

Abstract
Objective
To construct and validate a prediction model for estimating the risk of de novo stress urinary incontinence (SUI) after vaginal pelvic organ prolapse (POP) surgery and compare it to predictions using preoperative urinary stress testing and expert surgeons’ predictions.
Materials and Methods
Using the dataset (n = 457) from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial, a model using 12 clinical preoperative predictors of de novo SUI was constructed. De novo SUI was determined by Pelvic Floor Distress Inventory responses through 12 months postoperatively. After fitting the multivariable logistic regression model using the best predictors, the model was internally validated with 1,000 bootstrap samples to obtain bias-corrected accuracy using a concordance index. The model's predictions were also externally validated by comparing findings against actual outcomes using Colpopexy and Urinary Reduction Efforts trial patients (N = 316). The final model's performance was compared to experts using a test data set of 32 randomly chosen Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial patients via comparison of the model's area under the curve (AUC) against: 1) 22 experts’ predictions and 2) preoperative prolapse reduction stress testing.
Results
A model containing seven predictors discriminated between de novo SUI status (concordance index = 0.73, 95% CI 0.65, 0.80) in Outcomes Following Vaginal Prolapse Repair and Midurethral Sling participants and out-performed expert clinicians (AUC = 0.72 vs. 0.62, P<0.001) and preoperative urinary stress testing (AUC = 0.72 vs. 0.54, P <0.001). The concordance index for Colpopexy and Urinary Reduction Efforts trial participants was 0.62, 95% CI 0.56, 0.69.
Conclusion
This individualized prediction model for de novo SUI after vaginal pelvic organ prolapse surgery is valid and outperforms preoperative stress test, prediction by experts and preoperative reduction cough stress test. An online calculator is provided for clinical use.
Introduction
Pelvic surgeons regularly counsel patients regarding the risks, benefits and alternatives of reconstructive pelvic surgery for pelvic organ prolapse (POP) and stress urinary incontinence (SUI). In women without SUI symptoms, POP surgery may cause post-operative de novo SUI in 16-51%.(1,2,3,4,5,6) Recent studies have demonstrated effective prevention strategies including prophylactic incontinence surgery and provided refined estimates to better inform surgical counseling.(1,2,7,8) While these studies have advanced understanding of overall prevalence of de novo SUI, the risk prediction for a specific patient in clinical practice varies based on individual characteristics including age, weight, medical comorbidities and specific tests including prolapse reduction urinary stress tests. Given the growing awareness of the importance of patient preference in treatment selection, especially in quality of life conditions, a prediction model that more accurately predicts an individual's risk may further inform patient preference for a concomitant continence operation after weighing individual risks and benefits.
In this study, we used data from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial (2) to test the hypotheses that baseline characteristics can predict an individual's risk of de novo SUI risk within 12 months of POP surgery. In addition, we hypothesize this prediction model would be more accurate at predicting de novo SUI than preoperative stress testing and expert prediction. We constructed and validated a model for predicting the probability of developing de novo SUI 12 months after vaginal surgery for POP and compared the prediction model to expert estimates and preoperative stress test results.
Materials and Methods
Data from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial were used for the development and internal validation of a de novo SUI prediction model. External validation utilized data from the Colpopexy and Urinary Reduction Efforts trial.(2,7) The Colpopexy and Urinary Reduction Efforts and Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trials were conducted by the Pelvic Floor Disorders Network (PFDN), including seven clinical sites sponsored by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the NIH Office of Research on Women's Health. Both studies received institutional review board approval at all sites and all participants signed informed consent.
The Colpopexy and Urinary Reduction Efforts trial was designed to estimate the rates of de novo SUI for stress continent women undergoing abdominal sacral colpopexy surgery for pelvic organ prolapse and to evaluate the effectiveness of prophylactic continence surgery.(9,10) The Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial compared rates of de novo SUI for women who underwent concomitant vaginal prolapse surgery and a retropubic midurethral sling (TVT) compared with a sham retropubic midurethral sling procedure.(2) Both trials only included participants who did not have preoperative SUI and the original primary outcomes between the two trials differed. The Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial originally used two primary outcomes: 1) urinary incontinence (stress, urgency, or mixed) at 3 months, defined as a positive cough stress test, bothersome incontinence symptoms, or treatment for urinary incontinence; and 2) self-reported urinary incontinence (stress, urgency, or mixed) at 12 months, regardless of whether interim treatment for incontinence had been provided. The primary outcome for the Colpopexy and Urinary Reduction Efforts trial is described below.
A prediction model was developed using data from participants with 1-year outcomes from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling dataset (n = 465). A group of experts identified 12 preoperative patient and test characteristics clinicians commonly use to predict the risk of de novo SUI after surgery. Based on consensus among these PFDN investigators, the following risk factors were selected: increased age at surgery, self-reported white race, higher vaginal parity, higher body mass index (BMI), current smoker, current diagnosis of diabetes, higher pre-operative POPQ stage, higher POPQ point Aa measure, a positive pre-operative prolapse reduction stress test and performance of a concomitant retropubic midurethral sling. We also included the risk factor of presence of strenuous physical activity defined as any positive response to, “During the past month, on average, on how many days in each week did you do strenuous or very hard exercise; that is, exercise that caused you to work up a sweat and made your heart beat fast. For example, aerobics, dancing, jogging, or tennis?” or any positive response of, “During the past month, how often did you perform physical activities that required a major effort such as lifting heavy furniture, shoveling snow, or lifting people or objects weighing more than 25 lbs?” Finally, we included presence of any baseline urgency urinary incontinence symptoms defined using Pelvic Floor Distress Inventory (PFDI) question 19, “usually experiences urine leakage associated with a feeling of urgency, that is, a strong sensation of needing to go to the bathroom.”(11) We hypothesized that all risk factors except performance of a concomitant retropubic midurethral sling would increase the risk of the de novo SUI after surgery for POP.
We defined a clinically important primary outcome for our prediction model in this study as development of de novo SUI as determined by the response of ‘somewhat,’ ‘moderately,’ or ‘quite a bit’ on the PFDI questions 20-22 as these responses are highly relevant outcomes to patients.(11) These questions assess urine leakage up to and including 12 months after surgery as follows - “Do you usually experience urine leakage related to: coughing, sneezing, or laughing; physical exercise such as walking, running, aerobics, or tennis; or lifting or bending over?” The outcome for our current study was cumulative in the sense that if a participant reported symptoms at any postoperative visit through 12 months (i.e. 3, 6 or 12 month visit), then she was considered to have an affirmative value for the outcome variable. This outcome differed slightly from the SUI outcomes published in the existing Outcomes Following Vaginal Prolapse Repair and Midurethral Sling and Colpopexy and Urinary Reduction Efforts trial publications, as those studies looked at symptoms at each specific time point using slightly different definitions in each trial.
A multivariable logistic model was constructed using the above variables from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling dataset. Missing risk factor values were assessed for missing at random, and multiple imputation-chained equations were used to calculate missing values. Though imputed values may have been used within variables in the model, the outcome of SUI was based only on actual and not imputed events. Because we were looking at the presence of SUI symptoms through 12 months (and not just at the 12 month time point as in the original studies), this minimized the risk of obtaining ‘enhanced results’ in an alternative manner. All 12 variables were considered as candidate variables for the final model. The variable selection process was done using a step-down method of backwards elimination starting from the full model using a bootstrap bias-corrected concordance index as the stopping criteria. As a result, variables with individual p-values that were greater than 0.05 were left in the model if they offered information to improve the overall model. The removal of each variable was evaluated by determining which variable had the smallest impact on the adjusted R2 and was stopped when the bootstrap concordance index had a change of 0.001. This procedure was intended to give us the best fit, parsimonious model that was compared to the full model to determine which model was more accurate. The model's predictive ability was measured by the area under the curve (AUC) for the receiver operating characteristic (ROC) curve based on the sensitivity and specificity of the model. An AUC value closer to 1 indicates a better prediction of postoperative SUI and an AUC value of 0.5 indicates that the model predicts no better than chance. The AUC is also a representation of the concordance index and measures the model's ability to generate a higher predicted probability of the outcome occurring to a patient who has a worse outcome. For example, if we have a pair of patients, where one patient has a worse outcome than the other, the concordance index measures the models ability to assign a higher risk to the patient with the worst outcome. All concordance indices and receiver operating characteristic curves were internally validated using 1,000 bootstrap samples to correct for bias within the model and calibration curves where used to measure the relationship between the model's predicted outcome against the cohort's observed outcome, where a perfectly calibrated model follows a 45 degree line. The bootstrapping method of validation has been shown to be superior to other approaches to estimate internal validity such as split-sample methods where 50% or 33.33% of the sample is kept as an independent evaluation part for the model that was estimated on 50% or 66.67% of the sample, respectively.(12)
After the best model was selected and internally validated, it was externally validated using a separate validation dataset other than the one in which it was built. The Colpopexy and Urinary Reduction Efforts randomized trial dataset was chosen as an available dataset for this step. Although the Colpopexy and Urinary Reduction Efforts study design involved a different approach to surgically repairing pelvic organ prolapse, an open abdominal sacral colpopexy, and a different continence procedure, Burch colposuspension, Colpopexy and Urinary Reduction Efforts data were chosen since this study involved a primary research question similar to the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial and purpose of the model. The original primary outcomes for the Colpopexy and Urinary Reduction Efforts trial were SUI and urinary urgency symptoms three months after surgery; however, masking of participants was maintained for two years after surgery. In the original Colpopexy and Urinary Reduction Efforts study, women were characterized as having SUI if any of the following were present: 1) SUI symptoms, defined as an affirmative response to any of three SUI subscale items on the Pelvic Floor Distress Inventory (PFDI) regarding leakage with coughing, sneezing, or laughing; physical exercise; and lifting or bending over; 2) SUI during standardized stress testing in either the supine or standing position with Valsalva's maneuver or cough provocation at maximal bladder capacity or 300 ml, whichever was less; or 3) Any treatment for SUI after the study surgery.(11)
Since patients frequently ask clinicians to estimate their risk of leaking after surgery for pelvic organ prolapse, the model was compared to the best currently available method of estimating risk, a clinician's predictions. The performance of the model was also compared with results from the preoperative prolapse reduction stress test, also commonly used by clinicians to counsel patients on their postoperative risk of de novo SUI. To perform these two comparisons, a subset of 32 women were randomly selected from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling dataset for comparing the probability of developing de novo SUI between the model, the panel of experts, and results from the preoperative stress test. The number of patients was selected based upon estimates provided from investigators of a feasible number of patients that would be reasonably reviewed by a panel of experts. These 32 patients were used to compare predictions of the model to expert's predictions and not as a true independent validation subset. The model was rebuilt using the remaining participants in the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling dataset minus the 32 randomly selected patients.
The preoperative risk factors and stress test results of these 32 participants were given to 22 ‘expert’ surgeons representing each of the PFDN sites for review resulting in 704 predictions. All surgeons were considered to be experienced in treating patients with pelvic organ prolapse and urinary incontinence. Each of the 22 experts was asked to consider all 12 variables from the 32 randomly selected patients and provide their best estimated probability that, “Out of 100 women (with these exact characteristics), estimate the number of women with stress urinary incontinence at or within 12 months after surgery that is somewhat, moderately, or quite a bit bothersome?” The model's predictions were compared to both the experts’ predictions which included all risk factors and results from predictions based only on the preoperative prolapse reduction stress test to determine which was most accurate. This resulted in 22 expert clinician models compared to the statistical prediction model. The clinicians’ predictions were not averaged to yield a single prediction which would reduce statistical power. By incorporating each clinician's predictions, statistical power is substantially increased. The difference in accuracy was determined by using a bootstrap method from their respective receiver operating characteristic (ROC) curve. All analyses were performed using R version 2.15.2; publish data June 22, 2012.
Results
Of the 465 women in the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial, 457 (98%) had SUI data available 12 months after surgery. Table 1 illustrates baseline characteristics and stress test results in participants with and without de novo SUI up to and including 12 months after vaginal surgery for pelvic organ prolapse who underwent retropubic midurethral sling or sham operations. Of the women who underwent a retropubic midurethral sling procedure, 21% had de novo SUI, while of the women who did not undergo a retropubic midurethral sling procedure, 79% reported de novo SUI, (p-value <0.001).
Table 1.
Patient characteristics between women who developed de novo SUI after vaginal surgery for pelvic organ prolapse and women who did not in the Outcomes Following Vaginal Prolapse Repair andMidurethral Slingtria. (2)
| Positive SUI | Negative SUI | |||
|---|---|---|---|---|
| Variable | n* | Mean ± SD or n (%) | n* | Mean ± SD or n (%) |
| Age at Surgery | 115 | 62.26 ± 9.75 | 341 | 63.85 ± 10.25 |
| Race | 115 | 342 | ||
| White | 98(85%) | 300 (88%) | ||
| Black | 8(7%) | 19 (6%) | ||
| Other | 9 (8%) | 23 (6%) | ||
| Parity | 114 | 3.11 ± 1.98 | 336 | 2.93 ± 1.77 |
| Body Mass Index | 115 | 28.51 ± 5.24 | 342 | 27.72 ± 5.18 |
| POP-Q Stage | 115 | 341 | ||
| II | 32 (28%) | 101 (30%) | ||
| III | 73 (63%) | 213 (62%) | ||
| IV | 10 (9%) | 27 (8%) | ||
| POP-Q Point Aa | 115 | 1.4 ± 1.3 | 342 | 1.33 ± 1.44 |
| Preoperative Stress Test | 111 | 327 | ||
| Positive | 44 (40%) | 112 (34%) | ||
| Negative | 67 (60%) | 215 (66%) | ||
| Retropubic midurethral sling | 115 | 342 | ||
| Yes | 24 (21%) | 199 (58%) | ||
| No | 91 (79%) | 143 (42%) | ||
| Strenuous Activity | 110 | 320 | ||
| Yes | 76 (69%) | 226 (71%) | ||
| No | 34 (31%) | 94 (29%) | ||
| Leakage associated with a feeling of urgency | 110 | 322 | ||
| Yes | 46 (42%) | 110 (34%) | ||
| No | 64 (58%) | 212 (66%) | ||
| Current Smoker | 115 | 336 | ||
| Yes | 7 (6%) | 18 (5%) | ||
| No | 108 (94%) | 318 (95%) | ||
| Diabetes | 113 | 334 | ||
| Yes | 20 (18%) | 38 (11%) | ||
| No | 93 (82%) | 296 (89%) | ||
Patients with data available.
SUI , stress urinary incontinence; SD, standard deviation; POP-Q, pelvic organ prolapse quantification.
Two models were generated using multivariable logistic regression that had useful discrimination between women who ultimately did or did not experience de novo SUI after undergoing surgery for pelvic organ prolapse in the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial. These two models were the full model, which used all 12 available independent risk factors, and the parsimonious model, constructed using the step-down procedure which ultimately contained 7 risk factors. The parsimonious (concordance index = 0.73, CI 0.65, 0.80) model had a higher concordance index than the full model (concordance index = 0.71, CI 0.62, 0.77) and was selected as the final model (Figure 1). The parsimonious model also had a good calibration curve with slight tendencies to over-predict when the probability of developing SUI reached 50% or greater (Figure 2). The hypothesized direction of effect of all risk factors was accurate with the exception of age. We predicted that increasing age would increase the risk of developing de novo SUI. Contrary to that assumption, the results demonstrated that as age increased, a participant's risk of experiencing de novo SUI after pelvic organ prolapse surgery decreased (Table 2). An online calculator was created using the using the variables and their estimates from the parsimonious model for making predictions in the clinical setting (http://www.r-calc.com/ExistingFormulas.aspx?filter=CCQHS).
Figure 1.
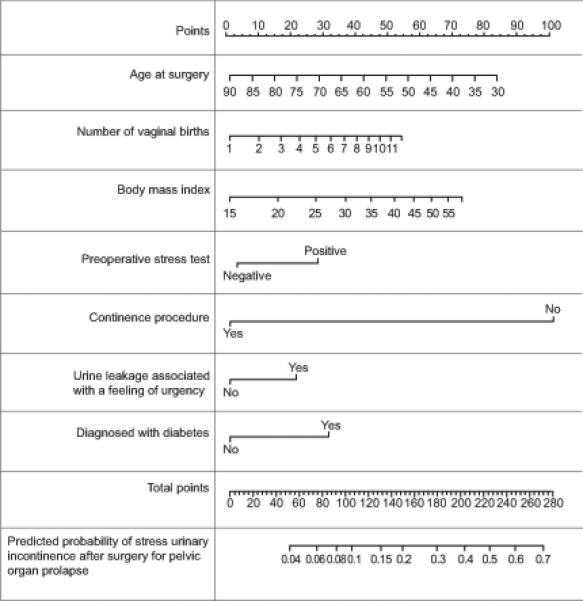
Nomogram for predicting the probability of de novo stress urinary incontinence (SUI) for women who undergo surgery for pelvic organ prolapse. The first row (Points) is the point that is assigned to each variable's measurement from rows 2–8, which are the variables that are included in the predictive model. The assigned points for all 7 variables are then summed up and the total can be located on line 9 (Total Points). Once the Total Points are located draw a vertical line down to the bottom line to obtain the predicted probability of de novo stress urinary incontinence (SUI).
Figure 2.
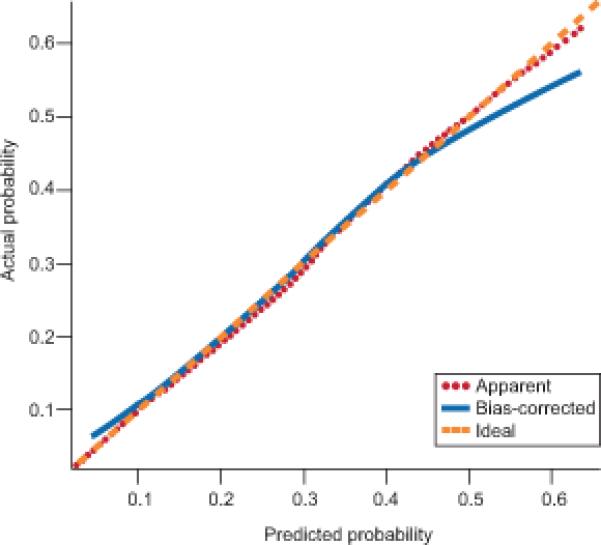
Calibration curve for a model predicting risk of developing De novo stress urinary incontinence (SUI) after surgery for pelvic organ prolapse.
Table 2.
Risk factors and their estimated contribution in the logistical model for predicting de novo Stress Urinary Incontinence after pelvic organ prolapse surgery in the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial (2)
| Variable | Estimate | P |
|---|---|---|
| Intercept | −2.98883 | 0.208 |
| Age at surgery | −0.02527 | 0.037 |
| Parity* | 0.39411 | 0.098 |
| Body mass index† | 0.94942 | 0.158 |
| Preoperative stress test positive | 0.46057 | 0.063 |
| Continence procedure | −1.83254 | <0.001 |
| Leakage associated with a feeling of urgency | 0.37543 | 0.137 |
| Diabetes | 0.56223 | 0.094 |
Square root transformation.
Natural Log transformation.
Logistic regression equation: −2.9888276 - 0.025271306 * AGESURGERY + 0.39411295 * PARITY + 0.94942361 * BMI + 0.4605713 * (LEAK = “Positive”) - 1.8324541 * (Continence procedure performed = “Yes”) + 0.37542553 * (Leaking associated with a feeling of urgency = “Yes”) + 0.56222837 * (DIABETES = “Yes”)
This model was externally validated using the data from 316 Colpopexy and Urinary Reduction Efforts trial participants with one-year data. The performance of the model on the Colpopexy and Urinary Reduction Efforts study population had a concordance index of 0.62 (bootstrap 95% confidence interval 0.56, 0.69) (Figure 3). The accuracy of the model on the entire Colpopexy and Urinary Reduction Efforts dataset, although lower than that for predictions after vaginal prolapse surgery, was significantly better than random chance in predicting whether women undergoing abdominal sacral colpopexy experienced de novo SUI after surgery.
Figure 3.
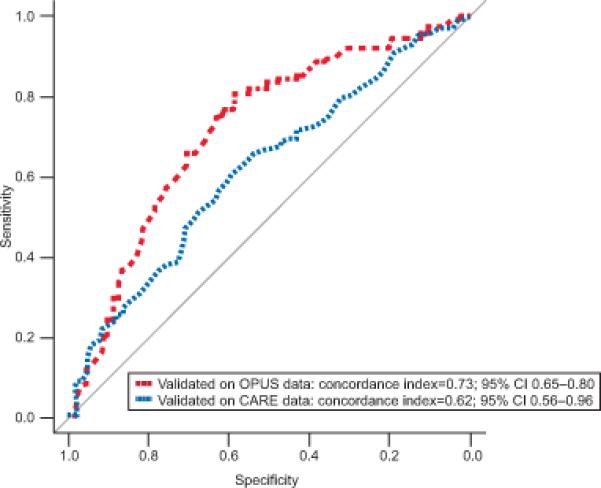
Receiver Operating Characteristic (ROC) curves generated when measuring the accuracy of the logistic models’ predictions using actual outcomes from patients from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling (2) study (internal validation = green) and the Colpopexy and Urinary Reduction Efforts (7) study (external validation = red).
Thirty-two patients were identified at random from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling data subset. Baseline characteristics and the results of the pre-operative stress tests on these 32 patients were presented to the panel of 22 experts. To avoid biasing the new model in favor of the random patients, the original parsimonious model created on the entire Outcomes Following Vaginal Prolapse Repair and Midurethral Sling dataset was rebuilt on the remaining 425 Outcomes Following Vaginal Prolapse Repair and Midurethral Sling patients. Experts’ predictions and the predictions from using the pre-operative stress test results alone were compared to the model's predictions on the removed 32 women (Figure 4). The model was statistically better at predicting the risk of de novo SUI than predictions by experts (concordance index = 0.72 vs. 0.62, p<0.001). The preoperative prolapse reduction stress test alone had a concordance index of 0.54, demonstrating that use of only the stress test result was much less accurate than either the model (concordance index = 0.72, p<0.001) or expert predictions (concordance index = 0.62, p<0.001). Expert predictions were also plotted against the model predictions in order to visualize the discrimination between the two (Figure 5). There was significant variation in the expert's predictions that was more noticeable when model predictions of de novo SUI were greater than 30%. At higher predicted risks, experts’ predictions of the probability of de novo SUI ranged from 0% to 100%.
Figure 4.
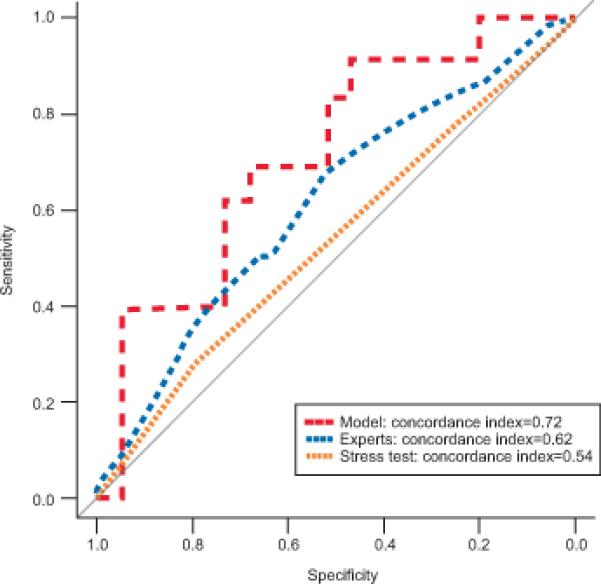
Comparing accuracy of the models’ predictions, experts’ predictions and the preoperative stress test results using Receiver Operating Characteristic (ROC) curves in predicting De novo stress urinary incontinence (SUI)for 32 random patients selected from the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling dataset. The model was significantly more accurate than experts who had knowledge of the same patient characteristics and preoperative prolapse reduction stress test results. The model was also significantly more accurate than the preoperative prolapse reduction stress test alone.
Figure 5.
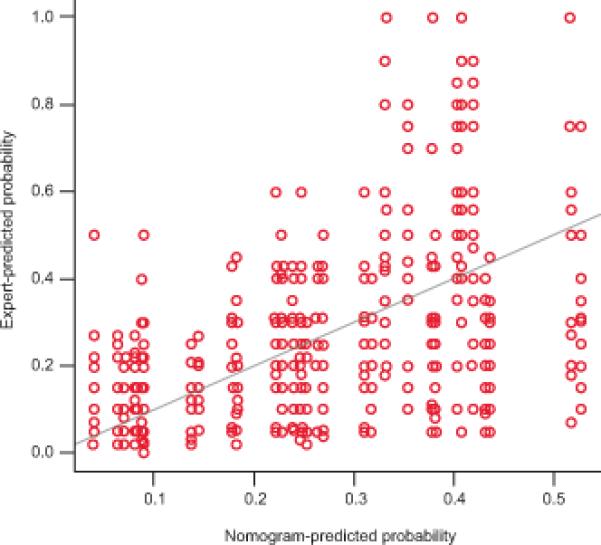
Scatter plot of the models’ predicted probabilities against the experts’ predicted probabilities. The solid diagonal line indicates perfect agreement between predictions. Experts’ predictions demonstrate increased variability as the model's predicted probabilities increase. For example, at predicted probabilities of De novo stress urinary incontinence (SUI)between 30%–50% the range of the experts’ predicted probabilities was highly variable and ranged from 0% to 100%.
Since some providers elect not to perform a pre-operative prolapse reduction stress test in clinical practice, the model's accuracy was assessed with removal of stress test variable. When excluding the pre-operative prolapse reduction stress test, there was no significant drop in accuracy of the model's predictions (concordance index = 0.73 versus 0.72 respectively, p= 0.3122). We recommend keeping the preoperative prolapse reduction stress test variable (effect = 0.46057, p = 0.0633) in the final model as the variable slightly (although with borderline significance) contributes to the most precise overall predicted risk of de novo SUI provided to the patient. However, this finding should reassure users that if the pre-operative stress test result is unknown or not performed, the model maintains accurate predictions.
Discussion
A significant proportion of women without SUI symptoms prior to surgery for POP develop bothersome symptoms of SUI after surgery. The sensitivity of currently available pre-operative prolapse reduction tests for predicting postoperative SUI is only 17 to 39 percent (1). Some surgeons perform a pre-operative reduction stress test to determine if the woman has objective leakage and relate this information to her regarding the potential need for a continence procedure at the time of her reconstructive surgery. Others adopt a staged approach where both the surgeon and patient “wait and see” what happens after surgery. Using information obtained from 2 robust surgical trials, we constructed and tested an individualized prediction model based on patient clinical characteristics to discriminate between women who will or will not develop de novo SUI after pelvic organ prolapse surgery. This model is easy to use and is significantly better at predicting de novo SUI in a clinically useful range of predicted values (<50% probability of leaking) than a pre-operative prolapse reduction stress test alone and subspecialty ‘experts’ who had baseline characteristics including preoperative stress test results available to them. When the model was tested in the Colpopexy and Urinary Reduction Efforts dataset on patients who underwent an abdominal surgery for pelvic organ prolapse, the model was better than random chance in predicting the probability of stress urinary incontinence after surgery; however, the concordance index was lower. This may have been because women in the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling dataset underwent vaginal surgery for prolapse while those in the Colpopexy and Urinary Reduction Efforts dataset underwent abdominal surgery. Although it performed less well in women undergoing abdominal prolapse surgery, a concordance index of 0.62 suggests that the model is a valuable adjunct for shared-decision making between clinician and patients prior to prolapse surgery.
In an era where personalized medicine is being increasingly emphasized, an individual prediction model provides more precise estimates of risk and allows treatment to be tailored to the patient's individual characteristics.(13) Our model demonstrated good predictive accuracy with a bias-corrected concordance index of 0.72. This compares favorably with other predictive models currently used in clinical practice whose concordance index generally range 0.6 to 0.8 (14,15,16,17,18) including widely used models such as the National Cancer Institute Gail model for prediction of Breast Cancer risk (concordance index 0.59) and the Framingham Cardiovascular Risk Model (concordance index 0.72).(19,20) The model is well calibrated; however, there was a tendency for the model to slightly over-predict when a probability of de novo SUI of 50% or greater is reached. For example, when the actual probability is 0.48, the predicted probability of de novo SUI based on the model is 0.5. However, this overestimation is likely of little clinical consequence as most clinicians will likely offer a prophylactic continence procedure with risks of de novo SUI greater than 50%.
Both the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling and Colpopexy and Urinary Reduction Efforts trials demonstrated an increased risk of de novo SUI with a positive prolapse reduction stress test. However, the predictive utility of the test is limited; in Outcomes Following Vaginal Prolapse Repair and Midurethral Sling, the rate of positive pre-operative stress test was similar in women who did or did not develop de novo SUI while this study demonstrated that its use as an isolated predictor also appears to be limited (concordance index 0.54). This is perhaps best is illustrated in Table 1 where it is noted that 40% of those who developed bothersome de novo SUI symptoms by 12 months in Outcomes Following Vaginal Prolapse Repair and Midurethral Sling had a positive pre-operative reduction stress test compared with 34% of those who did not develop de novo SUI over the same time period; a relatively minor 6% difference. Other clinical predictors such as age, BMI and diabetes appear to have a greater impact on an individual's risk of de novo SUI particularly when combined together in a clinical prediction model. Therefore, the prediction model developed in this study can be used to predict the probability of post-operative SUI even when a pre-operative prolapse reduction test is not performed.
Compared to the model, experts’ predictions had increased variability with predicted probabilities ranging from 0 to 100% when the model's predicted probabilities were above 30%. These findings illustrate the wide variation in how clinicians apply information from the published literature into clinical practice. An ideal method to distinguish performance of the model and expert's predictions would have been to sample approximately one third of the dataset for a more independent and robust comparison. However, we chose a feasible number of patients for clinicians to review.
Limitations of our study are that our prediction model is based on a population of women who underwent only vaginal surgery for the treatment of POP, had prolapse of the anterior vaginal wall within 1 cm of the hymenal ring with straining and have not had previous sling placement as described in the Outcomes Following Vaginal Prolapse Repair and Midurethral Sling trial. We do not know if it is accurate in predicting de novo SUI in patients undergoing an isolated rectocele repair. We did not use an objective post-operative measure such as a cough stress test and it is possible that a different set of predictors and/or model would be required if positive stress test were included in the outcome definition. The model does not completely account for spontaneous remission of the outcome during the 12 month post-operative period as a patient may have experienced bothersome de novo SUI leakage 3 or 6 months after surgery that resolved by 12 months. Finally, the prediction model measures its accuracy for predicting the probability of de novo SUI in an individual patient but does not address clinical consequences (e.g. bleeding, pain, etc.) such as the decision of whether the patient should receive an incontinence procedure or not. Strengths of this study include the use of a primary outcome that is relevant to patients and predicts patient-reported bothersome SUI. Furthermore, the availability of an online calculator makes this model convenient and allows real-time use in the office where Internet access is available. This study should also spur continued applications and research of this approach to other patient populations and outcomes both prospectively and retrospectively.
In summary, in women undergoing transvaginal POP surgery, this model provides a valid individualized risk estimate for the development of de novo SUI symptoms that performs better than an estimate from subspecialty experts and a preoperative stress test. The findings and model's ease of use also suggest that the model would be appropriate for physicians to use in clinical settings when discussing possible surgery for POP with their patients.
Acknowledgments
Supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (2U01HD41249, 2U10 HD41250, 2U10 HD41261, 2U10 HD41267, 1U10 HD54136, 1U10 HD54214, 1U10 HD54215, 1U10 HD54241,U10HD069013, U10HD069025, U10HD069010, U10HD069010, and U01HD069031) and the National Institutes of Health Office of Research on Women's Health.
Footnotes
Financial Disclosure
Rebecca G. Rogers has received royalties from UpToDate for writing a pelvic organ prolapse section, and from the American College of Obstetricians and Gynecologists for a DVD video (Repair of a Fourth Degree Obstetrical Laceration (2002)). She has also been the Data Safety Monitoring Chair for the TRANSFORM trial, sponsored by American Medical Systems. Holly E. Richter has received research grants from Astellas, Pelvalon, and the University of California San Francisco/Pfizer. She has served as a consultant for Pelvalon and Astellas.. The other authors did not report any potential conflicts of interest.
References
- 1.Visco AG, Brubaker L, Nygaard I, Richter HE, Cundiff G, Fine P, et al. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: The colpopexy and urinary reduction efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:607–14. doi: 10.1007/s00192-007-0498-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wei JT, Nygaard I, Richter HE, Nager CW, Barber MD, Kenton K, et al. A midurethral sling to reduce incontinence after vaginal prolapse repair. N Engl J Med. 2012;366:2358–67. doi: 10.1056/NEJMoa1111967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.de Tayrac R, Gervaise A, Chauveaud-Lambling A, Fernandez H. Combined genital prolapse repair reinforced with a polypropylene mesh and tension-free vaginal tape in women with genital prolapse and stress urinary incontinence: A retrospective case-control study with short-term follow-up. Acta Obstetricia Et Gynecologica Scandinavica. 2004;83(10):950–4. doi: 10.1111/j.0001-6349.2004.00499.x. [DOI] [PubMed] [Google Scholar]
- 4.Liang CC, Chang YL, Chang SD, Lo TS, Soong YK. Pessary test to predict postoperative urinary incontinence in women undergoing hysterectomy for prolapse. Obstet Gynecol. 2004;104:795–800. doi: 10.1097/01.AOG.0000140689.90131.01. [DOI] [PubMed] [Google Scholar]
- 5.Ennemoser S, Schonfeld M, von Bodungen V, Dian D, Friese K, Jundt K. Clinical relevance of occult stress urinary incontinence (OSUI) following vaginal prolapse surgery: Long-term follow-up. Int Urogynecol J. 2012;23:851–5. doi: 10.1007/s00192-012-1765-4. [DOI] [PubMed] [Google Scholar]
- 6.Groutz A, Levin I, Gold R, Pauzner D, Lessing JB, Gordon D. “Inside-out” transobturator tension-free vaginal tape for management of occult stress urinary incontinence in women undergoing pelvic organ prolapse repair. Urology. 2010;76:1358–61. doi: 10.1016/j.urology.2010.04.070. [DOI] [PubMed] [Google Scholar]
- 7.Brubaker L, Cundiff GW, Fine P, Nygaard I, Richter HE, Visco AG, et al. Abdominal sacrocolpopexy with burch colposuspension to reduce urinary stress incontinence. N Engl J Med. 2006;354:1557–66. doi: 10.1056/NEJMoa054208. [DOI] [PubMed] [Google Scholar]
- 8.Nygaard I, Brubaker L, Zyczynski HM, Cundiff G, Richter H, Gantz M, et al. Long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse. JAMA. 2013;309:2016–24. doi: 10.1001/jama.2013.4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brubaker L, Cundiff G, Fine P, Nygaard I, Richter H, Visco A, et al. A randomized trial of colpopexy and urinary reduction efforts (CARE): Design and methods. Control Clin Trials. 2003;24:629–42. doi: 10.1016/s0197-2456(03)00073-4. [DOI] [PubMed] [Google Scholar]
- 10.Wei J, Nygaard I, Richter H, Brown M, Barber M, Xiao X, et al. Outcomes following vaginal prolapse repair and mid urethral sling (OPUS) trial--design and methods. Clin Trials. 2009;6:162–71. doi: 10.1177/1740774509102605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barber MD, Kuchibhatla MN, Pieper CF, Bump RC. Psychometric evaluation of 2 comprehensive condition-specific quality of life instruments for women with pelvic floor disorders. American Journal of Obstetrics & Gynecology. 2001;185:1388–95. doi: 10.1067/mob.2001.118659. [DOI] [PubMed] [Google Scholar]
- 12.Steyerberg EW, Harrell FE, Jr, Borsboom GJJM, Eijkemans MJC, Vergouwe Y, Habbema JDF. Internal validation of predictive models: Efficiency of some procedures for logistic regression analysis. J Clin Epidemiol. 2001;54:774–81. doi: 10.1016/s0895-4356(01)00341-9. [DOI] [PubMed] [Google Scholar]
- 13.Goldberger JJ, Buxton AE. Personalized medicine vs guideline-based medicine. JAMA. 2013 doi: 10.1001/jama.2013.6629. [DOI] [PubMed] [Google Scholar]
- 14.Brennan MF, Kattan MW, Klimstra D, Conlon K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann Surg. 2004;240:293–8. doi: 10.1097/01.sla.0000133125.85489.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rudloff U, Jacks LM, Goldberg JI, Wynveen CA, Brogi E, Patil S, et al. Nomogram for predicting the risk of local recurrence after breast-conserving surgery for ductal carcinoma in situ. J Clin Oncol. 2010;28:3762–9. doi: 10.1200/JCO.2009.26.8847. [DOI] [PubMed] [Google Scholar]
- 16.Stephenson AJ, Scardino PT, Eastham JA, Bianco FJ, Jr, Dotan ZA, DiBlasio CJ, et al. Postoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Clin Oncol. 2005;23:7005–12. doi: 10.1200/JCO.2005.01.867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Van Zee KJ, Manasseh DM, Bevilacqua JL, Boolbol SK, Fey JV, Tan LK, et al. A nomogram for predicting the likelihood of additional nodal metastases in breast cancer patients with a positive sentinel node biopsy. Ann Surg Oncol. 2003;10:1140–51. doi: 10.1245/aso.2003.03.015. [DOI] [PubMed] [Google Scholar]
- 18.Albert JM, Liu DD, Shen Y, Pan IW, Shih YC, Hoffman KE, et al. Nomogram to predict the benefit of radiation for older patients with breast cancer treated with conservative surgery. J Clin Oncol. 2012;30:2837–43. doi: 10.1200/JCO.2011.41.0076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rockhill B, Spiegelman D, Byrne C, Hunter DJ, Colditz GA. Validation of the Gail et al. model of breast cancer risk prediction and implications for chemoprevention. J Natl Cancer Inst. 2001;93:358–66. doi: 10.1093/jnci/93.5.358. [DOI] [PubMed] [Google Scholar]
- 20.D'Agostino RBS, Grundy S, Sullivan LM, Wilson P, CHD Risk Prediction Group Validation of the framingham coronary heart disease prediction scores: Results of a multiple ethnic groups investigation. JAMA. 2001;286:180–7. doi: 10.1001/jama.286.2.180. [DOI] [PubMed] [Google Scholar]