

Abstract
Background:
Vast majority of cardiac patients who refer to cardiac rehabilitation program (CRP) are obese and obesity is associated with coronary heart disease (CHD). So, the aim of this study is to investigate the effects of CRP on obesity indexes, lipid profiles, and functional capacity (FC) in obese men with CHD and to explore whether significant weight reduction affected these risk factors and FC or not.
Materials and Methods:
In an observational study, we evaluated 536 patients, including 464 non-obese men and 72 obese men. All participants completed CRP for 2 months; then, obese patients were divided into two groups: patients with weight reduction ≥ 5% and patients who didn’t have significant weight reduction. Data were analyzed with SPSS software version 15. For comparing the mean of outcomes independent t-tests and paired t-tests were used.
Results:
Results showed following CRP, non-obese men had significant improvement in obesity indexes (P = 0.00), lipid profiles (P < 0.05), and FC (P = 0.00) and in obese men, favorable improvement were seen in obesity indexes (P = 0.00), FC (P = 0.00), and total cholesterol (P = 0.02). Comparing two groups revealed that there were significant differences in obesity indexes, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol/high-density lipoprotein cholesterol ratio. In addition, comparing subgroup of obese patients revealed that there were significant differences in FC (P = 0.00) and low-density lipoprotein cholesterol/ high-density lipoprotein cholesterol ratio (P = 0.04).
Conclusion:
CRP has more advantage in management of obesity, FC, and lipid profiles in both obese and non-obese patients. Also, weight reduction may cause greater improvement in FC and fitness levels in obese men with CHD.
Keywords: Coronary artery disease, obesity, risk factor cardiac rehabilitation program, weight reduction
INTRODUCTION
Nowadays, the prevalence of obesity has reached epidemic levels in both industrialized societies and developing countries.[1] More important, obesity, which defined as body mass index higher than 30,[2] has adverse effects on coronary artery disease (CAD) through its influence on some risk factors including hypertension, type 2 diabetes, glucose intolerance, left ventricular hypertrophy, and functional capacity (FC).[3,4,5,6] Also, some investigations proposed that obesity is an independent risk factor for CAD.[4,7] Generally, 80% of patients who referred to cardiac rehabilitation program (CRP) were overweight and obese.[3]
Many studies suggested that CRP improves cardiovascular adaptations by increasing FC, endurance, skeletal muscle strength, and decreasing the symptoms of cardiovascular disease.[8,9,10] In fact, these central and peripheral adaptations resulting in a widened difference in oxygen content between arterial and venous blood during maximal exercise and an increased capacity to deliver substrate to skeletal and cardiac muscle. Also, CRP has beneficial effects on associated risk factors such as high-density lipoprotein cholesterol (HDL-C), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), excess weight, and insulin resistance after cardiac events.[11,12] But, limited surveys exist in relation to the effectiveness of CRP on obesity indexes, lipid profiles, and FC in obese men with CAD, and the benefits of weight reduction in these obese patients; So, the aim of this study is to investigate the effects of CRP on obesity indexes, lipid profiles, and FC in obese men with coronary heart disease (CHD) and to explore whether significant weight reduction has effect on these risk factors or not?
MATERIALS AND METHODS
In an observational study between 2000 and 2011 we evaluated 536 men patients with CAD who referred to phase II cardiac rehabilitation of Isfahan Cardiovascular Research Institute. CAD was defined as a history of one of the following: myocardial infarction (MI), coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), and chronic stable angina. After admission to CRP, height (without shoes) and weight of each patient were measured by nurse after overnight fasting and after voiding and then body mass index (BMI) was calculated by weight/height2 (kg/m2). Blood sample was taken after 12-14 hours of fasting for measuring serum lipids including triglycerides (TG), TC, HDL-C using enzymatic methods and LDL-C was calculated according to the Friedewald formula.[13] All patients used their angina treatment and dose of these medications were not altered during the program and nobody received any other weight reduction drug treatment. Also, exercise test with the protocol of Naughton was performed on each patient under supervision of a cardiologist. Exercise test provides an opportunity to determine body reaction and FC. All tests were evaluated at the beginning of the study. Then all participants began CRP for 2 months which consisted of 24 sessions and three times a week. CRP included exercise training sessions, nutritional and psychological consultation, and risk factor management. Exercise sessions were similar in obese and non-obese patients. Exercise training consisted of combined aerobic and resistance training and it was performed in cardiac rehabilitation center under supervision of physician, exercise physiologist, and a nurse by using treadmill, stationary cycles, stationary steppers, stair climbing, rowing, jogging, and some resistance devices. Each session lasted up to 90 minutes, 20-minute warm-up followed by 60 minutes aerobic and resistance training, and finally 10 minutes cool-down. The intensity of training was established according to the clinical condition and calculated between 60% and 85% of maximum heart rate. As well, all participants had dietary instruction by visiting dietitian in this duration and all of them were encouraged by the physicians, exercise physiologists, and dietitians to complete CRP. After passing 2 months and finishing rehabilitation program, all tests were carried out by each patient again. Patients were classified into obese (BMI ≥ 30) and non-obese (BMI < 30); after that, obese patients who had 5% or more weight reduction set in the first group and patients who didn’t lose their weight or had less than 5% set in the second group. This research project with the number of 90126 was taken under the medical ethics standards and approved in ethic committee of Isfahan Cardiovascular Research Institute. Independent sample t-tests were used to identify baseline differences and also final differences. For investigation about changes between baseline and completion of CRP, we used paired t-tests. Results are expressed as mean and Standard Error (SE) and the level of significance was set at P < 0.05.
RESULT
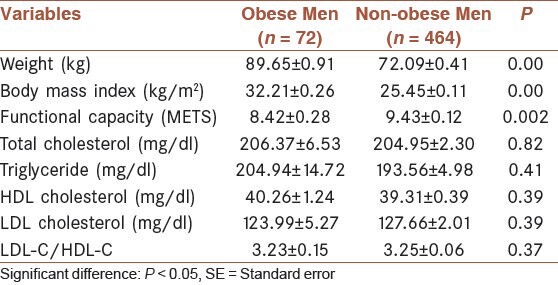
536 men patients with CHD were evaluated. At first, they were divided into two groups, patients who had BMI ≥ 30, n = 72 and age = 54.47 ± 9.63 years set as thenobese group and patients who had BMI <30, n = 464 and age = 56.21 ± 9.94 years set as the non-obese group. Subgroup of obese patients was divided into two groups. Obese patients who lost their weight ≥ 5%, n = 18 known as the first group and who didn’t have weight reduction or had less than 5%, n = 43 known as the second group. Independent sample t-tests were used to identify baseline differences among obese and non-obese men patients [Table 1]. At baseline, comparing two groups showed significant differences in obesity indexes (P = 0.00) and FC (P = 0.002).
Table 1.
Baseline differences between obese and non-obese men patients
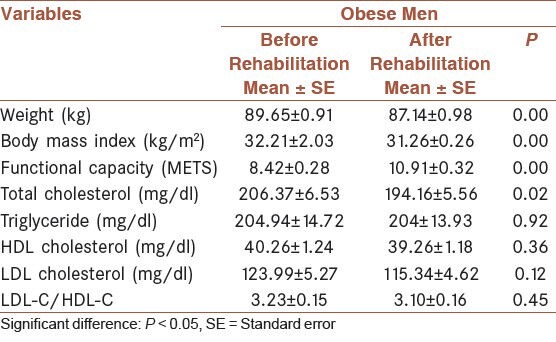
Also, paired t-tests were used to examine changes between baseline and completion of CRP in both groups. These tests revealed significant improvement in all evaluated factors such as obesity indexes (P = 0.00), FC (P = 0.00), and lipid profiles (P = 0.00) in the non-obese group. About the obese group, they had favorable differences in obesity indexes, FC, and TC; but, they didn’t have significant improvement in other lipid profiles [Table 2].
Table 2.
Comparison the changes in obese men following cardiac rehabilitation program
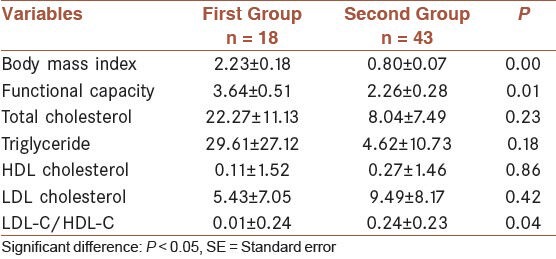
In addition, subgroups of obese men, first and second groups, were compared by independent t-tests [Table 3]. Findings showed significant differences in obesity indexes, FC, and LDL-C/HDL-C between the first group which had 5% or more weight reduction and the second group with no significant weight reduction.
Table 3.
Changes in lipid profiles and functional capacity in obese patients with ≥5% weight reduction versus obese patients with no significant weight reduction
DISCUSSION
The high prevalence of obesity is the most significant public health problem. Since, obesity is common in patients with CAD who referred to CRP; thus, present study investigated benefits of CRP in obesity indexes, FC and lipid profiles in obese and non-obese men with CAD, as well as, consideration the effects of weight reduction on evaluated factors in obese men with CAD.
In this study, following CRP, both groups achieved positive improvement in weight and BMI. Comparing two groups showed significant differences between these groups, and obese patients had greater improvement in weight reduction and BMI. In this regard, there are many studies which confirmed our results and they showed that CRP and exercise training have a positive effect in losing weight in all participants.[11] Ades et al showed high calorie expenditure exercise has advantage in losing weight in overweight coronary patients.[14] Also, another study showed the positive effects of short-term CRP on weight reduction and FC in obese patients with CAD.[15] But, Kiat et al suggested CRP didn’t had effect on weight reduction, while it is useful in increasing levels of FC.[16]
Also, obesity is known as a predictor in lower FC and fitness level in CAD patients. Like that, our finding showed that obese patients had lower FC than non-obese patients at baseline. Following CRP, both groups had significant improvement in FC, while obese patients attained greater development; however, this difference wasn’t significant. And finally, no significant difference was observed between two groups. Therefore, it should be interpreted, patients who had lower FC and higher weight in baseline, usually obtain greater improvement in these value after CRP.[17]
Our results illustrated that there were no differences in lipid profiles between obese and non-obese men patients, at baseline. But following CRP, significant improvements were seen in all lipid profiles in non-obese patients. In obese patients, this positive improvement was only perceived in TC. In fact, obese patients had modest overall lipid improvement. Comparing these changes between two groups didn’t show any significant differences in most lipid factors except HDL and LDL-C/HDL-C. These data revealed that passing one period of CRP is useful in most lipid profiles in both obese and non-obese men with CAD. Attributed study suggested that CRP have useful effects on losing body weight, decreasing TG, and increasing HDL-C in all CHD patients.[18] In addition, another research showed that the obese patients with CAD had improvement in BMI and some lipid factors after cardiac rehabilitation; but against our finding, it revealed that the differences in BMI, weight, and some lipid factors were not statistically significant in non-obese patients.[19] There are many studies which confirmed the significant improvement in FC, obesity indexes, and lipid profiles after CRP in CAD patients with each age without any attention to BMI levels.[12,20,21] Our pervious investigation by a comparison of the non-obese males and females with CAD revealed that CRP plays a key role in improving the FC and all lipid profiles in both groups, without any attention to gender differences.[22] Another study showed that CRP have positive effects in lipid profiles in both hypertriglyceridemia and non-hypertriglyceridemia patients.[23,24] In spite of some disparities, a number of these results are similar with our finding. We can deduce that the cause of these variations may exist in difference in cut point of BMI measuring for obese patients[6] or sex differences and even patients population.[2,20]
In addition, we examined the effect of CRP in obese patients who lost their weight ≥5% and who didn’t considerably lose their weight. Data showed these groups had significant differences in weight, BMI, FC, and LDL-C/HDL-C; however, other lipid profiles had no positive differences. Lavie proposed that CRP has a positive effect on weight reduction in obese patients with CAD.[19] Like our investigation, another study showed that patients who were successful in weight reduction had more improvement in obesity indexes, FC, and some lipid profiles than patients who weren’t successful in losing weight.[6] We can notify that significant weight reduction should be associated with increasing FC and fitness level in obese men with CAD. On the other hand, in relation to lipid profiles, more duration of exercise training and more attention to dietary restriction may be affect these patients and improve their lipid profiles.
Finally, according to our results and some other researches in this regard, we can state that CRP which was carried out by cardiac patients under supervision of physician and exercise physiologist plays an important role in management of obesity, FC, and lipid profiles in both obese and non-obese patients and both groups can similarly benefit from this program. Consequently, weight reduction may be caused greater improvement in FC and getting fitness levels through balance in lipid profiles in obese men with CAD. So, CRP is an acceptable organization for enhancement and maintenance of cardiovascular health through individualized programs and it should be noticed, high calorie expenditure exercise training combined with hypocaloric diet and even change in pharmacological treatment may be better consider to control risk factors in obese patients.
ACKNOWLEDGMENT
We thank Miss Yazdkhasti and all physicians and nurses and staffs in the Isfahan Cardiovascular Research Institute.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Eckel RH, York DA, Rössner S, Hubbard V, Caterson I, St Jeor ST, et al. American Heart Association. Prevention Conference 7: Obesity, a worldwide epidemic related to heart disease and stroke: Executive summary. Circulation. 2004;110:2968–75. doi: 10.1161/01.CIR.0000140086.88453.9A. [DOI] [PubMed] [Google Scholar]
- 2.Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX, et al. American Heart Association; Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Obesity and cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss: An update of the 1997 American Heart Association scientific statement on obesity and heart disease from the obesity committee of the council on nutrition, physical activity, and metabolism. Circulation. 2006;113:898–918. doi: 10.1161/CIRCULATIONAHA.106.171016. [DOI] [PubMed] [Google Scholar]
- 3.Gunstad J, Luyster F, Hughes J, Waechter D, Rosneck J, Josephson R. The effects of obesity on functional work capacity and quality of life in phase 2 cardiac rehabilitation. Prev Cardiol. 2007;10:64–7. doi: 10.1111/j.1520-037x.2007.05860.x. [DOI] [PubMed] [Google Scholar]
- 4.Al Orifan FH, Badr HE, Sabour Se’adah MA, Khadadah KE, Al Kordi B, Abass A. Obesity and cardiovascular risk factors in Kuwaiti adults. Kuwait Med J. 2007;39:162–6. [Google Scholar]
- 5.Lavie CJ, Milani RV. Obesity and cardiovascular disease: The hippocrates paradox? J Am Coll Cardiol. 2003;42:677–9. doi: 10.1016/s0735-1097(03)00784-8. [DOI] [PubMed] [Google Scholar]
- 6.Lavie CJ, Milani RV. Effects of cardiac rehabilitation, exercise training, and weight reduction on exercise capacity, coronary risk factors, behavioral characteristics, and quality of life in obese coronary patients. Am J Cardiol. 1997;79:397–401. doi: 10.1016/s0002-9149(97)89239-9. [DOI] [PubMed] [Google Scholar]
- 7.Ades PA, Savage PD, MS, Harvey-Berino J. The treatment of obesity in cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2010;30:289–98. doi: 10.1097/HCR.0b013e3181d6f9a8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thompson PD, Buchner D, Pina IL, Balady GJ, Williams MA, Marcus BH, et al. American Heart Association Council on Clinical Cardiology Subcommittee on Exercise, Rehabilitation, and Prevention; American Heart Association Council on Nutrition, Physical Activity, and Metabolism Subcommittee on Physical Activity. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: A statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity) Circulation. 2003;107:3109–16. doi: 10.1161/01.CIR.0000075572.40158.77. [DOI] [PubMed] [Google Scholar]
- 9.Steki Ghashghaei F, Taghian F, Najafian J, Marandi M, Ramezani MA, Moastafavi S, et al. Effect of cardiac rehabilitation on functional capacity of patients after cardiac surgery by assessing 6-minute walking test. ARYA Atheroscler. 2010;5:147–51. [Google Scholar]
- 10.Ghashghaei FE, Sadeghi M, Marandi SM, Ghashghaei SE. Exercise-based cardiac rehabilitation improves hemodynamic responses after coronary artery bypass graft surgery. ARYA Atheroscler. 2012;7:151–6. [PMC free article] [PubMed] [Google Scholar]
- 11.Lavie CJ, Milani RV. Benefits of cardiac rehabilitation and exercise training. Chest. 2000;117:5–7. doi: 10.1378/chest.117.1.5. [DOI] [PubMed] [Google Scholar]
- 12.Sarrafzadegan N, Rabiei K, Kabir A, Asgary S, Tavassoli A, Khosravi A, et al. Changes in lipid profile of patients referred to a cardiac rehabilitation program. Eur J Cardiovasc Prev Rehabil. 2008;15:467–72. doi: 10.1097/HJR.0b013e328300271f. [DOI] [PubMed] [Google Scholar]
- 13.Friedewald WT, Levy RI, Fridrikson DS. Estimation of concentrations of low-density lipoprotein cholesterol in plasma without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 14.Ades PA, Savage PD, Toth MJ, Harvey-Berino J, Schneider DJ, Bunn JY, et al. High-calorie-expenditure exercise: A new approach to cardiac rehabilitation for overweight coronary patients. Circulation. 2009;119:2671–8. doi: 10.1161/CIRCULATIONAHA.108.834184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Manzoni GM, Villa V, Compare A, Castelnuovo G, Nibbio F, Titon AM, et al. Short-term effects of a multidisciplinary cardiac rehabilitation programme on psychological well-being exercise capacity and weight in a sample of obese in-patients with coronary heart disease: A practice-level study. Psychol Health Med. 2011;16:178–89. doi: 10.1080/13548506.2010.542167. [DOI] [PubMed] [Google Scholar]
- 16.Kiat A, Cook E, Kiat H. Weight loss and fitness in patients with coronary artery disease through cardiac rehabilitation – A long term follow-up. Internet J Cardiovas Res. 2008;7:1. [Google Scholar]
- 17.Lavie CJ, Milani RV. Patients with high baseline exercise capacity benefit from cardiac rehabilitation and exercise training programs. Am Heart J. 1994;128:1105–9. doi: 10.1016/0002-8703(94)90740-4. [DOI] [PubMed] [Google Scholar]
- 18.Leon AS, Franklin BA, Costa F, Balady GJ, Berra KA, Stewart KJ, et al. Council on ClinicalCardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention); Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity); American association of Cardiovascular and Pulmonary Rehabilitation. Cardiac rehabilitation and secondary prevention of coronary heart disease. An American Heart Association scientific statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity), in collaboration with the American Association of Cardiovascular and Pulmonary Rehabilitation. Council on ClinicalCardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention); Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity); American association of Cardiovascular and Pulmonary Rehabilitation Cardiac rehabilitation and secondary prevention of coronary heart disease An American Heart Association scientific statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity), in collaboration with the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2005;111:369–76. doi: 10.1161/01.CIR.0000151788.08740.5C. [DOI] [PubMed] [Google Scholar]
- 19.Lavie CJ, Milani RV. Effects of cardiac rehabilitation and exercise training in obese patients with coronary artery disease. Chest. 1996;109:52–6. doi: 10.1378/chest.109.1.52. [DOI] [PubMed] [Google Scholar]
- 20.Shubair MM, Kodis J, McKelvie RS, Arthur HM, Sharma AM. Metabolic profile and exercise capacity outcomes: Their relationship to overweight and obesity in a Canadian cardiac rehabilitation setting. J Cardiopulm Rehabil. 2004;24:405–13. doi: 10.1097/00008483-200411000-00008. [DOI] [PubMed] [Google Scholar]
- 21.Savage PD, Ades PA. The obesity epidemic in the United States: Role of cardiac rehabilitation. Coron Artery Dis. 2006;17:227–31. doi: 10.1097/00019501-200605000-00004. [DOI] [PubMed] [Google Scholar]
- 22.Sadeghi M, Ghashghaei FE, Rabiei K, Roohafza H, Afshar H. Is there any difference between non-obese male and female in response to cardiac rehabilitation programs? J Res Med Sci. 2012;17:787–91. [PMC free article] [PubMed] [Google Scholar]
- 23.Lavie CJ, Milani RV. Effects of cardiac rehabilitation and exercise training on low-density lipoprotein cholesterol in patients with hypertriglyceridemia and coronary artery disease. Am J Cardiol. 1994;74:1192–5. doi: 10.1016/0002-9149(94)90546-0. [DOI] [PubMed] [Google Scholar]
- 24.Binder RK, Barth J, Schmid JP, Saner H. Burden of abdominal obesity in cardiac rehabilitation patients: Results from the Swiss CaRe study. Swiss Med Wkly. 2011;141:w13153. doi: 10.4414/smw.2011.13153. [DOI] [PubMed] [Google Scholar]