10HL084861, U10HL084875, U10HL084877, U10HL084889, U10HL084890, U10HL084891, U10HL084899, U10HL084907, and U10HL084931 for the clinical centers).
Footnotes
Disclosures: None.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127:e6–e245. doi: 10.1161/CIR.0b013e31828124ad. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:e391–e479. doi: 10.1161/CIRCULATIONAHA.109.192065. [DOI] [PubMed] [Google Scholar]
- 3.Mallat Z, Philip I, Lebret M, Chatel D, Maclouf J, Tedgui A. Elevated levels of 8-iso-prostaglandin F2alpha in pericardial fluid of patients with heart failure: a potential role for in vivo oxidant stress in ventricular dilatation and progression to heart failure. Circulation. 1998;97:1536–1539. doi: 10.1161/01.cir.97.16.1536. [DOI] [PubMed] [Google Scholar]
- 4.Karantalis V, Schulman IH, Hare JM. Nitroso-redox imbalance affects cardiac structure and function. J Am Coll Cardiol. 2013;61:933–935. doi: 10.1016/j.jacc.2012.12.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hare JM. Nitroso-redox balance in the cardiovascular system. N Engl J Med. 2004;351:2112–2114. doi: 10.1056/NEJMe048269. [DOI] [PubMed] [Google Scholar]
- 6.Anker SD, Doehner W, Rauchhaus M, Sharma R, Francis D, Knosalla C, Davos CH, Cicoira M, Shamim W, Kemp M, Segal R, Osterziel KJ, Leyva F, Hetzer R, Ponikowski P, Coats AJ. Uric acid and survival in chronic heart failure: validation and application in metabolic, functional, and hemodynamic staging. Circulation. 2003;107:1991–1997. doi: 10.1161/01.CIR.0000065637.10517.A0. [DOI] [PubMed] [Google Scholar]
- 7.Kittleson MM, St John ME, Bead V, Champion HC, Kasper EK, Russell SD, Wittstein IS, Hare JM. Increased levels of uric acid predict haemodynamic compromise in patients with heart failure independently of B-type natriuretic peptide levels. Heart. 2007;93:365–367. doi: 10.1136/hrt.2006.090845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nash HL, Fitz AE, Wilson WR, Kirkendall WM, Kioschos JM. Cardiorenal hemodynamic effects of ethacrynic acid. Am Heart J. 1966;71:153–165. doi: 10.1016/0002-8703(66)90178-5. [DOI] [PubMed] [Google Scholar]
- 9.Ogino K, Kato M, Furuse Y, Kinugasa Y, Ishida K, Osaki S, Kinugawa T, Igawa O, Hisatome I, Shigemasa C, Anker SD, Doehner W. Uric acid-lowering treatment with benzbromarone in patients with heart failure: a double-blind placebo-controlled crossover preliminary study. Circ Heart Fail. 2010;3:73–81. doi: 10.1161/CIRCHEARTFAILURE.109.868604. [DOI] [PubMed] [Google Scholar]
- 10.Leyva F, Anker S, Swan JW, Godsland IF, Wingrove CS, Chua TP, Stevenson JC, Coats AJ. Serum uric acid as an index of impaired oxidative metabolism in chronic heart failure. Eur Heart J. 1997;18:858–865. doi: 10.1093/oxfordjournals.eurheartj.a015352. [DOI] [PubMed] [Google Scholar]
- 11.Levy WC, Mozaffarian D, Linker DT, Sutradhar SC, Anker SD, Cropp AB, Anand I, Maggioni A, Burton P, Sullivan MD, Pitt B, Poole-Wilson PA, Mann DL, Packer M. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113:1424–1433. doi: 10.1161/CIRCULATIONAHA.105.584102. [DOI] [PubMed] [Google Scholar]
- 12.Ky B, French B, Levy WC, Sweitzer NK, Fang JC, Wu AH, Goldberg LR, Jessup M, Cappola TP. Multiple biomarkers for risk prediction in chronic heart failure. Circ Heart Fail. 2012;5:183–190. doi: 10.1161/CIRCHEARTFAILURE.111.965020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Thanassoulis G, Brophy JM, Richard H, Pilote L. Gout, allopurinol use, and heart failure outcomes. Arch Intern Med. 2010;170:1358–1364. doi: 10.1001/archinternmed.2010.198. [DOI] [PubMed] [Google Scholar]
- 14.Malek F, Ostadal P, Parenica J, Jarkovsky J, Vitovec J, Widimsky P, Linhart A, Fedorco M, Coufal Z, Miklik R, Kruger A, Vondrakova D, Spinar J. Uric acid, allopurinol therapy, and mortality in patients with acute heart failure--results of the Acute HEart FAilure Database registry. J Crit Care. 2012;27:737–24. doi: 10.1016/j.jcrc.2012.03.011. [DOI] [PubMed] [Google Scholar]
- 15.Gotsman I, Keren A, Lotan C, Zwas DR. Changes in uric acid levels and allopurinol use in chronic heart failure: association with improved survival. J Card Fail. 2012;18:694–701. doi: 10.1016/j.cardfail.2012.06.528. [DOI] [PubMed] [Google Scholar]
- 16.Murphy RM, Dutka TL, Lamb GD. Hydroxyl radical and glutathione interactions alter calcium sensitivity and maximum force of the contractile apparatus in rat skeletal muscle fibres. J Physiol. 2008;586:2203–2216. doi: 10.1113/jphysiol.2007.150516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ekelund UE, Harrison RW, Shokek O, Thakkar RN, Tunin RS, Senzaki H, Kass DA, Marban E, Hare JM. Intravenous allopurinol decreases myocardial oxygen consumption and increases mechanical efficiency in dogs with pacing-induced heart failure. Circ Res. 1999;85:437–445. doi: 10.1161/01.res.85.5.437. [DOI] [PubMed] [Google Scholar]
- 18.Cappola TP, Kass DA, Nelson GS, Berger RD, Rosas GO, Kobeissi ZA, Marban E, Hare JM. Allopurinol improves myocardial efficiency in patients with idiopathic dilated cardiomyopathy. Circulation. 2001;104:2407–2411. doi: 10.1161/hc4501.098928. [DOI] [PubMed] [Google Scholar]
- 19.Hirsch GA, Bottomley PA, Gerstenblith G, Weiss RG. Allopurinol acutely increases adenosine triphospate energy delivery in failing human hearts. J Am Coll Cardiol. 2012;59:802–808. doi: 10.1016/j.jacc.2011.10.895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Farquharson CA, Butler R, Hill A, Belch JJ, Struthers AD. Allopurinol improves endothelial dysfunction in chronic heart failure. Circulation. 2002;106:221–226. doi: 10.1161/01.cir.0000022140.61460.1d. [DOI] [PubMed] [Google Scholar]
- 21.George J, Carr E, Davies J, Belch JJ, Struthers A. High-dose allopurinol improves endothelial function by profoundly reducing vascular oxidative stress and not by lowering uric acid. Circulation. 2006;114:2508–2516. doi: 10.1161/CIRCULATIONAHA.106.651117. [DOI] [PubMed] [Google Scholar]
- 22.Cingolani HE, Plastino JA, Escudero EM, Mangal B, Brown J, Perez NG. The effect of xanthine oxidase inhibition upon ejection fraction in heart failure patients: La Plata Study. J Card Fail. 2006;12:491–498. doi: 10.1016/j.cardfail.2006.05.005. [DOI] [PubMed] [Google Scholar]
- 23.Erdogan D, Tayyar S, Uysal BA, Icli A, Karabacak M, Ozaydin M, Dogan A. Effects of allopurinol on coronary microvascular and left ventricular function in patients with idiopathic dilated cardiomyopathy. Can J Cardiol. 2012;28:721–727. doi: 10.1016/j.cjca.2012.04.005. [DOI] [PubMed] [Google Scholar]
- 24.Hare JM, Mangal B, Brown J, Fisher C, Jr, Freudenberger R, Colucci WS, Mann DL, Liu P, Givertz MM, Schwarz RP. Impact of oxypurinol in patients with symptomatic heart failure. Results of the OPT-CHF study. J Am Coll Cardiol. 2008;51:2301–2309. doi: 10.1016/j.jacc.2008.01.068. [DOI] [PubMed] [Google Scholar]
- 25.Freudenberger RS, Schwarz RP, Jr, Brown J, Moore A, Mann D, Givertz MM, Colucci WS, Hare JM. Rationale, design and organisation of an efficacy and safety study of oxypurinol added to standard therapy in patients with NYHA class. Expert Opin Investig Drugs. 2004;13:1509–1516. doi: 10.1517/13543784.13.11.1509. [DOI] [PubMed] [Google Scholar]
- 26.Setoguchi S, Stevenson LW, Schneeweiss S. Repeated hospitalizations predict mortality in the community population with heart failure. Am Heart J. 2007;154:260–266. doi: 10.1016/j.ahj.2007.01.041. [DOI] [PubMed] [Google Scholar]
- 27.Januzzi JL, Troughton R. Are serial BNP measurements useful in heart failure management? Serial natriuretic peptide measurements are useful in heart failure management. Circulation. 2013;127:500–507. doi: 10.1161/CIRCULATIONAHA.112.120485. [DOI] [PubMed] [Google Scholar]
- 28. [accessed March 30, 2013];2013 http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=13564.
- 29.Day RO, Graham GG, Hicks M, McLachlan AJ, Stocker SL, Williams KM. Clinical pharmacokinetics and pharmacodynamics of allopurinol and oxypurinol. Clin Pharmacokinet. 2007;46:623–644. doi: 10.2165/00003088-200746080-00001. [DOI] [PubMed] [Google Scholar]
- 30.Borstad GC, Bryant LR, Abel MP, Scroggie DA, Harris MD, Alloway JA. Colchicine for prophylaxis of acute flares when initiating allopurinol for chronic gouty arthritis. J Rheumatol. 2004;31:2429–2432. [PubMed] [Google Scholar]
- 31.Chao J, Terkeltaub R. A critical reappraisal of allopurinol dosing, safety, and efficacy for hyperuricemia in gout. Curr Rheumatol Rep. 2009;11:135–140. doi: 10.1007/s11926-009-0019-z. [DOI] [PubMed] [Google Scholar]
- 32.Dalbeth N, Stamp L. Allopurinol dosing in renal impairment: walking the tightrope between adequate urate lowering and adverse events. Semin Dial. 2007;20:391–395. doi: 10.1111/j.1525-139X.2007.00270.x. [DOI] [PubMed] [Google Scholar]
- 33.Rajendra NS, Ireland S, George J, Belch JJ, Lang CC, Struthers AD. Mechanistic insights into the therapeutic use of high-dose allopurinol in angina pectoris. J Am Coll Cardiol. 2011;58:820–828. doi: 10.1016/j.jacc.2010.12.052. [DOI] [PubMed] [Google Scholar]
- 34.Rekhraj S, Gandy SJ, Szwejkowski BR, Nadir MA, Noman A, Houston JG, Lang CC, George J, Struthers AD. High-dose allopurinol reduces left ventricular mass in patients with ischemic heart disease. J Am Coll Cardiol. 2013;61:926–932. doi: 10.1016/j.jacc.2012.09.066. [DOI] [PubMed] [Google Scholar]
- 35.Lee HY, Ariyasinghe JT, Thirumoorthy T. Allopurinol hypersensitivity syndrome: a preventable severe cutaneous adverse reaction? Singapore Med J. 2008;49:384–387. [PubMed] [Google Scholar]
- 36.Packer M. Proposal for a new clinical end point to evaluate the efficacy of drugs and devices in the treatment of chronic heart failure. J Card Fail. 2001;7:176–182. doi: 10.1054/jcaf.2001.25652. [DOI] [PubMed] [Google Scholar]
- 37.Green CP, Porter CB, Bresnahan DR, Spertus JA. Development and evaluation of the Kansas City Cardiomyopathy Questionnaire: a new health status measure for heart failure. J Am Coll Cardiol. 2000;35:1245–1255. doi: 10.1016/s0735-1097(00)00531-3. [DOI] [PubMed] [Google Scholar]
- 38.Larsen AI, Aarsland T, Kristiansen M, Haugland A, Dickstein K. Assessing the effect of exercise training in men with heart failure; comparison of maximal, submaximal and endurance exercise protocols. Eur Heart J. 2001;22:684–692. doi: 10.1053/euhj.2000.2286. [DOI] [PubMed] [Google Scholar]
- 39.Cahalin LP, Mathier MA, Semigran MJ, Dec GW, DiSalvo TG. The six-minute walk test predicts peak oxygen uptake and survival in patients with advanced heart failure. Chest. 1996;110:325–332. doi: 10.1378/chest.110.2.325. [DOI] [PubMed] [Google Scholar]
- 40.Bittner V, Weiner DH, Yusuf S, Rogers WJ, McIntyre KM, Bangdiwala SI, Kronenberg MW, Kostis JB, Kohn RM, Guillotte M. Prediction of mortality and morbidity with a 6-minute walk test in patients with left ventricular dysfunction. SOLVD Investigators. JAMA. 1993;270:1702–1707. [PubMed] [Google Scholar]
- 41.Chapman DG, Nam JM. Asymptotic power of chi square tests for linear trends in proportions. Biometrics. 1968;24:315–327. [PubMed] [Google Scholar]
- 42.Noman A, Ang DS, Ogston S, Lang CC, Struthers AD. Effect of high-dose allopurinol on exercise in patients with chronic stable angina: a randomised, placebo controlled crossover trial. Lancet. 2010;375:2161–2167. doi: 10.1016/S0140-6736(10)60391-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Stone PH. Allopurinol a new anti-ischemic role for an old drug. J Am Coll Cardiol. 2011;58:829–830. doi: 10.1016/j.jacc.2011.02.072. [DOI] [PubMed] [Google Scholar]
- 44. [Accessed April 1, 2013];2013 http://clinicaltrials.gov/ct2/show/NCT00987415?term=exact-hf&rank=1.
- 45.Kim JA, Montagnani M, Koh KK, Quon MJ. Reciprocal relationships between insulin resistance and endothelial dysfunction: molecular and pathophysiological mechanisms. Circulation. 2006;113:1888–1904. doi: 10.1161/CIRCULATIONAHA.105.563213. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.