

Tobacco use is recognized by global authoritative bodies, such as the Oxford Health Alliance, as a leading cause of preventable death in the world. Racial/ethnic minority groups (e.g., black and Hispanic people) as well as individuals of lower socioeconomic status (SES) (e.g., low-income individuals) experience disproportionately elevated rates of tobacco-related morbidity and mortality.1 These disparities may be explained in part by differential geographic access to tobacco products.
Existing research has found that neighborhoods with high racial/ethnic minority concentrations and lower SES tend to have a higher density of tobacco retailers.2–12 While informative, most of these studies ignore the spatial techniques that are often necessary when using spatial data, notwithstanding early tobacco retailer demographic disparities research explicitly noting the importance of accounting for spatial autocorrelation in future research.4 Limited research has evaluated demographic disparities in the tobacco retail environment that employed a spatial analytic perspective.2,10,12,13 Findings from some -studies suggest that performing spatial regressions was necessary when analyzing demographic disparities in the tobacco retail environment.2,13 Spatial regressions account for spatial autocorrelation explicitly by paying attention to the location and arrangement of neighborhood units, resulting in correct parameter estimates and p-values.14–20 Additionally, most studies measure population composition as a continuous variable. However, there may be threshold effects, whereby categorizing population composition (e.g., >60% of a certain racial/ethnic minority group) might matter in the spatial distribution of tobacco retailers.
All of the existing research evaluating demographic disparities in the tobacco retail environment of which we are aware used older demographic data (e.g., from the 2000 U.S. Census). Additional studies are needed to monitor current potential demographic disparities in the tobacco retail environment. Indeed, it is important that studies about demographic disparities in the tobacco retailer environment are conducted frequently because the retail landscape may change constantly in certain geographies. In addition, while a study by Laws et al. gathered data on tobacco outlets from three neighborhoods in Boston, Massachusetts, to examine demographic disparities in the tobacco retail environment,3 the results of the study may not be generalizable to other areas.
We evaluated racial/ethnic and socioeconomic disparities in the tobacco retail environment across neighborhoods in Boston, considering threshold effects of neighborhood demographics and employing a spatial analytic perspective with current demographic data.
METHODS
Geographic area
The geographic area of investigation for this study, Boston, is 89.63 square miles, including 48.43 square miles (or 54.03%) of land. Based on calculations using the 2010 U.S. Census, Boston has a population of more than 600,000 people.
Tobacco retailer geographic data
We obtained and geocoded geographic data on tobacco-selling retail outlets from the Cigarette and Tobacco Excise Unit of the Commonwealth of Massachusetts' Department of Revenue. The tobacco retailer data had various information including the business name and address for all tobacco retailers in Massachusetts from October 1, 2010, to September 30, 2012. These data included retailers that had tobacco licenses in Massachusetts during this specified time period and were restricted to the city of Boston for the current study. There were 1,025 licensed tobacco retailers in Boston during the 2010–2012 time period.
Using ArcGIS® version 10.1,18 we calculated tobacco retail density (i.e., tobacco retailers per square kilometer) for census tracts in Boston. Previous research on demographic disparities in the tobacco retail environment used census tracts as the geographic unit of investigation.2,4,5,7–11,13 We used 2010 U.S. Census tract boundaries in this study.
Census tract demographic data
Sociodemographic data at the census tract level for minority neighborhood racial/ethnic composition (i.e., percentage of non-Hispanic black residents and percentage of Hispanic residents) came from the 2010 U.S. Census data. These variables were measured as continuous and categorical variables (census tracts with >60% black [20 of the 167 tracts analyzed in this study] and Hispanic [five of the 167 tracts] populations were considered as predominantly black and Hispanic neighborhoods, respectively).21–23 Census tract data on socioeconomic conditions were not collected in the 2010 U.S. Census; therefore, census tract data on socioeconomic disadvantage (i.e., percentage of families below the federal poverty level) came from the 2006–2010 American Community Survey (ACS). Census tract poverty was operationalized as both a continuous and a categorical variable, where high-poverty neighborhoods were defined as those having at least 20% of families living in poverty (51 of the 167 tracts).24–26 Census tract data on population density (i.e., the total population per square kilometer) also came from the 2010 U.S. Census.
Spatial analysis
This study employed an explicit spatial approach to study demographic disparities in the tobacco retail environment. The initial analytic sample included contiguous 2010 Boston census tracts (n=179). Consistent with previously published neighborhood research in Boston, we excluded the sparsely populated Harbor Islands27–29 and a census tract that includes only the Massachusetts Bay. Also consistent with previous demographic disparities research,29,30 our analysis was restricted to census tracts with >500 people (final n=167), which ensured that census tracts with very small populations would not bias the results and remove missing or withheld ACS data due to small populations. Generally, the ACS does not release data for populations of <500 people at this scale to preserve anonymity.
After examining descriptive statistics for tobacco retail density (e.g., mean and range), we used geovisualization to explore potential spatial patterning. We then evaluated spatial autocorrelation via the Global Moran's I-test statistic.16,17,31 Our previous research with the 167 census tracts found significant spatial autocorrelation in census tract demographics in Boston (e.g., census tract percent black),29,32 so we did not evaluate spatial patterning in these variables in this study. The Moran's calculation for spatial patterning in the tobacco retail density was based on a row-standardized binary first-order Queen's contiguity spatial weights matrix. Moran's I-values fall between –1 (negative spatial autocorrelation) and +1 (positive spatial autocorrelation), with a zero value indicating no spatial autocorrelation. We determined statistical significance of the Global Moran's I-value via a Monte Carlo simulation of 999 random replications.
We computed Spearman's correlations between the demographic characteristics and tobacco retail density. Then, we computed Spearman's correlations accounting for spatial autocorrelation because existing spatial autocorrelation violates the independent observations assumption; thus, it can result in incorrect estimation of significance of effects in the conventional correlation tests of the significance.33–35 The method used to account for spatial autocorrelation in a correlation framework is an effective sample size methodology.33,34 Spatially adjusted significance of correlations also used the row-standardized binary first-order Queen's contiguity spatial weights matrix and six spatial lags. Correlation coefficients (rS-values) and significance values are reported.
After computing a natural logarithm transformation on tobacco retail density, with a transformation offset of 0.001 because tobacco retail density was highly skewed, log-linear bivariate and multivariate regression models were fit predicting tobacco retail density. Multivariate models controlled for all demographics assessed in the study as well as census tract population density. Multivariate analyses including all neighborhood sociodemographic characteristics were also conducted due to potential suppressor and/or interactive effects. Our regression approach began with the conventional ordinary least squares (OLS) regressions, followed by spatial regressions (which control for spatial autocorrelation) if the OLS regression residuals exhibited significant spatial autocorrelation.14–18 If we detected spatial autocorrelation in the OLS regression residuals, we planned to fit the spatial error model and the spatial lag model (as appropriate), in part because previous demographic disparities research has implemented both spatial models.36 The Global Moran's I-test statistic and the Lagrange Multiplier test for both spatial regression modeling approaches were used to evaluate the fitted OLS regression residuals for spatial autocorrelation with the row-standardized first-order Queen's spatial weights matrix.14,18,19,37,38 If the spatial error model or the spatial lag model was appropriate, we compared the OLS and spatial models using the Akaike Information Criterion (AIC).39 A smaller AIC shows a better model goodness of fit. Lastly, if spatial error models were computed, we conducted the spatial Hausman test to compare the magnitude of the OLS and spatial error model parameter estimates based on the null hypothesis of correct specification.14,40
We used the R statistical program version 2.15 with the spdep package for all calculations.41 For all analyses, we evaluated statistical significance at p<0.05.
RESULTS
For the analytic sample of 167 census tracts, the mean number of tobacco retailers was 5.92 (standard deviation [SD] = 5.72; range: 0–48). The mean tobacco retailer density was 14.24 per square kilometer (SD=14.20, range: 0–73.65) for the analytic sample of 167 census tracts. Geovisualization revealed spatial patterns in tobacco retailers across Boston census tracts, and there was significant global spatial autocorrelation in tobacco retailer density (Global Moran's I=0.3139, p=0.001) (Figure).
Figure.
Spatial distribution of tobacco retailers at the census tract level:a Boston, Massachusetts, October 1, 2010–September 30, 2012

aData culled from the Cigarette and Tobacco Excise Unit of the Commonwealth of the Massachusetts Department of Revenue (http://www.mass.gov/dor).
Only one neighborhood demographic characteristic was significantly correlated with tobacco retailer density (Table 1): predominantly Hispanic census tracts (rS=0.2005, p=0.0094).
Table 1.
Spearman's correlation between neighborhood-level demographics and tobacco retailer density in Boston
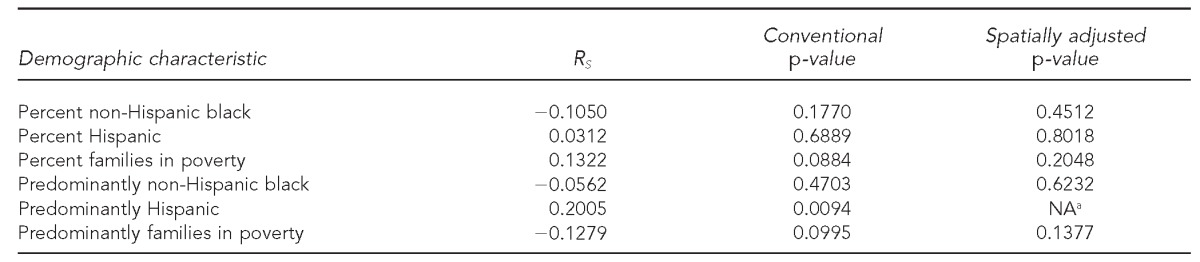
aDue to the small sample size of predominantly Hispanic neighborhoods, the spatially adjusted correlation between neighborhood predominantly Hispanic and tobacco retailer density could not be computed.
NA = not applicable
Results suggested the need for spatial regression modeling approaches when predicting the log of tobacco retailer density. Across all bivariate and multivariate OLS models, the Global Moran's I-values for spatial autocorrelation were statistically significant, as were the Lagrange multiplier terms for spatial models in most models, suggesting the appropriateness of the spatial lag model (p<0.05). The AIC values were lower in the spatial lag models compared with the OLS models. No significant demographic relationships between log of tobacco retailer density were detected in the bivariate spatial lag models (Table 2). Similarly, in multivariate spatial regression analyses, no demographic characteristics were associated with tobacco retailer density.
Table 2.
Association between neighborhood demographics and log of tobacco retailer density in Boston: spatial lag model estimation
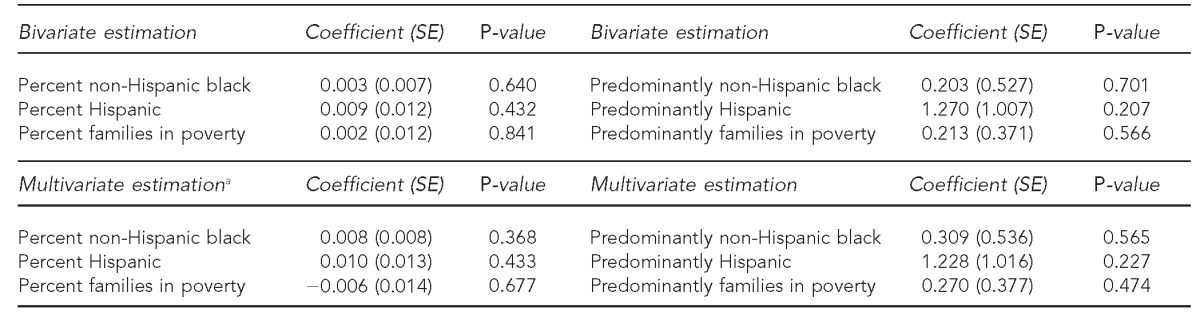
Note: In the spatial lag model, which was estimated via maximum likelihood, there was evidence of remaining spatial autocorrelation and heteroskedasticity in some models. However, findings overall did not change when more advanced spatial models were implemented, including a combination spatial model where spatial effects were accounted for, including a spatial lag of the dependent variable and a spatial lag of the error term (sometimes referred to as spatial autoregressive model with autoregressive disturbances [SARAR]) and a two-stage least-squares model for the spatial lag model with heteroskedasticity and autocorrelation consistent SEs. The spatial lag model estimated via maximum likelihood is presented because it is the most parsimonious, but appropriate, spatial model. For instance, the Akaike Information Criterion value is lower in the maximum likelihood spatial lag model compared with the SARAR model.
aMultivariate models are controlled for population density and other neighborhood sociodemographics.
SE = standard error
DISCUSSION
Previous research has found racial/ethnic minority and socioeconomic disparities in geographic access to tobacco retailers,2–13 including a study that analyzed three selected Boston neighborhoods.3 In contrast with previous studies, we found no demographic disparities in the tobacco retailer environment across Boston neighborhoods. Specifically, although Spearman's correlations found a positive association between predominantly Hispanic census tracts and tobacco retailer density, the multivariate spatial regression analyses showed no associations between demographic characteristics and tobacco retailer density.
With 36 colleges and universities, Boston is an atypical city in that it has a very large student population that is often concentrated in non-racial/ethnic minority and non-poor neighborhoods. This feature might account for the lack of patterning of tobacco retail stores by racial/ethnic and socioeconomic composition of neighborhoods. In addition to tobacco retailers placing themselves in racial/ethnic minority and poor neighborhoods, tobacco retailers may choose to be in places with high concentrations of students (for profit maximization).
Our study extends previous research in several ways. For example, this study employed a spatial perspective and considered threshold effects (both of which few studies have done). Mapping in ArcGIS suggested spatial patterning in tobacco retailers. Visually, there seem to be more tobacco retailers in certain neighborhoods of Boston, including Allston and East Boston. Using quantitative spatial analyses, we found spatial autocorrelation in tobacco retailer density and also found spatial autocorrelation in the OLS regression residuals when predicting the log of tobacco retail density. A previous study found no spatial autocorrelation in tobacco retailers, which likely would indicate no need for spatial regressions.12 However, results from other research, which examined demographic disparities in the tobacco retailer environment, similarly suggest the need for spatial regressions.2,13
Future studies examining demographic disparities in the tobacco retail environment are needed (including in other geographic locations and using various neighborhood definitions). These studies could potentially examine demographic disparities by specific types of tobacco retailers (e.g., convenience stores). Additionally, future studies can use price data from tobacco retailers on tobacco products to further examine demographic disparities in the price as well as type and quantity of tobacco products. In this study, given the structure of the business data, we were unable to account for the type of tobacco products potentially sold, which could influence the findings. It is known that a majority of non-Hispanic black people smoke menthol cigarettes; thus, knowing what tobacco products are sold and where could be useful in future investigations. Furthermore, future research should examine the potential demographic disparities in in-store tobacco advertising across neighborhoods in Boston and other locations. The proposed future research can inform whether and where policies are needed. If demographic disparities are found in tobacco retailers, zoning restrictions might be implemented to remedy any disparities.42,43
Limitations
This study was subject to several limitations. For one, we note that using GIS data to measure store location, including tobacco retailers (e.g., GIS data on tobacco-licensing locations and business code GIS data on potential tobacco retailers), can have some positional errors. However, in this study, we analyzed tobacco-licensing data, which are better than proxy data, on the tobacco retail environment, including using business codes to define the tobacco retail environment, which some studies have done.11,44,45 A validation study using North American Industry Classification System codes for operationalizing the tobacco retailer environment found that commercial datasets may underestimate the number of tobacco outlets, and there is likely some misclassification when using this method (e.g., not all grocery and convenience stores may sell tobacco products, such as cigarettes).11
Some other limitations pertain to the geographic area and unit investigated in this study. Because this study was conducted in one city (i.e., Boston), the results may not be generalizable to other geographies, including those that are non-urban. In this study, the definition of neighborhood selected was the U.S. census tract. We specifically used the census tract in this research because it is a frequently used neighborhood definition, including in previous demographic disparities in tobacco environment research2,4,5,7–11,13 and in Boston-based neighborhood research in general.24,29,46–48 Other neighborhood definitions in Boston exist (including based on the Boston Public Health Commission28 and the Boston Redevelopment Authority).49,50 However, these other neighborhood definitions are much larger than census tracts, so the sample size would be reduced, and using these definitions would increase the likelihood of less variation among the units being measured due to spatial aggregation at coarser scales.51
The modifiable areal unit problem was a concern in this study and all other geographic research.52–54 The fact that residents in census tracts that are adjacent to areas outside of Boston might have easy access to a high tobacco retailer density outside the city was not accounted for in this analysis, highlighting the potential for existing “edge effects” (i.e., ignoring interdependent or close-by geographies outside of the study area), which may influence associations. Additionally, there are different approaches to operationalize predominantly minority racial/ethnic and high-poverty neighborhoods. For example, predominantly minority neighborhoods could be operationalized as 50% and high-poverty neighborhoods could be operationalized as ≥30% of the population living in poverty. While our categorizations were based on previously published research, the categorizations chosen may have influenced our study findings.
CONCLUSION
Contrary to existing research, results from this study suggest that there are no demographic disparities in the tobacco retailer environment in Boston. Replication studies in Boston and other areas using census tracts and other neighborhood definitions should be conducted in addition to examining policies that may promote an equitable distribution of tobacco retailers across neighborhoods in Boston (yet to be examined).
Footnotes
Dustin Duncan was supported by the Alonzo Smythe Yerby Postdoctoral Fellowship at Harvard School of Public Health (HSPH). David Williams was supported in part by a grant from the National Cancer Institute (grant #1P50CA148596) to the Lung Cancer Disparities Center at HSPH. The views and opinions expressed in this article are those of the authors and do not necessarily represent the official views of the National Institutes of Health.
REFERENCES
- 1.Williams DR, Kontos EZ, Viswanath K, Haas JS, Lathan CS, MacConaill LE, et al. Integrating multiple social statuses in health disparities research: the case of lung cancer. Health Serv Res. 2012;47(3 Pt 2):1255–77. doi: 10.1111/j.1475-6773.2012.01404.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yu D, Peterson NA, Sheffer MA, Reid RJ, Schneider JE. Tobacco outlet density and demographics: analysing the relationships with a spatial regression approach. Public Health. 2010;124:412–6. doi: 10.1016/j.puhe.2010.03.024. [DOI] [PubMed] [Google Scholar]
- 3.Laws MB, Whitman J, Bowser DM, Krech L. Tobacco availability and point of sale marketing in demographically contrasting districts of Massachusetts. Tob Control. 2002;11(Suppl 2):ii71–3. doi: 10.1136/tc.11.suppl_2.ii71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hyland A, Travers MJ, Cummings KM, Bauer J, Alford T, Wieczorek WF. Tobacco outlet density and demographics in Erie County, New York. Am J Public Health. 2003;93:1075–6. doi: 10.2105/ajph.93.7.1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schneider JE, Reid RJ, Peterson NA, Lowe JB, Hughey J. Tobacco outlet density and demographics at the tract level of analysis in Iowa: implications for environmentally based prevention initiatives. Prev Sci. 2005;6:319–25. doi: 10.1007/s11121-005-0016-z. [DOI] [PubMed] [Google Scholar]
- 6.Peterson NA, Lowe JB, Reid RJ. Tobacco outlet density, cigarette smoking prevalence, and demographics at the county level of analysis. Subst Use Misuse. 2005;40:1627–35. doi: 10.1080/10826080500222685. [DOI] [PubMed] [Google Scholar]
- 7.Novak SP, Reardon SF, Raudenbush SW, Buka SL. Retail tobacco outlet density and youth cigarette smoking: a propensity-modeling approach. Am J Public Health. 2006;96:670–6. doi: 10.2105/AJPH.2004.061622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fakunle D, Morton CM, Peterson NA. The importance of income in the link between tobacco outlet density and demographics at the tract level of analysis in New Jersey. J Ethn Subst Abuse. 2010;9:249–59. doi: 10.1080/15332640.2010.522890. [DOI] [PubMed] [Google Scholar]
- 9.Siahpush M, Jones PR, Singh GK, Timsina LR, Martin J. Association of availability of tobacco products with socio-economic and racial/ethnic characteristics of neighbourhoods. Public Health. 2010;124:525–9. doi: 10.1016/j.puhe.2010.04.010. [DOI] [PubMed] [Google Scholar]
- 10.Peterson NA, Yu D, Morton CM, Reid RJ, Sheffer MA, Schneider JE. Tobacco outlet density and demographics at the tract level of analysis in New Jersey: a statewide analysis. Drugs Educ Prev Policy. 2011;18:47–52. [Google Scholar]
- 11.Rodriguez D, Carlos HA, Adachi-Mejia AM, Berke EM, Sargent JD. Predictors of tobacco outlet density nationwide: a geographic analysis. Tob Control. 2013;22:349–55. doi: 10.1136/tobaccocontrol-2011-050120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schneider S, Gruber J. Neighbourhood deprivation and outlet density for tobacco, alcohol and fast food: first hints of obesogenic and addictive environments in Germany. Public Health Nutr. 2013;16:1168–77. doi: 10.1017/S1368980012003321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Loomis BR, Kim AE, Goetz JL, Juster HR. Density of tobacco retailers and its association with sociodemographic characteristics of communities across New York. Public Health. 2013;127:333–8. doi: 10.1016/j.puhe.2013.01.013. [DOI] [PubMed] [Google Scholar]
- 14.LeSage J, Pace RK. Introduction to spatial econometrics. Boca Raton (FL): CRC Press; 2009. [Google Scholar]
- 15.Ward MD, Gleditsch KS. Spatial regression models. Thousand Oaks (CA): Sage Publications, Inc.; 2008. [Google Scholar]
- 16.Waller LA, Gotway CA. Applied spatial statistics for public health data. Hoboken (NJ): Wiley-Interscience; 2004. [Google Scholar]
- 17.Bailey TC, Gratrell AC. Interactive spatial data analysis. Harlow Essex (England): Longman Group Limited; 1995. [Google Scholar]
- 18.ESRI. ArcGIS: Release 10. Redlands (CA): ESRI; 2011. [Google Scholar]
- 19.Anselin L, Bera AK. Spatial dependence in linear regression models with an introduction to spatial econometrics. In: Ullah A, Giles DEA, editors. Handbook of applied economic statistics. New York: Marcel Dekker; 1998. pp. 237–89. [Google Scholar]
- 20.Anselin L. Spatial econometrics: methods and models. Dordrecht (Netherlands): Kluwer Academic Publishers; 1988. [Google Scholar]
- 21.Franco M, Diez Roux AV, Glass TA, Caballero B, Brancati FL. Neighborhood characteristics and availability of healthy foods in Baltimore. Am J Prev Med. 2008;35:561–7. doi: 10.1016/j.amepre.2008.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Moore LV, Diez Roux AV, Evenson KR, McGinn AP, Brines SJ. Availability of recreational resources in minority and low socioeconomic status areas. Am J Prev Med. 2008;34:16–22. doi: 10.1016/j.amepre.2007.09.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moore LV, Diez Roux AV. Associations of neighborhood characteristics with the location and type of food stores. Am J Public Health. 2006;96:325–31. doi: 10.2105/AJPH.2004.058040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Subramanian SV, Chen JT, Rehkopf DH, Waterman PD, Krieger N. Racial disparities in context: a multilevel analysis of neighborhood variations in poverty and excess mortality among black populations in Massachusetts. Am J Public Health. 2005;95:260–5. doi: 10.2105/AJPH.2003.034132. published erratum appears in Am J Public Health 2005;95:375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kelly CM, Schootman M, Baker EA, Barnidge EK, Lemes A. The association of sidewalk walkability and physical disorder with area-level race and poverty. J Epidemiol Community Health. 2007;61:978–83. doi: 10.1136/jech.2006.054775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Franzini L, Taylor W, Elliott MN, Cuccaro P, Tortolero SR, Janice Gilliland M, et al. Neighborhood characteristics favorable to outdoor physical activity: disparities by socioeconomic and racial/ethnic composition. Health Place. 2010;16:267–74. doi: 10.1016/j.healthplace.2009.10.009. [DOI] [PubMed] [Google Scholar]
- 27.Cradock AL, Kawachi I, Colditz GA, Hannon C, Melly SJ, Wiecha JL, et al. Playground safety and access in Boston neighborhoods. Am J Prev Med. 2005;28:357–63. doi: 10.1016/j.amepre.2005.01.012. [DOI] [PubMed] [Google Scholar]
- 28.Chen JT, Rehkopf DH, Waterman PD, Subramanian SV, Coull BA, Cohen B, et al. Mapping and measuring social disparities in premature mortality: the impact of census tract poverty within and across Boston neighborhoods, 1999–2001. J Urban Health. 2006;83:1063–84. doi: 10.1007/s11524-006-9089-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Duncan DT, Aldstadt J, Whalen J, White K, Castro MC, Williams DR. Space, race, and poverty: spatial inequalities in walkable neighborhood amenities? Demographic Res. 2012;26:409–48. doi: 10.4054/DemRes.2012.26.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Block JP, Scribner RA, DeSalvo KB. Fast food, race/ethnicity, and income: a geographic analysis. Am J Prev Med. 2004;27:211–7. doi: 10.1016/j.amepre.2004.06.007. [DOI] [PubMed] [Google Scholar]
- 31.Cliff AD, Ord JK. Spatial processes: models and applications. London: Pion Limited; 1981. [Google Scholar]
- 32.Duncan DT, Kawachi I, White K, Williams DR. The geography of recreational open space: influence of neighborhood racial composition and neighborhood poverty. J Urban Health. 2013;90:618–31. doi: 10.1007/s11524-012-9770-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Clifford P, Richardson S. Testing association between two spatial processes. Spacial statistics and imaging: papers from the research conference on image analysis and spatial statistics held at Bowdoin College, Brunswick, Maine, summer 1988. In: Possolo A, editor. Hayward (CA): Institute of Mathematical Statistics; 1991. pp. 295–308. [Google Scholar]
- 34.Haining R. Bivariate correlation with spatial data. Geogr Anal. 1991;23:210–27. [Google Scholar]
- 35.The elimination of spurious correlation due to position in time or space. Biometrika. 1914;10:179–80. [Google Scholar]
- 36.Smiley MJ, Diez Roux AV, Brines SJ, Brown DG, Evenson KR, Rodriguez DA. A spatial analysis of health-related resources in three diverse metropolitan areas. Health Place. 2010;16:885–92. doi: 10.1016/j.healthplace.2010.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Anselin L, Bera AK, Florax R, Yoon MJ. Simple diagnostic tests for spatial dependence. Reg Sci Urban Econ. 1996;26:77–104. [Google Scholar]
- 38.Anselin L. Lagrange multiplier test diagnostics for spatial dependence and spatial heterogeneity. Geogr Anal. 1988;20:1–17. [Google Scholar]
- 39.Akaike H. A new look at the statistical model identification. IEEE Transactions on Automatic Control. 1974;19:716–23. [Google Scholar]
- 40.Pace RK, LeSage JP. A spatial Hausman test. Econ Letters. 2008;101:282–4. [Google Scholar]
- 41.Bivand RS, Pebesma E, Gómez-Rubio V. Applied spatial data analysis with R. New York: Springer; 2008. [Google Scholar]
- 42.Cohen JE, Anglin L. Outlet density: a new frontier for tobacco control. Addiction. 2009;104:2–3. doi: 10.1111/j.1360-0443.2008.02389.x. [DOI] [PubMed] [Google Scholar]
- 43.Ashe M, Jernigan D, Kline R, Galaz R. Land use planning and the control of alcohol, tobacco, firearms, and fast food restaurants. Am J Public Health. 2003;93:1404–8. doi: 10.2105/ajph.93.9.1404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.D'Angelo H, Fleischhacker S, Rose SW, Ribisl K. Evidence of validity for commercial databases to identify tobacco retailers in a state without tobacco retailer licensing. National Conference on Tobacco or Health; 2012 Aug 15–17; Kansas City, Missouri. [Google Scholar]
- 45.Frick M, Castro MC. Tobacco retail clustering around schools in New York City: examining “place” and “space”. Health Place. 2013;19:15–24. doi: 10.1016/j.healthplace.2012.09.011. [DOI] [PubMed] [Google Scholar]
- 46.Krieger N, Chen JT, Waterman PD, Soobader MJ, Subramanian SV, Carson R. Geocoding and monitoring of US socioeconomic inequalities in mortality and cancer incidence: does the choice of area-based measure and geographic level matter?: the Public Health Disparities Geocoding Project. Am J Epidemiol. 2002;156:471–82. doi: 10.1093/aje/kwf068. [DOI] [PubMed] [Google Scholar]
- 47.Subramanian SV, Chen JT, Rehkopf DH, Waterman PD, Krieger N. Comparing individual- and area-based socioeconomic measures for the surveillance of health disparities: a multilevel analysis of Massachusetts births, 1989–1991. Am J Epidemiol. 2006;164:823–34. doi: 10.1093/aje/kwj313. [DOI] [PubMed] [Google Scholar]
- 48.Krieger N, Chen JT, Waterman PD, Rehkopf DH, Subramanian SV. Race/ethnicity, gender, and monitoring socioeconomic gradients in health: a comparison of area-based socioeconomic measures—the Public Health Disparities Geocoding Project. Am J Public Health. 2003;93:1655–71. doi: 10.2105/ajph.93.10.1655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Li W, Kelsey JL, Zhang Z, Lemon SC, Mezgebu S, Boddie-Willis C, et al. Small-area estimation and prioritizing communities for obesity control in Massachusetts. Am J Public Health. 2009;99:511–9. doi: 10.2105/AJPH.2008.137364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Li W, Land T, Zhang Z, Keithly L, Kelsey JL. Small-area estimation and prioritizing communities for tobacco control efforts in Massachusetts. Am J Public Health. 2009;99:470–9. doi: 10.2105/AJPH.2007.130112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Reynolds H, Amrhein CG. Using a spatial data set generator in an empirical analysis of aggregation effects on univariate statistics. Geogr Environ Modelling. 1997;1:199–220. [Google Scholar]
- 52.Openshaw S, Taylor PJ. A million or so correlation coefficients: three experiments on the modifiable areal unit problem. In: Wrigley N, editor. Statistical applications in spatial sciences. London: Pion Ltd.; 1979. pp. 127–44. [Google Scholar]
- 53.Wong D. The modifiable areal unit problem (MAUP) In: Fotheringham AS, Rogerson PA, editors. The SAGE handbook of spatial analysis. London: SAGE Publications; 2009. pp. 105–24. [Google Scholar]
- 54.Arbia G. Dordrecht (Netherlands): Kluwer Academic Publishers; 1989. Spatial data configuration in statistical analysis of regional economics and related problems. [Google Scholar]