

Abstract
The purpose of this study was to document the extent of adhesion of 99mTc-sestamibi to syringes in patient procedures, determine factors that influence the degree of adhesion, and evaluate alternatives to our current practice that would either result in a more reproducible degree of adhesion or, ideally, eliminate adhesion.
Methods
The extent of adhesion was documented in 216 patient procedures and evaluated in detail in an additional 73 patient procedures. We evaluated the nature of the adhesion and its possible causes, including the location of adhesion in injection sets, the effect of syringe type, and the effect of prerinsing of syringes with various solutions of nonradiolabeled sestamibi and 99mTc-sestamibi. The extent of adhesion was reevaluated in 50 procedures performed using the syringe type that demonstrated the lowest adhesion rate.
Results
The degree of adhesion of 99mTc-sestamibi to the injection set was found to be 20.1% ± 8.0%, with a range (10th–90th percentiles) of 9%–31%. The primary cause of adhesion appeared to be the lubricant used inside the syringe barrel. Evaluation of 6 different syringe types identified a brand with a lower adhesion rate. Reevaluation in patient procedures using this brand showed a 5.2% ± 2.5% degree of adhesion, with a range (10th–90th percentiles) of 2.5%–7.7%.
Conclusion
Selection of the appropriate type of syringe can significantly reduce the magnitude and variability of residual 99mTc-sestamibi activity. With more reproducible residual activities, we have been able to achieve an approximately 20% reduction in the dispensed dose of 99mTc-sestamibi used in clinical procedures and a more consistent injected dose with less interpatient variation. The frequent changes in syringe design by manufacturers require that a quality control program for monitoring of residual activity be incorporated into clinical practice. This program has allowed us to maintain image quality and achieve more consistent injected patient doses in clinical procedures that use 99mTc-sestamibi.
Keywords: 99mTc-sestamibi, plastic syringe, adhesion, adsorption
Over the last 3–5 y, there has been increased scrutiny of the radiation burden associated with many diagnostic procedures. In 2010, the Food and Drug Administration announced an initiative to reduce unnecessary radiation exposure from 3 types of medical imaging procedures, one of which was nuclear medicine (1). Achieving a meaningful dose reduction requires that we look at all aspects of the imaging procedure to determine where reductions in patient dose can be achieved while maintaining the diagnostic quality of the image data.
Molecular breast imaging is a promising screening technique for the detection of breast cancer. This technique uses the radiopharmaceutical 99mTc-sestamibi and a dedicated direct conversion semiconductor-based γ camera for the detection of breast lesions (2). A key consideration in the use of molecular breast imaging for screening is the radiation dose associated with the procedure. Recent studies of direct-conversion molecular breast imaging have used the lowest reported doses to date of approximately 300 MBq (~8 mCi) of 99mTc-sestamibi (3). Efforts to further reduce doses below this level have been confounded by wide interpatient variation in the measured uptake of 99mTc-sestamibi in breast tissue. In evaluating this issue, we have frequently observed substantial retention of the radiopharmaceutical in the injection syringe, meaning that in many patients who receive a dispensed dose of 300 MBq, the actual injected dose is much lower, leading to inadequate image count density.
The issue of adsorption of radiopharmaceuticals to syringes has received sporadic attention over the years, with contradictory findings. Although some particulate preparations, such as 99mTc-macroaggregated albumin, are known to be susceptible to settling and require agitation before injection, most 99mTc-labeled radiopharmaceuticals are not considered to be problematic with regard to adhesion to the syringe. The most recent evaluation of retention of 99mTc-based radiopharmaceuticals in syringes by Mushtaq et al. (4) showed insignificant adhesion (<5%) of all tested radiopharmaceuticals (including 99mTc-sestamibi) to the plastic syringes. The primary cause of residual activity is usually thought to be dead space near the needle hub or poor technique on the part of the technologist performing the injection (5).
Ponto (6) noted that enhanced retention of lipophilic myocardial perfusion radiopharmaceuticals, such as 99mTc-sestamibi, has been reported in syringes constructed with elastomeric plunger tips. This enhanced retention appears to be related to greater adsorption to the elastomeric component of the plunger. For 99mTc-sestamibi, flushing the syringe with normal saline has been reported to remove up to 70% of this retained activity (7). Earlier studies by Jannson et al. (8) and Hurless et al. (9) have indicated that high adsorption of 99mTc radiopharmaceuticals can occur and appears to be highly dependent on the particular radiopharmaceutical and type of syringe.
High residual activity in syringes can lead to several problems, including the delivery of a suboptimal dose to the patient, resulting in poor image quality or extended imaging times, and can confound efforts to lower the recommended minimum administered dose and reduce the radiation burden to the patient. The purpose of this study was to document the extent of adhesion of 99mTc-sestamibi to syringes in our molecular breast imaging procedures, determine factors that influence the degree of adhesion in syringes, and evaluate alternatives to our current practice that would either result in a more reproducible degree of adhesion or, ideally, eliminate adhesion.
MATERIALS AND METHODS
Preparation of 99mTc-Sestamibi Kits
All procedures were performed using a generic brand of sestamibi (DraxMIBI; DraxImage). Because of the large volume of procedures performed in our laboratory, there was considerable variability in the specific activity of the sodium pertechnetate used for kit preparation and in the age of the eluate from the 99Mo-generators. All sestamibi kits were prepared with the addition of 15–30 GBq (400–800 mCi) of 99mTc-sodium pertechnetate.
Patient Procedures
This was a prospective analysis of residual activity in the injection syringes used for patients who had been enrolled in a variety of Institutional Review Board–approved research protocols. Women who were pregnant or lactating were excluded from all protocols. Written informed consent was obtained from all participants. No patients were recruited solely for the purpose of this study.
Injections for Patient Procedures
For all patient procedures, 99mTc-sestamibi was drawn up in a 3-mL syringe to a volume of approximately 1 mL. Injections were performed using a winged infusion set and extension tubing. Once venous access had been established, the 99mTc-sestamibi was pushed into the tubing. A 10-mL syringe containing 0.9% sodium chloride solution (saline) was used to flush the 99mTc-sestamibi bolus. The saline was then used to rinse any remaining activity in the sestamibi syringe into the tubing, which was then flushed with the rest of the saline. For each study, the injection syringe was rinsed 3 times with saline. All patient procedures were initially performed using brand A syringes. Table 1 lists the various brands of syringes evaluated in this study.
TABLE 1.
Mean and SD of 10 Measurements of Residual Activity in 6 Different Types of Syringes
| Syringe | Syringe capacity (mL) | Manufacturer | Brand | Residual activity (%) | ||
|---|---|---|---|---|---|---|
| Mean | SD | P | ||||
| Brand A | 3 mL | Covidien | Monoject 3 cc | 19.7 | 2.6 | – |
| Brand B | 3 mL | BD Medical | BD 3 cc | 21.5 | 5.6 | NS |
| Brand C | 1 mL | Covidien | Monoject 1 cc insulin | 17.5 | 3.2 | NS |
| Brand D | 1 mL | Covidien | Monoject 1 cc tuberculin | 15.6 | 2.8 | P < 0.01 |
| Brand E | 1 mL | Terumo Medical | Terumo 1 cc | 13.1 | 3.0 | P < 0.001 |
| Brand F | 3 mL | DPS Meditech | DPS 3 cc | 11.4 | 3.6 | P < 0.001 |
NS = not statistically significant.
Documentation of Extent of Adhesion
The extent of adhesion was evaluated in brand A syringes, which were used in 216 low-dose molecular breast imaging procedures with dispensed doses of approximately 200 MBq (~5.5 mCi) of 99mTc-sestamibi. The dispensed activity in the 99mTc-sestamibi syringe and residual activity after injection in the complete syringe and infusion set tubing were assayed using a dose calibrator located in the injection room. The assay times were recorded and decay corrections applied to the residual activity. The percentage residual activity was calculated.
Influence of Patient Factors on Residual Activity
To rule out potential confounding factors that may be patient-dependent (e.g., effect of blood drawn back into the tubing on the adhesion of the 99mTc-sestamibi to the syringe or tubing), 2 identical injection sets were prepared for 7 patient procedures. One was used to administer the 99mTc-sestamibi to the patient as described above. The second set was used for a sham injection in which the 99mTc-sestamibi was injected into an empty vial (no rinsing was performed). The percentage residual activities in the syringes from the patient and sham injections were then compared.
Location of Residual Activity
A comprehensive analysis of the location of the residual activity was performed on the injection sets from 73 molecular breast imaging procedures that were performed with dispensed doses of 150–300 MBq (4–8 mCi) of 99mTc-sestamibi. In each study, after administration of the 99mTc-sestamibi, the injection set was dismantled and the amounts of activity in the syringe barrel, plunger, saline syringe, and tubing were separately measured. The percentage residual activity was recorded along with injection volume and the day of the week. The last factor was included to evaluate any potential impact of 99Mo-generator age on the adhesion properties of 99mTc-sestamibi.
Time Course of 99mTc-Adhesion to Syringe
To determine the effect of the residence time of the 99mTc-sestamibi in a syringe, each of 6 syringes (brand A) was used to draw up a 300-MBq (8-mCi) dose of 99mTc-sestamibi from the same reconstituted vial of 99mTc-sestamibi. The activity in each syringe was assayed. Every 10 min, the contents of one of the syringes were expelled into an empty glass vial, allowing residual activity to be assessed with residence times from 10 min to 1 h after preparation. The residual activity in each syringe was assayed with the appropriate correction for decay, and percentage residual activity was calculated.
Effect of Prerinse with Sestamibi and 99Tc-Sestamibi
We evaluated whether the amount of residual activity could be reduced by prerinsing syringes with either nonradiolabeled sestamibi or 99Tc-sestamibi. All procedures were performed using brand A syringes. Five syringes were used as controls, 5 syringes were prerinsed with nonradiolabeled sestamibi that had been reconstituted in saline (no 99mTc-pertechnetate was added to the vial during preparation), and 5 syringes were prerinsed with 99Tc-sestamibi (for this study, a 99mTc-sestamibi kit was allowed to decay over 24–48 h to 99Tc-sestamibi). Each syringe was then used to draw up a 300-MBq (8-mCi) dose of 99mTc-sestamibi from the same reconstituted vial of 99mTc-sestamibi. The activity in each syringe was assayed. The 99mTc-sestamibi was then expelled into empty glass vials. The residual activity in each syringe was assayed with the appropriate correction for decay, and percentage residual activity was calculated.
Effect of Syringe Type and Size
Six different types of syringes were available for evaluation in our radiopharmacy. Table 1 lists the brands and characteristics. Five of the syringe types (brands A–E) were in routine use in the laboratory before this study, and brand F was purchased and evaluated on the basis of feedback from other laboratories on the issue of residual activity. For each syringe, a 300-MBq (8-mCi) dose of 99mTc-sestamibi in a volume of 1 mL was drawn up and assayed. The activity in each syringe was then expelled into an empty glass vial. The syringes were not rinsed. The residual activity in each syringe was assayed with the appropriate correction for decay, and percentage residual activity was calculated. This process was repeated 10 times for each type of syringe (60 syringes evaluated).
Effect of Multiple Prerinses with 99mTc-Sestamibi
On the basis of the results from the prerinse experiment, we also evaluated whether adhesion of 99mTc-sestamibi was altered by repeatedly drawing up a dose of 99mTc-sestamibi, assaying the activity, expelling the activity into an empty vial, and drawing up another equivalent dose of 99mTc-sestamibi. We repeated this process 15 times, assaying the residual activity after each process. This process was performed on 2 types of syringes, brands A and F. The latter had demonstrated the lowest residual activity in the previous experiment. This process was also performed on brand A syringes after prerinsing with an acetone solution followed by a saline solution. The purpose was to determine whether partial washing of the syringe barrel and plunger would alter the characteristics of the plastic or remove any lubricants used in syringes and thereby affect adhesion of 99mTc-sestamibi to the syringes.
Adhesion to Syringe Surface
To determine whether the plastic material or the coating or lubricant used in the syringe barrel was the primary factor in adsorption of the 99mTc-sestamibi, an empty syringe was dipped into a solution of 99mTc-sestamibi, coating only the outside surface (which would not be coated with any lubricant). The surface was then washed with water. A second syringe was used to draw up 1 mL of the same 99mTc solution. The activity was then expelled, and the second syringe was rinsed 3 times with water. Both syringes were then imaged under a γ camera to determine the location and extent of residual activity.
Reevaluation of Residual Activity in Patient Procedures
After completion of the above experiments, we replaced brand A syringes with brand F for our molecular breast imaging procedures. Fifty molecular breast imaging procedures were performed with brand F syringes using dispensed doses of 150–300 MBq (4–8 mCi) of 99mTc-sestamibi. All injections were performed as described previously. Initial activity in the 99mTc-sestamibi syringe and residual activity were again assayed, and the percentage residual activity was determined.
Statistical Analysis
Paired t tests were used to compare residual activity in patient and sham injection procedures and to compare cumulative residual activity after multiple rinses with 99mTc-sestamibi. Unpaired t testing was used to determine differences in the percentage residual activity for different types of syringes, both in patient procedures and in testing.
RESULTS
Figure 1A shows the relationship between the dispensed activity and injected activity (dispensed – residual activity in syringe/tubing) of 99mTc-sestamibi in 216 patients who underwent molecular breast imaging procedures. Correlation was poor between the dispensed and injected activities (R2 = 0.19). Figure 1B shows the distribution of residual activities in the syringes and associated infusion set tubing, with a range (10th–90th percentiles) of 9%–31%. The average residual activity (±SD) was 20.1% ± 8.0%. These figures confirm a substantial and highly variable loss of activity due to adhesion of the 99mTc-sestamibi to the syringe and infusion set tubing with brand A syringes.
FIGURE 1.
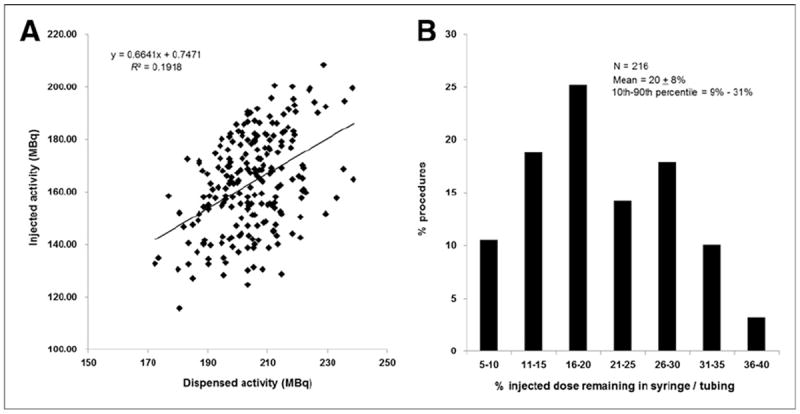
(A) Relationship between dispensed activity and injected activity of 99mTc-sestamibi in 216 patient procedures performed with brand A syringes. (B) Histogram showing distribution of residual activity in syringes and infusion sets used in 216 procedures.
Figure 2 compares the percentage residual activity in syringes after a patient injection and a sham injection. The average residual activity was 20.1% ± 8.4% in the patient procedures and 27.6% ± 11.4% in the sham injection procedures. The residual activity in the sham injection procedures was significantly higher than that in the patient procedures (P < 0.01) and was most likely due to the fact that no saline rinse was performed for the sham injections. More important, patient factors did not appear to contribute to the residual dose.
FIGURE 2.
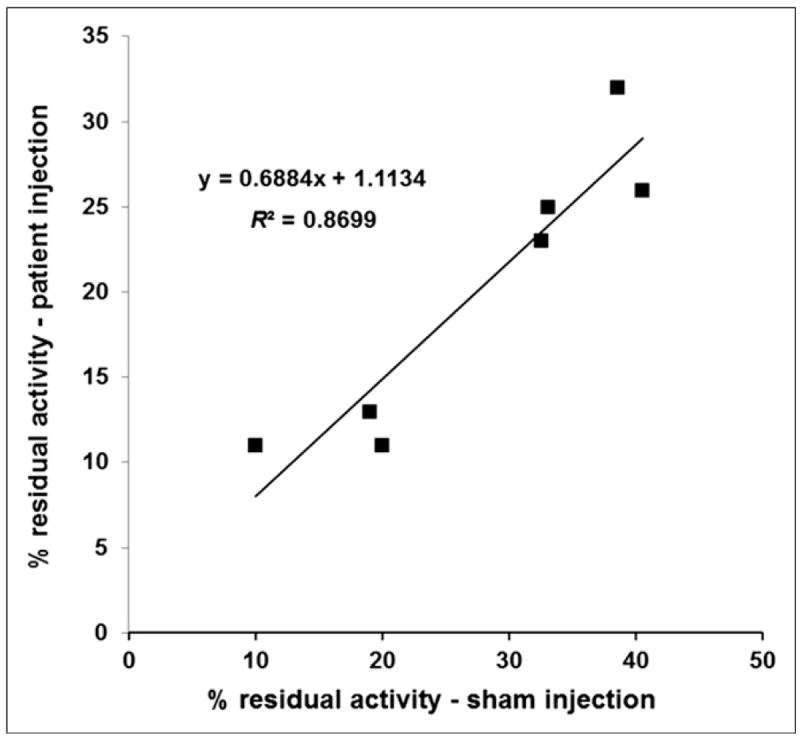
Correlation between percentage residual activity in patient syringe (rinsed 3 times with saline) and percentage residual activity in sham syringe (no rinsing) that was prepared under identical conditions to patient syringe.
Analysis of the location of the residual activity was performed in 73 procedures and showed that overall residual activity was 22% ± 8%, with 11% ± 4% in the syringe barrel, 9% ± 5% in the plunger, 1% in the needle and cap, and 1% in the butterfly tubing. No residual activity was recorded in the saline syringes. No correlation was found between the amount of residual activity and the day of the week. The average volume of the injection was 1.04 ± 0.26 mL, and within the small range of volumes used in these procedures, no correlation was observed between volume and residual activity. Results from the residence time experiment in which residual activity was assessed from 10 min to 1 h after the activity was drawn showed an average residual activity of 15.4% and no appreciable change over time, indicating that adhesion occurred within the first 10 min and remained unchanged afterward.
Prerinsing the syringes with either nonradiolabeled sestamibi or 99Tc-sestamibi did not eliminate adhesion to the syringes but did result in a small reduction in adhesion, which was significant only for syringes prerinsed with 99Tc-sestamibi. Unrinsed syringes had a residual activity of 20.1% ± 1.4%, compared with 19.6% ± 1.6% (unpaired t test, P = 0.6) for syringes prerinsed with nonradiolabeled sestamibi and 18.4% ± 0.6% (unpaired t test, P < 0.04) for syringes prerinsed with 99Tc-sestamibi. Figure 3 shows that with each successive loading and emptying of the same amount of 99mTc-sestamibi activity and volume, there was increased accumulation of residual activity in the syringe with no indication of a saturation point or plateau in the amount of residual activity in the syringe. Brand F syringes demonstrated a significantly lower cumulative activity than brand A (P < 0.001). Rinsing brand A syringes in acetone before use resulted in a small but significant reduction in the adhesion of 99mTc-sestamibi to the syringes (P < 0.01).
FIGURE 3.
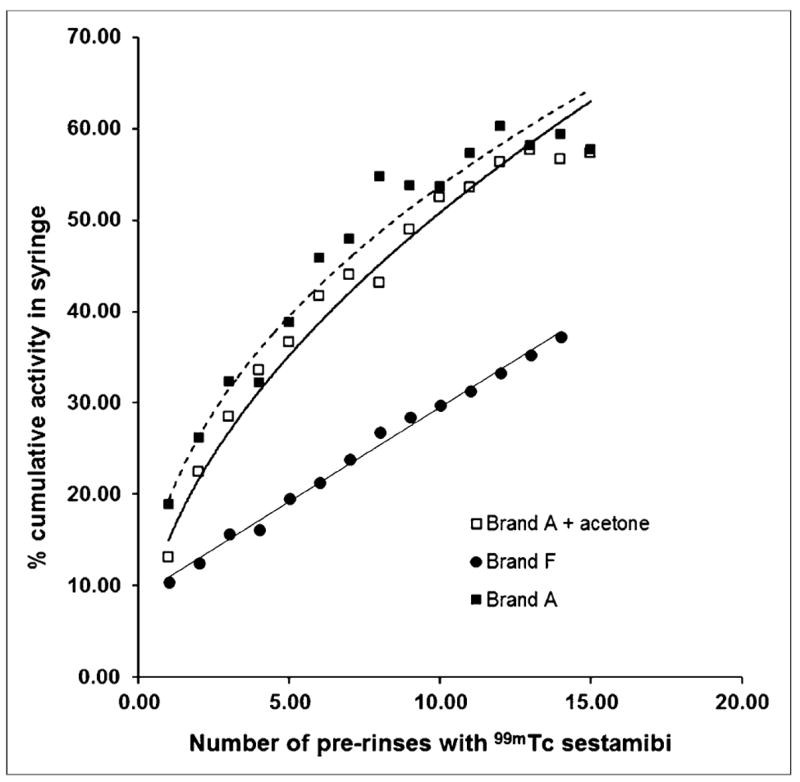
Effect of up to 15 prerinses on cumulative residual activity in brand A (both with and without prior wash in acetone) and brand F syringes.
Figure 4 shows γ-camera images of the 2 syringes exposed to 99mTc-sestamibi, one on its outer surface and the other internally. High levels of adsorption were observed internally in 2 parts of the syringe, the section of the syringe that contained the 1-mL solution of 99mTc-sestamibi and the plunger (Fig. 4, internal). Some activity was also seen on the remainder of the internal wall of the syringe, possibly because of contamination from the plunger when it was drawn back to the end of the barrel. Adhesion of the 99mTc-sestamibi was also observed on the outer surface (Fig. 4, external). Region-of-interest analysis, normalized to total residual activity in the syringe with internal activity, indicated that 48% of total activity was located on the 0- to 1-mL section of the internal wall, 50% of total activity was on the plunger, and 2% was on other parts of the barrel. In comparing total activity on the syringe with internal residual activity, activity on the external surface of the syringe was only 13%. Hence, adhesion appears to be influenced primarily by the type of coating or lubricant used inside the syringe barrel.
FIGURE 4.
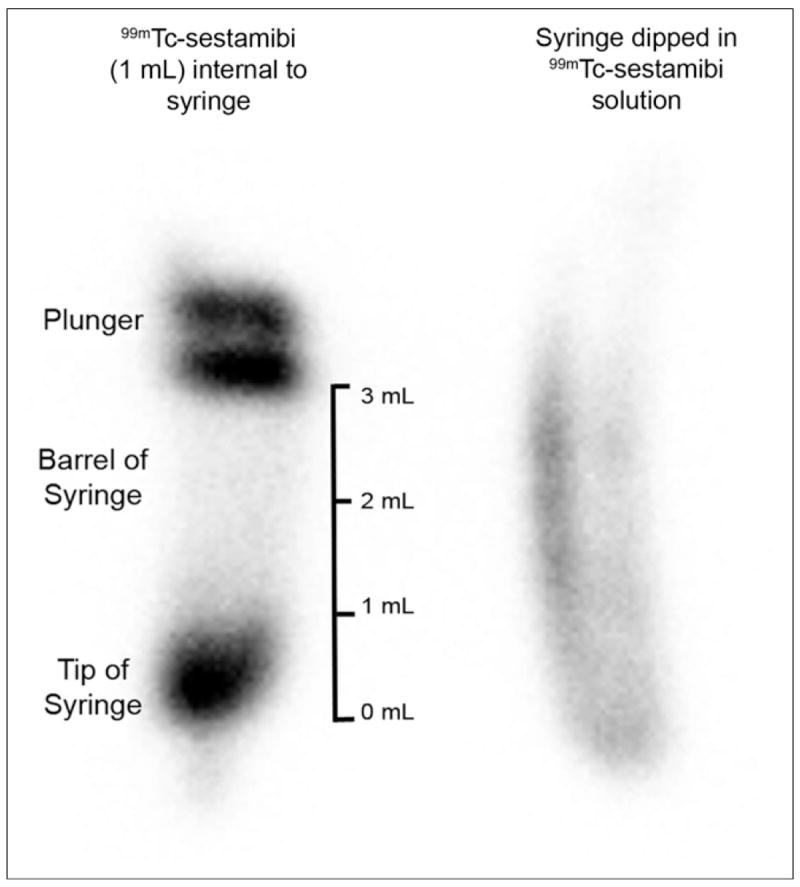
γ-camera image of 2 brand A syringes. Syringe on left was used to draw up 1 mL of 99mTc-sestamibi solution. Syringe on right was dipped in same 99mTc solution up to top of barrel. Both syringes were then emptied and rinsed with water.
Table 1 shows the average residual activity for 6 different types of syringes that were available in our radiopharmacy. The most commonly used 3-mL syringes in our nuclear medicine pharmacy (brands A and B) demonstrated the highest residual activities: approximately 20%. Only two of the 1-mL syringes (brands D and E) demonstrated significantly lower residual activities than the 3-mL syringes. The lowest residual activity was observed in brand F (~11%).
Reevaluation of residual activity in 50 patients using brand F showed that the average had decreased to 5.2% ± 2.5%. Figure 5A shows the distribution of residual activity in these 50 procedures with brand F compared with the 73 procedures with brand A described above, in which average residual activity was 22.0%. The use of brand F syringes also improved the correlation between the dispensed dose and injected dose of 99mTc-sestamibi (Fig. 5B) (R2 = 0.96 for brand F compared with R2 = 0.88 for brand A).
FIGURE 5.
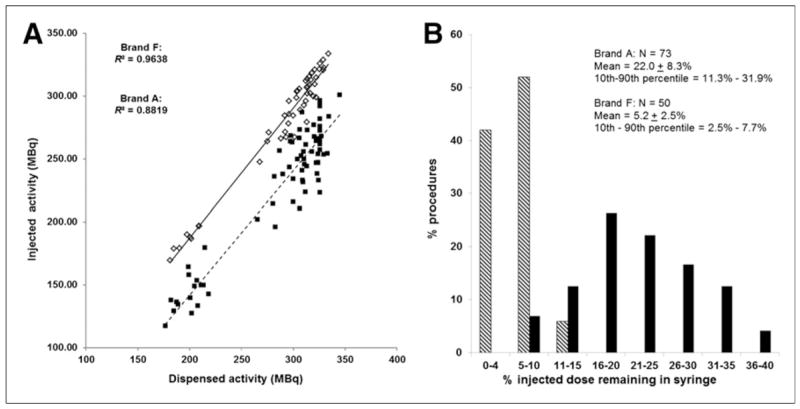
(A) Relationship between dispensed activity and injected activity of 99mTc-sestamibi in brand A syringes (73 procedures) and brand F syringes (50 procedures). (B) Histogram showing distribution of residual activity in brand A and brand F syringes.
DISCUSSION
The issue of adsorption of radiopharmaceuticals to syringes has been previously reported for a variety of 99mTc compounds (4-9). A study from 2008 had not indicated this to be a significant issue for 99mTc-sestamibi (4). In contrast, we have found that adsorption of 99mTc-sestamibi to syringes is a significant problem, in terms of both the magnitude of the adsorption and the variability. The results from Figure 1 show a poor correlation between the dispensed dose of 99mTc-sestamibi and the injected dose and highlight the magnitude of the problem. What is more problematic is the variability in the degree of adhesion: from 9%–31% in these studies. This large variability makes it difficult to use lower administered doses, as the result will likely be a small percentage of procedures with suboptimal uptake in the breast tissue, resulting in nondiagnostic images. Although there is a small possibility that interaction of the patient’s blood with the butterfly set and tubing may be partly responsible for this adhesion, both the finding of minimal residual activity in the butterfly and tubing and the finding of higher residual activity in sham injections relative to patient injections indicate that patient factors are unlikely to be the primary cause of high residual activity.
Evaluation of the factors contributing to adhesion does not clearly point to a single simple phenomenon. Adhesion of the sestamibi appears to occur both in the section of the syringe barrel that contained the 99mTc-sestamibi and on the plunger, with comparable activities on both parts. Adsorption onto the syringe appears to be rapid and did not change over the course of an hour. Multiple rinses of the syringes with saline failed to dislodge the activity.
We initially expected that this was a simple chemical phenomenon between the 99mTc-sestamibi and the syringe, involving adsorption of sestamibi onto binding sites in the plastic or rubber components of the syringe. However, if so, we would have expected that prerinsing the syringe with various formulations of sestamibi would saturate the available binding sites on the plastic and reduce or eliminate the degree of adsorption of the radioactivity.
As this did not appear to be the mechanism, we looked at multiple cycles of drawing 99mTc-sestamibi into a syringe and expelling it. Figure 3 shows that with each cycle, we observed increasing accumulation of the 99mTc-sestamibi on the syringes. Figure 4 shows that this adhesion occurred only inside the syringe and that little to no 99mTc-sestamibi adhered to the external surface. The only difference between the inner and outer surfaces of syringes is the coating or lubricant used to enable smooth movement of the plunger in the syringe. We believe that this coating or lubricant is the primary material to which the 99mTc-sestamibi is adhering. We hypothesize that as the syringe is depressed and loaded, the surface of the lubricant that had adsorbed some 99mTc-sestamibi is now changed, exposing a new surface that now allows for additional adsorption of the 99mTc-sestamibi.
Evaluation of different syringes indicated that, in this study, brand F demonstrated considerably less adhesion than other 3-mL syringes and lower adhesion than any of the 1-mL syringes evaluated. A previous study (9) found that brand A demonstrated lower adhesion than other brands. However, it is likely that manufacturers continuously alter and update their manufacturing process, resulting in changes in the type of plastic and the coating used in the syringes. Hence, although this study demonstrated that brand F had the lowest susceptibility to adhesion of 99mTc-sestamibi, these results may not hold true over time. A program of monitoring the residual activity in a percentage of clinical procedures should be implemented to ensure that any changes in syringe design and method of manufacture that could potentially affect the degree of adhesion are detected early so that alternative syringes can be investigated.
The results from the 2 smaller patient studies clearly show the significant reduction (P < 0.0001) in the variability of residual activity in patient doses with the switch from brand A (22.0% ± 8.3%) to brand F (5.2% ± 2.5%). With residual activities of approximately 5%, we have been able to achieve an approximately 20% reduction in the dispensed dose of 99mTc-sestamibi used in molecular breast imaging procedures (from 300 to 240.5 MBq [~8 to ~6.5 mCi]) and a more consistent injected dose with less interpatient variation. Monitoring of residual activity has become an important component in our dose reduction strategy for molecular breast imaging. Although this study has focused on use of 99mTc-sestamibi in molecular breast imaging, these results are obviously generalizable to the more common clinical procedures that use 99mTc-sestamibi, such as myocardial perfusion imaging and parathyroid imaging, and should allow for a more consistent injected dose for these procedures.
CONCLUSION
Selection of an appropriate type of syringe can significantly reduce the magnitude and variability of residual 99mTc-sestamibi activity. With more reproducible residual activities, we have been able to achieve an approximately 20% reduction in the dispensed dose of 99mTc-sestamibi used in clinical procedures and a more consistent injected dose with less interpatient variation. The frequent changes in syringe design by manufacturers require that a quality control program for monitoring of residual activity be incorporated into clinical practice. This program has allowed us to maintain image quality and achieve more consistent injected patient doses in clinical procedures that use 99mTc-sestamibi.
Acknowledgments
This research was funded in part by grants from the Mayo Foundation, Friends for an Earlier Breast Cancer Test, and the National Institutes of Health (grant CA128407).
Footnotes
NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNMMI WEB SITE (http://www.snmmi.org/ce_online) THROUGH DECEMBER 2015.
DISCLOSURE
No other potential conflict of interest relevant to this article was reported.
References
- 1.FDA unveils initiative to reduce unnecessary radiation exposure from medical imaging. U.S. Food and Drug Administration; [October 22, 2013]. Web site. http://www.fda.gov/News-Events/Newsroom/PressAnnouncements/ucm200085.htm. Published February 9, 2010. [Google Scholar]
- 2.Rhodes DJ, Hruska CB, Phillips SW, Whaley DH, O’Connor MK. Dedicated dual-head gamma imaging for breast cancer screening in women with mammographically dense breasts. Radiology. 2011;258:106–118. doi: 10.1148/radiol.10100625. [DOI] [PubMed] [Google Scholar]
- 3.Hruska CB, Weinmann AL, Tello-Skjerseth CM, et al. Proof of concept for low-dose molecular breast imaging with a dual-head CZT gamma camera. Part II. Evaluation in patients. Med Phys. 2012;39:3476–3483. doi: 10.1118/1.4719959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mushtaq A, Rehman T, Mansur MS, Jehangir M. Adsorption of 99m-Tc-radiopharmaceuticals onto injection vials and syringes. J Nucl Med Technol. 2008;36:91–94. doi: 10.2967/jnmt.107.048561. [DOI] [PubMed] [Google Scholar]
- 5.Keskinteppe D, Ozer AY. Residual radioactivity in the syringes used in injection of radiopharmaceuticals and factors affecting the amount of residual activity. FABAD J Pharm Sci. 2005;30:176–180. [Google Scholar]
- 6.Ponto JA. Preparation and dispensing problems associated with technetium Tc-99m radiopharmaceuticals. In: Hladik E, editor. Correspondence Continuing Education Courses for Nuclear Pharmacists and Nuclear Medicine Professionals. Vol. 2. Albuquerque, NM: University of New Mexico Health Sciences Center; 2004. [Google Scholar]
- 7.Cheng K, Ngo T. Stability and adsorption of Tc-99m sestamibi in plastic syringes. J Am Pharm Assoc. 2002;42:306. [abstract] [Google Scholar]
- 8.Jansson BA, Goransson MB, Agren BN. Adsorption of some technetium-99m radiopharmaceuticals onto disposable plastic syringes. J Nucl Med Technol. 1998;26:196–199. [PubMed] [Google Scholar]
- 9.Hurless LM, Graves MW, Mufti OI, Quinton TM. The adsorption of technetium-99m sestamibi onto three plastic syringes: an evaluation of dosage administration error. J Nucl Med. 2000;41(suppl):250P–251P. [Google Scholar]