

Abstract
The aim of this research is to determine the prevalence of soft tissue calcifications detectable on panoramic radiographs, in the mandibular angle area. 3,028 digital panoramic radiographs taken between June 2009 and June 2011 were evaluated. Soft tissue calcifications found in the mandibular angle area were recorded according to gender, age and bilaterality. Data were analyzed with the Chi squared test and Fisher’s exact test, with α< 0.05 being considered statistically significant. The panoramic radiographs analyzed revealed a total of 79 calcifications (2.61%) in 75 individuals, of which 55.7% were women and 44.3% were men. The calcifications found were tonsilloliths (56%), carotid artery calcification (29%), sialoliths (11%), calcified lymph nodes (4%). A statistically significant link was found between being over age 40 with tonsilloliths (p<0.001) and calcifications of the carotid artery (p<0.001). In terms of gender, men had a higher likelihood of tonsilloliths (p=0.007). Conclusions There is a low prevalence of soft tissue calcifications detectable on panoramic radiographs, which increases with age.
Keywords: Panoramic radiography, calcifications, calcinosis
Introduction
Soft tissue calcifications in the maxillofacial area are uncommon, and generally correspond to radiographic findings in routine examinations such as panoramic radiographs. The most important diagnostic criteria are anatomical location, distribution, number, size and shape of the calcifications [1]. The differential diagnosis must be made with hyoid bone, triticeous cartilage, styloid process, superior horn of thyroid cartilage and epiglottis. Epidemiologically, these calcifications are most frequently found in individuals over age 40, however, a few cases of children have been reported [2]. Additionally, Freitas [1] and White [3] presented a classification that could be useful in the diagnosis.
The few studies conducted regarding calcified lymph nodes deal with the diagnosis by means of ultrasonography and computerized tomography. Eisenkraft [4] studied 2,300 CT scans of the cervical area, of which 26 (1%) presented lymph node calcification without determining if it was benign or malignant. Ram [5] and De Moura [6] reported cases of patients with tonsilloliths found on panoramic radiographs that were later confirmed by CT scan. Cogolludo [7] and Silvestre [8] also reported cases of calcifications in patients with symptomatology analyzed by CT scan.
It has been indicated that the prevalence of carotid artery calcifications is between 3% to 5% of the general population [9-13], although the link between carotid artery calcifications detectable on panoramic radiographs, cardiovascular risk factors and a potential stroke remains controversial [14]. Nevertheless, most of the studies found are consistent in the high diagnostic and preventive value of panoramic radiography in detecting atheromas [9,10,13,15-21].
Another pathology that exhibits calcifications is sialolithiasis, the most common disease in the greater salivary glands after parotiditis with a higher incidence in men aged between 30 and 60 years [22]. Finally, the phleboliths are idiopathic calcifications of the thrombus, which are frequently associated with vascular lesions in the head and neck [23].
Considering the broad range of pathologies and the low research in recent years, the aim of this investigation is to identify calcifications in the mandibular angle area by analyzing digital panoramic radiographs.
Materials and methods
Patient selection
A population-based descriptive study was designed to evaluate 3,028 digital panoramic radiographs of patients who attended a private radiology center (Temuco, Chile) for the analysis and diagnosis of pathologies linked to implantology, orthodontics, oral surgery or general diagnosis between June 2009 and June 2011. The patients with facial deforming pathologies or maxillofacial operations associated with trauma or surgical resection of bone were excluded. All panoramic radiographs of subjects were included with no discrimination of age or gender.
Image acquisition
The panoramic radiographs were obtained from an orthopantomographic device, Instrumentarium 0P200 D, Finland, 2008, using Cliniview XV software on a LG 19” Flatron monitor. The radiographic images were taken by a specially trained assistant, with kV 66, mA 5-10 and an exposure time of 17.6 seconds. The images were approved by a oral and maxillofacial radiologist with 6 years of experience; later the same professional performed the evaluations to determine the study variables.
Image analysis
The presence of radiopacities over projected on compatible mandibles with calcifications and with a ghost image on the opposite side were studied as well as their uni- or bilateral characteristics. The area between the anterior border of the cervical spine, inferior border of the mandibular body and posterior border of the ramus and mandibular angle was assessed. The images where no cervical spine was observed were also included due to the possibility of finding calcifications close to the mandibular angle. Those images with an ambiguous diagnosis due to over projection of structures or lack of clarity were discarded (Figure 1).
Figure 1.
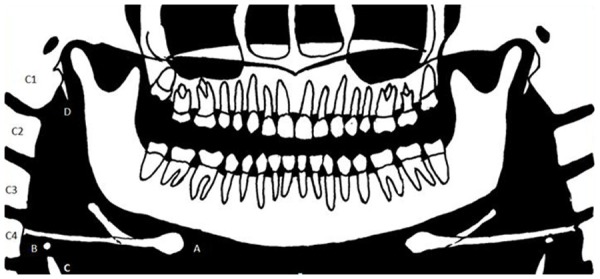
Structures on panoramic radiograph. At level of mandibular angle, the differential diagnosis among soft tissue calcifications is with: hyoid bone (A), superior horn of thyroid cartilage (C), triticeous cartilage (B) and with ossification of stylohyoid ligament, mainly in the portion next to the lesser spear of the hyoid bone.
The panoramic radiographs were observed on full screen; overexposed images or those with a greater density in the study area due to the presence of an airway were clarified using the software at two points so slightly calcified areas could be observed. Additionally, the compatible areas with calcifications and that had low radiopacity were evaluated using a software tool with a magnification of 2x. Only the radiopacities compatible with calcification were included; ossification of the stylohyoid ligament was excluded.
Statistical analysis
The statistics software Stata 9.0/SE was used, applying the Chi squared test and Fisher’s exact test; α=0.05 was considered statistically significant.
Results
Of the 3,028 panoramic radiographs analyzed 1,838 were women and 1,190 were men. The patients’ ages at the time the panoramic radiographs were taken ranged from 3 to 90 years, with a mean of 28 years (SD: 18.5) (Figure 2).
Figure 2.
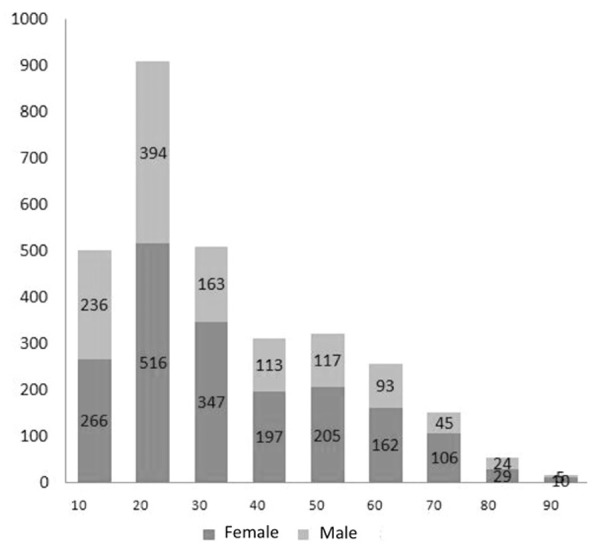
Age distribution and proportion of men and women.
A total of 79 calcifications (2.61%) were identified in 75 individuals, of which 44 (55.7%) were women and 35 (44.3%) were men. The proportion of calcification according to age group is shown in Figure 3. Of the individuals in whom calcifications were found, 25 (33.33%) were 40 years of age or younger, and 50 (66.66%) were over age 40 (Table 1).
Figure 3.
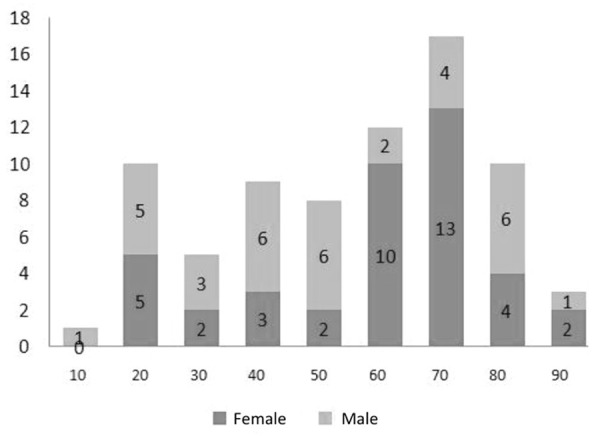
Distribution of calcifications according to gender and age.
Table 1.
Soft tissue calcifications in mandibular angle area related to age of patient
| Calcification | 3-40 year old | 40-90 year old | p | ||
|---|---|---|---|---|---|
|
| |||||
| n | % | n | % | ||
| Calcification of ganglion | 1 | 0.04 | 2 | 0.25 | 0.171 |
| Tonsilloliths | 19 | 0.85 | 25 | 3.14 | <0.001* |
| Carotid artery calcification | 1 | 0.04 | 22 | 2.76 | <0.001* |
| Calcification of salivary gland | 4 | 0.18 | 5 | 0.63 | 0.059 |
Statistically significant (Chi Square and Exact Fisher test).
The calcifications found were tonsilloliths, atheromas, sialoliths and calcified lymph nodes; no images compatible with phleboliths were found on the images (Figure 4). With respect to the presence of calcifications in terms of gender, only statistically significant differences were found in tonsilloliths (p=0.007) (Table 2).
Figure 4.
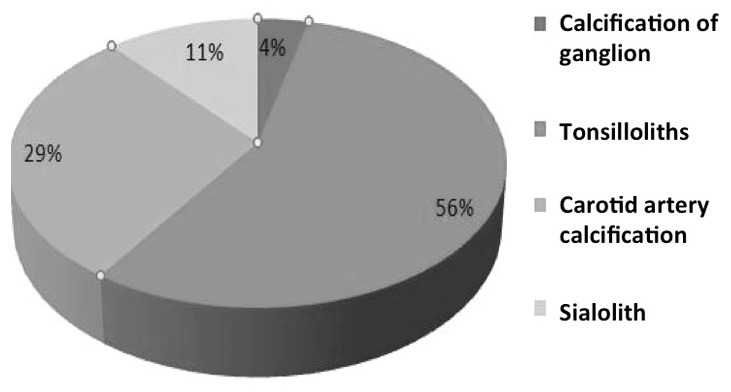
Distribution of calcifications.
Table 2.
Soft tissue calcifications in mandibular angle area related to the sex of patient
| Calcification | Female | Male | p | ||
|---|---|---|---|---|---|
|
| |||||
| n | % | n | % | ||
| Calcification of ganglion | 1 | 0.05 | 2 | 0.17 | 0.565 |
| Tonsilloliths | 18 | 0.98 | 26 | 2.18 | 0.007* |
| Carotid artery calcification | 18 | 0.98 | 5 | 0.42 | 0.090 |
| Calcification of salivary gland | 7 | 0.38 | 2 | 0.17 | 0.497 |
Statistically significant (Chi Square and Exact Fisher test).
A large number of the calcifications found were small, of low density and unilateral. There were no significant differences with regard to the uni- or bilaterality of the calcifications and there were also no significant differences in terms of laterality and gender.
Discussion
This study presents the classic limitations of cross-sectional studies, where it is not possible to obtain the patient’s entire history. Moreover, there is a bias in there being no other studies to corroborate the findings on the panoramic radiography; however, the size of the sample being 3,028 panoramic images makes it possible to gain valuable information and orient future investigations in this field.
According to the authors’ search, after the study published by Monsour [24], there are no other studies of prevalence in the literature regarding calcifications detectable on panoramic radiographs. In this study, a prevalence of 2.61% of the presence of calcifications was found on the panoramic radiographs, while Monsour [24] found calcifications in 4% of a total of 2,628 non-digital panoramic radiographs. The low percentage of radiopacities found in our study could significantly increase if it were to include ossification of the stylohyoid ligament or the elongated styloid process, a pathology not analyzed here as it deals with organized bone formation and not calcium salt deposits at the soft tissue level.
In addition, this study uses digital panoramic radiographs which, unlike the study by Monsour [24], which enables low density calcifications to be identified, given that the density characteristics and image contrast can be modified and/or magnified.
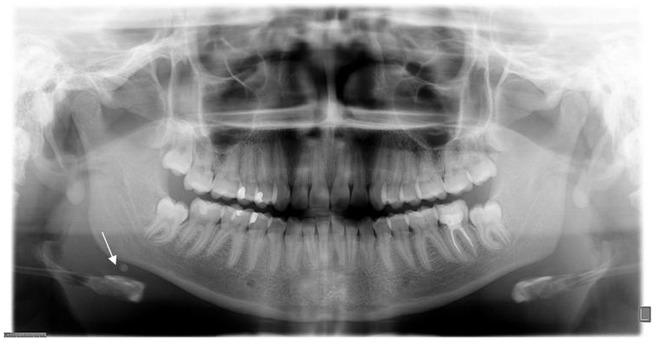
Tonsilloliths
These mainly produce a ghost artifact or image on the contralateral side, generally from above, which is related to what was suggested by Ram [5] and Monsour [24]. Although tonsilloliths are uncommon, radiopaque masses over projected on the mandibular ramus must be considered in the differential diagnosis in such a way that other studies, such as computerized tomography or magnetic resonance, maybe needed to define ghost images or a truly bilateral pathology (Figure 5).
Figure 5.
Tonsilloliths over-projected in right mandibular ramus, ghost image in left mandibular ramus.
We observed the presence of tonsilloliths in a broad age range, with the youngest patient being 10. Most of the tonsilloliths were observed in patients over age 40, with statistically significant differences being found between this group and those under 40, partially concurring with Monsour [24].
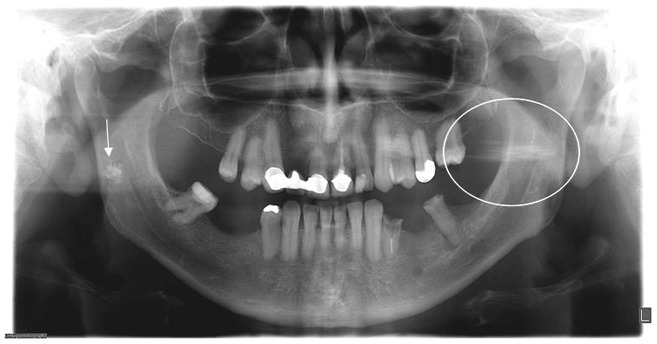
Carotid artery calcification
Most studies dealing with soft tissue calcification correspond to calcifications of atheromatous plaque at the bifurcation level of the carotid artery. Its prevalence is between 3% and 5% of the population [9-13]. In our study, a prevalence of 2.76% of atheromas was observed in the population aged over 40.
It is worthy of note that Kamikawa [25] conducted a study on cadavers, where the area of carotid bifurcation and triticeous cartilage was marked with gutta-percha, determining a wide variability between observers in recognizing the anatomical structures, which is indicative of the difficulty in determining calcifications of the carotid artery on panoramic radiographs and the probable diagnostic error in detection. In the observation from the anterior zone to the cervical spine, at C3 and C4, a differential diagnosis must be made with calcified lymph nodes, superior horn of thyroid cartilage and mainly triticeous cartilage. In our study, the images compatible with atheroma were observed to be of a low density, irregular edges and elongated (Figure 6).
Figure 6.
Bilateral carotid artery calcifications at level of third cervical vertebra. Superior horn of thyroid cartilage and triticeous cartilage observable at level of fourth cervical vertebra.
Bayer [13] reported that the images compatible with carotid artery calcification were more common in women (64.8%) than in men (32.5%). Our study is consistent with Bayer et al. [13], although with a higher percentage difference between men (22%) and women (78%). Phleboliths and other calcifications were not observed in this research.
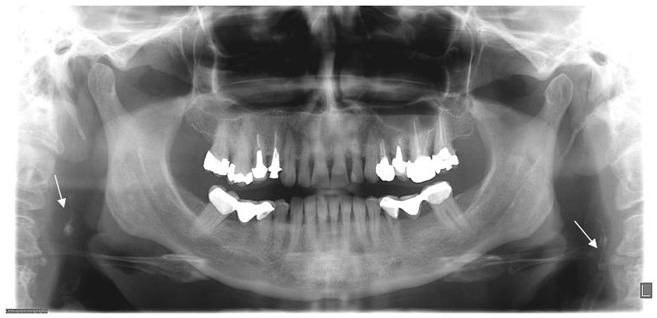
Calcification in salivary glands
In this sample, no images were observed to be over projected on the mandibular body or dental roots that were compatible with calcifications of the submandibular gland. These calcifications were observed under the mandibular border (Figure 7).
Figure 7.
Sialolith under right mandibular border.
El Deeb [22] reported that sialolithiasis affects 0.01% to 1% of the population, which is consistent with our results, as we found sialoliths in 0.3% of the general population. However, there are differences with this study regarding gender; Deeb [22] found a greater prevalence in men and our study observed a greater prevalence in women. In terms of age, a greater prevalence has been reported in the group aged between 30 and 60 [22,26], although in our investigation no differences were observed in the groups older and younger than 40.
Finally, we can conclude that the presence of calcifications on panoramic radiographs has a low prevalence, but their detection is important to orient the diagnosis and prevention of diseases. Other studies are needed to confirm the presence and severity of the different calcifications presented here.
Disclosure of conflict of interest
None.
References
- 1.White S, Pharoah M. Radiología Oral: principios e interpretación. 1st ed. Barcelona: Harcourt; 2002. pp. 552–65. [Google Scholar]
- 2.Thakur J, Minhas R, Thakur A, Sharma D, Mohindroo N. Giant tonsillolith causing odynophagia in a child: a rare case report. Cases J. 2008;1:50. doi: 10.1186/1757-1626-1-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Freitas A, Rosa J, Souza I. Radiología Odontológica. 6ª ed. São Paulo: Artes Médicas; 2004. pp. 102–155. [Google Scholar]
- 4.Eisenkraft BL, Som PM. The spectrum of benign and malignant etiologies of cervical node calcification. AJR Am J Roentgenol. 1999;172:1433–1437. doi: 10.2214/ajr.172.5.10227533. [DOI] [PubMed] [Google Scholar]
- 5.Ram S, Siar CH, Ismail SM, Prepageran N. Pseudo bilateral tonsilloliths: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:110–114. doi: 10.1016/j.tripleo.2003.11.015. [DOI] [PubMed] [Google Scholar]
- 6.De Moura M, Madureira D, Noman-Ferreira L, Abdo E, Aguiar E, Freire A. Tonsillolith: A report of three clinical cases. Med Oral Patol Oral Cir Bucal. 2007;12:E130–133. [PubMed] [Google Scholar]
- 7.Cogolludo F, Martín G, Olalla A, Poch J. A propósito de un caso: gran tonsilolito en amígdala palatine. Acta Otorrinolaringol Esp. 2002;53:207–210. doi: 10.1016/s0001-6519(02)78302-7. [DOI] [PubMed] [Google Scholar]
- 8.Silvestre F, Pla A, Estelles E, Martinez V. Giant tonsillolith: Report of a case. Med Oral Patol Oral Cir Bucal. 2005;10:239–242. [PubMed] [Google Scholar]
- 9.Friedlander A, Gratt B. Panoramic dental radiography as an aid in detecting patients at risk for stroke. J Oral Maxillofac Surg. 1994;52:1257–1262. doi: 10.1016/0278-2391(94)90047-7. [DOI] [PubMed] [Google Scholar]
- 10.Friedlander AH. Panoramic radiography: the differential diagnosis of carotid artery atheromas. Spec Care Dentist. 1995;15:223–227. doi: 10.1111/j.1754-4505.1995.tb00522.x. [DOI] [PubMed] [Google Scholar]
- 11.Carter L, Haller A, Nadarajah V, Calamel A, Aguirre A. Use of panoramic radiography among an ambulatory dental population to detect patients at risk of stroke. J Am Dent Assoc. 1997;128:977–984. doi: 10.14219/jada.archive.1997.0338. [DOI] [PubMed] [Google Scholar]
- 12.Almog DM, KIllig KA, Carter LC, Friedlander AH, Brooks SL, Grimes RM. Diagnosis of non-dental conditions. Carotid artery calcifications on panoramic radiographs identify patients at risk for stroke. N Y State Dent J. 2004;70:20–25. [PubMed] [Google Scholar]
- 13.Bayer S, Helfgen EH, Bös C, Kraus D, Enkling N, Mues S. Prevalence of findings compatible with carotid artery calcifications on dental panoramic radiographs. Clin Oral Investig. 2011;15:563–569. doi: 10.1007/s00784-010-0418-6. [DOI] [PubMed] [Google Scholar]
- 14.Mupparapu M, Kim I. Calcified carotid artery atheroma and stroke: A systematic review. J Am Dent Assoc. 2007;138:483–492. doi: 10.14219/jada.archive.2007.0200. [DOI] [PubMed] [Google Scholar]
- 15.Ravon NA, Hollender LG, McDonald V, Persson GR. Signs of carotid calcification from dental panoramic radiographs are in agreement with Doppler sonography results. J Clin Periodontol. 2003;30:1084–1090. doi: 10.1046/j.0303-6979.2003.00427.x. [DOI] [PubMed] [Google Scholar]
- 16.Tamura T, Inui M, Nakase M, Nakamura S, Okumura K, Tagawa T. Clinicostatistical study of carotid calcification on panoramic radiographs. Oral Dis. 2005;11:314–317. doi: 10.1111/j.1601-0825.2005.01125.x. [DOI] [PubMed] [Google Scholar]
- 17.Madden RP, Hodges JS, Salmen CW, Rindal DB, Tunio J, Michalowicz BS, Ahmad M. Utility of panoramic radiographs in detecting cervical calcified carotid atheroma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:543–548. doi: 10.1016/j.tripleo.2006.06.048. [DOI] [PubMed] [Google Scholar]
- 18.Kumagai M, Yamagishi T, Fukui N, Chiba M. Carotid artery calcification seen on panoramic dental radiographs in the Asian population in Japan. Dentomaxillofac Radiol. 2007;36:92–96. doi: 10.1259/dmfr/79378783. [DOI] [PubMed] [Google Scholar]
- 19.Uthman AT, Al-Saffar AB. Prevalence in digital panoramic radiographs of carotid area calcification among Iraqi individuals with stroke-related disease. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:e68–73. doi: 10.1016/j.tripleo.2007.11.009. [DOI] [PubMed] [Google Scholar]
- 20.Romano-Sousa C, Krejci L, Martins F, Graciosa filho R, Fonseca M, Novaes V, Fenyo-Pereira M. Diagnostic agreement between panoramic radiographs and color doppler images of carotid atheroma. J Appl Oral Sci. 2009;17:45–48. doi: 10.1590/S1678-77572009000100009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ertas ET, Sisman Y. Detection of incidental carotid artery calcifications during dental examinations: panoramic radiography as an important aid in dentistry. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112:11–17. doi: 10.1016/j.tripleo.2011.02.048. [DOI] [PubMed] [Google Scholar]
- 22.El Deeb M, Holte N, Gorlin RJ. Submandibular salivary gland sialoliths perforated through the oral floor. Oral Surg Oral Med Oral Pathol. 1981;51:134–139. doi: 10.1016/0030-4220(81)90029-3. [DOI] [PubMed] [Google Scholar]
- 23.Scolozzi P, Laurent F, Lombardi T, Richter M. Intraoral venous malformation presenting with multiple phleboliths. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:197–200. doi: 10.1016/s1079-2104(03)00098-2. [DOI] [PubMed] [Google Scholar]
- 24.Monsour P, Romaniuk K, Hutchings R. Soft tissue calcifications in the differential diagnosis of opacities superimposed over the mandible by dental panoramic radiography. Aust Dent J. 1991;36:94–101. doi: 10.1111/j.1834-7819.1991.tb01336.x. [DOI] [PubMed] [Google Scholar]
- 25.Kamikawa RS, Fenyo-Pereira M, Fernandes MA, Meurer MI. Study of the localization of radiopacities similar to calcified carotid atheroma by means of panoramic radiography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:374–378. doi: 10.1016/j.tripleo.2005.03.030. [DOI] [PubMed] [Google Scholar]
- 26.Andretta M, Tregnaghi A, Prosenikliev V, Staffieri A. Current opinions in sialolithiasis diagnosis and treatment. Acta Otorhinolaryngol Ital. 2005;25:145–149. [PMC free article] [PubMed] [Google Scholar]