

Abstract
A dentigerous cyst or follicular cyst is a form of odontogenic cyst. It is believed that it forms during the development of the tooth and is associated with pressure exerted by the crown of an unerupted (or partially erupted) tooth on the fluid within the follicular space. Typically, dentigerous cysts are painless and discovered during routine radiographic examination. However, they may be large and result in a palpable mass. Additionally, as they grow they displace adjacent teeth. They almost exclusively occur in permanent dentition. The cyst is lined by stratified squamous non-keratinizing epithelium. About 70% of dentigerous cysts occur in the mandible and 30% in the maxilla. Dentigerous cysts associated with ectopic teeth within the maxillary sinus are very rare. We report radiologic and pathologic features in a rare case of infected dentigerous cyst of maxillary sinus arising from an ectopic third molar in a 21-year-old female patient.
Keywords: Dentigerous cyst, ectopic third molar, maxillary sinus, maxilla
INTRODUCTION

Dentigerous cyst, a form of odontogenic cyst, develops by the accumulation of fluid within the follicular space of an unerupted tooth after its crown has fully formed.[1]
Dentigerous cyst is the second most common odontogenic cyst, next to radicular cyst. The teeth most involved are in descending order of occurrence, the third molars, the canines, and the second premolars.[1,2] Usually there are no symptoms associated with dentigerous cysts unless there is infection, when it is followed by a painful swelling. A late non-eruption of tooth could indicate the possibility of a cyst. A dentigerous cyst can expand causing facial asymmetry. As with other cysts, dentigerous cyst expands the cortical plates and may involve other teeth causing destruction of the tissues as it expands.[2] Radiographically, the dentigerous cysts typically show a unilocular radiolucent shadow with a well-defined sclerotic border associated with the crown of an unerupted tooth, but an infected cyst will show ill-defined borders.[3] Dentigerous cysts associated with ectopic teeth within the maxillary sinus are very rare.
A 21-year-old female patient was referred to the Department of Oral and Maxillofacial Surgery with a 3-month history of swelling on the right side of the face with discharge of pus from the right nostril [Figure 1]. The lesion had been slowly increasing in size, since it was first noticed. There was no history of trauma, pain, paresis, paresthesia, or lymphadenopathy. There was slight obvious facial asymmetry caused by the swelling over the right maxillary region. The mass was firm and non-tender on palpation and not adherent to the overlying skin. Intra-oral examination showed expansion of the right buccal cortex thus obliterating the buccal vestibule along with absence of the upper right third molar.
Figure 1.

21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Extra-oral photograph shows swelling on right side of the face.
RADIOLOGIC FEATURES
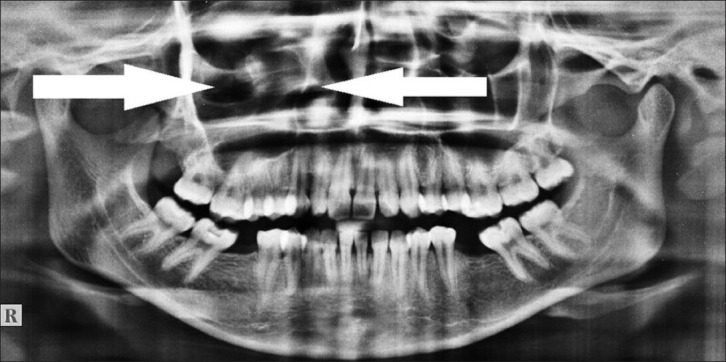
A panoramic radiograph showed a well-defined unilocular radiolucency involving the right maxillary sinus along with the impacted third molar on the floor of the maxillary sinus [Figure 2]. A paranasal sinus (PNS) radiograph showed impacted third molar in the right maxillary sinus with cloudy appearance of right maxillary sinus [Figure 3].
Figure 2.

21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Panoramic radiograph reveals well-defined unilocular radiolucent lesion (arrow) in the right maxillary sinus with impacted third molar.
Figure 3.

21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Paranasal sinus (PNS) radiographic view demonstrates dentigerous cyst (arrow) and impacted third molar in the right maxillary sinus. Also seen is the haziness or cloudy appearance of right maxillary sinus.
Coronal computed tomography (CT) scan showed an impacted tooth along with the radiopaque borders in the right maxillary sinus [Figure 4].
Figure 4.
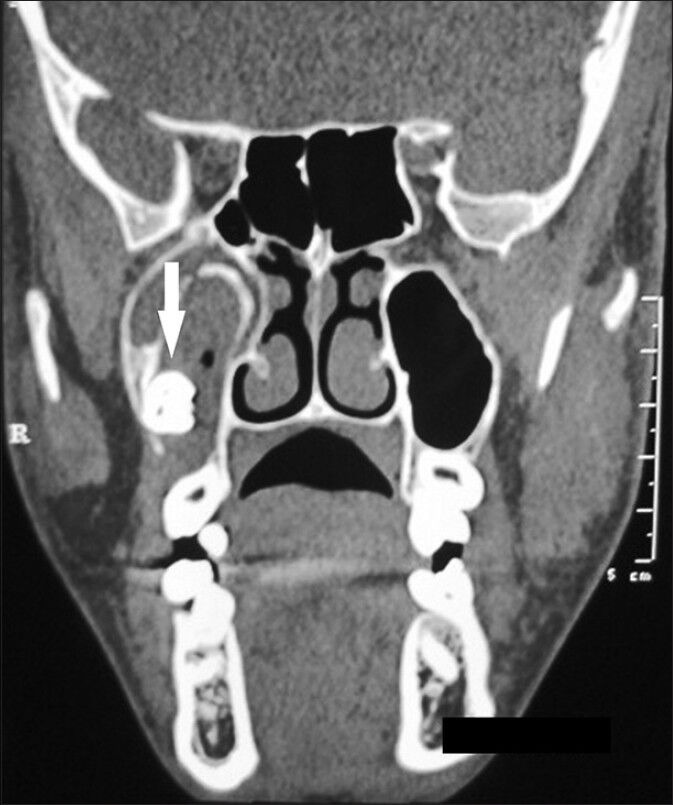
21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Coronal computed tomography (CT) scan shows impacted tooth along with the radiopaque borders (arrow) in the right maxillary sinus.
PATHOLOGIC FEATURES
Aspiration of the lesion yielded frank pus, which was foul-smelling. Based on the clinical and radiological findings, a diagnosis of infected dentigerous cyst of maxillary sinus arising from an ectopic third molar was arrived at. The cystic lesion was enucleated under general anesthesia using the Caldwell-Luc approach [Figures 5–8].
Figure 5.
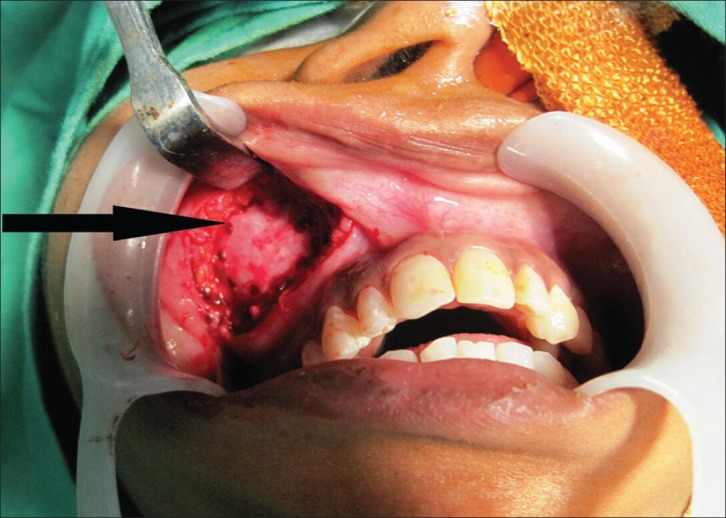
21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Intraoperative photograph shows anterior maxillary sinus wall (arrow) that is exposed using Caldwell-Luc approach.
Figure 8.
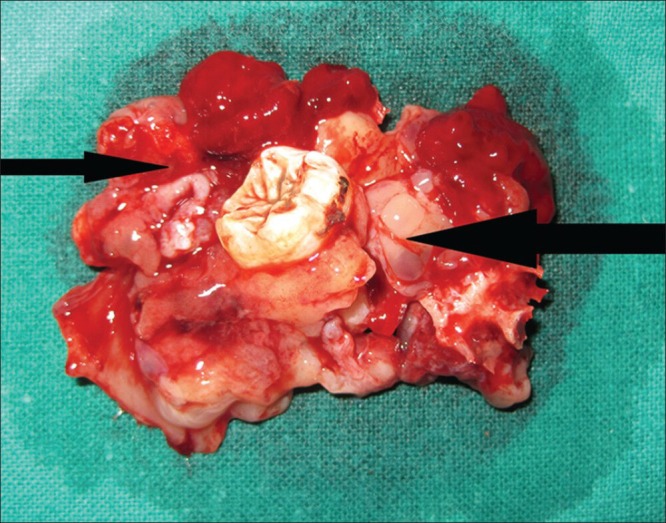
21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Excised specimen shows the cystic lining remnants along with the impacted third molar.
Figure 6.

21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Intra-operative photograph shows the exposed cystic lining (arrow).
Figure 7.

21-year-old female patient with swelling on the right side of the face and discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Photograph shows maxillary sinus (arrow) after removal of the cystic lining along with the impacted third molar.
Histopathological examination revealed non-keratinized stratified squamous epithelium confirming the clinical diagnosis of dentigerous cyst [Figure 9]. Postoperative panoramic radiograph after 6-months showed a normal maxillary sinus [Figure 10]. The patient was followed-up for a year and showed no abnormalities.
Figure 9.
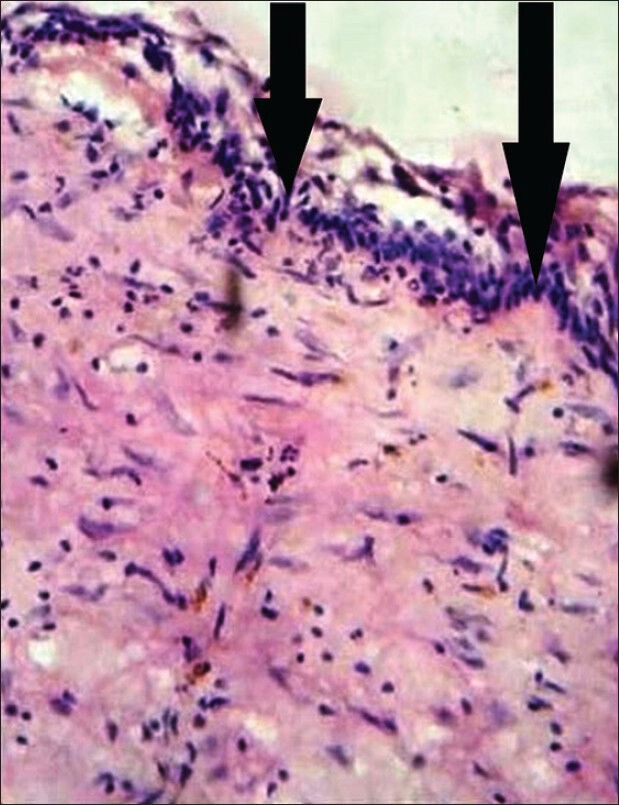
21-year-old female patient with swelling on the right side of the face with discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Histopathological slide reveals non-keratinized stratified squamous epithelium (arrow) of the cystic lining (hematoxylin and eosin stain, ×400).
Figure 10.
21-year-old female patient with swelling on the right side of the face with discharge of pus from the right nostril, diagnosed with dentigerous cyst of the maxillary sinus. Post-operative panoramic radiograph after 6 months shows normal appearance of the maxillary sinus (arrows).
DISCUSSION
Ectopic teeth are those located in the jaw bones or regions other than the alveolar arch. Ectopic eruption of a tooth is rare. However, there have been a few reports of tooth erupting in the nose, mandibular condyle, coronoid process, and maxillary sinus, which is also the largest of the paranasal sinuses.[4] Wisdom teeth are often impacted or in an ectopic position. One rather unusual location is the maxillary sinus. Usually these teeth are associated with dentigerous cysts, which can occupy the maxillary sinus partially or totally and can be the cause of various symptoms. Usually these teeth are detected during routine radiographic examination or the patient could have a history of typical, sinus-related symptoms.[4,5]
Dentigerous cyst is the most common of all follicular cysts, more common in males, occurring in the second or third decade of life. About 70% of dentigerous cysts occur in the mandible and 30% in the maxilla.[5,6] Teeth most commonly associated with dentigerous cyst are mandibular third molars, maxillary canines, mandibular premolars, and, very rarely, maxillary third molars. There are three variants of dentigerous cyst: (a) Central: Crown is enveloped by the follicle symmetrically, (b) Lateral: Dilatation of follicle on one aspect of the crown, and (c) Circumferential: The follicle expands in a manner which envelopes the entire tooth.
If infected, the treatment of choice is complete enucleation of the lesion intraorally with removal of the associated tooth. It is also important to completely remove all diseased antral tissues and thoroughly assess all resected soft tissue histologically with proper follow-up for a period of 1 year.[6]
When the cyst is smaller in size, it is difficult to differentiate a dentigerous cyst from a large but normal dental follicle. A working definition is that a dentigerous cyst exists when the distance between the crown and dental follicle is greater than 2.5-3.0 mm. The differential diagnosis of a dentigerous cyst includes unicystic ameloblastoma, adenomatoid odontogenic tumor (AOT), early stages of Gorlin cyst/calcifying epithelial odontogenic tumor (CEOT), ameloblastic fibroma, ameloblastic fibro-odontoma, and odontogenic keratocyst. Unicystic ameloblastoma occurs in people under the age of 30 years, is seen equally in both genders, and has a tendency to occur in the posterior mandible associated with the crown of an unerupted third molar.[7] AOT is common in the 2nd decade, affects females twice as often as males, and has a tendency to occur in the anterior maxilla and, in about 74% of cases, is associated with the crown of an unerupted canine and supernumerary teeth. However, AOT of the maxillary antrum is extremely rare. Gorlin cyst is commonly found in the incisor and canine area in about 65% of cases. Approximately one-third of cases are associated with an unerupted tooth, most often a canine. CEOT is an uncommon lesion, which is most often encountered between 3rd and 5th decades, occurs equally in both genders, and has a tendency to occur in posterior mandible associated with an impacted third molar. Ameloblastic fibroma is an uncommon tumor, occurs in the first 2 decades, more common in males, commonly found in posterior mandible, and is associated with an unerupted tooth in about 75% of cases. Ameloblastic fibro-odontoma often occurs in the maxilla and is associated with an impacted tooth. However, the ameloblastic fibro-odontoma is rarely found within the maxillary sinus and usually occurs in young adults under the age of 20 years. Odontogenic keratocyst may be found in patients in any age group, is commonly found in posterior body and ascending ramus of the mandible, and in 25-40% of cases, an unerupted tooth is involved.[7]
Histologically, dentigerous cysts are lined by a layer of non-keratinized stratified squamous epithelium, with a surrounding wall of thin connective tissue containing odontogenic epithelial rests. Cases of ameloblastoma or epidermoid carcinomas developing from the lining epithelium of a dentigerous cyst are adequately documented as potential long-term complications, whereas mucoepidermoid carcinomas are less well-documented.[8]
The standard treatment for a dentigerous cyst of maxilla is enucleation and extraction of the associated tooth via a Caldwell-Luc procedure under local or general anesthesia. In large cysts, an initial marsupialization to diminish the size of the osseous defect, followed by enucleation and tooth extraction, has been followed. The major disadvantage of marsupialization is recurrence or persistence of the lesion along with the residual cystic lining. Endoscopic approach for management of dentigerous cyst of maxilla is also described in the literature. This method is associated with lesser operative as well as postoperative morbidity.[9] Dentigerous cyst of maxilla may cause pathological jaw fracture if large enough, may transform into ameloblastoma, and has the potential of developing into squamous cell carcinoma and mucoepidermoid carcinoma if there is chronic infection. It has a recurrence rate of about 12-14%.[8,10]
CONCLUSION
Early diagnosis and treatment of odontogenic cyst lesions is very important to prevent morbidity. Imaging studies including CT scans aid in diagnosis of dentigerous cysts and associated tooth abnormalities. Knowledge of histopathologic features helps confirm the diagnosis. Management of dentigerous cyst arising from ectopic third molar in the maxillary sinus is usually enucleation. If left untreated, it has a tendency to transform into a tumor. Caldwell-Luc procedure along with enucleation and primary closure was followed in this case as the ectopic tooth was the cause of recurrent sinusitis and purulent rhinorrhea in spite of administering antibiotics repeatedly.
Footnotes
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2013/3/2/7/117461
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Szerlip L. Displaced third molar with dentigerous cyst--An unusual case. J Oral Surg. 1978;36:551–2. [PubMed] [Google Scholar]
- 2.Elango S, Palaniappan SP. Ectopic tooth in the roof of the maxillary sinus. Ear Nose Throat J. 1991;70:365–6. [PubMed] [Google Scholar]
- 3.Goh YH. Ectopic eruption of maxillary molar tooth-an unusual cause of recurrent sinusitis. Singapore Med J. 2001;42:80–1. [PubMed] [Google Scholar]
- 4.Amin ZA, Amran M, Khairudin Removal of extensive maxillary dentigerous cyst via a Caldwell-Luc procedure. Arch Orofac Sci. 2008;3:48–51. [Google Scholar]
- 5.Srinivasa Prasad T, Sujatha G, Niazi TM, Rajesh P. Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: A rare entity. Indian J Dent Res. 2007;18:141–3. doi: 10.4103/0970-9290.33793. [DOI] [PubMed] [Google Scholar]
- 6.Wang Chih-Jen, Huang Po-Hsien, Wang Yin-Lai, Shyng Yih-Chung, Kao Wen-Bin. Dentigerous cyst over maxillary sinus: A case report and literature review. Taiwan J Maxillofac Surg. 2009;20:116–24. [Google Scholar]
- 7.Mahesh KR, Umashankar DN, Nandakumar H, Radhika BM, Sudhakar Inflammatory variant of dentigerous cyst in maxillary sinus--A case report. Int J Oral Maxillofac Pathol. 2010;1:17–9. [Google Scholar]
- 8.Mohan S, Kankariya H, Harjani B, Sharma H. Ectopic third molar in the maxillary sinus. Natl J Maxillofac Surg. 2011;2:222–4. doi: 10.4103/0975-5950.94488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kasat VO, Karjodkar FR, Laddha RS. Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: A case report and review of literature. Contemp Clin Dent. 2012;3:373–6. doi: 10.4103/0976-237X.103642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yasuoka T, Yonemoto K, Kato Y, Tatematsu N. Squamous cell carcinoma arising in a dentigerous cyst. J Oral Maxillofac Surg. 2000;58:900–5. doi: 10.1053/joms.2000.8219. [DOI] [PubMed] [Google Scholar]