

Abstract
Background
Although Asian people are known to have lower bone mass than that of Caucasians, little is known about coffee-associated bone health in Asian. This study aimed to assess the relationship between coffee consumption and bone mineral density (BMD) in Korean premenopausal women.
Methods
Data were obtained from the Fourth Korea National Health and Nutrition Examination Survey 2008-2009. The study population consisted of 1,761 Korean premenopausal women (mean age 36 years) who were measured for lumbar spine and femoral neck BMD and who completed a standardized questionnaire about coffee intake frequency. We excluded the participants who took hormone replacement therapy or medication for osteoporosis. The cross-sectional relationship between coffee consumption and impaired bone health (osteopenia or osteoporosis) was investigated by bone densitometry.
Results
Coffee consumption showed no significant association with BMD of either femoral neck or lumbar spine, independent of other factors. The adjusted odds ratios for BMD for those who consumed once in a day, twice a day and three times a day were 0.94 (0.70-1.26), 0.93 (0.67-1.28), and 1.02 (0.69-1.50), respectively (P for trend = 0.927).
Conclusion
This study does not support the idea that coffee is a risk factor for impaired bone health in Korean premenopausal women.
Keywords: Coffee, Bone Density, Premenopause, Asian Continental Ancestry Group
INTRODUCTION
Coffee is probably the most commonly consumed pharmacologically active compound in the world, certainly in Europe and America.1) Korea is currently the 11th largest coffee consumer in the world, and the consumption rate has sharply increased in recent years, making coffee an important environmental exposure.2) It may be surprising that there were more than 10 thousand coffeehouses in 2011, compared with 9,400 coffeehouses in 2010. Estimated average Korean coffee consumption is about 1.28 cups per day, which is the equivalent of approximately 180 mg of caffeine daily.3) Recently, several investigators have reported that the consumption of coffee is associated with low bone density and osteoporotic fracture.4) Osteoporotic fractures are associated with morbidity and mortality, increasing health costs, and decreased quality of life. Thus, coffee-associated osteoporosis is an increasing concern among the Korean population, especially among young Korean women.
The measurement of bone mineral density (BMD) in absolute terms by dual-energy X-ray absorptiometry (DXA) made it possible to compare the BMD among the different ethnic groups.5) Several studies reported that Asian women have lower bone mass than Caucasians even after taking into account the differences between the body sizes of Caucasian and Asian women.6) However, less is known about the characteristics of osteoporosis in Asian populations compared to Western countries.5,7,8) Although some differences in gene polymorphisms related to osteoporosis between Asians and Caucasians were reported,9) demographic, behavioral, and cultural factors might be reflected in racial and ethnic disparities in osteoporosis rather than genetic differences.10,11) Among them, nutrition is an important modifiable factor in the development and maintenance of bone mass and the prevention and treatment of osteoporosis.12)
In this report, we explored the relationship between coffee consumption and bone health in Korean premenopausal women, taking into account potential confounding factors including age, body mass index (BMI), smoking status, alcohol consumption, physical activity, dietary intake of calcium, education level, and monthly income.
METHODS
1. Subjects
The present study is a cross-sectional study. The study population consisted of 11,064 women and 9,213 men who participated in the fourth Korean National Health and Nutritional Examination Survey (KNHANES IV), conducted between 2008 and 2009. KNHANES IV (2008-2009) was a nationwide survey representing the Korean general population and included comprehensive information on the health status, health behavior, and demographics of 20,277 individuals. The health interview survey was conducted through face-to face interviews by trained interviewers. Each participant gave informed consent prior to inclusion in the study. In this study premenopausal women under 50 years old were included (n = 6,994), taking into account the facts that young women usually drink more coffee than the elderly and bone health of postmenopausal women could be affected by hormonal changes.13,14) We selected individuals who had received DXA of lumbar spine and femoral neck between 2008-2009 and individuals who completed the coffee consumption questionnaire. We then excluded individuals who had undergone any hormone replacement therapy or medication for osteoporosis, recruiting 1,761 women as the final study population. As the survey data analyzed are publicly available, this study did not require the ethical approval of the institutional review board.
2. Measurements of Anthropometric Parameters and BMD
All the participants completed a questionnaire about smoking habits, alcohol consumption, physical activity, dietary intake of calcium, dietary supplements (any vitamins, minerals, or functional foods), education level, monthly income, menopause state, and medication. With regard to smoking, the participants were grouped as nonsmokers, ex-smokers, or current smokers. The other health behavioral risk variables included alcohol consumption (nondrinker, <3 standard drinks/occasion, and ≥3 standard drinks/occasion)15,16) and physical activity per week (3 quintiles: <12.0 metabolic equivalent [METs]/wk, 12-43.5 METs/wk, and >43.5 METs/wk).17) We divided educational background status into elementary school graduate, middle school or high school graduate, and college graduate or above. Menopause state was checked among women. All data were collected by trained staff using standardized protocols. Height and weight were measured with the participants wearing light, single-thickness clothing. BMI was calculated as the ratio of weight to the square of height (kg/m2) and was divided into 3 categories (≤20 kg/m2, >20-24.99 kg/m2, and ≥25 kg/m2).18) Dietary calcium intake was monitored by 24-hour recall and analyzed by CAN-Pro software 3.0 (Korean Nutrition Society, Seoul, Korea), and was divided into 3 quintiles (<231 mg/d, 231-422 mg/d, and >422 mg/d). Any vitamins, minerals, or functional foods taken or eaten for at least two weeks in recent years were included in dietary supplements. The KNHANES osteoporosis survey was a large-scale BMD survey undertaken by the Korean government in which accurate and reliable results were calculated from data gathered by educated and quality controlled osteoporosis examination surveyors.19) The BMD (g/cm2) measurements of the lumbar spine (L1-L4) and femoral neck were obtained using a DXA scan (DISCOVERY-W fan-beam densitometer; Hologic Inc., Waltham, MA, USA). L1-L4 values were used for BMD analysis in this study. The definitions of osteopenia or osteoporosis were made using World Health Organization T-score criteria (-2.5 < T-score < -1 and T-score ≤ -2.5, respectively). We considered osteopenia and osteoporosis indications of impaired bone health, taking into account that the proportion of osteoporosis was too small in this population (aged under 50). Additionally we considered participants who were taking prescription medications (e.g., bisphosphonate, raloxifene, hormonal agents, etc.) as having osteoporosis.
3. Coffee Consumption Assessment
The participants answered a questionnaire on the frequency of coffee consumption. We divided the participants into 4 categories on the basis of average coffee consumption. Group I (n = 599) included participants who reported drinking less than once a day. Group II (n = 497) consisted of participants who reported drinking once a day. Group III (n = 411) included participants who reported drinking twice a day, and group IV (n = 254) consisted of participants who reported drinking coffee three times a day. The general characteristic according to the frequency of coffee consumption is presented in Table 1.
Table 1.
Characteristics of the participants according to coffee consumption (n* = 1,761)

Values are presented as % (standard error). All data are weighted to the residential population of Korea.
METs: metabolic equivalent.
*Unweighted sample size. †Group I: <1 cup/d (n = 599), group II: 1 cup/d (n = 497), group III: 2 cups/d (n = 411), group IV: 3 cups/d (n = 254). ‡High-risk drinking is defined as consuming more than 3 standard drinks (=30 g of pure alcohol) per occasion on average. §Physical activity per week was divided into 3 tertiles (<12.0 METs/wk, 12-43.5 METs/wk, and >43.5 METs/wk). ∥Dietary calcium intake was divided into 3 tertiles (<231 mg/d, 231-422 mg/d, and >422 mg/d). ¶Dietary supplements include kinds of vitamins, minerals and health functional foods. **Impaired bone health included osteopenia and osteoporosis.
4. Statistics
We used a weighted population sample to reflect the sampling method and response rate. We calculated the estimated proportions and standard errors for osteoporosis (at lumbar spine, femoral neck, and both lumbar spine and femoral neck). We constructed a multivariate logistic regression analysis to estimated adjusted odds ratios (ORs) and 95% confidence intervals (CI) for the risk of osteoporosis (including osteopenia) using group I as a reference and controlling for confounding variables (age, BMI, smoking status, alcohol consumption, physical activity, dietary intake of calcium, education level, and monthly income). A trend test was carried out. All results were considered significant if P < 0.05. All analyses were performed using Stata SE ver. 12.0 (Stata Co., College Station, TX, USA).
RESULTS
1. Baseline Characteristics
The characteristics of the study participants are presented in Table 1. The prevalence of impaired bone health (osteopenia/osteoporosis) of both femoral neck and lumbar spine in the study subjects was 34.8%. Over sixty percent of the study population drank coffee at least once a day. Smoking habit did not seem to be related to coffee consumption. Almost one fourth of the participants did not drink alcohol at all. Although their recommended calcium intake was 1,000 mg per day, more than seventy percent of participants ingested less than 422 mg per day.20)
2. Coffee and Bone Mineral Density of Both Femoral Neck and Lumbar Spine
Table 2 presents the relationship between coffee consumption and impaired bone health. Subjects were stratified into groups according to the site of impaired bone health. Coffee consumption showed no significant association with impaired bone health of both the lumbar spine and femoral neck (P = 0.927). In participants who consumed coffee once a day, the adjusted ORs for impaired bone health were 0.94 (0.70-1.26) after adjustment for age, BMI, smoking status, alcohol consumption, physical activity, dietary calcium level, dietary supplements, education level, and monthly income. In participants who consumed twice and three times a day, the multivariate adjusted ORs for impaired bone health were 0.93 (0.67-1.28) and 1.02 (0.69-1.50), respectively.
Table 2.
Relationship between coffee consumption and impaired bone health (lumbar spine or femoral neck T-score < -1.0, or taking anti-osteoporotic medications) according to site
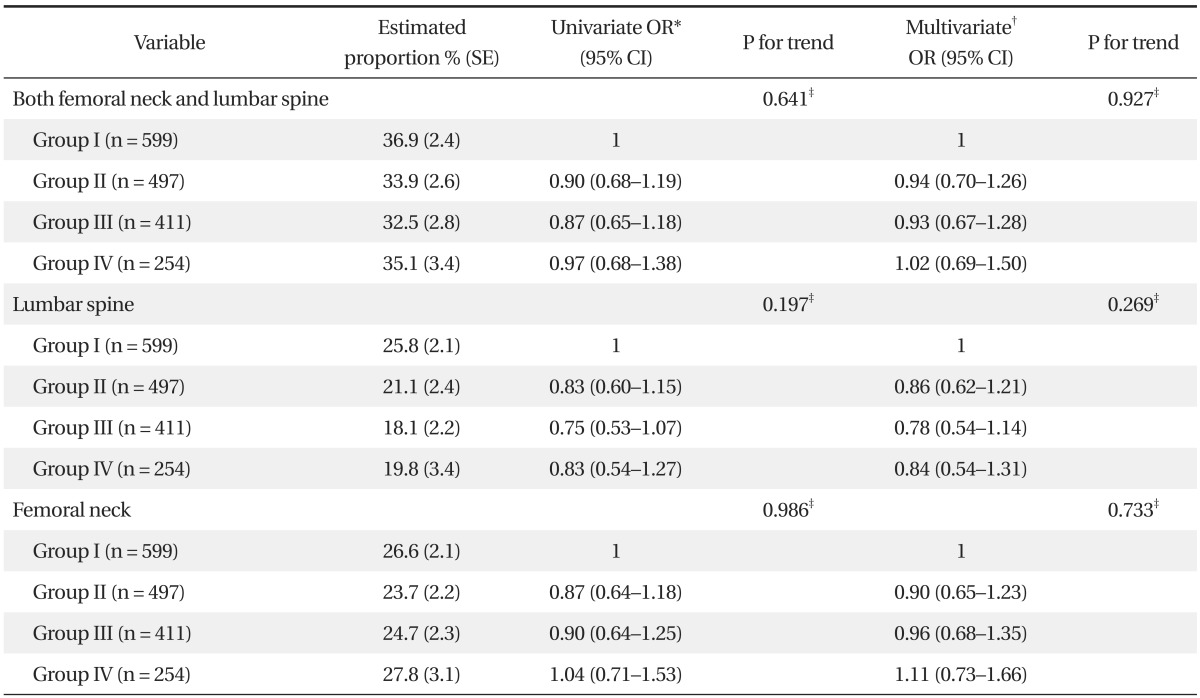
All data are weighted to the residential population of Korea.
SE: standard error, OR: odds ratio, CI: confidence interval, METs: metabolic equivalent.
*Univariate adjusted ORs for age. †Multivariate adjusted ORs for age, body mass index, smoking status, alcohol consumption, physical activity, dietary calcium intake, education level, and monthly income. ‡P for trend from logistic regression analysis.
3. Coffee and Bone Mineral Density of Lumbar Spine
Similarly, no statistically significant associations (P-value for trend = 0.269) were found when we adjusted for age, BMI, smoking status, alcohol consumption, physical activity, dietary calcium level, education level, or monthly income. Multivariate adjusted OR of group II was 0.86 (95% CI, 0.62 to 1.21) and that of group III and group IV was 0.78 (95% CI, 0.54 to 1.14), 0.84 (95% CI, 0.54 to 1.31), respectively.
4. Coffee and Bone Mineral Density of Femoral Neck
Femoral neck is considered to be a better site than the lumbar spine for the clinical evaluation of osteoporosis with the duel energy radiography technique.21) We, however, found no associations between coffee consumption and osteoporosis of the femoral neck (P-value for trend = 0.733). Multivariate adjusted OR of group II was 0.90 (95% CI, 0.65 to 1.23) and that of group III and group IV was 0.96 (95% CI, 0.68 to 1.35), 1.11 (95% CI, 0.73 to 1.66), respectively.
DISCUSSION
This study shows that high consumption of coffee is not associated with increased risk for impaired bone health. Our results are in agreement with some recent cross-sectional studies showing no association between caffeine and impaired bone health, and in disagreement with others which focused on BMD of various skeletal sites.22-26) Habitual dietary caffeine intake was found not to be associated with impaired bone health in healthy postmenopausal women in a longitudinal study in Pennsylvania (USA), on the basis of self-reported questionnaires collected in 2000.23) In elderly men and women from the population-based Framingham Osteoporosis Study, the same results were found.24) These studies are in agreement with our study. Although the frequency consumed and the species of coffee could be significantly affected by cultural differences and socioeconomic status, and the metabolism of caffeine and other constituents can be affected by genetic predisposition, our results in Korean premenopausal women did not appear to contradict those of previous studies.
The role of coffee intake in bone health, however, seems controversial. There are several studies showing a negative association between caffeine and bone health. Daily intake of 330 mg of caffeine, equivalent to 4 cups (600 mL) of coffee, or more may be associated with a modestly increased risk of osteoporotic fractures, especially in women with a low intake of calcium, as shown in a study on Swedish women aged 40 to 76 years.4) Also, in a cohort study, Men consuming 4 cups of coffee or more per day had 4% lower BMD at the proximal femur (P = 0.04) compared with low or non-consumers of coffee. This difference was not observed in women, suggesting that rapid metabolizers of caffeine may constitute a risk group for bone loss induced by coffee.24)
The difference between the studies is considered to be due to the characteristics of the participants. Bone loss is usually seen in postmenopausal women and it is known to be due to hormonal changes (e.g., loss of serum estrogen).27) In this study, however, most of the participants were in the premenopausal state, so a bone loss could not be observed. Further, among young adults the duration of regular caffeine consumption may not have been long enough to have had a measurable effect on bone health. In addition to age of participants, caffeine dose is also a major difference between the latter studies. Negative effects of coffee consumption on bone mass was seen only when caffeine intake was more than 300 mg (equivalent to four cups of coffee).
It should be noted that our brief food frequency questionnaire did not ask specific questions regarding ingredient added to the coffee (milk, cream powder, sugar-contained or decaffeinated, etc.). It is likely that a high caffeine intake is often a marker for a low calcium intake which is linked to skeletal fragility. The negative effect of caffeine on calcium absorption is small enough to be fully offset by as little as 1 to 2 tablespoons of milk.25) Although differences in milk and sugar contents of regular and decaffeinated roasted coffees appear to be relatively small, they may be enough to affect flavor characteristics as well as the biopharmacological properties of the final beverage, suggesting the need for further study.28) In Korea, most women are thought to consume an instant form of coffee which contains various ingredients (milk, cream powder, sugar, etc.),29) possibly offsetting the negative effects of the coffee on bone health. Further studies may be needed to assess the effects of coffee on bone health with specific investigation into the ingredients of the various coffees that are consumed.
Our study had certain limitations. First, this study was cross-sectional. Thus, we could not establish a cause-and-effect relationship between coffee consumption and risk of impaired bone health. However, the majority of populations were over 30 years of age and they were supposed to have consumed coffee for several years, compared with the younger women. Second, in assessing intake frequency, the reference group could not be the non-consumer due to the limitations of the questionnaire about the coffee intake frequency in the KNHANES. Also the maximal dose of coffee intake was three cups a day, comparing to the other study has shown the adverse effect of coffee amount in amount of three cups and over per day.30) Third, we used the T-score for evaluation of bone health, although the Z-score is more suitable to evaluate that of premenopausal women. This is due to the fact that the reference group of the Z-score consists of people of the same age and gender, whereas the reference group of the T-score consists of healthy people of young age. In the KNHANES, however, we could not get BMD data on the Z-score.
Despite these limitations, our study had several strengths. Our study represents one of the few of its kind to investigate bone health among the Asian population. Moreover, using the sample of participants derived from a nationally representative sample which was objectively verified makes our results more applicable to the general population of premenopausal Korean women. The KNHANES osteoporosis survey was a large-scaled BMD survey undertaken by the Korean government, in which accurate and reliable results were calculated from data gathered by educated and quality-controlled osteoporosis examination surveyors.19) The BMD (g/cm2) measurements were obtained using a DXA scan. We also adjusted as many variables as possible which have been considered to be associated with bone health.
Estimates suggest that among South Koreans, almost 63% of premenopausal women consume coffee at least once a day.2) In light of rapidly increasing coffee consumption in Asia, including Korea, the effect of coffee on bone health should be considered, and no association was presented in this study. Considering different characteristics by ethnicity, further investigation into the individual effects of coffee is needed.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Mandel HG. Update on caffeine consumption, disposition and action. Food Chem Toxicol. 2002;40:1231–1234. doi: 10.1016/s0278-6915(02)00093-5. [DOI] [PubMed] [Google Scholar]
- 2.United States Department of Agriculture, Foreign Agricultural Service. Coffee: world markets and trade. Washington (DC): United States Department of Agriculture, Foreign Agricultural Service; 2012. [Google Scholar]
- 3.Grigg D. The worlds of tea and coffee: patterns of consumption. GeoJournal. 2002;57:283–294. [Google Scholar]
- 4.Hallström H, Wolk A, Glynn A, Michaelsson K. Coffee, tea and caffeine consumption in relation to osteoporotic fracture risk in a cohort of Swedish women. Osteoporos Int. 2006;17:1055–1064. doi: 10.1007/s00198-006-0109-y. [DOI] [PubMed] [Google Scholar]
- 5.Shin CS, Choi HJ, Kim MJ, Kim JT, Yu SH, Koo BK, et al. Prevalence and risk factors of osteoporosis in Korea: a community-based cohort study with lumbar spine and hip bone mineral density. Bone. 2010;47:378–387. doi: 10.1016/j.bone.2010.03.017. [DOI] [PubMed] [Google Scholar]
- 6.Barrett-Connor E, Siris ES, Wehren LE, Miller PD, Abbott TA, Berger ML, et al. Osteoporosis and fracture risk in women of different ethnic groups. J Bone Miner Res. 2005;20:185–194. doi: 10.1359/JBMR.041007. [DOI] [PubMed] [Google Scholar]
- 7.Fatima M, Nawaz H, Kassi M, Rehman R, Kasi PM, Kassi M, et al. Determining the risk factors and prevalence of osteoporosis using quantitative ultrasonography in Pakistani adult women. Singapore Med J. 2009;50:20–28. [PubMed] [Google Scholar]
- 8.Karunanayake AL, Pinidiyapathirage MJ, Wickremasinghe AR. Prevalence and predictors of osteoporosis in an urban Sri Lankan population. Int J Rheum Dis. 2010;13:385–390. doi: 10.1111/j.1756-185X.2010.01566.x. [DOI] [PubMed] [Google Scholar]
- 9.Ongphiphadhanakul B, Chanprasertyothin S, Payattikul P, Saetung S, Rajatanavin R. The implication of assessing a polymorphism in estrogen receptor alpha gene in the risk assessment of osteoporosis using a screening tool for osteoporosis in Asians. Osteoporos Int. 2003;14:863–867. doi: 10.1007/s00198-003-1464-6. [DOI] [PubMed] [Google Scholar]
- 10.Nakajima T, Ota N, Shirai Y, Hata A, Yoshida H, Suzuki T, et al. Ethnic difference in contribution of Sp1 site variation of COLIA1 gene in genetic predisposition to osteoporosis. Calcif Tissue Int. 1999;65:352–353. doi: 10.1007/s002239900711. [DOI] [PubMed] [Google Scholar]
- 11.Megyesi MS, Hunt LM, Brody H. A critical review of racial/ethnic variables in osteoporosis and bone density research. Osteoporos Int. 2011;22:1669–1679. doi: 10.1007/s00198-010-1503-z. [DOI] [PubMed] [Google Scholar]
- 12.Ilich JZ, Kerstetter JE. Nutrition in bone health revisited: a story beyond calcium. J Am Coll Nutr. 2000;19:715–737. doi: 10.1080/07315724.2000.10718070. [DOI] [PubMed] [Google Scholar]
- 13.Ahn YJ. Survey on the actual condition for adults' knowledge, attitude, and intake of caffeinated beverages [dissertation] Daegu: Keimyung University; 2011. [Google Scholar]
- 14.Kim MS, Koo JO. Analysis of factors affecting bone mineral density with different age among adult women in Seoul area. Korean J Community Nutr. 2007;12:559–568. [Google Scholar]
- 15.Ganry O, Baudoin C, Fardellone P. Effect of alcohol intake on bone mineral density in elderly women: The EPIDOS Study. Epidemiologie de l'Osteoporose. Am J Epidemiol. 2000;151:773–780. doi: 10.1093/oxfordjournals.aje.a010277. [DOI] [PubMed] [Google Scholar]
- 16.Felson DT, Zhang Y, Hannan MT, Kannel WB, Kiel DP. Alcohol intake and bone mineral density in elderly men and women. The Framingham Study. Am J Epidemiol. 1995;142:485–492. doi: 10.1093/oxfordjournals.aje.a117664. [DOI] [PubMed] [Google Scholar]
- 17.Hallal PC, Victora CG. Reliability and validity of the International Physical Activity Questionnaire (IPAQ) Med Sci Sports Exerc. 2004;36:556. doi: 10.1249/01.mss.0000117161.66394.07. [DOI] [PubMed] [Google Scholar]
- 18.De Laet C, Kanis JA, Oden A, Johanson H, Johnell O, Delmas P, et al. Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int. 2005;16:1330–1338. doi: 10.1007/s00198-005-1863-y. [DOI] [PubMed] [Google Scholar]
- 19.Lewiecki EM, Gordon CM, Baim S, Leonard MB, Bishop NJ, Bianchi ML, et al. International society for clinical densitometry 2007 adult and pediatric official positions. Bone. 2008;43:1115–1121. doi: 10.1016/j.bone.2008.08.106. [DOI] [PubMed] [Google Scholar]
- 20.National Osteoporosis Foundation. NOF responds to the U.S. Preventive Services Task Force recommendations on calcium and vitamin D [Internet] Washington (DC): National Osteoporosis Foundation; 2013. [cited 2013 Feb 26]. Available from: http://www.nof.org. [Google Scholar]
- 21.Griffin MG, Rupich RC, Avioli LV, Pacifici R. A comparison of dual energy radiography measurements at the lumbar spine and proximal femur for the diagnosis of osteoporosis. J Clin Endocrinol Metab. 1991;73:1164–1169. doi: 10.1210/jcem-73-6-1164. [DOI] [PubMed] [Google Scholar]
- 22.Hannan MT, Felson DT, Dawson-Hughes B, Tucker KL, Cupples LA, Wilson PW, et al. Risk factors for longitudinal bone loss in elderly men and women: the Framingham Osteoporosis Study. J Bone Miner Res. 2000;15:710–720. doi: 10.1359/jbmr.2000.15.4.710. [DOI] [PubMed] [Google Scholar]
- 23.Lloyd T, Johnson-Rollings N, Eggli DF, Kieselhorst K, Mauger EA, Cusatis DC. Bone status among postmenopausal women with different habitual caffeine intakes: a longitudinal investigation. J Am Coll Nutr. 2000;19:256–261. doi: 10.1080/07315724.2000.10718924. [DOI] [PubMed] [Google Scholar]
- 24.Hallström H, Melhus H, Glynn A, Lind L, Syvanen AC, Michaelsson K. Coffee consumption and CYP1A2 genotype in relation to bone mineral density of the proximal femur in elderly men and women: a cohort study. Nutr Metab (Lond) 2010;7:12. doi: 10.1186/1743-7075-7-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Heaney RP. Effects of caffeine on bone and the calcium economy. Food Chem Toxicol. 2002;40:1263–1270. doi: 10.1016/s0278-6915(02)00094-7. [DOI] [PubMed] [Google Scholar]
- 26.Chouinard LE, Randall Simpson J, Buchholz AC. Predictors of bone mineral density in a convenience sample of young Caucasian adults living in southern Ontario. Appl Physiol Nutr Metab. 2012;37:706–714. doi: 10.1139/h2012-049. [DOI] [PubMed] [Google Scholar]
- 27.Conlisk AJ, Galuska DA. Is caffeine associated with bone mineral density in young adult women? Prev Med. 2000;31:562–568. doi: 10.1006/pmed.2000.0742. [DOI] [PubMed] [Google Scholar]
- 28.Farah A, de Paulis T, Moreira DP, Trugo LC, Martin PR. Chlorogenic acids and lactones in regular and water-decaffeinated arabica coffees. J Agric Food Chem. 2006;54:374–381. doi: 10.1021/jf0518305. [DOI] [PubMed] [Google Scholar]
- 29.Kim MJ. Economics of coffee. Seoul: Jihoon Publishing House; 2008. [Google Scholar]
- 30.Harris SS, Dawson-Hughes B. Caffeine and bone loss in healthy postmenopausal women. Am J Clin Nutr. 1994;60:573–578. doi: 10.1093/ajcn/60.4.573. [DOI] [PubMed] [Google Scholar]