

Abstract
Objective To examine the risk of postoperative meningitis following expanded endoscopic endonasal skull base (EESB) surgery.
Setting A systematic analysis of publications identified through searches of the electronic databases from Embase (1980–July 17, 2012), Medline (1950–July 17, 2012), and references of review articles.
Main Outcome Measures Incidence of meningitis following EESB surgery.
Results A total of 2,444 manuscripts were selected initially, and full-text analysis produced 67 studies with extractable data. Fifty-two contained data regarding the frequency of postoperative meningitis. The overall risk of postoperative meningitis following EESB surgery was 1.8% (36 of 2,005). For those reporting a cerebrospinal fluid (CSF) leak, meningitis occurred in 13.0% (35 of 269). For those not reporting a CSF leak, meningitis occurred in 0.1% (1 of 1,736). The odds ratio for the development of meningitis in the presence of a postoperative CSF leak was 91.99 (95% confidence interval, 11.72–721.88; p < 0.01). There was no difference in reported incidence of meningitis or CSF leak between anterior and posterior cranial fossa surgery. There was one reported case of meningitis-related mortality following EESB surgery.
Conclusion The evidence in skull base surgery is limited. This study demonstrates a low incidence of meningitis (1.8%) following EESB procedures. The incidence of meningitis from EESB surgery without an associated CSF leak is uncommon.
Keywords: systematic review, endoscopy, endonasal, skull base, meningitis, CSF rhinorrhea
Introduction
Advancements in endoscopic endonasal skull base (EESB) surgery continue to evolve with increasing surgical complexity.1 2 3 4 5 6 7 8 9 10 The establishment of the endonasal route enables access and visualization to the ventral cranial base through the narrowest practical corridor with minimal trauma to surrounding tissue. Within anatomical limitations, the degree of tumor resection and vascular manipulation is often considered comparable with conventional microsurgical skull base techniques.9 10 11 12 13 14 15 16 17 18 19 20 21
Major concerns following an EESB surgery, however, are the risk of cerebrospinal fluid (CSF) rhinorrhea and meningitis. Much improvement has been made with the development of vascularized mucosal flaps to aid in the reconstruction of the skull base after EESB surgery.7 22 23 These endoscopic reconstructions not only provide a reliable separation of the cranial and sinonasal cavity but are robust over time.24 A recent systematic review demonstrated that the rate of CSF leak after true intradural EESB was 15.6% (representing 51 of 326 patients) with free graft techniques and 6.7% with vascularized flap reconstructions (representing 19 of 283 patients).7 This is comparable with open craniofacial surgery,25 but questions still arise due to the inability to formally provide a sterile field and connection with the upper aerodigestive tract.
Skull base pathologies are uncommon, and thus the published evidence base is limited to centers with small numbers. Establishing the frequency of complications from small populations is challenging. The aim of this study was to review critically and systematically the data available on the perioperative outcomes of published case series, cohorts, and case-control studies for endoscopic endonasal approaches to various cranial base pathologies. The primary outcome measure was to identify the incidence of meningitis following an intradural EESB procedure and to correlate this with the reported incidence of postoperative CSF leak rates. The secondary outcome measure was to establish if a difference in the risk of meningitis exists following EESB surgery to the anterior cranial fossa (ACF) versus a posterior cranial fossa (PCF) approach.
Methods
A systematic review of published literature was performed for the primary outcome of postoperative meningitis following endoscopic skull base surgery. A Preferred Reporting Items for Systematic Reviews and Meta-analysis (www.prisma-statement.org) style was adhered to where possible, but quality assessment was not performed because the target study type was case series and cohorts.
Eligibility Criteria
Published manuscripts in English were eligible. Case series, case-control studies, cohort studies, and randomized controlled trials were included. Only manuscripts reporting original data on patients undergoing endoscopic endonasal transcranial surgery were eligible, including those with any intervention for the treatment of specific pathologies, such as meningioma, craniopharyngioma, skull base metastasis, chordoma, and chondrosarcoma where a transcranial transdural approach would be required. Because this review is of large skull base defects, outcomes of patients undergoing simple closure of CSF fistulae or encephaloceles and transellar approaches for pituitary or intrasellar lesions were excluded because the vast majority of these defects were relatively small. Only studies where an endonasal craniotomy was created as part of a procedure were included. Trials that included subjects of any age, with any comorbidity, and with varied duration of follow-up were included. Local and regional flap reconstructions of endonasal skull base surgery series were included.
Search Criteria
The Medline database was searched from 1950 to July 17, 2012, and the Embase database was searched from 1980 to July 17, 2012. The Cochrane Collaboration database and the National Health Service Evidence Health Information Resources Web site were also searched. The bibliographies of identified manuscripts were reviewed for additional data sources. No unpublished trials were included. We designed a search strategy to include manuscripts relevant to any aspect of endoscopic skull base surgery and skull base reconstruction. Table 1 shows the search strategy used for Embase and Medline databases.
Table 1. Medline search strategy (similar modified version used in Embase).
| 1. exp Cranial Fossa, Anterior/in, pa, su [Pathology, Surgery] or anterior cranial fossa.mp. |
| 2. exp Cranial Fossa, Middle/in, pa, su [Pathology, Surgery] or middle cranial fossa.mp. |
| 3. exp Cranial Fossa, Posterior/in, pa, su [Pathology, Surgery] or posterior cranial fossa.mp. |
| 4. exp Sella Turcica/in, pa, su [Pathology, Surgery] or Sella Turcica.mp. |
| 5. exp Skull Base Neoplasms/co, pa, su [Complications, Pathology, Surgery] or skull base neoplasm$.mp |
| 6. exp Skull Base/in, pa, su [Pathology, Surgery] or skull base.mp. |
| 7. or 1–6 |
| 8. exp Endoscopy/ae, co [Adverse Effects, Complications] or endoscop$.mp. |
| 9. exp Neuroendoscopy/ae [Adverse Effects] or neuroendoscop$.mp. |
| 10. (transethm$ or transsphen$ or transcliv$ or transplan$).mp. |
| 11. (trans-ethm$ or trans-sphen$ or trans-cliv$ or trans-plan$).mp. |
| 12. (transnas$ or trans-nas$ or endonas$ or endosin$).mp. |
| 13. (endoscopic endonas$ or expanded endoscopic endonas$).mp |
| 14. exp Craniotomy/ae, su [Adverse Effects, Surgery] or craniotomy.mp. |
| 15. craniectomy.mp. |
| 16. exp Dura Mater/su [Surgery] |
| 17. exp Surgical Procedures, Minimally Invasive/ae [Adverse Effects] or Surgical Procedures, Minimally Invasive.mp. |
| 18. |
| 19. or 8–17 |
| 20. exp Meningitis/co, su [Complications, Surgery] or meningitis.mp. |
| 21. exp Cerebrospinal Fluid Rhinorrhea/co, su [Complications, Surgery] or cerebrospinal fluid rhinorrhea.mp. |
| 22. exp postoperative complication/ |
| 23. exp Treatment Outcome/ or treatment outcome.mp. |
| 24. or 19–22 |
| 25. 7 and 18 and 23 |
| 26. Limit 24 to English language |
Two authors (LTL and ST) selected the studies in an unblinded standardized manner once the searches were completed. The publications extracted were grouped by title; duplicates were excluded. The abstracts were then reviewed to ascertain whether they met the inclusion and exclusion criteria as previously described.
Data Extraction
Standardized data sheets were used for each study. The primary outcomes were recorded as the presence or absence of reporting on postoperative CSF leak and meningitis events. Secondary analysis of this outcome focused on the dichotomization of data for anterior cranial fossa (via a transcribiform or a transplanum route) and posterior cranial fossa surgeries (via a transclival route) to establish if a difference exists in the rate of meningitis following these two types of endonasal approaches. For each group, the number of patients, the type of approach, pathology, and perioperative morbidity relevant to the skull base surgery was recorded. The large range of methods, study aims, and pathologies were reported qualitatively in the data. Studies were deemed suitable for inclusion only if they documented the presence or absence of postoperative meningitis following EESB surgery or explicitly stated that patients had no further adverse events other than that reported. Where duplicate publication was anticipated from centers republishing updated reports on their EESB experience over time,26 27 28 29 30 31 32 33 the most recent or largest published data were included for analysis in the current study.
Statistical Analysis
Statistical assessments were performed primarily with descriptive data. Case-by-case analysis was performed for summary data. Comparison of proportions for small numbers was performed with a Fisher exact test; where appropriate, significance was set to a probability value of 0.05. Logistic regression analysis was used to calculate the odds ratio (OR) in predicting the likelihood of meningitis. Assessment of different pathologies was performed as nominal data and analyzed using SPSS software v.19 (SPSS, Inc., Chicago, IL).
Results
Literature Review Results
The search of Embase and Medline produced a total of 2,429 studies written in English. Additional records identified through bibliographic and referencing resources yielded a further 15 studies that were included in the analysis, totaling 2,444 studies. After exclusion of duplicates, 1,985 studies remained. A title search found 293 articles on skull base surgery. Those studies captured in the search that described simple CSF leak repairs (n = 49; 16.7%), repairs for encephaloceles (n = 14; 4.8%), and microscopic skull base series (n = 59; 20.1%) were excluded from the analysis. This selection process is outlined in Fig. 1.
Fig. 1.
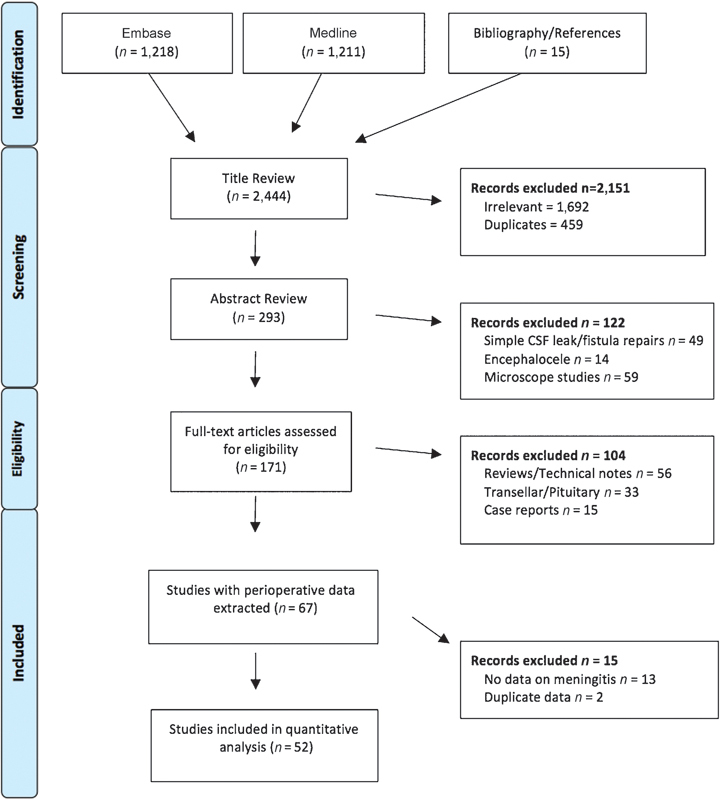
Article selection process from the Embase and Medline database searches. CSF, cerebrospinal fluid.
The remaining 171 articles describing EESB surgery were subjected to full-text assessment. Of these, 56 (32.7%) were reviews of endoscopic or endonasal techniques, 33 (19.3%) were pituitary series utilizing the transellar approach, and 15 (8.8%) were simple case reports. These simple case report studies were excluded due to strong publication bias.
Perioperative outcomes were recorded for 67 EESB studies. An additional 15 studies were excluded due to duplicity of data (n = 2) and nonextractable outcomes for meningitis (n = 13). Fifty-two studies with reports of posttreatment meningitis were included in the final analysis (Table 2).
Table 2. Characteristics of included studies.
| Study | Study period | EESB cases | Age, y (SD or range) | Female, % | CSF leak,% | Meningitis, % | Mortality related to meningitis, % |
|---|---|---|---|---|---|---|---|
| Batra et al2 | 1995–2003 | 9 | 55 (26–77) | 33 | 11 | 0 | 0 |
| Solares et al32 | 2000–2004 | 6 | 50 (29–66) | 33 | 0 | 0 | 0 |
| Carrau et al26 | NR | 20 | NR | 55 | 15 | 5 | 0 |
| Frank et al61 | 1998–2005 | 11 | 59.4 (32–76) | 55 | 0 | 0 | 0 |
| Frank et al5 | 1998–2005 | 10 | 41.5 (11–61) | 60 | 30 | 10 | 0 |
| Leong et al34 | 2000–2005 | 10 | 57.4 (26–84) | 60 | 0 | 20 | 0 |
| Cavallo et al35 | 2004–2006 | 16 | NR | NR | 13 | 0 | 0 |
| Dave et al36 | 1997–2006 | 19 | 61.6 (39–81) | 42 | 0 | 0 | 0 |
| de Divitiis et al37 | 2005–2006 | 6 | 56.1 (44–77) | 50 | 17 | 0 | 0 |
| Santos Rde et al38 | 2001–2005 | 8 | 47.6 (9–79) | NR | 25 | 25 | 0 |
| Fortes et al62 | NR | 3 | 54 (51–57) | 67 | 67 | 0 | 0 |
| Kassam et al74 | 2000–2005 | 18 | 13.5 (3–18) | 72 | 6 | 0 | 0 |
| Laufer et al39 | NR | 10 | 54 (38–73) | NR | 10 | 0 | 0 |
| Cappabianca et al75 | 2004–2006 | 24 | 47.3 | 83 | 13 | 4 | 0 |
| Carrabba et al63 | 2005–2008 | 17 | 48.0 | 41 | 24 | 0 | 0 |
| de Divitiis et al40 | 1983–2006 | 7 | NR | NR | 29 | 0 | 0 |
| de Divitiis et al41 | 2004–2007 | 11 | 55.3 (35–80) | 64 | 27 | 0 | 0 |
| Dehdashti et al4 | 2005–2007 | 12 | 49.4 (22–77) | 33 | 33 | 0 | 0 |
| El-Banhawy et al42 | 1997–2006 | 10 | NR | NR | 0 | 0 | 0 |
| El-Sayed et al43 | 2006–2007 | 20 | 52 (18–56) | 75 | 0 | 0 | 0 |
| Gardner et al44 | 1999–2006 | 16 | 55 (36–80) | 38 | 69 | 0 | 0 |
| Gardner et al31 | 2002–2005 | 35 | 55 (39–79) | 83 | 40 | 0 | 0 |
| Kassam et al29 | 2006–2007 | 48 | 47 (4–80) | 58 | 17 | 0 | 0 |
| Kassam et al28 | NR | 10 | 44.4 (16–78) | 30 | 50 | 0 | 0 |
| Leng et al76 | 2005–2007 | 10 | NR | NR | 0 | 0 | 0 |
| Nicolai et al45 | 1996–2006 | 134 | 58.7 (4–85) | 50 | 3 | 1 | 0 |
| Stamm et al46 | 2000–2007 | 7 | 23.4 (16.3) | 14 | 29 | 0 | 0 |
| Zhang et al64 | 2002–2006 | 9 | 35 (14–63) | 44 | 0 | 0 | 0 |
| Arbolay et al1 | 2006–2007 | 5 | 41.4 (25–60) | 20 | 0 | 20 | 20 |
| Cavallo et al47 | 2004–2008 | 22 | 49.4 (18–80) | 32 | 14 | 0 | 0 |
| Cohen et al48 | 2000–2006 | 18 | 53 (19–91) | 50 | 17 | 0 | 0 |
| Dehdashti et al3 | 2005–2007 | 19 | 44 (20–78) | 37 | 21 | 5 | 0 |
| Eloy et al49 | 1997–2006 | 18 | 61.2 (39–81) | 44 | 6 | 0 | 0 |
| Fatemi et al50 | 2000–2008 | 14 | 45 (8–79) | 57 | 36 | 0 | 0 |
| Folbe et al51 | 1994–2006 | 16 | 56.6 (15–79) | 44 | 25 | 0 | 0 |
| Harvey et al22 | 2007–2008 | 22 | 45.5 (20.2) | 59 | 5 | 0 | 0 |
| Liu and Di52 | 2004–2008 | 10 | 38.4 (20–58) | 50 | 10 | 0 | 0 |
| Stippler et al33 | 2003–2007 | 20 | 44.4 (4–76) | 40 | 25 | 0 | 0 |
| Vergez et al53 | 1994–2008 | 17 | 68 (44–82) | 12 | 0 | 6 | 0 |
| Batra et al54 | 2000–2008 | 31 | 57.5 (14–84) | 42 | 6 | 3 | 0 |
| Fraser et al77 | NR | 17 | 52.4 (22–87) | 35 | 6 | 6 | 0 |
| Greenfield et al55 | 2004–2009 | 43 | 55.4 (17–85) | 63 | 7 | 0 | 0 |
| Horiguchi et al78 | 2005–2009 | 19 | 55.9 (20–79) | 63 | 26 | 0 | NR |
| Jane et al56 | 2005–2009 | 12 | 50.8 (29–76) | 58 | 0 | 8 | NR |
| Madhok et al57 | 1998–2008 | 35 | 34 (12–67) | NR | 0 | 0 | 0 |
| Nyquist et al79 | 2008–2008 | 5 | 56.4 (31–72) | 60 | 0 | 0 | 0 |
| Prevedello et al30 | NR | 2 | 44.5 (42–47) | 0 | 0 | 0 | 0 |
| Villaret et al58 | 1996–2008 | 62 | 61.7 (25–84) | 29 | 13 | 0 | 0 |
| Gallia et al59 | 2005–2010 | 8 | 56.9 (44–72) | 38 | 0 | 0 | 0 |
| Kono et al69 | 1998–2008 | 1000 | 49 (18.0) | 50 | 14 | 2 | 0 |
| Kurschel et al80 | 2004–2009 | 58 | 39.9 (4–78) | 50 | 10 | 7 | 0 |
| Carta et al60 | 2000–2009 | 16 | 59.0 | NR | 6 | 0 | 0 |
Abbreviations: EESB, expanded endoscopic endonasal skull base; NR, not reported; SD, standard deviation.
EESB patients were defined by true intracranial surgery with dural resection.
Primary Outcome: Overall Risk of Meningitis following Expanded EESB Surgery
Quantitative analysis revealed a total of 2,363 patients, of which 2,005 were considered to have undergone an expanded EESB surgery. An attempt was made to exclude from the analysis all patients with pituitary adenomas in which a transellar approach was used. The mean age was 49.8 years (range: 3–91 years) and the mean follow-up was 21.8 months (range: 0.2–152 months). Of the studies that report on sex, females accounted for 49.8% of the cases (943 of 1,893).
The overall incidence of postoperative meningitis following EESB surgery was 1.8% (36 of 2,005). Of the total population, 269 experienced a postoperative CSF leak (Table 3). This was represented as a 13.0% (35 of 269) risk of meningitis for those patients with CSF leak compared with 0.1% (1 of 1,736) for non-CSF leak cases (chi-square = 221.64; p < 0.01). Overall, the odds of developing meningitis in the presence of a postoperative CSF leak following an EESB procedure were 91.99 (95% confidence interval [CI], 11.72 to 721.88; p < 0.01).
Table 3. Risk of meningitis following expanded endoscopic endonasal skull base surgery.
| Overall meningitis risk | Meningitis with associated postoperative CSF leak | Meningitis with no associated postoperative CSF leak | p value | |
|---|---|---|---|---|
| All studies (n = 52) | 1.8% (36/2,005) | 13.0% (35/269) | 0.1% (1/1,736) | < 0.01 |
| EESB to the anterior cranial base studies (n = 32) | 1.7% (11/664) | 13.3% (10/75) | 0.2% (1/589) | < 0.00 |
| EESB studies to the posterior cranial base (n = 9) | 1.0% (1/97) | 6.3% (1/16) | 0% (0/81) | < 0.00 |
Abbreviations: EESB, expanded endoscopic endonasal skull base; SD, standard deviation; CSF, cerebrospinal fluid.
One death related to postoperative meningitis was reported in a 42-year-old man following an endoscopic transsphenoidal supradiaphragmatic resection of a hypothalamic astrocytoma.1 This patient underwent an uneventful subtotal resection of the tumor but experienced postoperative meningitis and died 2 weeks following surgery.
Secondary Outcome: Subgroup Analysis for Risk of Meningitis following Expanded EESB surgeries to the Anterior Cranial versus Posterior Cranial Fossae
Thirty-two studies described the endoscopic endonasal transcribiform or transplanum approach to the anterior skull base.2 5 26 28 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 Of these 32 studies, 664 patients were considered to have undergone expanded EESB surgery of the ACF. The mean age was 51.9 years (range: 4–91 years), and the mean follow-up was 26.3 months (range: 0.8–152 months). Sinonasal malignancies with transcranial extension was accounted for in 409 cases (61.6%), craniopharyngioma in 112 cases (16.9%), meningioma in 66 cases (9.9%), Rathke cleft cyst in 43 cases (6.5%), chordoma in 7 cases (1.1%), metastasis in 5 cases (0.8%), glioma in 1 case (0.2%), and chondrosarcoma in 1 case (0.2%).
The risk of postoperative meningitis following EESB surgery to the ACF was 1.7% (11 of 664) and an 11.3% (75 of 664) CSF leak rate. The odds of developing postoperative meningitis among the ACF cases with a postoperative CSF leak were 90.46 (95% CI, 11.40–717.99; p < 0.01). In contrast, only 1 patient experienced meningitis (0.2%) among the 589 patients with no postoperative CSF leak.
Nine studies described the endonasal transclival approach to the PCF in 97 patients with a mean age of 48.6 years (range: 4–87 years).4 30 32 33 61 62 63 64 65 There were 39 females (40.2%), and the mean follow-up was 14.9 months (range: 0.2–69 months). Chordoma was accounted for in 73 cases (75.3%), chondrosarcoma in 5 cases (5.2%), metastasis in 2 cases (2.1%), meningioma in 2 cases (2.1%), sinonasal malignancy with posterior cranial fossa extension in 1 case (1.3%), and vascular in 1 case (1.3%).
The risk of meningitis following an EESB approach to the PCF was 1.0% (1 of 97) and a 16.5% (16 of 97) CSF leak rate. There were no reported meningitis cases in the 81 patients with no postoperative CSF leak, and therefore no OR was calculated. However, the presence of a postoperative CSF leak was significantly associated with the development of meningitis (chi-square: 5.12; p = 0.02).
Overall, no differences between ACF and PCF outcomes were seen. The incidences of meningitis following an expanded EESB surgery to the ACF and PCF were similar, 1.7% (1 of 97) and 1.0% (1 of 97), respectively (chi-square: = 0.21; p = 0.64). The incidences of postoperative CSF leak following an EESB surgery to the ACF was 11.3% (75 of 664) and 16.5% (16 of 97) to the PCF (chi-square: 2.17; p = 0.14).
Discussion
In the past decade, the application of EESB surgery to midline cranial base pathologies has been established through various cadaveric and clinical studies.9 10 21 66 67 68 The rapid expansion of this technique, however, carries with it a particular concern for the infectious ramifications of operating through the “clean-contaminated” field of the sinonasal cavities.69 Problems with closure of the dura mater and prevention of CSF leaks remain a challenge and a significant source of postoperative morbidity following an endoscopic transnasal craniotomy.
In the current study, a systematic analysis of the literature was performed to establish the incidence of meningitis following expanded EESB surgery. Our results indicated an overall 1.8% risk of postoperative meningitis. The risk, however, was not substantially different for an endoscopic endonasal approach to the anterior cranial base (1.7%) or a posterior cranial base (1.0%) (p = 0.64). These rates are comparable with conventional transcranial or transfacial surgical approaches that harbor a reported infectious risk ranging from 0.9 to 2.5%.70 71 Mortality related to meningitis was reported in 1 patient among the 36 reported cases of postoperative meningitis following an EESB procedure.1
As expected, the presence of postoperative CSF leak was associated with subsequent meningitis (OR: 91.99; 95% CI, 11.72–721.88; p < 0.01). In a large retrospective series of 1000 endoscopic skull base patients treated at the University of Pittsburgh, Kono and colleagues identified several risk factors for subsequent meningitis.69 Included among the factors that were recognized to predispose to meningitis were male sex, a history of prior craniotomy or endonasal surgery, the presence of ventriculoperitoneal shunt or an external ventricular drain at the time of surgery, and higher complexity intradural surgeries. The presence of a postoperative CSF leak was, not surprisingly, considered by many as an important factor in predisposing to the subsequent development of meningitis. The incidence of meningitis without an associated CSF, as demonstrated in this study, was very low (0.1% [1 of 1,736]).
Although it is considered that endonasal surgery to the PCF is associated with a higher risk of both CSF leak and meningitis, the data presented in this study demonstrate no difference across 761 patients in which a comparison of approach could be made. Over the past few years, the application of multilayer reconstructions and the routine use of vascularized mucosal flaps in expanded endonasal surgery have drastically decreased the risk of postoperative CSF complications and meningitis.72 73 Harvey and colleagues reported a 0.9% risk of subsequent intracranial complication with a delayed CSF leak rate of 1.9% in 106 endoscopic skull base repairs over a 5-year period.22 In a systematic review of endoscopic skull base reconstruction of large dural defects, postoperative CSF leak following vascularized endonasal reconstruction for expanded endoscopic skull base surgery was estimated to be 6.7%.7 The dramatic effect of vascularized dural closure techniques for EESB procedures was also emphasized in several studies.7 22 43 In particular, Kono and colleagues observed a fivefold reduction in postoperative infections among intradural EESB patients from 11.5 to 2.4% following the introduction of vascularized endonasal flap reconstruction.69
Study Limitation
EESB surgery is an evolving field, and the risk of postoperative CSF and infectious complications may vary through time. In the current analysis, study heterogeneity was considerable because investigations from various centers presented different study designs, methodologies, management paradigms, and patient populations. Most of the studies presented in this systematic review were retrospective case series, and the potential confounding in a nonrandomized setting is not fully compensated by the use of multivariate analysis. The inherent publication bias, differences in patient demographic and clinical characteristics, and potential duplication of patients need to be taken into account.
In the current review, there is an overrepresentation of the 2005 published cases by one group.69 The University of Pittsburgh Medical Center (UPMC) data accounts for 1,000 of the total 2,005 included cases (49.9%). However, in a subanalysis, the meningitis rate was similar for the UPMC experience of 1.8% (18 of 1,000) as compared with the remaining publications: 1.8% (18 of 1,005). The bias of a single large center publishing report does not appear to alter significantly the published reports for other centers.
Furthermore, our assumption of EESB patients were those who underwent endonasal surgery for pathologies other than simple pituitary adenomas, repair of CSF leakages, or fistulas and encephaloceles repairs. Tumors such as chordoma and chondrosarcoma may not often involve a full-thickness dural defect, and a transcranial approach in such cases would not be necessary. However, this is difficult to establish in the reported case series. Attempts were made to exclude such cases, but some contamination in studies may occur.
Conclusion
Skull base pathologies are uncommon, and the evidence base is mostly limited to small case series. Current evidence in this systematic review suggests that the risk of meningitis following expanded EESB surgery is low (1.8%). There was no difference in the reported incidence of meningitis or CSF leak between anterior and posterior cranial fossa surgery. The incidence of meningitis from EESB surgery without an associated CSF is uncommon. Progress in EESB techniques that have reduced the incidence of subsequent CSF leaks will allow an expansion of indications of this direct approach to midline lesions.
Acknowledgments
Richard J. Harvey has served on an advisory board for Schering Plough, NeilMed Pharmaceuticals, and Glaxo-Smith-Kline. He has also acted as a consultant for Olympus and Medtronic, and for the speaker's bureau for Merck Sharp & Dohme, Glaxo-Smith-Kline, and Arthrocare. He has received grant support from NeilMed Pharmaceuticals.
Leon T. Lai is supported by a scholarship funded by Carl Zeiss Pty Ltd.
The authors declare that they have no further financial or other conflicts of interest in relation to this research and its publication.
References
- 1.Arbolay O L, González J G, González R H, Gálvez Y H. Extended endoscopic endonasal approach to the skull base. Minim Invasive Neurosurg. 2009;52(3):114–118. doi: 10.1055/s-0028-1119414. [DOI] [PubMed] [Google Scholar]
- 2.Batra P S, Citardi M J, Worley S, Lee J, Lanza D C. Resection of anterior skull base tumors: comparison of combined traditional and endoscopic techniques. Am J Rhinol. 2005;19(5):521–528. [PubMed] [Google Scholar]
- 3.Dehdashti A R Ganna A Witterick I Gentili F Expanded endoscopic endonasal approach for anterior cranial base and suprasellar lesions: indications and limitations Neurosurgery 2009644677–687.; discussion 687–689 [DOI] [PubMed] [Google Scholar]
- 4.Dehdashti A R Karabatsou K Ganna A Witterick I Gentili F Expanded endoscopic endonasal approach for treatment of clival chordomas: early results in 12 patients Neurosurgery 2008632299–307.; discussion 307–309 [DOI] [PubMed] [Google Scholar]
- 5.Frank G Pasquini E Doglietto F et al. The endoscopic extended transsphenoidal approach for craniopharyngiomas Neurosurgery 200659101ONS75–ONS83.; discussion ONS75–ONS83 [DOI] [PubMed] [Google Scholar]
- 6.Frank G Sciarretta V Calbucci F Farneti G Mazzatenta D Pasquini E The endoscopic transnasal transsphenoidal approach for the treatment of cranial base chordomas and chondrosarcomas Neurosurgery 200659101ONS50–ONS57.; discussion ONS50–ONS57 [DOI] [PubMed] [Google Scholar]
- 7.Harvey R J, Parmar P, Sacks R, Zanation A M. Endoscopic skull base reconstruction of large dural defects: a systematic review of published evidence. Laryngoscope. 2012;122(2):452–459. doi: 10.1002/lary.22475. [DOI] [PubMed] [Google Scholar]
- 8.Harvey R J, Winder M, Parmar P, Lund V. Endoscopic skull base surgery for sinonasal malignancy. Otolaryngol Clin North Am. 2011;44(5):1081–1140. doi: 10.1016/j.otc.2011.06.020. [DOI] [PubMed] [Google Scholar]
- 9.Lai L T, Morgan M K, Chin D CW. et al. Endoscopic endonasal transclival approach to the basilar artery. J Clin Neurosci. 2013;20(4):587–592. doi: 10.1016/j.jocn.2012.03.042. [DOI] [PubMed] [Google Scholar]
- 10.Lai L, Morgan K M, Chin D W, Snidvongs K, Harvey R J. Endoscopic endonasal transplanum approach to the paraclinoid internal carotid artery. J Neurol Surg B. 2013;20((4)):587–592. doi: 10.1055/s-0033-1347370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Komotar R J Raper D M Starke R M Anand V K Schwartz T H Endoscopic versus open clival chordoma resection: a systematic review: skull base Paper presented at: 21st Annual Meeting of the North American Skull Base Society; February 18–20, 2011; Scottsdale, AZ
- 12.Komotar R J Raper D M Starke R M Anand V K Schwartz T H Endoscopic endonasal versus transsphenoidal microscopic and open transcranial resection of craniopharyngiomas: a systematic meta-analysis of outcomes: skull base Paper presented at: 21st Annual Meeting of the North American Skull Base Society; February 18–20, 2011; Scottsdale, AZ
- 13.Raper D MS, Komotar R J, Starke R M, Anand V K, Schwartz T H. Endoscopic versus open approaches to the skull base: a comprehensive literature review. Oper Tech Otolaryngol—Head Neck Surg. 2011;22(4):302–307. [Google Scholar]
- 14.Rigante M, Massimi L, Parrilla C. et al. Endoscopic transsphenoidal approach versus microscopic approach in children. Int J Pediatr Otorhinolaryngol. 2011;75(9):1132–1136. doi: 10.1016/j.ijporl.2011.06.004. [DOI] [PubMed] [Google Scholar]
- 15.Dehdashti A R Ganna A Karabatsou K Gentili F Pure endoscopic endonasal approach for pituitary adenomas: early surgical results in 200 patients and comparison with previous microsurgical series Neurosurgery 20086251006–1015.; discussion 1015–1017 [DOI] [PubMed] [Google Scholar]
- 16.Drazin D, Zhuang L, Schievink W I, Mamelak A N. Expanded endonasal approach for the clipping of a ruptured basilar aneurysm and feeding artery to a cerebellar arteriovenous malformation. J Clin Neurosci. 2012;19(1):144–148. doi: 10.1016/j.jocn.2011.07.013. [DOI] [PubMed] [Google Scholar]
- 17.Enseñat J Alobid I de Notaris M et al. Endoscopic endonasal clipping of a ruptured vertebral-posterior inferior cerebellar artery aneurysm: technical case report Neurosurgery 201169(1, Suppl Operative):E121–E127.; discussion E127–E128 [DOI] [PubMed] [Google Scholar]
- 18.Kassam A B, Gardner P A, Mintz A, Snyderman C H, Carrau R L, Horowitz M. Endoscopic endonasal clipping of an unsecured superior hypophyseal artery aneurysm. Technical note. J Neurosurg. 2007;107(5):1047–1052. doi: 10.3171/JNS-07/11/1047. [DOI] [PubMed] [Google Scholar]
- 19.Kassam A B Mintz A H Gardner P A Horowitz M B Carrau R L Snyderman C H The expanded endonasal approach for an endoscopic transnasal clipping and aneurysmorrhaphy of a large vertebral artery aneurysm: technical case report Neurosurgery 200659101E162–E165.; discussion E162–E165 [DOI] [PubMed] [Google Scholar]
- 20.Froelich S, Cebula H, Debry C, Boyer P. Anterior communicating artery aneurysm clipped via an endoscopic endonasal approach: technical note. Neurosurgery. 2011;68 02:310–315. doi: 10.1227/NEU.0b013e3182117063. [DOI] [PubMed] [Google Scholar]
- 21.Germanwala A V Zanation A M Endoscopic endonasal approach for clipping of ruptured and unruptured paraclinoid cerebral aneurysms: case report Neurosurgery 201168(1, Suppl Operative):234–239.; discussion 240 [DOI] [PubMed] [Google Scholar]
- 22.Harvey R J, Nogueira J F Jr, Schlosser R J, Patel S J, Vellutini E, Stamm A C. Closure of large skull base defects after endoscopic transnasal craniotomy. Clinical article. J Neurosurg. 2009;111(2):371–379. doi: 10.3171/2008.8.JNS08236. [DOI] [PubMed] [Google Scholar]
- 23.Hadad G, Bassagasteguy L, Carrau R L. et al. A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope. 2006;116(10):1882–1886. doi: 10.1097/01.mlg.0000234933.37779.e4. [DOI] [PubMed] [Google Scholar]
- 24.Harvey R J, Smith J E, Wise S K, Patel S J, Frankel B M, Schlosser R J. Intracranial complications before and after endoscopic skull base reconstruction. Am J Rhinol. 2008;22(5):516–521. doi: 10.2500/ajr.2008.22.3223. [DOI] [PubMed] [Google Scholar]
- 25.Ganly I, Patel S G, Singh B. et al. Complications of craniofacial resection for malignant tumors of the skull base: report of an International Collaborative Study. Head Neck. 2005;27(6):445–451. doi: 10.1002/hed.20166. [DOI] [PubMed] [Google Scholar]
- 26.Carrau R L, Kassam A B, Snyderman C H, Duvvuri U, Mintz A, Gardner P. Endoscopic transnasal anterior skull base resection for the treatment of sinonasal malignancies. Oper Tech Otolaryngol—Head Neck Surg. 2006;17(2):102–110. [Google Scholar]
- 27.Kassam A B, Prevedello D M, Carrau R L. et al. Endoscopic endonasal skull base surgery: analysis of complications in the authors' initial 800 patients. J Neurosurg. 2011;114(6):1544–1568. doi: 10.3171/2010.10.JNS09406. [DOI] [PubMed] [Google Scholar]
- 28.Kassam A B Prevedello D M Thomas A et al. Endoscopic endonasal pituitary transposition for a transdorsum sellae approach to the interpeduncular cistern Neurosurgery 20086230157–72.; discussion 72–74 [DOI] [PubMed] [Google Scholar]
- 29.Kassam A B Thomas A Carrau R L et al. Endoscopic reconstruction of the cranial base using a pedicled nasoseptal flap Neurosurgery 200863101ONS44–ONS52.; discussion ONS52–ONS53 [DOI] [PubMed] [Google Scholar]
- 30.Prevedello D M, Fernandez-Miranda J C, Gardner P. et al. The transclival endoscopic endonasal approach (EEA) for prepontine neuroenteric cysts: report of two cases. Acta Neurochir (Wien) 2010;152(7):1223–1229. doi: 10.1007/s00701-009-0563-3. [DOI] [PubMed] [Google Scholar]
- 31.Gardner P A Kassam A B Thomas A et al. Endoscopic endonasal resection of anterior cranial base meningiomas Neurosurgery 200863136–52.; discussion 52–54 [DOI] [PubMed] [Google Scholar]
- 32.Solares C A, Fakhri S, Batra P S, Lee J, Lanza D C. Transnasal endoscopic resection of lesions of the clivus: a preliminary report. Laryngoscope. 2005;115(11):1917–1922. doi: 10.1097/01.mlg.0000172070.93173.92. [DOI] [PubMed] [Google Scholar]
- 33.Stippler M Gardner P A Snyderman C H Carrau R L Prevedello D M Kassam A B Endoscopic endonasal approach for clival chordomas Neurosurgery 2009642268–277.; discussion 277–278 [DOI] [PubMed] [Google Scholar]
- 34.Leong J L, Citardi M J, Batra P S. Reconstruction of skull base defects after minimally invasive endoscopic resection of anterior skull base neoplasms. Am J Rhinol. 2006;20(5):476–482. doi: 10.2500/ajr.2006.20.2931. [DOI] [PubMed] [Google Scholar]
- 35.Cavallo L M, Messina A, Esposito F. et al. Skull base reconstruction in the extended endoscopic transsphenoidal approach for suprasellar lesions. J Neurosurg. 2007;107(4):713–720. doi: 10.3171/JNS-07/10/0713. [DOI] [PubMed] [Google Scholar]
- 36.Dave S P, Bared A, Casiano R R. Surgical outcomes and safety of transnasal endoscopic resection for anterior skull tumors. Otolaryngol Head Neck Surg. 2007;136(6):920–927. doi: 10.1016/j.otohns.2007.01.012. [DOI] [PubMed] [Google Scholar]
- 37.De Divitiis E, Cavallo L M, Esposito F, Stella L, Messina A. Extended endoscopic transsphenoidal approach for tuberculum sellae meningiomas. Neurosurgery. 2008;62 06:SHC1192–SHC1200. doi: 10.1227/01.neu.0000333785.04435.2c. [DOI] [PubMed] [Google Scholar]
- 38.Santos Rde P, Zymberg S T, Abucham Filho J Z, Gregório L C, Weckx L LM. Endoscopic transnasal approach to sellar tumors. Braz J Otorhinolaryngol. 2007;73(4):463–475. doi: 10.1016/S1808-8694(15)30098-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Laufer I, Anand V K, Schwartz T H. Endoscopic, endonasal extended transsphenoidal, transplanum transtuberculum approach for resection of suprasellar lesions. J Neurosurg. 2007;106(3):400–406. doi: 10.3171/jns.2007.106.3.400. [DOI] [PubMed] [Google Scholar]
- 40.de Divitiis E Esposito F Cappabianca P Cavallo L M de Divitiis O Tuberculum sellae meningiomas: high route or low route? A series of 51 consecutive cases Neurosurgery 2008623556–563.; discussion 556–563 [DOI] [PubMed] [Google Scholar]
- 41.de Divitiis E, Esposito F, Cappabianca P, Cavallo L M, de Divitiis O, Esposito I. Endoscopic transnasal resection of anterior cranial fossa meningiomas. Neurosurg Focus. 2008;25(6):E8. doi: 10.3171/FOC.2008.25.12.E8. [DOI] [PubMed] [Google Scholar]
- 42.El-Banhawy O A, Halaka A N, Altuwaijri M A, Ayad H, El-Sharnoby M M. Long-term outcome of endonasal endoscopic skull base reconstruction with nasal turbinate graft. Skull Base. 2008;18(5):297–308. doi: 10.1055/s-0028-1086055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.El-Sayed I H, Roediger F C, Goldberg A N, Parsa A T, McDermott M W. Endoscopic reconstruction of skull base defects with the nasal septal flap. Skull Base. 2008;18(6):385–394. doi: 10.1055/s-0028-1096202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gardner P A, Kassam A B, Snyderman C H. et al. Outcomes following endoscopic, expanded endonasal resection of suprasellar craniopharyngiomas: a case series. J Neurosurg. 2008;109(1):6–16. doi: 10.3171/JNS/2008/109/7/0006. [DOI] [PubMed] [Google Scholar]
- 45.Nicolai P, Battaglia P, Bignami M. et al. Endoscopic surgery for malignant tumors of the sinonasal tract and adjacent skull base: a 10-year experience. Am J Rhinol. 2008;22(3):308–316. doi: 10.2500/ajr.2008.22.3170. [DOI] [PubMed] [Google Scholar]
- 46.Stamm A C, Vellutini E, Harvey R J, Nogeira J F Jr, Herman D R. Endoscopic transnasal craniotomy and the resection of craniopharyngioma. Laryngoscope. 2008;118(7):1142–1148. doi: 10.1097/MLG.0b013e318170b5dc. [DOI] [PubMed] [Google Scholar]
- 47.Cavallo L M, Prevedello D M, Solari D. et al. Extended endoscopic endonasal transsphenoidal approach for residual or recurrent craniopharyngiomas. J Neurosurg. 2009;111(3):578–589. doi: 10.3171/2009.2.JNS081026. [DOI] [PubMed] [Google Scholar]
- 48.Cohen M A, Liang J, Cohen I J, Grady M S, O'Malley B W Jr, Newman J G. Endoscopic resection of advanced anterior skull base lesions: oncologically safe? ORL J Otorhinolaryngol Relat Spec. 2009;71(3):123–128. doi: 10.1159/000209312. [DOI] [PubMed] [Google Scholar]
- 49.Eloy J A, Vivero R J, Hoang K. et al. Comparison of transnasal endoscopic and open craniofacial resection for malignant tumors of the anterior skull base. Laryngoscope. 2009;119(5):834–840. doi: 10.1002/lary.20186. [DOI] [PubMed] [Google Scholar]
- 50.Fatemi N Dusick J R de Paiva Neto M A Malkasian D Kelly D F Endonasal versus supraorbital keyhole removal of craniopharyngiomas and tuberculum sellae meningiomas Neurosurgery 200964502269–284.; discussion 284–286 [DOI] [PubMed] [Google Scholar]
- 51.Folbe A, Herzallah I, Duvvuri U. et al. Endoscopic endonasal resection of esthesioneuroblastoma: a multicenter study. Am J Rhinol Allergy. 2009;23(1):91–94. doi: 10.2500/ajra.2009.23.3269. [DOI] [PubMed] [Google Scholar]
- 52.Liu H S, Di X. Endoscopic endonasal surgery for biopsy of cavernous sinus lesions. Minim Invasive Neurosurg. 2009;52(2):69–73. doi: 10.1055/s-0029-1192015. [DOI] [PubMed] [Google Scholar]
- 53.Vergez S, Nadeau S H, Percodani J, Pessey J J, Serrano E. Endoscopic resection of sinonasal adenocarcinomas. Rev Laryngol Otol Rhinol (Bord) 2009;130(4–5):255–259. [PubMed] [Google Scholar]
- 54.Batra P S, Luong A, Kanowitz S J. et al. Outcomes of minimally invasive endoscopic resection of anterior skull base neoplasms. Laryngoscope. 2010;120(1):9–16. doi: 10.1002/lary.20680. [DOI] [PubMed] [Google Scholar]
- 55.Greenfield J P Anand V K Kacker A et al. Endoscopic endonasal transethmoidal transcribriform transfovea ethmoidalis approach to the anterior cranial fossa and skull base Neurosurgery 2010665883–892.; discussion 892 [DOI] [PubMed] [Google Scholar]
- 56.Jane J A Jr, Kiehna E, Payne S C, Early S V, Laws E R Jr. Early outcomes of endoscopic transsphenoidal surgery for adult craniopharyngiomas. Neurosurg Focus. 2010;28(4):E9. doi: 10.3171/2010.1.FOCUS09319. [DOI] [PubMed] [Google Scholar]
- 57.Madhok R, Prevedello D M, Gardner P, Carrau R L, Snyderman C H, Kassam A B. Endoscopic endonasal resection of Rathke cleft cysts: clinical outcomes and surgical nuances. J Neurosurg. 2010;112(6):1333–1339. doi: 10.3171/2009.10.JNS09348. [DOI] [PubMed] [Google Scholar]
- 58.Villaret A B, Yakirevitch A, Bizzoni A. et al. Endoscopic transnasal craniectomy in the management of selected sinonasal malignancies. Am J Rhinol Allergy. 2010;24(1):60–65. doi: 10.2500/ajra.2010.24.3397. [DOI] [PubMed] [Google Scholar]
- 59.Gallia G L, Reh D D, Salmasi V, Blitz A M, Koch W, Ishii M. Endonasal endoscopic resection of esthesioneuroblastoma: the Johns Hopkins Hospital experience and review of the literature. Neurosurg Rev. 2011;34(4):465–475. doi: 10.1007/s10143-011-0329-2. [DOI] [PubMed] [Google Scholar]
- 60.Carta F, Kania R, Sauvaget E, Bresson D, George B, Herman P. Endoscopy skull-base resection for ethmoid adenocarcinoma and olfactory neuroblastoma. Rhinology. 2011;49(1):74–79. doi: 10.4193/Rhino09.128. [DOI] [PubMed] [Google Scholar]
- 61.Frank G Sciarretta V Calbucci F Farneti G Mazzatenta D Pasquini E The endoscopic transnasal transsphenoidal approach for the treatment of cranial base chordomas and chondrosarcomas Neurosurgery 200659101ONS50–ONS57.; discussion ONS50–ONS57 [DOI] [PubMed] [Google Scholar]
- 62.Fortes F SG, Carrau R L, Snyderman C H. et al. The posterior pedicle inferior turbinate flap: a new vascularized flap for skull base reconstruction. Laryngoscope. 2007;117(8):1329–1332. doi: 10.1097/mlg.0b013e318062111f. [DOI] [PubMed] [Google Scholar]
- 63.Carrabba G, Dehdashti A R, Gentili F. Surgery for clival lesions: open resection versus the expanded endoscopic endonasal approach. Neurosurg Focus. 2008;25(6):E7. doi: 10.3171/FOC.2008.25.12.E7. [DOI] [PubMed] [Google Scholar]
- 64.Zhang Q, Kong F, Yan B, Ni Z, Liu H. Endoscopic endonasal surgery for clival chordoma and chondrosarcoma. ORL J Otorhinolaryngol Relat Spec. 2008;70(2):124–129. doi: 10.1159/000114536. [DOI] [PubMed] [Google Scholar]
- 65.Fraser J F, Nyquist G G, Moore N, Anand V K, Schwartz T H. Endoscopic endonasal transclival resection of chordomas: operative technique, clinical outcome, and review of the literature. J Neurosurg. 2010;112(5):1061–1069. doi: 10.3171/2009.7.JNS081504. [DOI] [PubMed] [Google Scholar]
- 66.Alfieri A Jho H D Endoscopic endonasal approaches to the cavernous sinus: surgical approaches Neurosurgery 2001492354–360.; discussion 360–362 [DOI] [PubMed] [Google Scholar]
- 67.Alfieri A Jho H D Schettino R Tschabitscher M Endoscopic endonasal approach to the pterygopalatine fossa: anatomic study Neurosurgery 2003522374–378.; discussion 378–380 [DOI] [PubMed] [Google Scholar]
- 68.Holzmann D, Reisch R, Krayenbühl N, Hug E, Bernays R L. The transnasal transclival approach for clivus chordoma. Minim Invasive Neurosurg. 2010;53(5–6):211–217. doi: 10.1055/s-0030-1267929. [DOI] [PubMed] [Google Scholar]
- 69.Kono Y, Prevedello D M, Snyderman C H. et al. One thousand endoscopic skull base surgical procedures demystifying the infection potential: incidence and description of postoperative meningitis and brain abscesses. Infect Control Hosp Epidemiol. 2011;32(1):77–83. doi: 10.1086/657635. [DOI] [PubMed] [Google Scholar]
- 70.Korinek A M Baugnon T Golmard J L van Effenterre R Coriat P Puybasset L Risk factors for adult nosocomial meningitis after craniotomy: role of antibiotic prophylaxis Neurosurgery 2006591126–133.; discussion 126–133 [DOI] [PubMed] [Google Scholar]
- 71.Korinek A M, Golmard J L, Elcheick A. et al. Risk factors for neurosurgical site infections after craniotomy: a critical reappraisal of antibiotic prophylaxis on 4,578 patients. Br J Neurosurg. 2005;19(2):155–162. doi: 10.1080/02688690500145639. [DOI] [PubMed] [Google Scholar]
- 72.Harvey R J, Nogueira J F, Schlosser R J, Patel S J, Vellutini E, Stamm A C. Closure of large skull base defects after endoscopic transnasal craniotomy. Clinical article. J Neurosurg. 2009;111(2):371–379. doi: 10.3171/2008.8.JNS08236. [DOI] [PubMed] [Google Scholar]
- 73.Snyderman C H, Kassam A B, Carrau R, Mintz A. Endoscopic reconstruction of cranial base defects following endonasal skull base surgery. Skull Base. 2007;17(1):73–78. doi: 10.1055/s-2006-959337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Kassam A Thomas A J Snyderman C et al. Fully endoscopic expanded endonasal approach treating skull base lesions in pediatric patients J Neurosurg 2007106(2, Suppl):75–86. [DOI] [PubMed] [Google Scholar]
- 75.Cappabianca P, Cavallo L M, Esposito F, de Divitiis O, Messina A, de Divitiis E. Extended endoscopic endonasal approach to the midline skull base: the evolving role of transsphenoidal surgery. Adv Tech Stand Neurosurg. 2008;33:151–199. doi: 10.1007/978-3-211-72283-1_4. [DOI] [PubMed] [Google Scholar]
- 76.Leng L Z Brown S Anand V K Schwartz T H “Gasket-seal” watertight closure in minimal-access endoscopic cranial base surgery Neurosurgery 200862502E342–E343.; discussion E343 [DOI] [PubMed] [Google Scholar]
- 77.Fraser J F Nyquist G G Moore N Anand V K Schwartz T H Endoscopic endonasal minimal access approach to the clivus: case series and technical nuances Neurosurgery 201067(3, Suppl Operative):ons150–ons158.; discussion ons158 [DOI] [PubMed] [Google Scholar]
- 78.Horiguchi K Murai H Hasegawa Y Hanazawa T Yamakami I Saeki N Endoscopic endonasal skull base reconstruction using a nasal septal flap: surgical results and comparison with previous reconstructions Neurosurg Rev 2010332235–241.; discussion 241 [DOI] [PubMed] [Google Scholar]
- 79.Nyquist G G, Anand V K, Singh A, Schwartz T H. Janus flap: bilateral nasoseptal flaps for anterior skull base reconstruction. Otolaryngol Head Neck Surg. 2010;142(3):327–331. doi: 10.1016/j.otohns.2009.12.020. [DOI] [PubMed] [Google Scholar]
- 80.Kurschel S, Gellner V, Clarici G, Braun H, Stammberger H, Mokry M. Endoscopic rhino-neurosurgical approach for non-adenomatous sellar and skull base lesions. Rhinology. 2011;49(1):64–73. doi: 10.4193/Rhino10.046. [DOI] [PubMed] [Google Scholar]