

Abstract
Peripheral neuropathy is a severe dose limiting toxicity associated with cancer chemotherapy. Ever since it was identified, the clear pathological mechanisms underlying chemotherapy induced peripheral neuropathy (CIPN) remain sparse and considerable involvement of oxidative stress and neuroinflammation has been realized recently. Despite the empirical use of antioxidants in the therapy of CIPN, the oxidative stress mediated neuronal damage in peripheral neuropathy is still debatable. The current review focuses on nerve damage due to oxidative stress and mitochondrial dysfunction as key pathogenic mechanisms involved in CIPN. Oxidative stress as a central mediator of apoptosis, neuroinflammation, metabolic disturbances and bioenergetic failure in neurons has been highlighted in this review along with a summary of research on dietary antioxidants and other nutraceuticals which have undergone prospective controlled clinical trials in patients undergoing chemotherapy.
Keywords: Chemotherapy, Mitochondria, Mitotoxicity, Nutraceuticals, Oxidative stress, Peripheral neuropathy
Graphical abstract
Targeting chemotherpay induced peripheral neuropathy with natural antioxidants.
Highlights
-
•
Oxidative stress contributes to the pathophysiology of chemotherapy induced peripheral neuropathies (CIPN).
-
•
Mitotoxicity and mitochondrial dysfunction contribute to amplified oxidative stress.
-
•
Pharmacological interventions targeted at maintenance of mitochondrial health and function may be beneficial against CIPN.
Introduction
Chemotherapy induced peripheral neuropathy (CIPN) remains one of the major limitations in oncology clinics due to increasing number of cancer patients, lack of effective treatment strategy, relapse of disease [1]. Around 30–40% of patients undergoing chemotherapy develop peripheral neuropathy and experience symptoms of pain and sensory disturbances [2]. According to National Cancer Institute (NCI), CIPN is one of the major reasons responsible for cessation of treatment, and hence is responsible for decreased chemotherapeutic efficacy and higher relapses [3]. Symptoms of peripheral nerve damage range from sensorimotor deficits (tingling sensation, burning pain in the arms, allodynia and hyperalgesia) to various functional deficits (impaired axonal transmission and reduced nutritive blood flow to nerves [4]). The most frequent agents causing CIPN are platinum compounds, taxane derivatives, vinca alkaloids, epothilones, thalidomide and bortezomib, which adversely affect the peripheral nervous system through dissimilar mechanisms summarized in Fig. 1 [5]. Although, the molecular pathomechanism and severity may vary with the inducing agent, physical damage to the neurons by chemotherapeutic agent is a common mechanism underlying the disease pathology [4]. The physical damage by chemotherapeutic drugs leads to functional impairment in neurons through oxidative stress, inflammation, apoptosis and electrophysiological disturbances. The scope of the present review is to present a basic idea on the possible role of oxidative stress and related pathomechanisms in CIPN based upon the existing experimental evidences.
Fig. 1.
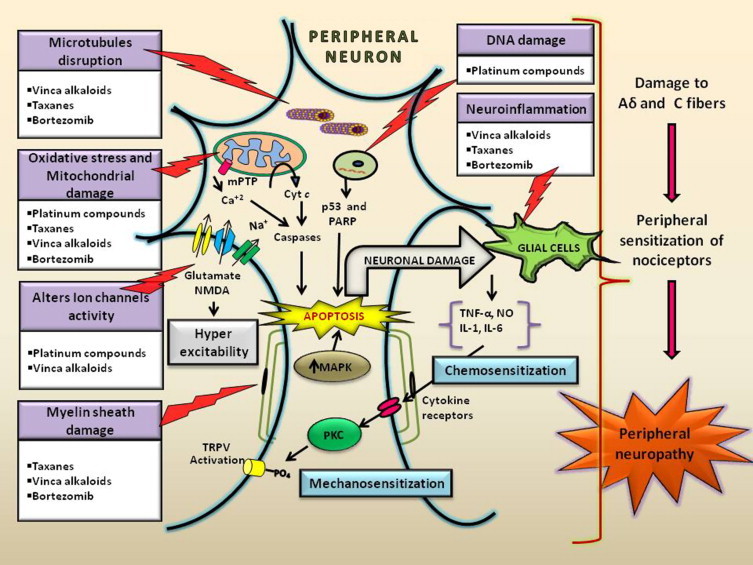
Pathobiology of peripheral neuropathy induced by several chemotherapeutic agents: peripheral nerve damage associated with taxanes, vinca alkaloids and bortezomib is characterized by various mechanisms like microtubular damage, mitochondrial dysfunction, neuronal apoptosis etc. [24]. Damage to the microtubules causes impairment in axonal transmission and mitochondrial dysfunction. The mitochondrial dysfunction is due to opening of mitochondrial permeability transition pore (mPTP), swollen and vacuolated mitochondria which brings Ca2+ deregulation and activation of caspases thus driving the neuronal cell towards apoptosis [34]. These changes consequently stimulate microglia cells which releases the proinflammatory mediators and growth factors to the damaged areas leading to peripheral sensitization thus causing spontaneous discharge and hyper excitability [3]. Further proinflammatory mediators are also capable of damaging myelin sheath [35]. Platinum compounds like cisplatin and oxaliplatin can affect mitochondrial DNA, leading to mitochondrial dysfunction and also induces neuronal apoptosis through activation of mitogen activated protein kinase (MAPK) pathway. These chemotherapeutic agents are also reported to cause peripheral sensitization by the up regulation of N-methyl D-aspartate (NMDA) receptors, transient receptor potential vanilloid (TRPV) channels, and protein kinase C (PKC) [34].Oxaliplatin also alters the Na+ channel conductance through chelation of Ca2+[36]. All these effects can damage the sensory neurons such as Aδ and C fibers, which leads to neuropathic pain characterized by hyperalgesia and allodynia.
Susceptibility of peripheral nervous system (PNS) to oxidative stress
It is a recognized fact that antineoplastic agents produce reactive oxygen species (ROS) to induce apoptosis in cancer cells [6]. However, ROS generated during chemotherapy may interfere with the normal cells and tissues and may be associated with the various toxic events like cardio toxicity, nephrotoxicity, neurotoxicity, etc. Certain structural and functional attributes of peripheral nervous system (PNS) make it more susceptible for accumulation of chemotherapeutics and some neurotoxins (Fig. 2) [5]. Lack of an efficient vascular barrier and absence of lymph drainage make the PNS more prone to toxic chemical insults. In addition mammalian nerves are known to be more susceptible to oxidative stress because of their high content of phospholipids, mitochondria rich axoplasm and also due to weak cellular antioxidant defences [7]. It has also been recently observed that structural and functional impairment caused by anti-cancer drugs enhances mitochondrial free radical production. Oxidative stress generated in this regard causes physical damage to neurons by demyelination, mitochondrial dysfunction, microtubular damage and apoptosis [8].
Fig. 2.
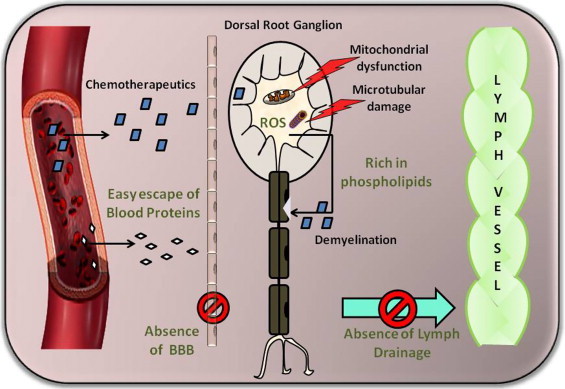
Susceptibility of peripheral nervous system (PNS) to chemotherapeutic insult and oxidative stress: structural architecture of peripheral sensory and motor neurons makes them more susceptible to drug induced nervous damage [5]. Dorsal root ganglion lacks an efficient vascular barrier and hence, drugs like chemotherapeutics and other neurotoxins can gain easy access to cell bodies of the sensory neurons. Unlike the central nervous system, the PNS doesn't have an analogy of blood brain barrier, and hence allows contact with some dangerous drug molecules, toxins and other blood proteins. Further, the absence of lymphatic system and cerebrospinal fluid around the peripheral nerves makes the potential dangerous substances to accumulate in the extracellular matrix around nervous tissue, which exacerbates the neuropathic damage [37]. Chemotherapeutics accumulate in this manner can cause oxidative stress in the neurons directly by forming DNA adducts or indirectly by mitochondrial impairment of electron transport chain [24]. Oxidative stress generated can cause nerve damage through microtubular disruption and or demyelination [14].
Role of oxidative stress in the neuronal damage and incidence of neuropathic pain
Although neurotoxicity caused by different classes of chemotherapeutic drugs differs to a significant extent, peripheral neuronal degeneration or small fiber neuropathy remains the end result of all CIPNs. It is been suspected that this might occur by a common mechanism i.e. increased neuronal oxidative stress as presented in Fig. 3. In fact, oxidative stress is identified to be responsible for the neuronal damage in different models of neuropathies such as diabetic neuropathy, acrylamide induced neuropathy and Charcot–Marie neuropathy [9], [10], [11], [12]. These observations laid the foundation for investigating possible involvement of oxidative stress in CIPN. Chemotherapy induced mitochondrial dysfunction and corresponding oxidative stress generation mediate the peripheral nerve damage. Oxidative stress mediated neurodegeneration can execute through bioenergetic failure, depletion of antioxidant defences, bio molecular damage, microtubular disruption, ion channel activation, demyelination, neuroinflammation, mitophagy impairment and neuronal death through apoptosis [13], [14], [15]. The redox imbalance produced in neuronal cells can be pharmacologically modulated through adjustment of nuclear erythroid factor-2 related factor and nuclear factor kappa light chain enhancer of B cells balance (Nrf2–NF-κB axis), and hence these modulators have been tested for their efficacy in animal models of peripheral neuropathy [16], [17]. An attempt has been made to test peroxynitrite scavengers, PARP inhibitors in animal models of CIPN, based on previous reports of their beneficial effect in diabetic neuropathy [18], [19]. Attenuation of symptoms of CIPN by the usage of peroxynitrite scavengers and PARP inhibitors further supports a role of nitrosative–oxidative stress in CIPN [15], [20].
Fig. 3.
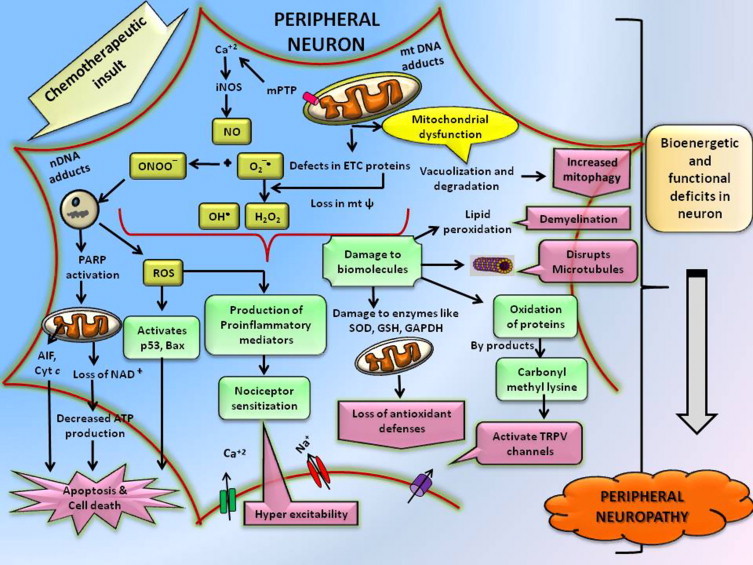
Role of oxidative stress in chemotherapy induced peripheral neuropathy (CIPN): the chemotherapeutic agents can form mitochondria DNA adducts and brings defects in electron transport chain proteins leading to mitochondrial dysfunction [13]. This is accompanied with an imbalance in the intracellular redox potential and elevation of reactive oxygen species especially superoxide. These major reactive species can elicit various alterations in peripheral neurons like redundant mitochondrial damage leading to apoptosis, inflammation and finally neurodegeneration. These reactive species are also reported to cause damage to bio molecules like phospholipids that result in demyelination, oxidation of proteins, releasing carbonyl bye products which can sensitize TRPV channels, inactivate antioxidant enzymes, and damage microtubules [14]. Nuclear DNA adducts and peroxynitrite creates strand breaks therefore activates PARP and p53, which forces the neuronal cell towards apoptosis [15]. Intracellular oxidative stress can also cause peripheral nociceptor sensitization by elevating the levels of proinflammatory mediators [3]. All these metabolic, bioenergetic and functional deficits in neuron lead to the development of peripheral neuropathic damage.
Mitochondrion: an emerging target in CIPN
Several prospective experimental studies in animal models suggested that mitochondrial dysfunction is associated with chemotherapy and axonal mitotoxicity contributes to neuropathic symptoms produced by various chemotherapeutic agents such as taxanes, vinca alkaloids, platinum compounds and bortezomib [21], [22], [23], [24], [25]. In fact histological and microscopic observation of peripheral nerve sections of chemotherapeutic drug treated animals showed swollen and vacuolated mitochondria. These features indicate neuronal apoptosis that may be through pathways like caspase activation and Ca2+ dysregulation. Paclitaxel induced apoptosis is mainly due to cytochrome c (Cyt c) release and Ca2+ dysregulation through the opening of mPTP of mitochondria [26], [27]. Frataxin deficiency, mt DNA damage, formation of defective electron transport chain (etc) components and loss in antioxidant defense enzymes has been demonstrated as mechanism for platinum compounds induced neuropathy [27]. Accumulation of dysfunctional mitochondria due to inefficient mitophagy further increases the free radical leakiness and this vicious cycle of oxidative damage to the bio molecules and mitochondria provides a feed-forward mechanism, that leads to further accumulation of ROS and RNS in the neurons during the development and progression of CIPN (Fig. 4). These experimental evidences clearly indicate that oxidative stress induced mitochondrial dysfunction is a central mediator of redox imbalance, apoptotic, autophagic and bioenergetic failure in peripheral neurons. It has also been widely observed that accumulation of oxidant damaged proteins and organelles due to inefficient autophagic pathway might be responsible for neurodegeneration, and hence therapeutic alleviation of Autophagy/Mitophagy is an unexplored potential target in peripheral neuropathies associated with nerve damage [28].
Fig. 4.
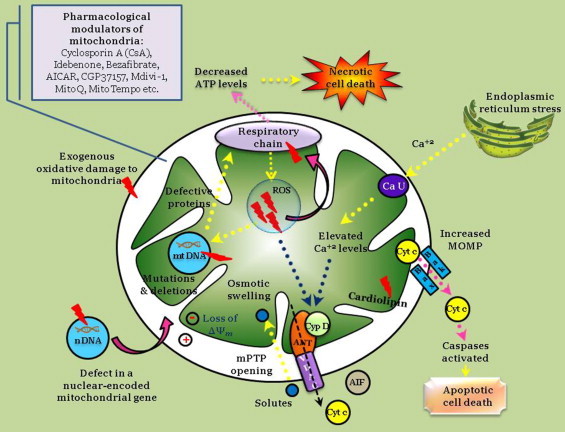
Mitochondrial dysfunction in CIPN and role of its pharmacological modulation: the common factors associated with oxidative stress induced mitochondrial dysfunction are disruption of calcium homeostasis, increased mitochondrial outer membrane permeability (MOMP), defective mitochondrial ATP synthesis, alteration in the mitochondrial membrane potential (↓ΔΨm), induction of mPTP, release of Cyt c (since it loose its binding ability by oxidative induced damage to the cardiolipin), mitochondrial swelling etc. [26]. All these steps occur together or one orchestrates with other and forms a vicious cycle which further disrupts mitochondrial function. This finally leads to the cell death via apoptosis or necrosis. Pharmacological manipulation of mitochondrial toxicity with mitochondria-targeted antioxidants could help us to get the better therapeutic outcome in CIPN through alleviation of mitochondria mediated oxidative stress [20], [27], [38].
Oxidative stress in CIPN: biomarkers and therapeutic strategies
Experimental evidences support the involvement of mitochondria mediated oxidative, nitrosative stress in development of peripheral nerve damage. Identification of these mechanisms might be helpful in identifying newer biomarkers for the CIPN and thus increases the chances of getting improved therapeutic strategies. Currently diagnosis is based mainly on clinical examination and electrophysiological changes to monitor CIPN, hence identification of newer disease pathomechanisms will be helpful in identifying new candidate biomarkers through which disease progression can be identified at an earlier stage [3]. Oxidative damage to peripheral neurons can cause damage to myelin sheath, mitochondrial proteins and other antioxidant enzymes. Hence, identification of levels of malondialdehyde, glutathione (GSH), superoxide dismutase (SOD) and activities of mitochondrial enzymes such as citrate synthase and ATP synthase can be helpful in monitoring the course of peripheral neuropathy and response of neuropathy to the treatment.
Due to the wide range of safety and tolerability, some of the dietary antioxidants and nutraceuticals have been tested for their clinical efficacy against chemotherapy induced peripheral neuropathy in large scale controlled clinical trials (Table 1). These agents were reported to have clinical utility by their protective action on neurons and they were found to alleviate functional disturbances of neurons by improving the mitochondrial function and physiology as shown in Fig. 5 [29], [30].
Table 1.
List of clinical studies conducted using nutraceuticals and dietary antioxidants in patients suffering from CIPN.
| S.no. | Model used | Treatment schedule | Parameters evaluated | Results observed | References |
|---|---|---|---|---|---|
| 1. | Paclitaxel/ cisplatin induced neuropathy in patients | N-acetyl carnitine oral (1 g t.i.d for 8 consecutive weeks) | Neurological examination, total neuropathic score (TNS) and quantitative sensory testing were measured. | Improvement in TNS, sensory symptoms and neurophysiology were observed in N-acetyl carnitine treated patients. | [29] |
| 2. | Cisplatin/ docetaxel induced neuropathy in patients | α-lipoic acid 600 mg i.v. once a week for 3–5 weeks followed by 1800 mg td p.o upto 6 months | Neurological examinations and WHO toxicity score assessment were evaluated | Improvement in neurological symptoms after treatment with α-lipoic acid. | [30] |
| 3. | Cisplatin induced neurotoxicity in women. | Glutathione (3 mg/m2) i.v every 3 weeks for six courses. | A questionnaire on the subjective symptoms of peripheral neuropathy and quality of life was assessed. | Decreased incidence of CINP in glutathione treated arm. | [39] |
| Oxaliplatin induced neuropathy in patients | GSH (1500 mg/m2 over a 15-min infusion period before oxaliplatin) | Electrophysiological parameters and assessment of neurological symptoms | Increased sural sensory nerve conduction velocity observed in GSH treated patients | [40] | |
| 4. | Paclitaxel/ docetaxel induced neuropathy in patients | Melatonin 21 mg daily at bedtime | Neurological examinations, toxicity assessment as per NCI-CTC 3.0 scale and FACT-Taxane quality of life questionnaire were evaluated. | FACT-Taxane quality of life end of study score was 137. Reduced incidence of neuropathy was observed in melatonin treated patients. | [41] |
| 5. | Oxaliplatin induced neuropathy in patients | Oral N-acetyl cysteine (1200 mg) (arm A) or placebo (arm B). | Electrophysiological parameters and assessment of neurological symptoms. | Improved NCV (nerve conduction velocity), CMAP (compound muscle action potential) and decreased SAP (sensory amplitude potential) were observed after N-acetyl cysteine treatment. | [42] |
| 6. | Paclitaxel induced peripheral neuropathy in patients | ω-3 fatty acids 640 mg t.i.d orally/placebo | Electrophysiological parameters and assessment of neurological symptoms. | Reduced total sensory neuropathy score, improved NCV after treatment with ω-3 fatty acids. | [43] |
| 7. | Oxaliplatin induced neuropathy in patients | Glutamine (15 g twice a day orally for seven consecutive days every 2 weeks starting on the day of oxaliplatin infusion) | Electrophysiological parameters and neurological symptoms were assessed | Lower percentage of grade 1–2 peripheral neuropathy after 2 cycles and lower incidence of grade 3, 4 neuropathy after 4–6 cycles of glutamine administration was observed. | [44] |
| 8. | Taxanes, platinum compounds and combination drug induced neuropathy in patients. | Twice daily dosing of vitamin E (400 mg)/ placebo. | The outcome was evaluated using the common terminology criteria for adverse events (CTCAE v 3.0) and A questionnaire on the subjective symptoms of peripheral neuropathy. | Significant difference in the incidence of sensory neuropathy between the two arms was not observed. | [46] |
| Vitamin E did not appear to reduce the incidence of sensory neuropathy. | |||||
| Cisplatin induced neurotoxicity in patients | vitamin E (300/day mg/placebo) | The outcome was evaluated by measuring total neuropathic score (TNS) and quantitative sensory testing | Vitamin E reduced the incidence of sensory neuropathy | [47], [48] | |
Fig. 5.
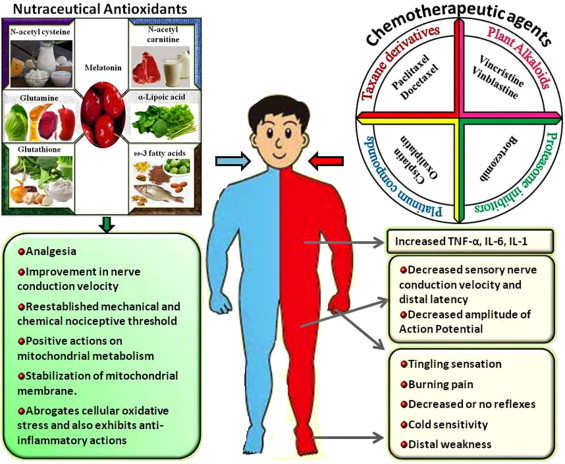
Role of nutraceutical antioxidants in the treatment of chemotherapy induced peripheral neuropathy (CIPN): nutraceutical antioxidants exhibited significant neuroprotection towards chemotherapy induced neurotoxicity by decreasing cellular oxidative stress through their inherent free radical scavenging property (glutathione [39], [40], melatonin [41], n-acetyl cysteine [42], ω-3 fatty acids [43], α-lipoic acid [30] etc) and indirectly by increasing whole blood concentrations of antioxidant enzymes (glutamine [44], n-acetyl cysteine [42]), normalizing mitochondrial functions (n-acetyl carnitine [29], α-lipoic acid [30]), attenuating the production of proinflammatory mediators (ω-3 fatty acids [43]) etc. Totally these nutraceutical antioxidants normalize the cellular functions, rescue mitochondrial impairment, inhibit neuronal inflammation, apoptosis and therefore diminish the sensory nerve degeneration [2], [45].
Despite their wide usage and clinical efficacy, the available antioxidants present so far could only provide mild to moderate pain relief in peripheral neuropathy [31]. Failure of antioxidants in clinical trials might be due to their inability to reverse established oxidative damage, radical specificity and interference with physiological redox signaling pathways [28]. Targeted delivery of antioxidants and employing the mechanism based approach, clinical pathology and concentration dependent dosage schedule in antioxidant trials will help us to develop better understanding and might help us in devising newer strategies in CIPN [32]. Another possible explanation of translational failures of these trials are the common toxicity criteria (CTC) assessment scales used in CIPN trials, which should be remodified to include necessary parametric measures, that will ensure accurate quantification of the drug induced effect [33].
Summary
This review highlighted the possible involvement of oxidative stress as a vital pathogenic mechanism of CIPN. Molecular insight into oxidant induced neuronal damage can probe a chance of getting an alternative therapy for CIPN in the form of natural phyto antioxidants or synthetic radical traps. Further, identification of antioxidant molecules having pleiotropic activity on other pathophysiological pathways involved in the CIPN could aid in the development of improved therapies. Since mitochondria are found to be a primary source of cellular ROS, pharmacological interventions targeted at maintenance of mitochondrial health and function is an alternative therapeutic approach for CIPN over direct scavengers of free radicals for the treatment of CIPN.
Footnotes
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial-No Derivative Works License, which permits non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- 1.Ferrier J., Pereira V., Busserolles J., Authier N., Balayssac D. Emerging trends in understanding chemotherapy-induced peripheral neuropathy. Current Pain and Headache Reports. 2013;17:364–371. doi: 10.1007/s11916-013-0364-5. [DOI] [PubMed] [Google Scholar]
- 2.Wolf S., Barton D., Kottschade L., Grothey A., Loprinzi C. Chemotherapy-induced peripheral neuropathy: prevention and treatment strategies. Eur. J. Cancer. 2008;44:1507–1515. doi: 10.1016/j.ejca.2008.04.018. [DOI] [PubMed] [Google Scholar]
- 3.Wang X.-M., Lehky T.J., Brell J.M., Dorsey S.G. Discovering cytokines as targets for chemotherapy-induced painful peripheral neuropathy. Cytokine. 2012;59:3–9. doi: 10.1016/j.cyto.2012.03.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brzezinski K. Chemotherapy-induced polyneuropathy. Part I. Pathophysiology. Contemp. Oncol. (Poznań, Poland) 2012;16:72–80. doi: 10.5114/wo.2012.27341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Argyriou A.A., Bruna J., Marmiroli P., Cavaletti G. Chemotherapy-induced peripheral neurotoxicity (CIPN): an update. Crit. Rev. Oncol./Hematol. 2012;82:51–77. doi: 10.1016/j.critrevonc.2011.04.012. [DOI] [PubMed] [Google Scholar]
- 6.Conklin K.A. Chemotherapy-associated oxidative stress: impact on chemotherapeutic effectiveness. Integr. Cancer Ther. 2004;3:294–300. doi: 10.1177/1534735404270335. [DOI] [PubMed] [Google Scholar]
- 7.Low P.A., Nickander K.K., Tritschler H.J. The roles of oxidative stress and antioxidant treatment in experimental diabetic neuropathy. Diabetes. 1997;46:S38–S42. doi: 10.2337/diab.46.2.s38. [DOI] [PubMed] [Google Scholar]
- 8.Xiao W.H., Bennett G.J. Effects of mitochondrial poisons on the neuropathic pain produced by the chemotherapeutic agents, paclitaxel and oxaliplatin. Pain. 2012;153:704–709. doi: 10.1016/j.pain.2011.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Negi G., Kumar A., Joshi R.P., Sharma S.S. Oxidative stress and Nrf2 in the pathophysiology of diabetic neuropathy: old perspective with a new angle. Biochem. Biophys. Res. Commun. 2011;408:1–5. doi: 10.1016/j.bbrc.2011.03.087. [DOI] [PubMed] [Google Scholar]
- 10.Negi G., Kumar A., Sharma S.S. Melatonin modulates neuroinflammation and oxidative stress in experimental diabetic neuropathy: effects on NF-kB and Nrf2 cascades. J. Pineal Res. 2011;50:124–131. doi: 10.1111/j.1600-079X.2010.00821.x. [DOI] [PubMed] [Google Scholar]
- 11.Prasad S.N., Muralidhara Neuroprotective effect of geraniol and curcumin in an acrylamide model of neurotoxicity in Drosophila melanogaster: relevance to neuropathy. J. Insect Physiol. 2013;60:7–16. doi: 10.1016/j.jinsphys.2013.10.003. [DOI] [PubMed] [Google Scholar]
- 12.Saifi G.M., Szigeti K., Snipes G.J., Garcia C.A., Lupski J.R. Molecular mechanisms, diagnosis, and rational approaches to management of and therapy for Charcot–Marie–Tooth disease and related peripheral neuropathies. J. Investig. Med.: Off. Publ. Am. Fed. Clin. Res. 2003;51:261–283. doi: 10.1136/jim-51-05-14. [DOI] [PubMed] [Google Scholar]
- 13.McDonald E.S., Windebank A.J. Cisplatin-induced apoptosis of DRG neurons involves bax redistribution and cytochrome c release but not fas receptor signaling. Neurobiol. Dis. 2002;9:220–233. doi: 10.1006/nbdi.2001.0468. [DOI] [PubMed] [Google Scholar]
- 14.Salvemini D., Little J.W., Doyle T., Neumann W.L. Roles of reactive oxygen and nitrogen species in pain. Free Radic. Biol. Med. 2011;51:951–966. doi: 10.1016/j.freeradbiomed.2011.01.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ta L.E., Schmelzer J.D., Bieber A.J., Loprinzi C.L., Sieck G.C., Brederson J.D., Low P.A., Windebank A.J. A novel and selective poly (ADP-ribose) polymerase inhibitor ameliorates chemotherapy-induced painful neuropathy. PloS One. 2013;8:e54161. doi: 10.1371/journal.pone.0054161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ganesh Yerra V., Negi G., Sharma S.S., Kumar A. Potential therapeutic effects of the simultaneous targeting of the Nrf2 and NF-kB pathways in diabetic neuropathy. Redox Biol. 2013;1:394–397. doi: 10.1016/j.redox.2013.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Negi G., Kumar A., Sharma S. S. Nrf2 and NF-kB modulation by sulforaphane counteracts multiple manifestations of diabetic neuropathy in rats and high glucose-induced changes. Curr. Neurovasc. Res. 2011;8:294–304. doi: 10.2174/156720211798120972. [DOI] [PubMed] [Google Scholar]
- 18.Lupachyk S., Shevalye H., Maksimchyk Y., Drel V.R., Obrosova I.G. PARP inhibition alleviates diabetes-induced systemic oxidative stress and neural tissue 4-hydroxynonenal adduct accumulation: correlation with peripheral nerve function. Free Radic. Biol. Med. 2011;50:1400–1409. doi: 10.1016/j.freeradbiomed.2011.01.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Negi G., Kumar A., Sharma S.S. Concurrent targeting of nitrosative stress & PARP pathway corrects functional, behavioral and biochemical deficits in experimental diabetic neuropathy. Biochem. Biophys. Res. Commun. 2010;391:102–106. doi: 10.1016/j.bbrc.2009.11.010. [DOI] [PubMed] [Google Scholar]
- 20.Janes K., Doyle T., Bryant L., Esposito E., Cuzzocrea S., Ryerse J., Bennett G.J., Salvemini D. Bioenergetic deficits in peripheral nerve sensory axons during chemotherapy-induced neuropathic pain resulting from peroxynitrite-mediated post-translational nitration of mitochondrial superoxide dismutase. Pain. 2013;154:2432–2440. doi: 10.1016/j.pain.2013.07.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jin H.W., Flatters S.J.L., Xiao W.H., Mulhern H.L., Bennett G.J. Prevention of paclitaxel-evoked painful peripheral neuropathy by acetyl-L-carnitine: effects on axonal mitochondria, sensory nerve fiber terminal arbors, and cutaneous Langerhans cells. Exp. Neurol. 2008;210:229–237. doi: 10.1016/j.expneurol.2007.11.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Podratz J.L., Knight A.M., Ta L.E., Staff N.P., Gass J.M., Genelin K., Schlattau A., Lathroum L., Windebank A.J. Cisplatin induced mitochondrial DNA damage in dorsal root ganglion neurons. Neurobiol. Dis. 2011;41:661–668. doi: 10.1016/j.nbd.2010.11.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zheng H., Xiao W.H., Bennett G.J. Mitotoxicity and bortezomib-induced chronic painful peripheral neuropathy. Exp. Neurol. 2012;238:225–234. doi: 10.1016/j.expneurol.2012.08.023. [DOI] [PubMed] [Google Scholar]
- 24.Zheng H., Xiao W.H., Bennett G.J. Functional deficits in peripheral nerve mitochondria in rats with paclitaxel-and oxaliplatin-evoked painful peripheral neuropathy. Exp. Neurol. 2011;232:154–161. doi: 10.1016/j.expneurol.2011.08.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Xiao W.H., Zheng H., Zheng F.Y., Nuydens R., Meert T.F., Bennett G.J. Mitochondrial abnormality in sensory, but not motor, axons in paclitaxel-evoked painful peripheral neuropathy in the rat. Neuroscience. 2011;199:461–469. doi: 10.1016/j.neuroscience.2011.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Flatters S.J.L., Bennett G.J. Studies of peripheral sensory nerves in paclitaxel-induced painful peripheral neuropathy: evidence for mitochondrial dysfunction. Pain. 2006;122:245–257. doi: 10.1016/j.pain.2006.01.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Melli G., Taiana M., Camozzi F., Triolo D., Podini P., Quattrini A., Taroni F., Lauria G. Alpha-lipoic acid prevents mitochondrial damage and neurotoxicity in experimental chemotherapy neuropathy. Exp. Neurol. 2008;214:276–284. doi: 10.1016/j.expneurol.2008.08.013. [DOI] [PubMed] [Google Scholar]
- 28.Giordano S., Darley-Usmar V., Zhang J. Autophagy as an essential cellular antioxidant pathway in neurodegenerative disease. Redox Biol. 2013;2 doi: 10.1016/j.redox.2013.12.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bianchi G., Vitali G., Caraceni A., Ravaglia S., Capri G., Cundari S., Zanna C., Gianni L. Symptomatic and neurophysiological responses of paclitaxel-or cisplatin-induced neuropathy to oral acetyl-L-carnitine. Eur. J. Cancer. 2005;41:1746–1750. doi: 10.1016/j.ejca.2005.04.028. [DOI] [PubMed] [Google Scholar]
- 30.Gedlicka C., Kornek G.V., Schmid K., Scheithauer W. Amelioration of docetaxel/cisplatin induced polyneuropathy by α-lipoic acid. Ann. Oncol. 2003;14:339–340. doi: 10.1093/annonc/mdg051. [DOI] [PubMed] [Google Scholar]
- 31.Schloss J.M., Colosimo M., Airey C., Masci P., Linnane A.W., Vitetta L. Nutraceuticals and chemotherapy induced peripheral neuropathy (CIPN): a systematic review. Clin. Nutr. 2013;32:888–893. doi: 10.1016/j.clnu.2013.04.007. [DOI] [PubMed] [Google Scholar]
- 32.Kamat C.D., Gadal S., Mhatre M., Williamson K.S., Pye Q.N., Hensley K. Antioxidants in central nervous system diseases: preclinical promise and translational challenges. J. Alzheimers Dis. 2008;15:473–493. doi: 10.3233/jad-2008-15314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cavaletti G., Frigeni B., Lanzani F., Mattavelli L., Susani E., Alberti P., Cortinovis D., Bidoli P. Chemotherapy-induced peripheral neurotoxicity assessment: a critical revision of the currently available tools. Eur. J. Cancer. 2010;46:479–494. doi: 10.1016/j.ejca.2009.12.008. [DOI] [PubMed] [Google Scholar]
- 34.Jaggi A.S., Singh N. Mechanisms in cancer–chemotherapeutic drugs-induced peripheral neuropathy. Toxicology. 2012;291:1–9. doi: 10.1016/j.tox.2011.10.019. [DOI] [PubMed] [Google Scholar]
- 35.Scripture C.D., Figg W.D., Sparreboom A. Peripheral neuropathy induced by paclitaxel: recent insights and future perspectives. Curr. Neuropharmacol. 2006;4:165–172. doi: 10.2174/157015906776359568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Argyriou A.A., Polychronopoulos P., Iconomou G., Chroni E., Kalofonos H.P. A review on oxaliplatin-induced peripheral nerve damage. Cancer Treat. Rev. 2008;34:368–377. doi: 10.1016/j.ctrv.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 37.Jain K.K. In: Drug-Induced Neurological Disorders. Jain K.K., editor. Hogrefe & Huber; 2001. Drug-induced peripheral neuropathies; pp. 263–294. [Google Scholar]
- 38.Smith R.A.J., Hartley R.C., Cocheme H.M., Murphy M.P. Mitochondrial pharmacology. Trends Pharmacol. Sci. 2012;33:341–352. doi: 10.1016/j.tips.2012.03.010. [DOI] [PubMed] [Google Scholar]
- 39.Smyth J.F., Bowman A., Perren T., Wilkinson P., Prescott R.J., Quinn K.J., Tedeschi M. Glutathione reduces the toxicity and improves quality of life of women diagnosed with ovarian cancer treated with cisplatin: results of a double-blind, randomised trial. Ann. Oncol. 1997;8:569–573. doi: 10.1023/a:1008211226339. [DOI] [PubMed] [Google Scholar]
- 40.Cascinu S., Catalano V., Cordella L., Labianca R., Giordani P., Baldelli A.M., Beretta G.D., Ubiali E., Catalano G. Neuroprotective effect of reduced glutathione on oxaliplatin-based chemotherapy in advanced colorectal cancer: a randomized, double-blind, placebo-controlled trial. J. Clin. Oncol. 2002;20:3478–3483. doi: 10.1200/JCO.2002.07.061. [DOI] [PubMed] [Google Scholar]
- 41.Nahleh Z., Pruemer J., Lafollette J., Sweany S. Melatonin, a promising role in taxane-related neuropathy. Clin. Med. Insights: Oncol. 2010;4:35–41. doi: 10.4137/cmo.s4132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Lin P.-C., Lee M.-Y., Wang W.-S., Yen C.-C., Chao T.-C., Hsiao L.-T., Yang M.-H., Chen P.-M., Lin K.-P., Chiou T.-J. N-acetylcysteine has neuroprotective effects against oxaliplatin-based adjuvant chemotherapy in colon cancer patients: preliminary data. Support. Care Cancer. 2006;14:484–487. doi: 10.1007/s00520-006-0018-9. [DOI] [PubMed] [Google Scholar]
- 43.Ghoreishi Z., Esfahani A., Djazayeri A., Djalali M., Golestan B., Ayromlou H., Hashemzade S., Jafarabadi M.A., Montazeri V., Keshavarz S.A. Omega-3 fatty acids are protective against paclitaxel-induced peripheral neuropathy: a randomized double-blind placebo controlled trial. BMC Cancer. 2012;12:1–8. doi: 10.1186/1471-2407-12-355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Wang W.-S., Lin J.-K., Lin T.-C., Chen W.-S., Jiang J.-K., Wang H.-S., Chiou T.-J., Liu J.-H., Yen C.-C., Chen P.-M. Oral glutamine is effective for preventing oxaliplatin-induced neuropathy in colorectal cancer patients. Oncologist. 2007;12:312–319. doi: 10.1634/theoncologist.12-3-312. [DOI] [PubMed] [Google Scholar]
- 45.Visovsky C., Collins M., Abbott L., Aschenbrenner J., Hart C. Putting evidence into practice: evidence-based interventions for chemotherapy-induced peripheral neuropathy. Clin. J. Oncol. Nurs. 2007;11:901–913. doi: 10.1188/07.CJON.901-913. [DOI] [PubMed] [Google Scholar]
- 46.Kottschade L.A., Sloan J.A., Mazurczak M.A., Johnson D.B., Murphy B.P., Rowland K.M., Smith D.A., Berg A.R., Stella P.J., Loprinzi C.L. The use of vitamin E for the prevention of chemotherapy-induced peripheral neuropathy: results of a randomized phase III clinical trial. Support. Care Cancer. 2011;19:1769–1777. doi: 10.1007/s00520-010-1018-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Pace A., Savarese A., Picardo M., Maresca V., Pacetti U., Del Monte G., Biroccio A., Leonetti C., Jandolo B., Cognetti F. Neuroprotective effect of vitamin E supplementation in patients treated with cisplatin chemotherapy. J. Clin. Oncol. 2003;21:927–931. doi: 10.1200/JCO.2003.05.139. [DOI] [PubMed] [Google Scholar]
- 48.Pace A., Giannarelli D., Galia E., Savarese A., Carpano S., Della Giulia M., Pozzi A., Silvani A., Gaviani P., Scaioli V. Vitamin E neuroprotection for cisplatin neuropathy A randomized, placebo-controlled trial. Neurology. 2010;74:762–766. doi: 10.1212/WNL.0b013e3181d5279e. [DOI] [PubMed] [Google Scholar]