

Abstract
Introduction:
In this study, by using a problem-oriented approach in the needs assessment, identifying the defects and deficiencies in emergency health training centers has been determined as the basis for the requirements. The main objective of the study was the implementation of surgical emergencies integration of the five surgical groups (general surgery, urology, orthopedics, neurosurgery, and ENT) to meet the needs and determining its efficacy.
Materials and Methods:
This interventional study was conducted in three phases: (1) Phase I (design and planning): Needs assessment, recognition of implementation barriers and providing the objectives and training program for integrated emergencies. (2) Phase II (implementation): Justification of the main stakeholders of the project, preparation of students’ duties in the emergency department, preparation of on-duty plans, supervising the implementation of the program, and reviewing the plan in parallel with the implementation based on the problems. (3) Phase III (evaluation): Reviewing the evidences based on the amount of efficiency of the plan and justification for its continuation. In the first and the second phase, the data were collected through holding focus group meetings and interviews. In the third phase, the opened-reply and closed-reply researcher-made questionnaires were used. The questionnaire face and content validity were confirmed by experts and the reliability was assessed by calculating the Cronbach's alpha.
Results:
According to the views of the interns, assistants, teachers, and emergency personnel, the positive features of the plan included the following: Increasing the patients’ satisfaction, reducing the patients’ stay in the Emergency Department, increasing the speed of handling the patients, balancing the workloads of the interns, direct training of interns by young teachers of emergency medicine, giving the direct responsibility of the patient to the intern, practical and operational training of emergency issues, increasing the teamwork, facing a variety of patients, practicing the role of general practitioners, role-playing on a real patient's bedside, having a multilateral approach to the patient, reducing the wasting time on minor wards, balancing the work and rest schedules of the interns, and better learning and satisfaction of the interns. Over 60% of the participants believed the program has the following benefits: More attention on the training plan, improving the learning of patient management, being more responsive for the training of interns, increasing operational approach to emergency patients, being more aware of the performed actions, and increasing the quality and speed of services provided to patients. The mean score assigned to the whole questionnaire of investigating the viewpoints was 37.5 out of 50. The mean score of the interns’ questionnaire was significantly more than the mean score of the assistants.
Discussion:
The results obtained indicated that the greatest existing consensus about this plan was the positive impact on the learning of interns in the emergency setting. Thus, it will not only increase the number of patients who the interns are managing during the internship course, but also increases the balance of their workload and they can learn and manage the emergency patients with more leisure.
Keywords: Emergency medicine, internship, surgical emergency
INTRODUCTION
In recent years, most of the world's prestigious universities have attempted on improving the quality of educating the medical students in relation to emergency patients and the way of dealing with them. It is important to note that the objective of emergency training is not only for the practical training such as intravenous and nasogastric tube insertion, but instead, it is more important for the students to be familiar with the emergency knowledge and the scope of its application in dealing with emergency patients.[1] The nature of emergency patients is in such a way that the quick and lifesaving treatment requires not only clinical skills, but also challenges for the physician's personality and character. Increasing the contact with emergency patients and learning to make regular and systematic approach can reduce the stress and increase the quality of caring.[2] Clinical and educational settings are different for medical students in different medical schools. Therefore, in order to achieve the core skills in dealing with emergency patients and the core learning objectives in this area, a variety of opportunities should be given to the students for developing their professional skills. These opportunities should be provided to them during the pre-clinical and clinical years.[3] Management of acute illnesses and management of affected patients is an essential component of medical education based on the set of standards by the Liaison Committee on Medical Education. Medical training plans should provide educational opportunities for the students in a setting with multidisciplinary content.[4] There are countless opportunities to teach students in emergency from training at the bedside up to teaching emergency in the classrooms. There is also a wide range of knowledge, skills, and procedures that the teachers of emergency medicine are able to teach them.[5] Although it is always said to medical students that the emergency department is a good place to learn many skills and they can devote their spare time to learning important trainings in emergency medicine, most students without obtaining the desired results, are only immersed in emergency cases. Due to little control and direction, teaching and learning are very low.[6] Medical students in the 4th and the 5th years have experiences of history taking and physical examination, but do not have knowledge of making decisions in acute caring and efficient clinical attempts in emergency conditions.[7] In most medical schools, emergency medicine not only plays a role in the early years of medical education curriculum, but even in the years of clinical training, the main experiences of the students are in the specialty and sub-specialty fields that traditionally have been classified (surgical, women, internal, urology, pediatric.). These fields are in the main body of the educational program, and therefore, traditionally, the training of emergency medicine has not acquired priority in the educational programs.[7] Undoubtedly, the presence of the emergency medicine department in the emergency center and guiding the students learning in the emergency center will improve the quality of training in this setting. Teachers of emergency medicine are qualified to work in the chaotic environment of emergency center and by training; they are able to make skillful students in such environments.[5] Emergency medicine teachers can act as counselors in many areas of medicine. They have a wide perspective on patient care, patient-care systems, and they also have a lot of experience in different fields of medicine. Thus, these experiences allow them to be an effective advisor for the medical students.[7] International Federation for Emergency Medicine has established a committee consisting of specialists and physicians from all around the world to provide a curriculum that includes cores for teaching emergency medicine to medical students. The program includes some core objectives that all medical schools in the world should teach their students.[3] Evidence obtained upon searching the scientific literature indicates that the emergency medical training course, as a separate course or unit is not so old. For example, Australia had implemented the first emergency medical training as a separate course in 1997.[8] In 2007, only one-third of medical schools of the United States had mandatory emergency training courses in their internship. However, a standard curriculum was not provided for the course and they were mostly included in emergency shifts and sometimes lecture classes. Less than half of these schools in their programs had practical laboratory training of the emergency procedures.[9] In a study conducted in Canada in 2007, 10 of 14 schools of medicine, which had participated in the study, had a mandatory clinical rotation in emergency medicine.[10] In many studies, short-period courses have been used for education of knowledge and skills of emergency medicine.[11,12,13,14] For example, at the University of Witwatersrand in South Africa, they have designed a lesson block for emergency care training of medical students, named as the “acute and preoperative care.”[15] At Graz University in Australia, all of the students received a comprehensive education about emergency treatment of the acutely injured patients through lectures and exercises in an initial short-period course. The course was in fact a primitive conduction course designed to learn emergency medicine.[16] In a study conducted in 2006 at the hospital of the Holy Prophet Mohammad in Tehran, a 15-day course on emergency medicine was administered to the students. The interns had participated in theoretical and practical classes at the same time.[13] Fatehi et al. in the Isfahan University of Medical Sciences in 2002, in a course of 1-month duration in both theoretical and practical sections have trained the clinical course students in dealing with common emergencies, particularly the trauma emergency.[1] In two other studies, in an emergency course of 1-month duration, the required training was given to the students for emergency treatment in the elderly patients and it was evaluated at the end of the period.[17,18] Till et al. in their study have compared two courses. The first was a 4-week period of emergency medicine course, which was performed through problem-solving in small groups and seminars and training skills with direct supervision in the emergency department. The second one was a 9-week course in another university that was conducted by lectures and practices on simulators in addition to a 1-day practice on a simulated incident.[19] Within Iran, Iran and Mashad universities have added 1 or 2 month's emergency courses to their internship. The Shahid Beheshti University of Medical Sciences also proposed emergency courses at the end of Phase IV of the program in line with its reform program in general medicine in 2004. The emergency course was designed as a program with the aim of training the interns on handling clinical problems in emergency departments. After completion of their academic course, the students would have applied all of their knowledge and skills for the successful management of emergency patients in an academic environment and under supervision, extend their knowledge and experience in this field.[20]
The present study has been performed in the Isfahan University of Medical Sciences when it was at the verge of launching the emergency medicine group, while there was no such course in its general practitioner program. Therefore, a problem-based approach has been tried to be used for the needs assessment. Identification of the defects and deficiencies of training in emergency centers based on needs, implementation of the integrated surgical emergencies training, and afterwards the evaluation and determination of the impact of interventions on the quality of training and services in Al-Zahra hospital surgical emergency were the main features of this study.
MATERIALS AND METHODS
This study was an interventional study that was conducted in the Isfahan University of Medical Sciences. In fact, different parts of the study were designed and implemented consistent with the context, input, process, product evaluation model. This study was conducted in three phases. The first phase was included the assessment of the situation or context (context evaluation), and evaluation of the inputs (input evaluation). The second phase of the study was the evaluation of processing (process evaluation) and the third phase was to evaluate the product or output (product evaluation).
Phase I: Design and planning
Planning the program, recognition of implementation barriers and preparation of curriculum goals were performed in this phase. Some focus groups that participated at this stage of design and planning included the group managers, some of faculty members of the five surgical groups (general surgery, urology, orthopedics, neurosurgery, and ENT) and educational authorities of Al-Zahra Hospital of Isfahan Medical School. These groups discussed the problems in the internship program, the interns on emergency duties, the methods of interns’ training in the emergency department setting, and workflow management in the surgical emergency center. They investigated the current situation of surgical emergency centers and their problems. A researcher proposal for the integration of emergency training of the five surgery specialty departments was also suggested. The proposed plan was about the presence of the interns from the five surgery wards at the emergency department during their on-duties. The interns, regardless of the type of patients, manage the referred patients with the guidance and direct supervision of the emergency medicine teachers or in-charge emergency physicians. They could also use different specialties’ advice if needed. It is noteworthy that before the implementation of this plan, the interns of each group worked under the supervision of assistants in the emergency center and were only associated with the emergency patients of one of the five surgical fields.
In addition to bedside teaching in surgical-integrated emergencies, the classes should be conducted in accordance with the objectives, which were designed to teach emergency medicine and to increase the knowledge of interns in the field of emergency medicine. The second stage was to evaluate the efficacy rate and the feasibility of integrated emergency training plan. This was conducted through focus groups. The limits and obstacles were determined and appropriate methods were investigated to deal with them. In the third stage, the training objectives in surgical emergency were prepared by the cooperation of the masters and medical experts. Initially, the literatures were reviewed and the prepared lesson plans for the courses of emergency medicine in other medical schools inside and outside of the country were investigated. Then, in order to localize these objectives and develop them in accordance with the existing conditions in Iranian surgical emergency centers and approved headlines, the objectives were revised. In the fourth stage, the titles of curriculum topics (theoretical classes) of emergency medicine have been determined in order to cover the designated learning objectives. This stage was performed using focus group meetings. Necessary coordination was carried out to run this program (the required facilities for theoretical and practical training).
Phase II: Implementation
The following were performed in this phase: Justification of the project's main stakeholders, preparing the students’ duties in the emergency center, preparation of on-duty plans, supervising the implementation of the plan and reviewing the program in parallel with its implementation based on the problems. In the first stage of the second phase, the main involved stakeholders in the project were justified. The involved groups included the managers of the five surgical groups (general surgery, neurosurgery, ENT, urology, and orthopedics), assistants of the mentioned groups, the hospital's managers, EMS personnel, physicians, the emergency attending, and the interns’ representatives. This stage was performed through focus groups. These meetings were held in two stages, at the beginning of the implementation phase and then, five months after the start of the project, which was cited as the problem during implementation and the tailored solutions were adopted. Briefings were held with the five groups’ surgical assistants. These meetings were held at the beginning of the project and repeated for several times according to the requirements and during the implementation. The assistants were justified about the integrated surgical emergency training plan, their duties, and responsibilities in this plan. In the next stage of the second phase, the job descriptions of the emergency interns were prepared and compiled by the teachers of emergency medicine, emergency authorities. Interns’ rotation plan was also prepared for the emergency center. This stage was carried out in collaboration with teachers in emergency medicine and in-charge internship teachers in different surgical groups. During this phase, all of the interns who spent their emergency on-duties in all of the five surgical wards were enrolled with the intervention at Al-Zahra hospital based on the produced plan. During the implementation of the plan, a detailed monitoring program was carried out by the executors of the plan with the collaboration of emergency medicine teachers. The monitoring was performed through direct observation and process monitoring in Al-Zahra hospital emergency department time to time by the executors and interviews with various stakeholders of the program (EMS personnel, teachers, assistants, supervisors, interns, emergency physicians, and emergency medicine attending).
Phase III: Evaluation
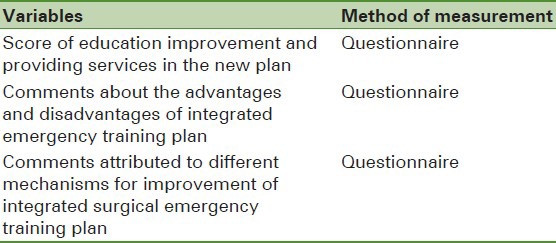
This phase was carried out in order to achieve evidences based on the rate of effectiveness of the plan and justification of its continuation. In fact, the second and the third phases of the plan were started at the same time. The fundamental variables in this evaluation are given in Table 1.
Table 1.
The fundamental variables in the evaluation and methods of measurement
-
(a)
Determining the relative mean score of education improvement and providing services in new plan than the old program:
The assessment tool in this section was a researcher-made questionnaire. It was used for determining the viewpoints of interns, assistants, and the emergency medicine teachers about the extent of recovery and existing problems in the surgical emergencies after the integrated surgical emergency training plan.
-
(b)
Determining the relative abundance of supporters and opponents with the advantages and disadvantages of the integrated surgical emergency training plan and determining the relative abundance of supporters and opponents with different solutions for improving this plan:
In order to clarify various aspects of the plan and its possible advantages and disadvantages, at first, by using an opened-reply questionnaire, the viewpoints of the interns, assistants, teachers and EMS staff were collected about the plan. Then, a questionnaire was developed based on these viewpoints about the advantages, disadvantages, and different approaches to improve the plan. The questionnaire was completed by the interns who had attended the emergency on-duties for at least five times.
The validity of the questionnaires was confirmed by the face and content validity. The questionnaire reliability was assessed by calculating Cronbach's alpha using the experts’ viewpoints and after conducting the pilot study. Descriptive statistics were used for data analysis of the evaluation phase (mean, standard deviation, variance, and frequency of agreed and completely agreed). T-test was used for the comparison of the questionnaire mean scores of the interns and assistants.
RESULTS
The results obtained from reviewing the viewpoints of surgical groups’ faculty members about the existing situation at the emergency center and the methods for training the interns in the surgical emergency center are listed below:
The existence of the problem in the emergency center workflow is due to the shortage in the total number of interns, the lack of active interns in the emergency center which consequently results in the increase of dissatisfaction in the involved groups
Several consultation requests with other services and repetitive tasks, ranging from the numerous history-taking up to the repeated orders
Lack of balance in the workloads of the emergency interns in the major and minor surgical wards (high volume of workload in general surgery and low volume in the minor wards) resulting in increased errors and reduction of learning in the surgical ward
Lack of a special trustee for intern training in the emergency center.
The results obtained from the explanation of the authorities’ comments about the viability of the integrated surgical emergency training plan and its potential subsequent barriers are listed below:
Evidences of the viability of the plan
Efficient use of the limited number of interns
Coping with the perspective of using an intern as a tool and as an individual for rewriting the patients’ orders, transferring the files, following-up the counseling, writing briefs, and not involving in the treatment of patients and consequently the good welcoming of interns from the plan
Having the approval of the majority of faculty members of the surgical group and hospital educational authorities, and therefore, the possibility of their intervention and management of arising challenges during the implementation.
Potential subsequent barriers of the plan
Lack of cooperation between the attending physician and the assistants of minor surgical groups
Potential problems in handling the ward-related issues due to the increased workload of the on-duty intern in the emergency center
The possibility of rejection of the viewpoints of the emergency medicine-attending physician by the assistants of surgical groups.
The results of the explanation of the comments of faculty members of emergency medicine and medical experts about surgical emergencies training purposes for the interns in the three fields were defined as follows:
Knowledge
To apply the necessary knowledge for providing the primary care in patients referred to the emergency department
To apply necessary knowledge at any time in the field of urgency of each patients’ conditions
To apply theoretical knowledge of primary care in patients referred to the emergency department at the level of a general practitioner.
Skills
To perform the basic life support (BLS) correctly
To perform advanced life support (ALS) correctly at the level of a general practitioner
Proper management of the patient until the time of determination and referral
Proper management of the patients with multiple traumas
To perform the required practical steps correctly for a general practitioner, these actions are required:
Infusions - venipuncture – urine catheterization - arterial puncture for ABG (arterial blood gas) analysis- nasogastric (NG) Tube insertion - suture handling - lumbar puncture (LP) - splint investment - gastric lavage - Thoracentesis - wound care and dressing – electrocardiogram (EKG) taking and interpretation- cardiac Monitoring – airway intubation - electrical shock - cardiac massage and oral airway insertion
To perform the required efforts to establish and maintain the airway correctly.
Attitude
To communicate properly with the patient and his entourage by applying the necessary communication skills
To communicate effectively with the emergency team members
To train the patient and his relatives properly in any situation, in accordance with the situation.
According to the determined objectives, it was decided to integrate the clinical skills into the training classes at the appropriate time by the teachers of emergency medicine (after launching the emergency medicine department). The clinical skills included the establishment and proper airway management, BLS skills, ALS skills at the level of GP, and skills in the care of patients with multiple traumas.
The results of the explanation of the teachers’ comments about the intern's duties in an emergency center are provided below:
All of the interns are obliged to get the patient's full history and carry out the necessary examinations before visiting the patients by emergency medicine teachers and assistants, and then introduce the patient to the emergency medicine teachers
The interns are required to follow up all of the diagnostic and prescribed therapeutic decisions for the patient and they should completely be aware of the patient's disease process
The interns are required to follow up the para-clinical tests, radiographic results, and other para-clinical measures of the patient. They should be informed of the results and record them in the patient's records
It is necessary for the interns to cooperate with the surgical services assistants, follow up their diagnostic and therapeutic orders, and participate in their training rounds
The intern should accompany the patient while being discharged from the hospital or being transferring to the ward by the coordinating with emergency medicine teachers
The intern is required to attend the training classes or rounds, which are being held at the time of his presence at the emergency center in coordination with emergency medicine teachers.
The results of the survey of the interns, assistants, teachers, and EMS personnel using an opened-reply questionnaire about the advantages and disadvantages of emergency intern plan are listed below:
Positive initiatives of the plan in the management of emergency department from the perspectives of interns, assistants, teachers, and EMS personnel
Increasing the patients’ satisfaction
Reducing the time of patients’ stay in the emergency center
Increasing speed of handling the patient
Creating a balance in the workloads of the different groups of interns from different departments
The existence of a specific trustee for each patient
Preventing working repeatedly and inappropriate ritualistic history-making
Following-up all of the patient's diagnostic and therapeutic needs by an intern
The existence of cohesion in the steps taken for the patient
Creating a specified order in the emergency caring
Establishing a calming atmosphere in the emergency center due to the reduction of the workload of the surgical assistants
Reducing miss-management
No need to do non-invasive and invasive actions without indications and act only according to the legal terms.
Positive and negative points of the integrated emergency training plan in the field of interns’ training from the perspectives of interns, assistants, teachers, and emergency personnel are:
Positive points
Direct training of interns by young teachers of emergency medicine
Rigorous and integrated training based on planning
Giving the responsibility to interns in concerning the patients
Operational and applied training of emergency topics
Direct contact of interns with the patients and performing actions such as writing the orders and treatment progress sheets
Carrying out the emergency procedures under the supervision of the attending physician
Holding training classes about the emergency topics by the clinical faculty members
Preventing inappropriate behaviors between the interns and assistants due to the determination of job description
Enhancing the team work
Dealing with various cases
Dealing with the patient as a whole
Preventing interns’ wasting of time in the minor section
Possibility to exercise the role of a general practitioner
Reducing the intern confusion among the commands of various services’ assistants
Possibility of role-playing at the real patient's bedside
Ability to exercise in having a multidimensional view of the patient
Balancing the workload of the interns and thus allowing better rest and providing better learning conditions
Decreasing routine orders and training of writing the orders for each particular patient
Using all of the opportunities of the intern in the emergency center in order to be trained more
Increasing the intern satisfaction and thus, better learning.
Negative points
Lack of necessary coordination between emergency medicine department and other departments
Lack of management and supervision tools from emergency medicine department for the surgical interns
Disruption in emergency duties during handling the patients of wards by interns
Disruption in ward duties during rush-hours in emergency center
Lack of the presence of specialty assistants in the training cycle of emergency
Reducing the visit of more specialized patients due to the reduction of attending in specialty clinics.
Interfering the training classes hours of other services with the working hours of the interns in the emergency center
Lack of regular presence of interns in the morning report.
The results of the survey using the self-made closed-reply questionnaire are listed below:
Among all the completed questionnaires for comparing the integrated emergency training plan with the previous trend, 56 questionnaires were analyzed. Twenty-eight cases (53.8%) were female, 24 (46.2%) were male and there were four subjects with unknown gender. Thirty questionnaires had been completed by interns, 16 questionnaires by the assistants of the five surgical departments and six questionnaires by the employed members of the surgical emergency center. Among the interns’ questionnaires, those who had at least five on-duties in emergency department were investigated.
The results of investigating the relative mean scores of training improvement and providing services in the integrated emergency training plan compared to the previous trend and advantages and disadvantages are given in Tables 2 to 6.
Table 2.
Results of reviewing the comments toward the rate of improvement of training and providing services in the integrated emergency training plan compared to previous trend
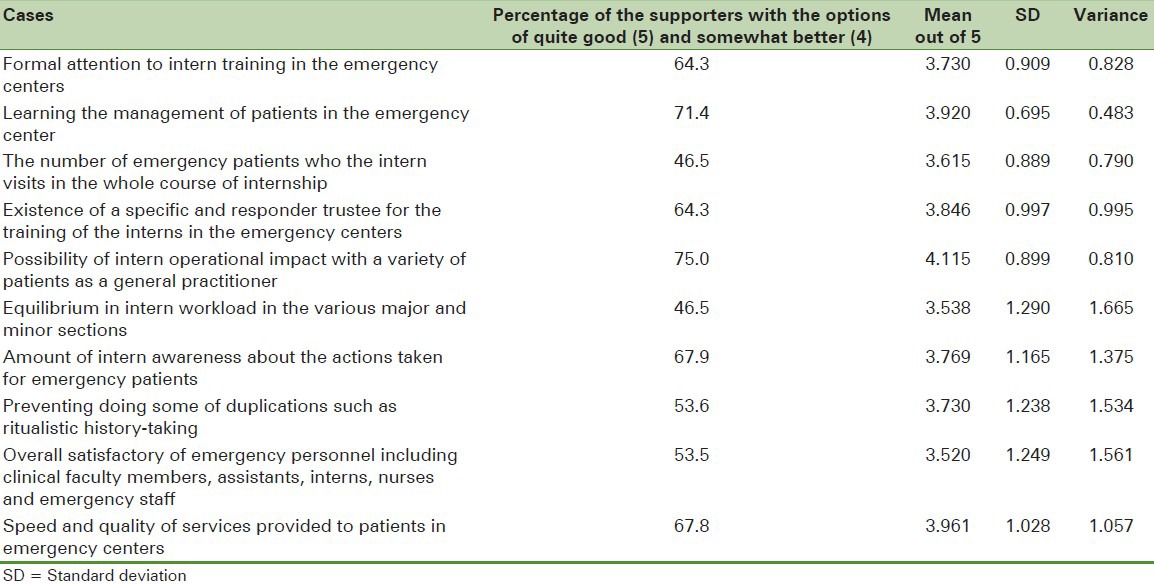
Table 6.
Comparison of the mean scores of interns and assistants from the survey questionnaire about the implementation of integrated emergency training plan and its advantages and disadvantages
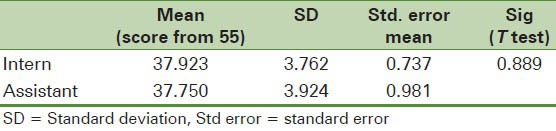
Table 3.
Mean score of the questionnaire for the evaluation of training improvement and providing services in the integrated emergency training plan compared to the previous trend

Table 4.
Comparison of the mean scores of the interns and assistants about the training improvement and providing services in the integrated emergency training plan compared to the previous trend

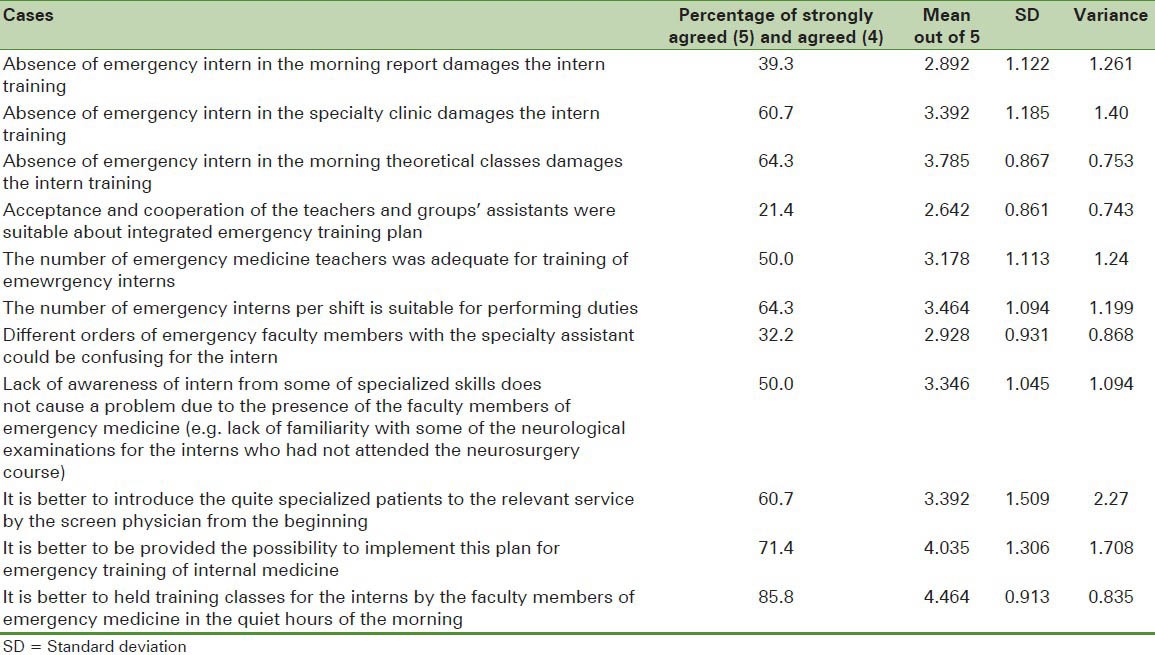
Table 5.
Results of the questionnaire (by using the Likert scale) related to the survey about the implementation of integrated emergency training plan and its advantages and disadvantages
DISCUSSION AND CONCLUSION
The first phase of this study was to identify the existing problems. Two main problems were identified. The first problem was the disorder in matters related to the patient and the other one was the disturbance in the training of the interns in the emergency department. It seems that the main factor of the problems raised in matters related to the patients was the lack of an emergency medicine department at the time of performing this part of this study. In this review, in total, there were references to two fundamental issues. One of them was the unbalanced workload of the intern and the high volume of his work in emergency center of some major departments and the other one was the lack of a trustee and planning for the training of the interns in this field. Therefore, the results of this study emphasized, the need of a systematic training for interns in the field of emergency medicine again. Fatehi has come to this conclusion in his study that the best place for training and gaining familiarity with common emergencies was the affiliated emergency departments of the universities of medical sciences. However, most of these trainings in this field did not follow a fundamental structure and codified systematic planning. The considered training in internal and surgical courses and the widely dispersed on duties during this period did not meet the students’ needs in the emergency medical field.[1] Johnson in his study concluded that the students in emergency rotations were involved with higher risks in activities such as initial assessment of the patient, differential diagnosis and decision-making. More likely, the possibility of performing the procedures would be provided for them.[21] Therefore, when a student is placed in such a useful training situation, it is necessary to plan systematically for these training opportunities to ensure the maximum productivity. If the different wards of EMS have a trustee for training and this trustee would be present continuously in this arena, definitely the interns would be receiving better training.
The next stage of the first phase, which was related to the evaluation of viability of the integration plan for surgical emergencies, the learning objectives of the interns after the integration and educational topics and titles had some results. Actually, these results provided the groundwork for the next phase. In this phase, the objectives that the interns were required to achieve upon completion of the rotation in the integrated surgical emergencies were found in three areas, i.e. knowledge, skills, and attitudes. The required training plan was determined. The results of this phase of the study were actually underlying to add a 1-month course of emergency medical applications to GP program. In fact, by the completion of the results of this phase, the required training plan was provided by the 1-month EMS course for the internship level. At the time of this research, only a few medical schools in Iran had EMS departments in their GP programs. Simultaneously, with the implementation of this plan, the program overview of GP training and the minimum expected completion of the capabilities of medical graduates in the universities of medical sciences in Iran were also undertaken by the General Medical Council. Within the approvals of this Secretariat, all medical universities were responsible for applying a department of emergency medicine, providing sufficient emergency medicine faculty members, and adding a course of 1-month internship in their emergency medicine program.[22] Therefore, the results of the first phase of this study provided the groundwork for the implementation of this approval in the Isfahan University of Medical Sciences. In the second phase, the duties of interns were assigned and the attending of the interns in the integrated surgical emergency training in Al-Zahra Hospital were planned too. Accordingly, the presence of the emergency intern and the method of dealing with the emergency medical team were determined in order to increase the efficiency and to facilitate better training of the interns. According to the results of the evaluation phase and regarding the viewpoints of the interns, assistants, faculty members, and emergency personnel, there were some positive features in the plan for the management of the emergency center. They included increasing the patient satisfaction, reducing the time of the patients, stay in the hospital, increasing the speed of handling the patients, balancing the workloads of the interns, and so on. However, there were some problems in the field of emergency management such as insufficient number of interns and problems occurred when the interns were needed to accompany the patient out of the hospital. On the other hand, the following were among the positive points that were raised: Direct training of the interns by young faculty members of emergency medicine, bringing the direct responsibility of the patients to interns, practical and operational training on emergency issues, increasing the teamwork, visiting a variety of cases, serving as a general practitioner, role playing at the bedside of the real patient, possibility to practice a multilateral approach to the patient, preventing wastage of time in the minor wards, balancing the work and rest of the interns, better learning, and increasing the satisfaction of the interns. The Matthew study about the integration of the objectives of emergency medicine in medical education curriculum concluded that the emergency medicine provided essential learning experiences for medical students and would have a positive impact on the quality and relevance of training with the future roles of every student.[7] Gallagher while investigating the results of establishment of the EMS department concluded that it was associated with significant quantitative and statistically improvements in faculty conditions and different specialties.[23] Among these, the problems that have been raised in the field of training the interns in this plan were mostly related to the lack of justification of the individuals. There were some disharmonies at the start of the plan in the various groups involved. The results of the scaling studies indicated that over 60% of the users of the plan believed in the following matters: Better attention to the training of interns, improving learning of patients’ management, being more responsive for the training of the interns, increasing the operational impact of intern with the emergency patients, having more information about the performed steps, and increasing the quality and speed of the services provided to the patients. These results indicated that the greatest existing consensus on this plan was its positive impact on the learning of the interns in the emergency setting. Although, the mean assigned score to the entire questionnaire of investigating the viewpoints regarding the rate of improvement was 37.5 out of 50. However, the mean questionnaire score of the interns was significantly higher than the mean score of the assistants. This would indicate greater satisfaction with interns compared to the assistants regarding the changes made by this plan. Anyhow, more than 60% of the survey participants believed that the absence of the emergency intern in specialized clinics and the morning theoretical classes could damage the training of the interns. In this regard, the majority of the participants were demanded to organize training classes by the department of emergency medicine in the morning hours. In a similar study conducted by Yeung et al. in 2010, the amount of the students’ perception was investigated from the new applications of emergency medicine for training of the students. In this 4-week rotation, they took advantages of different methods of teaching for the principles of emergency medicine. Working shifts in the emergency center and the workshops of enhanced cardiac and pulmonary resuscitation were among those, which were preferred more than the others were by the students.[24] Therefore, holding classes and workshops might be an appropriate method along with other methods for training in emergencies. Moreover, more than 70% of the participants requested about the implementation of the plan for the emergency training of internal medicine departments. It indicated their overall satisfaction of the implementation of an integrated surgical emergency training plan. In the event of implementing such a plan for the emergency training of internal medicine, the whole training of the interns in the field of emergencies would be provided by the EMS department. Emergency medicine is a young field with relatively young faculty members with no interest of dealing with the old training methods. They also have certain characteristics that are important for the recent changes in medical education. These are cases such as having a broad approach to patient care, emphasizing on basic clinical skills and availability within 24 h. In most of the clinical sites, the faculty members of emergency medicine manage the patient as a whole, but the experts and the internal and surgical sub-specialists do not look at the body as a whole and teach the diseases individually and in a specialized manner.[25] With regard to the requirement of launching the department of EMS, this plan provided the necessary background for the establishment of this department in various universities. The positive and distinguishing point of this plan was the fact that it was applicable without reducing the training time of the interns in the five surgical departments, without adding a separate course and even without the presence of EMS department. Therefore, it could be applied in most of medical schools of Iran. Another advantage compared to other plans was the attention to emergency medicine training in the internship course and not in a short-period course. This type of training would surely lead to better learning. On the other hand, this plan, besides giving a boost to the training of emergency medicine, would lead to a better handling of the emergency center.
LIMITATIONS
Some of the problems encountered in the implementation phase could be the following: Difficult access to the interns who have had sufficient numbers of on-duties, the low number of faculty members in emergency medicine, and lack of cooperation from assistants to complete the questionnaires (either due to the lack of time or because they disagreed with the plan, which caused an increase in responder bias). In the evaluation phase of this study, it was only focused on the survey of the people involved in this plan. We were unable to measure as an objective that the plan has had an impact on increasing the skills in students in dealing with emergencies due to the fact that the students enrolled in this plan were in different levels of their internship course. Following-up and access to every single one of them was very difficult after the internship course. In fact, this study was limited to one university and the results of other similar plans could be affected by other factors such as EMS management, combination of patients admitted to EMS, teachers, and previous learning experiences of the students. During the implementation of the plan, it was attempted to reduce the negative impacts of the pilot plan by continuous monitoring of the implementation method, removing the problems and obstacles, frequent justification of the people involved in the plan, rapid interventions when needed, and the training of the interns who attended this plan as the first group should not be overwhelmed by the problems that occurred until the establishment of the plan. This article was the result of a research project No. 289034 in the Research Center for medical education (Isfahan University of Medical Sciences).
Footnotes
Source of Support: This article was the result of a research project No. 289034 in the Research Center for medical education (Isfahan University of Medical Sciences)
Conflict of Interest: None declared
REFERENCES
- 1.Fatehi F, Ghassemi M, Sabouri M, Refaei E. Teaching Common Emergencies to Medical Students: An Experience. IJME. 2002;2:45–52. [Google Scholar]
- 2.Schull MJ, Ferrise LE, Tu JV, Hux JE, Redelmeier DA. Problems for clinical judgement: Thinking clearly in a emergency. CMAJ. 2001;164:1170–5. [PMC free article] [PubMed] [Google Scholar]
- 3.Hobgood C, Anantharaman V, Bandiera G, Cameron P, Halpern P, Holliman CJ, et al. ; International Federation for Emergency Medicine. International Federation for Emergency Medicine model curriculum for medical student education in emergency medicine. Int J Emerg Med. 2010;3:1–7. doi: 10.1007/s12245-009-0142-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liaison Committee on Medical Education (LCME). Functions and Structure of a Medical School. [Last accessed on 2011 Jul 17]. Available from: http://www.lcme.org/functions2010jun.pdf .
- 5.Coates WC. An educator's guide to teaching emergency medicine to medical students. Acad Emerg Med. 2004;11:300–6. doi: 10.1111/j.1553-2712.2004.tb02215.x. [DOI] [PubMed] [Google Scholar]
- 6.Kelly AM. What should medical student be taught in emergency medicine? Emerg Med. 1998;10:9–11. [Google Scholar]
- 7.Tews MC, Hamilton GC. Integrating emergency medicine principles and experience throughout the medical school curriculum: Why and how. Acad Emerg Med. 2011;18:1072–80. doi: 10.1111/j.1553-2712.2011.01168.x. [DOI] [PubMed] [Google Scholar]
- 8.Celenzo A, Jelink GA, Jacobs I, Kruk C, Graudone R, Murray L. Implementation and evaluation of an undergraduate emergency medicine curriculum. Emerg Med. 2001;13:98–103. doi: 10.1046/j.1442-2026.2001.00186.x. [DOI] [PubMed] [Google Scholar]
- 9.Wald DA, Manthey DE, Kruus L, Tripp M, Barrett J, Amoroso B. The state of the clerkship: A survey of emergency medicine clerkship directors. Acad Emerg Med. 2007;14:629–33. doi: 10.1197/j.aem.2007.02.035. [DOI] [PubMed] [Google Scholar]
- 10.Frank JR, Penciner R, Upadhye S, Nuth J, Lee AC. State of the nation: A profile of Canadian EM clerkships 2007 [abstract] CJEM. 2008;10:266. [Google Scholar]
- 11.Saxer T, Duperrex O, Vermeulen B, Vu Nu V. Emergency medicine training: A prospective, comparative study of undergraduate clinical clerkship and an army programme. Swiss Med Wkly. 2009;139:423–9. doi: 10.4414/smw.2009.12691. [DOI] [PubMed] [Google Scholar]
- 12.Harrison GA, Hillman KM, Fulde GW, Jacques TC. The need for undergraduate education in critical care. Results of a questionnaire to year 6 medical undergraduates, University of New South Wales and recommendations on a curriculum in critical care. Anaesth Intensive Care. 1999;27:314. doi: 10.1177/0310057X9902700111. [DOI] [PubMed] [Google Scholar]
- 13.Mahshidfar B, Kianmehr N, Mofidi M. Assessment of Emergency Medical Education on Knowledge Alterations of Medical Students in Rasoul Akram Hospital (2005-2006) J Qom Med Univ. 2007;1:31–8. [Google Scholar]
- 14.Thomas RE, Crutcher R, Lorenzetti D. A systematic review of the methodological quality and outcomes of RCTs to teach medical undergraduates surgical and emergency procedures. Can J Surg. 2007;50:278–90. [PMC free article] [PubMed] [Google Scholar]
- 15.MacFarlane C, Green-Thompson L. Medical student education in emergency medicine: New model from South Africa. Emerg Med Australas. 2006;18:276–81. doi: 10.1111/j.1742-6723.2006.00853.x. [DOI] [PubMed] [Google Scholar]
- 16.Prause G, Kröll W, Metzler H, Fuchs G, Kaloud H, Kaltenböck F, List WF. Education of the medical student in first aid, emergency and disaster medicine-the Graz model. Anasthesiol Intensivmed Notfallmed Schmerzther. 1995;30:236–9. doi: 10.1055/s-2007-996482. [DOI] [PubMed] [Google Scholar]
- 17.Tabas JA, Rosenson J, Price DD, Rohde D, Baird CH, Dhillon N. A comprehensive, Unembalmed cadaver- based course in advanced emergency procedures for medical students. Acad Emerg Med. 2005;12:782–5. doi: 10.1197/j.aem.2005.04.004. [DOI] [PubMed] [Google Scholar]
- 18.Shah MN, Heppard B, Medina-Walpole A, Clark NS, McCann R. Emergency medicine management of the geriatric patient: An educational program for medical students. J Am Geriatr Soc. 2005;53:141–4. doi: 10.1111/j.1532-5415.2005.53024.x. [DOI] [PubMed] [Google Scholar]
- 19.Saxer T, Duperrex O, Vermeulen B, Vu Nu V. Emergency medicine training: A prospective, comparative study of an undergraduate clinical clerkship and an army programme. Swiss Med Wkly. 2009;139:423–9. doi: 10.4414/smw.2009.12691. [DOI] [PubMed] [Google Scholar]
- 20.Yazdani SH, Hoseyni F, Homayooni Zand R. Tehran: Educational Development Center Shaheed Beheshti University of Medical Science and Health Services; 2007. Reform in General medical degree curriculum. Basic science phase. [Google Scholar]
- 21.Johnson GA, Pipas L, Newman-Palmer NB, Brown LH. The emergency medicine rotation: A unique experience for medical students. J Emerg Med. 2002;22:307–11. doi: 10.1016/s0736-4679(01)00497-8. [DOI] [PubMed] [Google Scholar]
- 22.Tehran: Vezarate behdasht darman va amoozeshe pezeshki; 2009. Vezarate behdasht darman va amoozeshe pezeshki moavenate amoozeshi va omoore daneshjooee dabeerkhaneye shoraye amoozeshe pezeshki omoomi [Mosavabeye 7; Barnameye amoozeshiye zaroori tebe organs dar maghtaea karvarzi] Persian. [Google Scholar]
- 23.Gallagher EJ, Henneman PL. Changes in academic attributes associated with establishment of departments of emergency medicine. Task Force on the Development of Emergency Medicine at Academic Medical Centers. Acad Emerg Med. 1998;5:1091–5. doi: 10.1111/j.1553-2712.1998.tb02668.x. [DOI] [PubMed] [Google Scholar]
- 24.Yeung M, Beecker J, Marks M, Nuth J, Weitzman B, Lee AC, Frank JR. A new emergency medicine clerkship program: Students’ perceptions of what works. CJEM. 2010;12:212–9. doi: 10.1017/s1481803500012264. [DOI] [PubMed] [Google Scholar]
- 25.Burdick WP. Emergency medicine's role in the education of medical students: Directions for change. Ann Emerg Med. 1991;20:688–91. doi: 10.1016/s0196-0644(05)82397-2. [DOI] [PubMed] [Google Scholar]