

Abstract
The purpose of this study was to quantify head impact exposure (frequency, location and magnitude of head impacts) for individual male and female collegiate ice hockey players and to investigate differences in exposure by sex, player position, session type, and team. Ninety-nine (41 male, 58 female) players were enrolled and 37,411 impacts were recorded over three seasons. Frequency of impacts varied significantly by sex (males: 287 per season, females: 170, p<0.001) and helmet impact location (p<0.001), but not by player position (p=0.088). Head impact frequency also varied by session type; both male and female players sustained more impacts in games than in practices (p<0.001), however the magnitude of impacts did not differ between session types. There was no difference in 95th percentile peak linear acceleration between sexes (males: 41.6g, females: 40.8g), but 95th percentile peak rotational acceleration and HITsp (a composite severity measure) were greater for males than females (4424, 3409 rad/s2, and 25.6, 22.3, respectively). Impacts to the back of the helmet resulted in the greatest 95th percentile peak linear accelerations for males (45.2g) and females (50.4g), while impacts to the side and back of the head were associated with the greatest 95th percentile peak rotational accelerations (males: 4719, 4256 rad/sec2, females: 3567, 3784 rad/sec2 respectively). It has been proposed that reducing an individual’s head impact exposure is a practical approach for reducing the risk of brain injuries. Strategies to decrease an individual athlete’s exposure need to be sport and gender specific, with considerations for team and session type.
Keywords: impact biomechanics, hockey, gender, concussion
Introduction
Sports related concussions are a growing public health problem that affects millions of individuals in the United States (Langlois et al., 2006). Of particular concern are athletes who participate in contact sports, who are not only at risk for multiple concussions whose cumulative effects are not know (Thurman et al., 1998), but who are also exposed to repetitive head impacts, which have been suggested as a possible cause of chronic brain injury (Chamard et al., 2012; Koerte et al., 2012a, 2012b). Female participation in contact sports has been steadily increasing in the United States since the inception of Title IX in 1972. Research conducted in contact sports where male and females participate at the same level, such as ice hockey, has shown that females are at a higher risk of concussion (0.82/1000 athletic exposures (AE)) than their male counterparts (0.72/1000 AE)(Dick, 2009), but the reasons for this are not well understood.
It has been accepted that the mechanism of concussion is related to accelerations of the head after a direct or indirect impact to the head or body (McCrory et al., 2009), but the exact relationship between the biomechanics of head impacts and clinical outcome is unknown (Duhaime et al., 2012). While the kinematics of head impacts associated with injury are important to understand, it has been proposed that it is equally important to examine impacts that are not associated with diagnosis of concussion (Hutchison, 2011). Evaluating the biomechanics of all impacts may lead to a better understanding of the relative risk of head impacts, while also allowing for the evaluation of the relationship between repetitive impacts and long term cognitive deficits.
Several recent studies have focused on understanding the biomechanics of head impacts sustained in contact sports by utilizing an accelerometer-based head impact monitoring device, the Head Impact Telemetry (HIT) System (Simbex, Lebanon, NH). The HIT System allows researchers to monitor and record head impacts sustained by individual helmeted athletes during play. Utilizing this system and the unique laboratory that the playing field provides, researchers have directly measured the frequency, magnitude, and location of head impacts in a variety of sports (boxing, soccer, skiing), however the majority of studies have focused on football and ice hockey (Broglio et al., 2009; Brolinson et al., 2006; Crisco et al., 2012, 2010; Mihalik et al., 2012, 2008). In our approach to understanding the biomechanics of concussions, we have used data collected by the HIT System to quantify head impact exposure, a multifactorial term that includes the frequency, magnitude, and impact location of head impacts for individual athletes. Previously, we have quantified and reported head impact exposure by specific player positions in collegiate football players (Crisco et al., 2011). In a subsequent study, where this analysis was expanded to impacts associated with diagnosed concussions, we found that a relationship exists between head impact exposure and diagnosis of concussion (Beckwith et al., 2013). Based on these findings, we have proposed that reducing an individual’s head impact exposure is a practical approach for reducing the risk of brain injuries (Crisco and Greenwald, 2011).
Considering the high rate of concussions in ice hockey, the relative youth of its players, and the fact that both males and females participate, the expansion to and application of our previously used methods for quantifying head impact exposure to hockey is warranted. The only previous study of collegiate hockey players compared distributions of head impact exposure between sexes and reported that males experience a higher number of impacts than females and also sustain head impacts greater in magnitude (Brainard et al., 2012). While the study provided valuable insights into sex differences in the biomechanics of head impacts sustained in collegiate ice hockey, it did not provide a player-specific, detailed analysis of the exposure to all head impacts for individual players by sex, position, session type, or team.
The aim of this study was to quantify the frequency, magnitude, and location on the helmet of all head impacts sustained by individual collegiate male and female ice hockey players. Specifically, we tested the hypothesis that male hockey players would have a higher frequency of head impacts and would sustain head impacts that resulted in greater magnitudes than female players. We also tested the null hypotheses that head impact frequency, location, and magnitude sustained by individual athletes would not differ by player position, session type, or team.
Methods
Ninety-nine (41 male and 58 female) players from two men’s and two women’s National Collegiate Athletic Association (NCAA) hockey programs (Brown University and Dartmouth College, teams denoted arbitrarily as M1, M2 for males and F1, F2 for females) participated in this observational study after informed consent was obtained with institutional review board approval. Teams M1, F1, and F2 participated during the 2009–2010, 2010–2011, and 2011–2012 hockey seasons, while team M2 participated in a single season (2010–2011). Thirty males and 19 females were monitored during one season, 5 males and 20 females during two seasons, and 6 males and 19 females during three seasons. Players were categorized into one of two positions, forward or defense. Goalies were not included in this study. Of the 41 male players, 16 were defenders and 25 were forwards. The 58 female players included 21 defenders and 37 forwards.
Players wore S9 Easton (Van Nuys, CA) or CCM Vector (Reebok-CCM Hockey, Inc., Montreal, Canada) helmets instrumented with the HIT System. The HIT System measures and records biomechanical data from head impacts including linear and rotational acceleration at the head center of gravity (CG) and impact location on the helmet. The instrumented helmets were equipped with six single-axis accelerometers arranged tangentially to the head and mounted elastically within the helmet’s foam liner to maintain contact with the head and decouple shell vibrations (Brainard et al., 2012; Manoogian et al., 2006; Mihalik et al., 2008). The system collects acceleration data at 1 kHz, time stamps and stores the data on the helmet. Data are then transmitted by radiofrequency telemetry to a computer and entered into a secure database. System design, validation, accuracy, and data reduction methods have been previously described in detail (Crisco et al., 2004; Gwin et al., 2009, 2006; Mihalik et al., 2012, 2010a, 2010b, 2008; Wilcox et al., 2013).
Head impact exposure, including frequency of head impacts, magnitude of head impacts and impact location on the helmet for individual players, was quantified. This was accomplished using previously established methods used to quantify head impact exposure in collegiate football players (Crisco et al., 2012, 2011, 2010). A session was defined as either a practice or a game. An individual participated in a session when the player was present and partook in a game or practice, regardless of whether they sustained an impact during that particular session. Practices were sessions where players wore protective equipment with the potential of head contact. Game sessions included both competitions and scrimmages. Five measures of impact frequency were computed for each player: practice impacts, game impacts, impacts per season, impacts per practice, and impacts per game. Practice impacts and game impacts are the total number of head impacts for a player during all practices and all games, respectively. To calculate the number of impacts per game and per practice, the frequency of impacts players received was normalized by the number of sessions the player participated in. This accounted for differences in schedules and player attendance. Impacts per season, per game, and per practice are the average number of head impacts for a player during all sessions in a single season, during all games, and during all practices, respectively.
Impact magnitude variables included peak linear acceleration (g), peak rotational acceleration (rad/s2), and HITsp. HITsp is a composite measure of head impact severity that includes linear and rotational acceleration, impact duration, and impact location (Greenwald et al., 2008). Each individual player’s distribution of peak linear acceleration (g), peak rotational acceleration (rad/s2), and HITsp were quantified by the 50th and 95th percentile value of all seasonal impacts. Additionally, impacts were further reduced for analysis by computing the 50th and 95th percentile value of all seasonal impacts at each location.
Impact location variables were computed as azimuth and elevation angles relative to the center of gravity of the head (Crisco et al., 2004) and then categorized as front, side (left and right), back, and top. Four equally spaced regions centered on the mid-sagittal plane make up the front, left, right and back locations. Impacts to the top of the head were defined as all impacts above an elevation angle of 65° from a horizontal plane through the CG of the head (Greenwald et al., 2008).
Statistical Analysis
Results were expressed as median values and [25–75% interquartile range] because study variables were not normally distributed (Shapiro-Wilk test; P < 0.05). Differences in impacts per season among team and sex were examined separately using a Kruskal-Wallis one-way ANOVA on ranks with a Dunn’s post-hoc test for all pairwise comparisons. The significance of the differences in sex and player positions in impact frequency (impacts per practice, impacts per game, and impacts per season) and in severity measures (50th and 95th percentile peak linear and rotational acceleration, and HITsp) were examined using a two-way ANOVA with a Holm-Sidak post-hoc test for all pairwise comparisons. Statistical significance was set at α = 0.05 and the reported p-values are those for the post hoc test. An identical approach was used to examine the significance of the differences among sex and player positions in frequency and severity measures at each location. Statistical comparison among impact location were performed with a Friedman repeated measures ANOVA on ranks. All statistical analyses were performed using SigmaPlot 12.0 (Systat Software, Chicago, IL).
Results
Overall Impact Distributions
A total of 37,411 head impacts were analyzed in this study with 19,880 impacts sustained by males and 17,531 by females. These data were collected during a player median of 109 [96–113] practices and 36 [27–43] games for males and a player median of 142.5 [77.5–174] practices and 53.5 [32–68] games for females. Distributions of the magnitudes of all impacts by peak linear acceleration, rotational acceleration, and HITsp were skewed towards lower values (Figure 1). The total number of impacts received by an individual male player during a single season was a median of 287 [200–446] with a maximum of 785 and females received a median of 170 [116–230] and a maximum of 489. The percentages of players receiving any given number of season impacts are plotted by sex and by team using cumulative histograms (Figure 2). The number of season impacts for male players was significantly higher than for female players (p<0.001) (Figure 2A). The number of season impacts for players on Team M2 was higher than the number of season impacts for players on team M1, F1, and F2 (p<0.001)(Figure 2B). After normalizing for differences in the number of sessions, there was no difference in the number of impacts per game or impacts per practice between M1 and M2 (p>0.05) or F1 and F2 (p>0.05).
Figure 1.
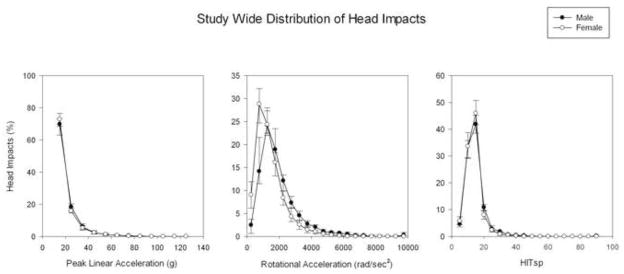
Study wide peak linear acceleration (g), peak rotational acceleration (rad/s2) and HITsp distributions of head impacts. Data are a percentage of all impacts for individual players with median [25–75%] values plotted at each bin in the distribution.
Figure 2.

The cumulative distribution of the percentage of players for the number of impacts per season by sex (A) and team (B).
Impact Frequency
Males experienced a significantly higher number of impacts per game 6.3 [3.5–9.0] than impacts per practice 1.3 [1.0–1.7] (p<0.001). Similarly, females had a significantly higher number of impacts per game 3.7 [2.5–4.9] than impacts per practice 0.9 [0.6–1.0] (p<0.001). Males experienced a significantly higher number of impacts per season, impacts per practice, and impacts per game than females (Table 1). Across all players and within sex, there were no statistically significant differences in the frequency of impacts per game or per practice between forwards and defenders (Figure 3)
Table 1.
Median [25–75th percentile] impacts per season, per practice, per game for male and female players.
| Impacts Per Season | Impacts Per Practice | Impacts Per Game | |
|---|---|---|---|
| Male | 287.0 [201.5–444.6] | 1.3 [1.0–1.7] | 6.3 [3.5–9.0] |
| Female | 169.8 [119.0–230.0] | 0.9 [0.6–1.0] | 3.7 [ 2.5–4.9] |
| p-value | <0.001 | <0.001 | <0.001 |
Figure 3.

After categorizing by sex and player position, the median [25%–75%] 95th percentile peak linear acceleration as a function of the frequency of the median head impacts per session [25%–75%]. Filled markers represent men; unfilled markers represent women.
Impact Magnitude
When compared to females, males were found to sustain impacts with greater 50th percentile peak linear and peak rotational acceleration, as well as HITsp (Table 2). Males also sustained impacts with greater peak 95th rotational acceleration and HITsp, but the trend in differences in peak linear acceleration did not reach significance. Position was not a factor in magnitude of head impacts for males or females (Table 3). There were no increases from practices to games in head impact magnitude regardless of sex or position (Figure 3).
Table 2.
Median [25–75th percentile] impacts per season, 50th and 95th percentile peak linear acceleration, peak rotational acceleration and HITsp for male and female players.
| Peak Linear Acceleration (g) | 50th Percentile Peak Rotational Acceleration (rad/sec2) | HITsp | Peak Linear Acceleration (g) | 95th Percentile Peak Rotational Acceleration (rad/sec2) | HITsp | |
|---|---|---|---|---|---|---|
| Male | 15.7 [14.8–17.1] | 1630 [1454–1733] | 13.6 [13.4–14.1] | 41.6 [36.6–49.5] | 4424 [4076–5182] | 25.6 [22.7–29.5] |
| Female | 15.0 [14.5–15.5] | 1211 [1091–1353] | 13.1 [12.9–13.6] | 40.8 [36.5–49.9] | 3409 [3152–3839] | 22.3 [21.0–25.2] |
| p-value | 0.007 | <0.001 | <0.001 | 0.366 | <0.001 | 0.002 |
Table 3.
Median [25–75th percentile] 95th percentile peak linear acceleration, peak rotational acceleration and HITsp for male and female players by position.
| Position | n | Peak Linear Acceleration (g) | Peak Rotational Acceleration (rad/sec2) | HITsp | |
|---|---|---|---|---|---|
| Male | Defense | 16 | 38.5 [33.1–48.4] | 4420 [3955–5115] | 23.6 [22.0–29.0] |
| Forward | 25 | 43.4 [38.5–49.8] | 4499 [4076–5221] | 26.4 [24.0–29.6] | |
| Female | Defense | 21 | 40.6 [34.3–50.0] | 3431 [3108–3786] | 21.5 [20.9–22.7] |
| Forward | 37 | 40.9 [36.8–49.2] | 3371 [3170–3883] | 23.0 [21.3–25.5] |
Impact Location
For both male and female players, frequency and magnitude of head impacts varied by impact location on the helmet. The lowest percent of impacts occurred to the top of the helmet (p<0.001)(Table 4). There were no statistically significant differences between males and females in the frequency of impacts to different locations on the helmet (p-values ranging from 0.31–0.87).
Table 4.
Impact location distribution, median [25–75th percentile] percentages of all head impacts to the front, side, top, and back of the helmet.
| Front (%) | Side (%) | Top (%) | Back (%) | |
|---|---|---|---|---|
| Male | 28.0 [21.2–33.5] | 30.1 [26.5–36.4] | 7.5 [5.3–10.4] | 28.4 [23.2–37.1] |
| Female | 29.3 [24.8–32.1] | 27.9 [21.5–33.4] | 9.1 [5.2–12.1] | 31.3 [28.2–37.9] |
Location was found to be a factor in impact magnitude for both male and female players. Males experienced greater 95th percentile peak linear acceleration from impacts to the back of the helmet than impacts to the front or side (p=0.002) (Figure 4A). Males also experienced impacts to the side of the helmet that were greater in 95th percentile peak rotational acceleration when compared to impacts to the front (p=0.002). For females, impacts to the back and top of the helmet were greater in 95th peak linear acceleration than impacts to the front and side (p<0.001) (Figure 4B). Females also experienced greater 95th percentile peak rotational acceleration from impacts to the side and back of the helmet than impacts to the top or front (p<0.001). Impacts to the front of the head and side of the head were significantly greater in 95th percentile peak linear acceleration for males than females (p=0.028, p<0.001 respectively) (Figure 4A). Impacts to all four locations (front, side, top, back) were significantly greater in peak rotational acceleration for males compared to females (p=<0.001, p<0.001, p=0.028, p=0.024 respectively) (Figure 4B). Position did not play a factor in frequency or magnitude of impact location for males or females.
Figure 4.
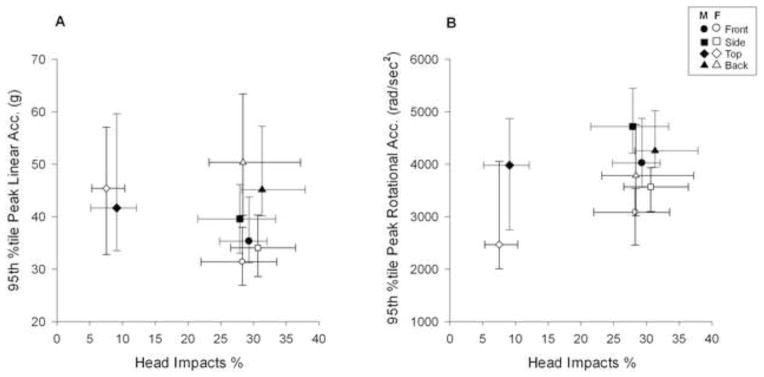
Median [25%–75%] of the 95th percentile peak linear (g) (A) and peak rotational (rad/sec2) acceleration (B) as a function of the median [25%–75%] frequency of impacts at each helmet location and categorized by sex. Filled markers represent men; unfilled markers represent women.
Discussion
The purpose of this study was to quantify head impact exposure in individual male and female collegiate ice hockey players and then examine the relationships between head impact frequency, location, and magnitude as a function of sex, player position, session type, and team.
Male players were found to have a higher frequency of head impacts per practice, per game and per season than female players. The difference in impact frequency between sexes can most likely be attributed to gender-specific rules in ice hockey. Checking, or purposeful body contact of an opposing player, is allowed in men’s hockey whereas it is illegal in women’s. In a previous study in the same subject population, we found that while head impacts that resulted from contact with another player occurred at a higher rate per game for males compared to females, contact with another player was the most frequent head impact mechanism for both sexes (Wilcox et al., 2013). Similar to previous studies in collegiate football and youth hockey, both male and female players were found to have higher impacts per games than impacts per practice (Crisco et al., 2011, 2010; Mihalik et al., 2008). Accordingly, overall injury rates in collegiate ice hockey have been reported to be eight times higher in games than in practices for males and five times higher for females (Agel et al., 2007a, 2007b). The number of impacts per practice, per game, and per season for male and female hockey players were considerably lower than those previously reported in collegiate football (Crisco et al., 2011, 2010). When considering the difference in head impact frequency between the two sports, it should be noted that, in this study, the number of head impacts were normalized by the number of sessions individual players participated in, regardless of whether they received a head impact or not. Crisco et al. normalized the frequency of head impacts by the number of sessions where a player sustained at least one impact (Crisco et al., 2011, 2010). For an individual athlete, the number of AE will be higher than or equal to the number of sessions where a single impact occurs.
Male hockey players were found to sustain head impacts that resulted in greater acceleration magnitudes than females. When one considers that impacts of greater magnitude have more associated risk for concussion and that females are reported to have a higher incidence of concussion, the data presented here may seem counterintuitive (Beckwith et al., 2013; Dick, 2009). Several additional factors may contribute to the differences in biomechanics of head impacts and concussion incidence between males and female players in collegiate ice hockey, including physiological differences, psychological factors, and rule variations within the sport by gender. Mihalik et al. (Mihalik et al., 2012) reported an average linear acceleration in male youth hockey players of 18.3g for defensemen and 18.4g for forwards which was substantially higher than our median 50th percentile linear acceleration for male and female defensemen and forwards, which ranged from 15.0–15.8g. This discrepancy may be associated with differences in analysis; in that study average values were computed, while in the present study we computed the median value to account for the positively skewed, non-normally distributed data. While the 95th percentile peak rotational acceleration for male hockey players in this study, 4424 rad/sec2, was comparable to the reported value of 4378 rad/sec2 in collegiate football, both of these values are considerably greater than what we found in female hockey players, 3409 rad/sec2. The 95th percentile peak linear acceleration, 62.7g, and HITsp, 32.6, reported in collegiate football are considerably greater than those reported in this study for both male and female hockey players. This suggests that that type of sport is likely a key factor in individual athlete’s head impact exposure.
Impacts to the back of the head resulted in greater 95th percentile peak linear acceleration than impacts to the front, top, and side for both male and female players. This is consistent with previous findings in collegiate ice hockey that reported impacts to the back of the head had the greatest magnitudes (Gwin et al., 2009). Interestingly, epidemiological studies dating back to the 1960’s that were used to develop the first ice helmets standard suggested that increased protection is needed for the back of the head due to the prevalence of falling backward and hitting the ice (Odelgard, 1989). Similarly, in a previous study that synchronized data from the HIT system with game video, we found that head contact with the ice resulted in the greatest magnitudes (Wilcox et al., 2013). While linear acceleration was highest for impacts to the back of the head, impacts to both the back and side of the head resulted in the highest rotational accelerations. This is similar to findings in a group of youth hockey players (Mihalik et al., 2012), and the authors postulated that impacts to the side of the head may elicit rotation of the head about the neck more easily than impacts to other locations. Interestingly, impact location, along with rule variations, may also explain why male hockey players were found to sustain head impacts that resulted in greater rotational, but not linear, acceleration magnitudes than females. It has been reported that males sustain a higher rate of impact with the boards than female athletes and these impacts result in higher rotational, but comparable linear, accelerations than other head impact mechanisms (Wilcox et al., 2013). While linear and rotational acceleration have shown to be correlated; the data presented in this study along with previously reported collegiate football data, have shown this relationship is dependent upon impact location (Crisco et al., 2012). Anecdotally, for male players, we can speculate that the majority of head impacts that occur with the boards are a result of checking and are to the side of the head, a location associated with high rotational accelerations.
While player position was found to have the most significant effect on head impact exposure in collegiate football (Crisco et al., 2011), we found no differences between player positions in collegiate ice hockey. This disparity may be attributed to the fact that player positions in football tend to be highly specialized with very different objectives. Similar to findings in previous studies in youth hockey (Mihalik et al., 2008), we observed no differences in frequency or magnitude of head impacts between defenders and forwards. There are conflicting data available on player position and injury rates in hockey; some studies have reported that forwards sustain higher overall injury and concussion rates than defenders, while others found no differences (Agel et al., 2007a, 2007b; Flik et al., 2005; Hutchison, 2011; McKnight et al., 1992). A limitation of this study is that we did not analyze the relationship between head impact exposure and the diagnosis of concussion.
This study has several additional limitations. There were a disproportionate number of females to males (58 vs. 41) included in this study, however we captured a relatively large number of head impacts and observed statistically significant differences, so it is unlikely that additional data collection would alter the results. There were also differences in the numbers of seasons in which each team participated. Data collection for team M1 was limited to a single season because the team accepted a new equipment contract after that season, and HIT System technology was not compatible with helmet models specified within the new contract.
In summary, we have shown that head impact exposure for collegiate ice hockey players is dependent upon sex, session type, and team but not on player position. Male players have higher frequencies of head impacts and experience impacts greater in magnitude than females. Head impacts occur at a higher frequency in games than in practices but these impacts are not greater in magnitude. Impacts to the back of the helmet result in the greatest peak linear accelerations, while impacts to the side and back of the helmet are associated with high rotational accelerations. Our findings also suggest, when compared to the literature, that head impact exposure for individual athletes is dependent upon which sport they play. It has been proposed that reducing an individual’s head impact exposure is a practical approach for reducing the risk of brain injuries (Crisco and Greenwald, 2011). Strategies to decrease an individual athlete’s exposure need to be sport and gender specific, with considerations for team and session type.
Acknowledgments
Research reported in this publication was supported by the National Institute of Child Health and Human Development and the National Institute of General Medical Sciences at the National Institute of Health under award numbers R01HD048638, R25GM083270 and R25GM083270-S1 and the National Operating Committee on Standards for Athletic Equipment. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We gratefully acknowledge and thank the engineering team at Simbex for all of their technical support. We would like to thank Lindley Brainard and Wendy Chamberlin at Simbex for their role in data collection and clinical coordination. We would also like to thank Russell Fiore, M.Ed., A.T.C, Emily Burmeister M.S., A.T.C, and Brian Daigneault, MS, A.T.C at Brown University; as well as Jeff Frechette, A.T.C., and Tracey Poro, A.T.C., Dartmouth College Sports Medicine and Mary Hynes, R.N., M.P.H. Dartmouth Medical School for their support on this project.
Footnotes
Conflict of Interest Disclosure
Joseph J. Crisco, Richard M. Greenwald, Jeffrey J. Chu, and Simbex have a financial interest in the instruments (HIT System, Sideline Response System (Riddell, Inc)) that were used to collect the biomechanical data reported in this study.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Agel J, Dick R, Nelson B, Marshall SW, Dompier TP. Descriptive epidemiology of collegiate women’s ice hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 2000–2001 through 2003–2004. J Athl Train. 2007a;42:249–54. [PMC free article] [PubMed] [Google Scholar]
- Agel J, Dompier TP, Dick R, Marshall SW. Descriptive epidemiology of collegiate men’s ice hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007b;42:241–8. [PMC free article] [PubMed] [Google Scholar]
- Beckwith JG, Greenwald RM, Chu JJ, Crisco JJ, Rowson S, Duma SM, Broglio SP, McAllister TW, Guskiewicz KM, Mihalik JP, Anderson S, Schnebel B, Brolinson PG, Collins MW. Head Impact Exposure Sustained by Football Players on Days of Diagnosed Concussion. Med Sci Sports Exerc. 2013;45:737–746. doi: 10.1249/MSS.0b013e3182792ed7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brainard LL, Beckwith JG, Chu JJ, Crisco JJ, McAllister TW, Duhaime AC, Maerlender AC, Greenwald RM. Gender differences in head impacts sustained by collegiate ice hockey players. Med Sci Sports Exerc. 2012;44:297–304. doi: 10.1249/MSS.0b013e31822b0ab4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broglio SP, Sosnoff JJ, Shin S, He X, Alcaraz C, Zimmerman J. Head impacts during high school football: a biomechanical assessment. J Athl Train. 2009;44:342–9. doi: 10.4085/1062-6050-44.4.342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brolinson PG, Manoogian S, McNeely D, Goforth M, Greenwald R, Duma S. Analysis of linear head accelerations from collegiate football impacts. Curr Sports Med Rep. 2006;5:23–28. doi: 10.1097/01.csmr.0000306515.87053.fa. [DOI] [PubMed] [Google Scholar]
- Chamard E, Théoret H, Skopelja EN, Forwell LA, Johnson AM, Echlin PS. A prospective study of physician-observed concussion during a varsity university hockey season: metabolic changes in ice hockey players. Part 4 of 4. Neurosurg Focus. 2012;33:E4. doi: 10.3171/2012.10.FOCUS12305. [DOI] [PubMed] [Google Scholar]
- Crisco JJ, Chu JJ, Greenwald RM. An algorithm for estimating acceleration magnitude and impact location using multiple nonorthogonal single-axis accelerometers. J Biomech Eng. 2004;126:849–54. doi: 10.1115/1.1824135. [DOI] [PubMed] [Google Scholar]
- Crisco JJ, Fiore R, Beckwith JG, Chu JJ, Brolinson PG, Duma S, McAllister TW, Duhaime AC, Greenwald RM. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train. 2010;45:549–59. doi: 10.4085/1062-6050-45.6.549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crisco JJ, Greenwald RM. Let’s get the head further out of the game: a proposal for reducing brain injuries in helmeted contact sports. Curr Sports Med Rep. 2011;10:7–9. doi: 10.1249/JSR.0b013e318205e063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crisco JJ, Wilcox BJ, Beckwith JG, Chu JJ, Duhaime AC, Rowson S, Duma SM, Maerlender AC, McAllister TW, Greenwald RM. Head impact exposure in collegiate football players. J Biomech. 2011;44:2673–2678. doi: 10.1016/j.jbiomech.2011.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crisco JJ, Wilcox BJ, Machan JT, McAllister TW, Duhaime AC, Duma SM, Rowson S, Beckwith JG, Chu JJ, Greenwald RM. Magnitude of head impact exposures in individual collegiate football players. J Appl Biomech. 2012;28:174–183. doi: 10.1123/jab.28.2.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dick RW. Is there a gender difference in concussion incidence and outcomes? Br J Sports Med. 2009;43(Suppl 1):i46–50. doi: 10.1136/bjsm.2009.058172. [DOI] [PubMed] [Google Scholar]
- Duhaime A-C, Beckwith JG, Maerlender AC, McAllister TW, Crisco JJ, Duma SM, Brolinson PG, Rowson S, Flashman LA, Chu JJ, Greenwald RM. Spectrum of acute clinical characteristics of diagnosed concussions in college athletes wearing instrumented helmets: clinical article. J Neurosurg. 2012;117:1092–1099. doi: 10.3171/2012.8.JNS112298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flik K, Lyman S, Marx RG. American collegiate men’s ice hockey: an analysis of injuries. Am J Sports Med. 2005;33:183–187. doi: 10.1177/0363546504267349. [DOI] [PubMed] [Google Scholar]
- Greenwald RM, Gwin JT, Chu JJ, Crisco JJ. Head impact severity measures for evaluating mild traumatic brain injury risk exposure. Neurosurgery. 2008;62:789–98. doi: 10.1227/01.neu.0000318162.67472.ad. discussion 798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gwin JT, Chu JJ, Greenwald RM. Head impact telemetry system™ for measurement of head acceleration in ice hockey. Journal of Biomechanics. 2006;39(Supplement 1):S153. [Google Scholar]
- Gwin JT, Chu JJ, McAllister TW, Greenwald R. In situ Measures of Head Impact Acceleration in NCAA Division I Men’s Ice Hockey: Implications for ASTM F1045 and Other Ice Hockey Helmet Standards. Journal of ASTM INternational. 2009:6. [Google Scholar]
- Hutchison M. PhD Thesis. Vol. 2011. University of Toronto; Toronto, Ontario, Canada: 2011. Concussions in the National Hockey League (NHL): The Video Analysis Project. [Google Scholar]
- Koerte IK, Ertl-Wagner B, Reiser M, Zafonte R, Shenton ME. White matter integrity in the brains of professional soccer players without a symptomatic concussion. JAMA. 2012a;308:1859–1861. doi: 10.1001/jama.2012.13735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koerte IK, Kaufmann D, Hartl E, Bouix S, Pasternak O, Kubicki M, Rauscher A, Li DKB, Dadachanji SB, Taunton JA, Forwell LA, Johnson AM, Echlin PS, Shenton ME. A prospective study of physician-observed concussion during a varsity university hockey season: white matter integrity in ice hockey players. Part 3 of 4. Neurosurg Focus. 2012b;33:E3. doi: 10.3171/2012.10.FOCUS12303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375–8. doi: 10.1097/00001199-200609000-00001. [DOI] [PubMed] [Google Scholar]
- Manoogian S, McNeely D, Duma S, Brolinson G, Greenwald R. Head acceleration is less than 10 percent of helmet acceleration in football impacts. Biomed Sci Instrum. 2006;42:383–8. [PubMed] [Google Scholar]
- McCrory P, Meeuwisse W, Johnston K, Dvorak J, Aubry M, Molloy M, Cantu R. Consensus statement on concussion in sport: the 3rd International Conference on Concussion in Sport held in Zurich, November 2008. J Athl Train. 2009;44:434–48. doi: 10.4085/1062-6050-44.4.434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKnight CM, Ferrara MS, Czerwinska JM. Intercollegiate Ice Hockey Injuries: A Three-Year Analysis. J Athl Train. 1992;27:338–343. [PMC free article] [PubMed] [Google Scholar]
- Mihalik JP, Blackburn JT, Greenwald RM, Cantu RC, Marshall SW, Guskiewicz KM. Collision type and player anticipation affect head impact severity among youth ice hockey players. Pediatrics. 2010a;125:e1394–1401. doi: 10.1542/peds.2009-2849. [DOI] [PubMed] [Google Scholar]
- Mihalik JP, Greenwald RM, Blackburn JT, Cantu RC, Marshall SW, Guskiewicz KM. Effect of infraction type on head impact severity in youth ice hockey. Med Sci Sports Exerc. 2010b;42:1431–1438. doi: 10.1249/MSS.0b013e3181d2521a. [DOI] [PubMed] [Google Scholar]
- Mihalik JP, Guskiewicz KM, Jeffries JA, Greenwald RM, Marshall SW. Characteristics of head impacts sustained by youth ice hockey players. IMechE. 2008;222:45–52. [Google Scholar]
- Mihalik JP, Guskiewicz KM, Marshall SW, Blackburn JT, Cantu RC, Greenwald RM. Head impact biomechanics in youth hockey: comparisons across playing position, event types, and impact locations. Ann Biomed Eng. 2012;40:141–149. doi: 10.1007/s10439-011-0405-3. [DOI] [PubMed] [Google Scholar]
- Odelgard B. The Development of Head, Face, and Neck Protectors for Ice Hockey Players. In: Castaldi C, Hoerner E, editors. Safety in Ice Hockey. ASTM International; 100 Barr Harbor Drive, PO Box C700, West Conshohocken, PA 19428-2959: 1989. pp. 220–220–15. [Google Scholar]
- Thurman DJ, Branche CM, Sniezek JE. The epidemiology of sports related traumatic brain injuries in the United States: recent developments. J Head Trauma Rehabil. 1998;13:1–8. doi: 10.1097/00001199-199804000-00003. [DOI] [PubMed] [Google Scholar]
- Wilcox BJ, Machan JT, Beckwith JG, Greenwald RM, Burmeister E, Crisco JJ. Head impact mechanisms in men’s and women’s collegiate ice hockey. Journal of Athletic Training Accepted for publication. 2013 Mar; doi: 10.4085/1062-6050-49.3.19. 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]