

Abstract
This study examined the effect of proprioceptive neuromuscular facilitation (PNF) coupled with an internal mental imagery technique (PNFI) on both the attainment and retention of increased range-of-movement (ROM) at the hip joint. Twenty-four young adult subjects were randomly allocated to PNF, PNFI, and control treatments administered in fifteen sessions over a three-week period. ROM was assessed prior to training then at the completion of sessions 1 day, 3, 7, and 14 during training, then 28 days after program completion. Analysis-of-Variance with repeated measures showed both significant treatment (p < 0.01) and time effects (p < 0.05). Mean change of ROM values were always larger under the PNFI condition and significantly different (p < 0.05) at day 1 and 3 following training program completion. Thereafter, the diminution of ROM was comparable to the PNF condition. Mean ROM increment relative to baseline was 7.55 and 9.45 degrees for PNF and PNFI respectively receding to 5.86 and 6.5 degrees at twenty-eight days following treatment cessation. Motor imagery coupled with PNF to enhance and retain ROM yields superior results to physical training used alone and can benefit both athletes and those undergoing rehabilitation.
Key Points.
A Proprioceptive Neuromuscular Facilitation (PNF) technique applied to enhance range-of-movement (ROM) at the hip joint was successful.
The effect produced greater gains in participants who received and applied a motor imagery technique to supplement the regular PNF.
Both effects receded by about 50% across a no-practice period of 21 days.
Incorporation of motor imagery with physical therapy deemed worthwile.
Key words: Mental and physical practice, flexibility training
Introduction
An appropriately fluid range-of-motion in the body’s various joint complexes is a desirable attribute for the comfortable completion of daily tasks. In more specific circumstances selected sports demand enhanced levels of flexibility thus it is usual for athletes to devote training time to attaining and maintaining desired levels of suppleness to ensure successful participation. Techniques that promote the most effective acquisition of the attributes in question are sought after and incorporated into the training program. Such a line of thought was the stimulus for the present research when one of the authors was assisting with the flexibility training of a group of women gymnasts. During stretching exercises targeted at improved hip mobility, several athletes commented to the effect that they were unsure as to the potentially achievable range of movement and that the uncertainty presented a barrier to improvement. To minimize ambiguity, a model skeleton was used to convey articular potential at the hip. In subsequent stretching sessions, the athletes were encouraged to visualize the range of motion demonstrated by means of the model skeleton and to attempt to incorporate the image formed into their own repertoire. The athletes reported that they were able to comply and, subjectively, claimed that their flexibility had improved. It was decided to test empirically the apparent enhanced effect of a PNF stretching program augmented with a visual imagery technique.
Various authorities differ in both the methods used to achieve targeted flexibility levels and the effectiveness of certain of those modalities, the technique referred to as proprioceptive neuromuscular facilitation (PNF) which originated in rehabilitation therapy (Voss et al., 1985) is widely practiced in athletic preparation and touted as successful in producing desired range-of-motion effects required in either sports performance or return to healthy status following injury (Alter, 1988, McAtee and Charland, 1999). Although the literature varies somewhat when explaining the exact cause of improved joint laxity, it is generally agreed that enhancement of range-of-movement is brought about through exploitation of a protective mechanism centred on the Golgi tendon organs (proprioceptors) whose function is to monitor tendon load. Stimulation of tendon load through stretch or forceful muscular contraction causes the muscles to relax via neurological inhibition in order to prevent tissue damage (McAtee and Charland, 1999). The resultant effect facilitates increased range-of-motion. Several studies and reviews of research support the view that PNF in its various forms is more successful than other techniques such as ballistic and static stretching for achieving desired range-of-motion (Sady et al., 1982, Shellock and Prentice, 1985, Surburg, 1981).
Less clear is the extent to which a momentarily attained range-of-motion can be retained without persistent training though preservation of a desired level of flexibility would be of interest to performers. In a comprehensive study targeted at retention of flexibility (range-of-motion). Zebas and Rivera (1985) compared the effects of three stretching methods, one of which was modified PNF, undertaken for six weeks on the ankle, neck, shoulder, hip and trunk laxity of coeducational students. Retention was assessed at two and four weeks after cessation of training. Although there were significant initial gains in flexibility, there were also significant losses of flexibility overall. Range-of-movement regression was least in the modified PNF group, and most notably between the end of the program and two weeks post-exercise. Clearly, the application of a training process that augments a selected stretching technique to facilitate both acquisition and, then, retention of a desired level of flexibility would be advantageous.
A plausible supplement to be used to improve both acquisition and retention of range of movement in a joint complex is to combine stretching with some variant of mental practice. The collated findings from a substantial body of research focusing mostly on motor skill acquisition inclines to the conclusion that some combination of physical and mental practice yields superior results to either physical or mental practice applied alone (Feltz and Landers, 1983). Could a similar effect be achieved by using the neuromuscular system to enhance range-of-motion? As indicated earlier, presenting gymnasts with a tangible perceptual frame-of-reference for the realization of potential range-of-motion at the hip using a skeleton model and requesting that they attempt to incorporate this percept into the physical process of PNF training apparently resulted in improvement.
Mental practice comes in a number of guises and its relationship with action is not fully understood. Nonetheless, sufficient support for the value of imagery as a representational process whereby physical tasks and related goals can be cognitively practiced with positive results renders the possibility of incorporating mental practice with PNF worthwhile (Jeannerod, 1994, Jeannerod and Frak, 2001). Mental imagery is defined here after Denis (Denis, 1985) as “a psychological activity which evokes the physical characteristics of an object either permanently or temporarily absent from the perceptual field.” The process can apply to static or dynamic events, past, recent or yet to be accomplished.
Imagery is classified as either “external” which is predominantly visual and characterized as a third-person perspective (seeing oneself performing) or “internal” which is kinesthetic and explained as a first-person perspective (feeling oneself performing) (Epstein, 1980). Research has demonstrated that the two types of imagery were physiologically distinct by observing greater muscle activity during internal imagery (Epstein, 1980, Jacobson, 1932, Shaw, 1940). Furthermore it has been determined that the internal version is more effective when used in connection with motor performance (Weinberg, 1982). Jeanerrod and Frak (2001) found that neuron discharges in the parietal and premotor cortices ‘map’ a pattern of action even when the given action is not being physically performed. Further, they asserted that applied studies should be undertaken to explore the possibility that motor imagery could be a potent tool in improving the function of the motor system. Thus, an internal (motor) imagery technique was applied in this study. The working definition of motor imagery used in this study is akin to that proposed by Jeanerrod (2001) namely, that it is of the ‘internal’ type within which the performer represents the self in action. In this case, the participant imagines the feelings associated with the movement of the limb through a possible range-of-motion. The purpose was to determine whether a proprioceptive neuromuscular facilitation technique coupled with motor imagery, applied to elicit enhanced range-of-motion at the hip joint produced significantly better performance and retention than the proprioceptive neuromuscular facilitation training applied alone.
Methods
Subjects
A mixed gender sample of twenty-four undergraduate students mean age 21.01 (± 2.09) years participated with written informed consent in keeping with the University of Liverpool, UK regulations for research with human subjects. There were twelve men and twelve women who reported sound health and no neuromuscular ailments. Several other volunteer participants were eliminated because they had not fully recovered from recent sports injury.
ROM Measures
Both Range-of-Movement (ROM) and Reported Vividness-of-Imagery (RVI) were measured to control for its potential influence on performance (10) prior to the start of the training program. Both sets of data were used to form balanced treatment groups each comprising eight subjects, namely, Control, Proprioceptive Neuromuscular Facilitation (PNF), and PNF plus Mental Imagery (PNFI). The pre-testing group ROM means were 85.40 (± 13.30), 87.30 (± 13.85), and 86.33 (± 11.45) and not significantly different (p > 0.05). The RVI means were 8.00 (± 1.90), 8.32 (± 2.71), and 8.40 (± 1.62) respectively and not significantly different (p > 0.05).
The ROM measurements were taken from the dominant limb identified as the leg used for kicking. All measures were taken by one of the investigators using a photographic technique in which leg position was captured via a camera positioned at a lateral viewpoint and printed as a single frame, video-processed hard-copy (Mitsubishi P70B). ROM value was recorded by taking the table edge as the zero line, drawing lines to the joint markers then measuring the angle with a protractor. Each measure was cross-checked immediately with three types of goniometer, specifically, international standard (Bissell, #7512), spirit level (Medical Research Ltd., UK #8401841), and digital (Soar Nagano, DL 1000). For the purpose of reliability estimation, the ROM data were submitted to a one-way Analysis-of-Variance which resulted in F 3, 92 0.05 (p > 0.01) and Kendall Coefficient-of-Concordance of W = 0.97 (p > 0.01). This result was taken to be indicative of both consistency and objectivity in the ROM measurement process. The photographic technique described was used to derive raw data in the experimental portion of the study because this method reduced necessity to maintain the limb at the end position for a lengthy period while the angle was measured.
Reported vividness of imagery was assessed using an “ability to image” rating scale developed specifically for limb positioning during related pilot work.
The protocol was as follows:
A four-minute warm-up of jogging and calisthenics without stretching.
Subject positioned supine on a firm table.
Reference markers placed at hip and lateral condyle of knee.
Subject instructed to keep both legs extended, arms crossed on the chest, and head touching the table throughout.
Hip joint was actively flexed to static limit without swinging or bouncing. Non-dominant limb in contact with the table surface at all times.
Subject permitted one practice leg lift for familiarization purposes.
On the measurement trial, subject raised leg and confirmed when limit was reached.
ROM value was recorded by taking the table edge as the zero line, drawing lines to the joint markers on the photograph, then measuring the angle with a protractor.
For vividness of imagery assessment, participants viewed video clips of leg raising movements and, immediately following observation, were requested to close their eyes and attempt to imagine what they had seen, then rate the “clearness of the image seen in the mind’s eye”. The rating was made by promptly circling a number on a continuum ranging from 0 (no image at all) through 9 (very clear, vivid picture of the leg raising motion). The imagery ability of subjects assessed by this method was relatively high though statistical analysis showed that there were no significant differences between the three groups. The respective means and standard deviations were Control 8.0 (±1.9), PNF 8.3 (± 2.7) and PNFI 8.4 (±1.6).
Motor Imagery Training
First, subjects assigned to the motor imagery treatment viewed a short video presentation showing possible ranges of hip flexion demonstrated with both a skeleton and human model. An audio commentary drew the observer’s attention to the manner in which the head of femur rotates freely within the hip socket to permit full range of movement and how hip flexion is constrained by the hamstring muscles when the knee is extended. Also, the commentary stated and showed that movement range as great as 150 degrees was attainable with appropriate training.
Following the video presentation, subjects were requested to assume a comfortable position, close their eyes, and mentally image, specifically, feel themselves producing the observed range-of-movement. It was confirmed verbally that they were able to engage in the imaging process (motor imagery) as requested. The subjects were instructed (and reminded) to use the practiced motor imagery technique during the upcoming flexibility training to imagine the motion felt as they moved their limb through the range demonstrated in the video. To counteract the possibility that the PNF-only group might also use motor imagery, these subjects were engaged in conversation during training. Such conversation consisted of typical ‘patient-client’ interactions that might occur during a treatment regimen timed so as not to interfere with full compliance in the process.
Flexibility Training
This was preceded with the standardized warm-up referred to above. An agonist-directed PNF technique was selected following consultation with the physical therapist member of the experimental team who trained another member of the team who, in turn, administered the flexibility program that was standardized for each subject and all sessions.
The procedure was as follows:
The subject’s leg was positioned with hip extended, abducted, and internally rotated. The knee was extended and the ankle plantar flexed and everted.
The subject isotonically contracted the agonist through a flexion, adduction, external rotation pattern then returned the leg to its resting position.
The movement pattern was repeated five times. On the final attempt, the leg was kept at its maximum active range then repositioned to its extended, abducted, internally rotated state. Verbal confirmation of maximum range was provided on all trials by all subjects combined with a “certain” statement by the trainer.
The trainer’s hands were readjusted and the subject repeated the same pattern of flexion, adduction and external rotation commencing from the limit of movement range, this time with isometric contraction brought about by the trainer’s resistance to motion of the leg maintained for ten seconds.
The subject was instructed to relax for ten seconds while the trainer applied passive pressure to further stretch the extensor muscles.
The procedure was repeated four times, each time commencing at a new angle.
Post training flexibility measures were administered as described above, on the following day, then 3, 7, fourteen, and twenty-eight days after cessation of the program using the photographic technique described above.
Results
The ROM data in degrees were acquired using the photographic technique explained above. Descriptive statistics for the three groups in each phase of the experiment are provided in Table 1.
Table 1.
Range-of-Motion (ROM) values in degrees for Control, PNF and PNFI groups relative to baseline (in text) following training. Data are means (standard deviations).
| Group | 1 day | 3 days | 7 days | 14 days | 28 days |
|---|---|---|---|---|---|
| Control | 86.1 (13.5) | 86.0 (14.3) | 86.5 (13.8) | 85.0 (11.6) | 85.6 (13.5) |
| PNF | 97.5 (14.5) | 96.5 (13.3) | 96.3 (13.9) | 95.6 (13.9) | 94.4 (14.1) |
| PNFI | 97.4 (11.6) | 99.5 (10.4) | 96.8 (9.7) | 95.5 (10.0) | 94.0 (10.4) |
To examine potential treatment effects, ‘change’ values that represented increment, zero change or decrement were derived from each subject’s pre-test data. Inspection of these data showed relatively normal distribution (slight positive skew) with a reasonable balance of decrement (11 cases), zero change (6 cases) and increment (23 cases) in control subjects. By contrast, there were three decrements and four zero change values in the PNF treatment group and incremental changes only in the PNFI treatment group. The range of change was –6 through 24 degrees. The change values were submitted to analysis-of-variance with repeated measures on the ‘time/ assessment’ factor (Hinkle et al, 1979). The main effect of the training treatment was highly significant; F 2,23 8.78, p < 0.01. The main effect of the time factor (maintenance of ROM) was significant F 4,96 6.27, p < 0.05 with a significant linear trend as can be seen from the decreasing size of the values in Figure 1 and providing a clear picture of the trend (time periods on the x-axis are 1= 1 day, 2= 3days, 3= 7days, 4= 14 days, 5= 28 days post-training).
Figure 1.
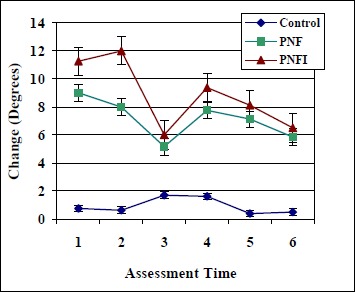
Adaptation and retention of ROM at hip joint: Comparison PNF, PNFI with controls.
For the most part, ROM progressively diminished under both treatment conditions; a regression of some 50 per cent during the 28- day period of no training. Using the Tukey (HSD) procedure, a follow-up analysis was undertaken to examine differences between the mean scores for the two treatment effects (Hinkle et al, 1979). Statistically significant differences (p< 0.05) between the experimental conditions were found at the first and second assessments (1 and 3 days after cessation of training).
Discussion
The purpose of the study was to examine whether proprioceptive neuromuscular facilitation training applied to a hip joint in combination with motor imagery would result in a greater increase in range-of-motion following training. Further, it was expected that superior retention in range-of-motion would prevail when training with motor imagery had ceased compared to training in the PNF without imagery condition. The research project was stimulated by apparent progress witnessed in a practical training context when visualization was suggested coupled with the established finding in the motor learning area that physical and mental practice combined to produce better results than either mode used alone (Feltz and Landers, 1983). Added to the foregoing evidence, recent neuromuscular control studies that have demonstrated substantial physical changes in strength via imagined actions (Yue and Cole, 1992) and the suggestion that motor imagery might act to improve function in the motor system due to the fact that motor pathways are generally activated during motor imagery (Jeannerod and Frak, 2001) raised the possibility that positive findings brought about by such a coupling could be beneficial to both athletes and rehabilitation patients alike.
The results demonstrated that the PNF technique on its own administered five times per week for twenty-one days realized an average increase of some 9 degrees which receded to just less than 6 degrees following a twenty-eight day no-training period. The values of the basic PNF mediated training were highly similar (6 to 10 degrees) to those reported elsewhere (Sady et al, 1982, Wallin et al, 1985, Zebas and Rivera, 1985). The recession effect was more pronounced than that reported elsewhere perhaps because a six-week rather than the three-week training regimen was used in the prior study (Zebas and Rivera, 1985). From a therapeutic standpoint, an improvement of ten degrees is regarded as substantial. In the athletic context, relatively small increments to the dynamic range-of-movement translated into performance such as a gymnast’s split leap or a hurdler’s pick-up of the lead leg can make a significant impact on performance. Likewise, in rehabilitation, even minor improvements are indicative of progress and improved function.
The application of PNF incorporating motor imaging in which the ‘mental’ component was designed to provide a working frame-of-reference for a potentially attainable range-of-motion boosted performance over PNF training used alone. The incremental margin was 2.5 degrees rising to 4 degrees three days following cessation of training. Thereafter, the differential narrowed to become non-significant. Both sets of values showed a highly similar overall trend with the PNFI values always greater than those for the PNF treatment.
A process-related issue begs the question, why might imagery provide a boost? Further, why was the effect in this instance transitory? From a statistical standpoint, it is plausible that the relatively small subject numbers attenuated differences and, as the effect of both treatments receded, the likelihood of statistically significant differences also diminished. A procedural possibility is that the greater amount of time spent with the PNFI group served to reinforce the objective of improving range-of-movement perhaps motivating subjects to perform better. The practical issue is whether the effect of the motor imagery observed in the present study is artifactual. Apparently not, as baseline measures showed that participants in all groups were relatively high imagers. Only one group was trained and instructed to use imagery while undergoing PNF. The no-progress record of the control group testifies to the effects of PNF which was boosted when motor imagery was incorporated.
A perplexing issue arising from these data is that of exactly why the apparent motor imagery effect ‘decays’ and fails to maintain a consistent, relative level of performance that the extra ‘practice’ would suggest. A possible answer could lie in the coupling rather than separation of the ‘perceptuo-motor’ effect. As the term indicates motor- imagery is a coupled process whereby the visual/ imaginal element provides the frame-of-reference for perceiving the possibilities combined with a kinesthetic/ motor element that enables the actual traverse of the limb to the limits of the range. Completion of the task, in the present case, raising the limb through its potential range-of-motion is always achieved by combination of an ‘image-of-the-act’ and ‘production-of-the-act’. The imagery training in the present study may have acted predominantly as an attentional device whose effect was considerable initially but transient with a diminished effect on performance when physical practice had ceased. In future research, the incorporation of an ‘imagery-only’ condition into the experimental design could shed light on this issue.
Conclusions
In keeping with the summary findings of motor skill research, the combination of mental (motor) imagery and physical (PNF) practice applied in this study brought about small but perhaps important increments of improvement in the flexibility of the participants compared with the changes produced by physical practice applied alone. Following appropriate training, the minimal time cost to the individual apparently warrants the incorporation of motor imagery into flexibility training for both athletes and those undergoing physical therapy.
Biographies
John G. WILLIAMS
Employment
Professor in Exercise Science
Degrees
PhD, Chartered Psychologist
Research interests
Motor Control / Learning, Sport & Exercise Psychology
E-mail: jwilliams@wcupa.edu
Jenna L. ODLEY
Employment
Cardiac Rehabilitation
Degrees
MS
Research interests
Rehabiltation therapy
Michael CALLAGHAN
Employment
Physical Therapist
Degrees
Chartered Physiotherapist, MSc
Research interests
Therapeutic methods.
References
- Alter M.J. (1988) Science of Stretching. Champaign, IL: Human Kinetics; 85-95 [Google Scholar]
- Denis M.V. (1985) Visual imagery and the use of mental practice in the development of motor skills. Canadian Journal of Applied Sport Science 10, 45-165 [PubMed] [Google Scholar]
- Epstein M.L. (1980) The relationship of mental imagery and mental rehearsal to performance of a motor task. Journal of Sport Psychology 2, 211-220 [Google Scholar]
- Feltz D. L., Landers D. M. (1983) The effects of mental practice on motor skill learning and performance: A meta-analysis. Journal of Sport Psychology 5, 25-57 [Google Scholar]
- Hinkle D.E., Wierzma W., Jurs S. (1979) Applied Statistics for the Behavioral Sciences, Boston: Houghton-Mifflin; 320-322 [Google Scholar]
- Jacobson E. (1932) Electromyography of mental activities. American Journal of Psychology 44, 677-694 [Google Scholar]
- Jeannerod M. (1994) The representing brain: neural correlates of motor intention and imagery. Behavior and Brain Sciences 17, 187-245 [Google Scholar]
- Jeannerod M. (2001) Consciousness of action and self-consciousness. A cognitive neuroscience approach. Institute of Cognitive Sciences Working Paper 2000-1, 5-6 [Google Scholar]
- Jeannerod M., Frak V. (2001) Mental imaging of motor activity in humans. Institute of Cognitive Sciences, Working Paper 99-8, 5-7 [Google Scholar]
- Katz A.N. (1983) What does it mean to be a high imager? Imagery, Memory, and Cognition. Yuile J. C.Hillsdale, NJ: Lawrence Erlbaum [Google Scholar]
- McAtee R. E., Charland J. (1999) Facilitated Stretching. Champaign, IL: Human Kinetics; 13-16 [Google Scholar]
- Sady S.P., Wortman M., Blanke D. (1982) Flexibility training: ballistic, static or proprioceptive neuromuscular facilitation? Archives of Physical Medicine and Rehabilitation 63, 261-263 [PubMed] [Google Scholar]
- Shaw W. A. (1940) The distribution of muscular action potentials to imagined weight lifting. Archives of Psychology, 247, 1-50 [Google Scholar]
- Shellock F. G., Prentice W.E. (1985) Warming-up and stretching for improved physical performance and prevention of sports-related injuries. Sports Medicine, 2, 267-278 [DOI] [PubMed] [Google Scholar]
- Surburg P. R. (1981) Neuromuscular facilitation techniques in sports medicine. Physician and Sports Medicine, 9, 115-127 [DOI] [PubMed] [Google Scholar]
- Voss D. E., Ionta M. K., Meyers B. J. (1985) Proprioceptive Neuromuscular Facilitation. Philadelphia, PA: Harper and Row; vi-vii, 291-311 [Google Scholar]
- Weinberg R. S. (1982) The relationship between mental preparation strategies and motor performance: a review and critique. Quest 33, 195-213 [Google Scholar]
- Wallin D., Ekblom B., Grahn R., Nordenborg T. (1985) Improvement of muscle flexibility: A comparison between two techniques. American Journal of Sports Medicine 13, 263-268 [DOI] [PubMed] [Google Scholar]
- Yue G., Cole K. J. (1992) Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. Journal of Neurophysiology 67, 1114-1123 [DOI] [PubMed] [Google Scholar]
- Zebas C. J., Rivera M. L. (1985) Retention of flexibility in selected joints after cessation of a stretching exercise program. In: Exercise Physiology. Dotson C. O., Humphrey J. H..New York: AMS Press, 181-191 [Google Scholar]