

Abstract
Purpose:
Changes in undergraduate medical curricula, combined with reforms in postgraduate education, have training implications for surgical skills acquisition in a climate of reduced clinical exposure. Confidence and prior experience influences the educational impact of learning. Currently there is no basic surgical skills (BSS) programme integrated into undergraduate curricula in the United Kingdom. We explored the role of a dedicated BSS programme for undergraduates in improving confidence and influencing careers in King’s College London School of Medicine, and the programme was evaluated.
Methods:
A programme was designed in-line with the established Royal College of Surgeons course. Undergraduates were taught four key skills over four weeks: knot-tying, basic-suturing, tying-at-depth and chest-drain insertion, using low-fidelity bench-top models. A Likert-style questionnaire was designed to determine educational value and influence on career choice. Qualitative data was collected.
Results:
Only 29% and 42% of students had undertaken previous practice in knot-tying and basic suturing, respectively. 96% agreed that skills exposure prior to starting surgical rotations was essential and felt a dedicated course would augment undergraduate training. There was a significant increase in confidence in the practice and knowledge of all skills taught (p<0.01), with a greater motivation to be actively involved in the surgical firm and theatres.
Conclusion:
A simple, structured BSS programme can increase the confidence and motivation of students. Early surgical skills targeting is valuable for students entering surgical, related allied, and even traditionally non-surgical specialties such as general practice. Such experience can increase the confidence of future junior doctors and trainees. We advocate the introduction of a BSS programme into United Kingdom undergraduate curricula.
Keywords: Surgical skills, Undergraduate training, Evaluation, Career choice, Confidence, United Kingdom
INTRODUCTION
The UK undergraduate medical curriculum has undergone numerous changes. There is now a greater emphasis on ethics and law and community medicine, with less time spent on traditional attachments such as surgery [1]. The demands of surgical training programmes have made it important that graduates entering residency/core training bring with them greater surgical skill experience, so as to more quickly and efficiently progress in a time-constrained and European Working-Time Directive (EWTD) limited training environment [2]. We have explored whether basic surgical skills training for interested undergraduates can be addressed by a basic surgical skills course aimed at increasing confidence in surgical skills, but also interest in the surgical specialty, by exposing students to current surgical trainees as potential mentors and role models. There are no major reports in the literature from UK medical schools on simulation strategies provided by undergraduates for undergraduates. The King’s College London Surgical Society (KCLSS) at King’s College London School of Medicine (KCLSM) trialled a basic surgical skills programme for medical students. The course is modelled on the Royal College of Surgeons’ Basic Surgical Skills Course (RCSENG BSS), and lasts for four weeks with weekly small group sessions. The skills covered include basic knot-tying, basic suturing, tying at depth and a more complex skill of chest drain insertion. This paper presents the results of the first two KCLSS BSS courses with students’ evaluation of the courses.
METHODS
Programme implementation
The KCLSS BSS course was held twice per academic year, in the autumn and then the spring terms in 2008/09 academic year. All of the courses were held in the Clinical Skills Laboratory, adhering to local KCL policy. The course was implemented by the KCLSS and was an undergraduate society initiative in collaboration with KCLSM-affiliated surgical trainees at Guy’s & St Thomas’ Hospitals. A maximum of 25 students were taught each time and reservations made on a first-come firstserve basis. The course was advertised on the KCLSM and KCLSS websites. All KCLSM students were allowed to participate. The student to faculty ratio was 4:1, with skills taught in 4 sessions over 4 weeks, each 3 hours in duration. Teaching was small-group-based and interactive. Faculty volunteered to provide their services at no cost; they consisted of core surgical trainees and final year medical students who were members of the KCLSS. As part of their training, the surgical trainees had undergone formal RCSENG BSS and Adult Trauma Life Support (ATLS) courses, as well as Training the Trainers courses. The final year medical students who taught the course were tutored by surgical trainees to competently teach the skills. A range of expired suturing material (on curved needles and straight needles), out-of-date surgical ties, and plastic tubes (used to simulate chest drains) were donated by the theatres. Synthetic foam was used to simulate skin and underlying tissue; half was donated by Ethicon, and the other half was provided by the clinical skills laboratory. Surgical instruments were provided free of charge by the clinical skills laboratory (needle holders, forceps, artery clips and scissors).
Programme evaluation
A questionnaire was designed to assess course relevance, educational value and influence on career choice. Students were asked to score their answers on a 5-point Likert scale, where 5, strongly agree; 4, agree; 3, neutral; 2, disagree; and 1, strongly disagree. Precourse questions explored students’ interests in surgery, previous surgical skills teaching and practice, and confidence in performing the four skills taught in the course. Postcourse questions examined students’ opinions on the course in relation to their undergraduate teaching, motivation to participate in theatres, and confidence to participate more during clinical rotations. Confidence in performing the four skills after the course was assessed to determine any impact the four weeks of teaching may have had on their perceptions of their skills. There was also a qualitative section which allowed students to make any comments about any aspect of the course in their own words. The pre-course questionnaire was completed by the students prior to starting the first of the four sessions of the course and the postcourse questions were completed one week following course completion. Consent was obtained from all participants as per local policy prior to completing the pre- and postcourse questionnaires. All of the information was collected anonymously and stored in a security protected Microsoft Excel database.
Analysis
The quantitative Likert data is presented as percentiles in tables, with agreeable (i.e., scores of 5 or 4; “strongly agree” or “agree”) and disagreeable (i.e., scores of 1 or 2; “strongly disagree” or “disagree”) responses amalgamated to more easily distinguish overall positive or negative sentiment. Pre- and postcourse skills confidence is represented in a full 5-point Likert format. The Kruskal-Wallis test and Mann-Whitney tests were used to establish significance of differences in confidence between skills and the Wilcoxon signed rank test to determine statistical significance of any changes in confidence after completion of the course. A 2-tailed P-value of less than 0.05 was considered indicative of statistical significance.
RESULTS
Forty-seven 3rd and 4th year clinical students took part in the first course and all completed both pre- and post-course questionnaires. Twenty-five students completed it in the autumn term, and 22 the following spring term (a necessary reduction due to the last-minute limited availability of suitable tutors). The precourse questionnaire results are reported in Table 1. Prior to starting the course, the students lacked confidence equally in performing all of the four specific skills that the course aimed to teach (p>0.05) (Fig. 1).
Table 1.
Responses to precourse questions determining students’ previous surgical skill learning and experience in 2008/09 academic year, King’s College London School of Medicine
| Question | Strongly agree or agree (%) | Neutral (%) | Disagree or strongly disagree (%) |
|---|---|---|---|
| You would like to specialise in surgery or a surgical sub-specialty | 75.6 | 20.0 | 4.4 |
| You have had operative room experience | 86.5 | 5.4 | 8.1 |
| You have practised knot-tying before | 28.6 | 14.3 | 57.1 |
| You have practised suturing before | 44.4 | 13.9 | 41.7 |
Fig. 1.
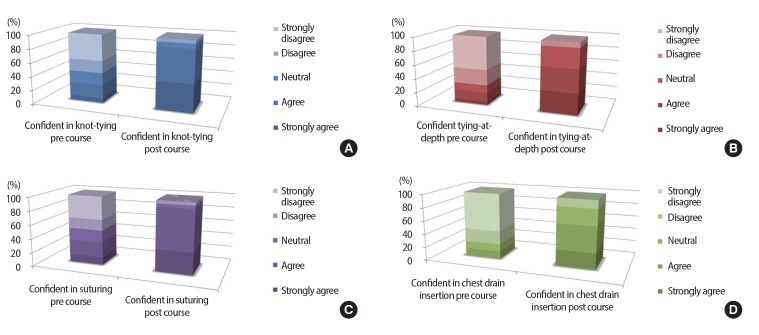
Reported confidence in performing knot tying (A), knot tying at depth (B), suturing (C), and chest drain insertion (D) prior to enrolling in the course and after completion, with significant increase across all four skills (p<0.01) in 2008/09 academic year, King’s College London School of Medicine.
The postcourse questionnaire results are shown in Table 2. More than 90% of the students graded the quality of teaching provided as good or excellent, with 70% finding experienced surgical trainees as tutors a beneficial source of surgical insight and knowledge on relevant anatomy, procedural indications, and potential complications during the course. There was a significant increase in confidence in all four of the skills taught over the four weeks (p<0.01), with the majority of students ‘agreeing’ or ‘strongly agreeing’ that they were now more confident in each skill (Fig. 1). There was no difference reported in postcourse confidence among the four skills taught (p>0.05). More than 80% felt better prepared for their surgical rotations and for allied surgical specialty rotations such as emergency medicine and obstetrics and gynaecology. They also reported an increase in confidence and motivation to attend and involve in the operation room.
Table 2.
Responses to postcourse questions examining students’ evaluation of the course and relevance to their training in 2008/09 academic year, King’s College London School of Medicine
| Questions | Strongly agree or agree (%) | Neutral (%) | Disagree or strongly disagree (%) |
|---|---|---|---|
| You found the course complemented your education | 95.5 | 4.5 | 0 |
| The course motivated you to participate in theatres | 76.7 | 20.9 | 2.4 |
| You feel you are now more likely to enjoy your surgical rotations | 79.5 | 20.5 | 0 |
| You feel more confident in other rotations where such skills are still required e.g., Accident and Emergency or Obstetrics and Gynecology, Dermatology | 79.5 | 20.5 | 0 |
| You feel you are more likely to enjoy other related rotations e.g. suturing in Accident and Emergency or Obstetrics and Gynecology, Dermatology | 86.4 | 13.6 | 0 |
| You feel you could perform some of these skills in theatres unassisted | 52.3 | 31.8 | 15.9 |
Prior to the course, 96% of the students agreed that increased exposure to basic surgical skills before the start of surgical rotations was essential; they also felt that a dedicated skills course would be useful in undergraduate clinical training. After the course, 70% reported that attending such a course could influence future students in their choice of a surgical career, whilst 90% believed it was ideal for integration into the undergraduate curriculum.
Repetitive comments made in the qualitative section of the postcourse questionnaire included suggestions to ‘extend the course to enable further practice of previously taught skills and allow teaching of other surgical suturing skills’; ‘include more technical and general surgical teaching in the “quiet” practice time of the sessions’; that the ‘course should be taught as early as possible before 3rd year (1st clinical year at KCLSM)’; and ‘improve continuity (of learning sessions) with the (same) tutors’ as well as provide ‘more demonstrators’.
DISCUSSION
At present, formal basic surgical skills are taught through RCSENG/intercollegiate licensed BSS courses 12-24 months after completing medical school. These courses, and others such as ATLS, teach basic surgical skill foundations, and are essential for any doctor wishing to pursue a surgical career. In general, the spectrum of skills taught in undergraduate training is limited in comparison. In addition to improving confidence, prior exposure to select skills at an undergraduate level may have an enhanced effect on early post-graduate skill acquisition, and allow more time-efficient training [3]. Because students are technically able to acquire these skills, some postgraduate skills programmes could be instituted into undergraduate curricula.
KCLSM, and a number of other UK medical schools, have adopted a vertically integrated and systems-based teaching approach in recent years, a shift away from the historic clinical and preclinical divide. Early patient contact is intended to provide a clinical perspective and context to basic science teaching and improve confidence prior to the start of clinical rotations. Many of these initiatives, however, target communication and physical examination skills, without a focus on surgical skills. There have been patients have higher expectations of quality and personnel training than in the past in addition to decreased opportunities for teaching by clinical staff. In addition there has been a shift in the culture of medical education away from the apprenticeship model towards competencybased learning and assessment [4].
In current medical school curricula, students typically receive little or no exposure to surgical skills or surgical educators before their surgical rotation in their clinical years [5]. At KCLSM, suturing (instrument tie; interrupted) is taught as part of the 4th year emergency medicine placement and tested in the end-of-year objective structured clinical examination (OSCE) assessment, one year following a student’s clinical surgery rotation. Competency-based training seeks to improve the learning of key clinical skills, but this can only be achieved if the appropriate skills are first identified, taught, practised and then assessed. We believe further integration of basic surgical skills into undergraduate education can be strengthened through specific use of simulation training to introduce and allow practice of these identified specific surgical competencies, prior to their performance in a clinical setting.
This study focused on the impact of a dedicated surgical skills course on medical student confidence during surgical rotations, and the potential influence such a course could have on student attitudes and interests towards a surgical career. To the best of our knowledge, there is no formal BSS programme in undergraduate medical curricula in the UK. The KCLSS BSS course, which began in 2007, is a novel student-led initiative, with input and supervision from surgical trainees at Guy’s and St Thomas’, and King’s College London Hospitals. Our study highlights the benefits and impact that a simple, low fidelity BSS programme can have on medical student confidence and interest in surgery. Prior to enrolling in the course, the students reported low confidence in basic surgical skills, namely suturing, knot tying, tying at depth, and a more complex procedure of chest drain insertion. In spite of the fact that many students had previous operation room experience, only a minority reported having any specific skills teaching or practice. Following course completion, all of the students were markedly more confident and less anxious in performing all four skills. In addition, they were more motivated to be involved in the OR and play a role in the surgical firm.
Importantly, feedback demonstrated that it was feasible to teach both knot tying (basic and at depth) and suturing (skills essential to assist in the theatre as both a student and a junior doctor) to undergraduates, as well as a more complex technique- surgical chest drain insertion. Its complexity lies in teaching correctly both the specific anatomy and technique, but also the indications and potential complications in clinical practice. The students enjoyed the course and strongly believed it was an ideal programme for those interested in surgery. They also felt that being taught by experienced surgical trainees provided them with career insight during skills training.
An important and related issue in teaching surgical skills is that of timing and retention. Ideally the time between instruction and students performing the skill in a clinical setting should be as short as possible [4]. In practice, this is not always possible, as it requires an available supervising surgeon, a suitable patient, and an interested and prepared medical student. One possible solution includes regular practice in a simple BSS course, with the availability of expert assistance allowing for regular feedback and guidance [6]. Subsequently, students can be encouraged to actively seek opportunities to perform these skills clinically when appropriate. Low fidelity simulation programmes, such as our BSS course, not only have a positive impact on skills training, but are also accessible and inexpensive [7]. However, the experience of working on a plastic model is considerably different from performing the same procedure on a human. Ideally, practising on prosthetic bench-top models should be used in the initial training phases, where the main focus is on acquisition of technical aspects of BSS. Such a BSS course could also be integrated into anatomy teaching in the dissection room in the preclinical years, where both technical and practical aspects could be combined and emphasised using cadavers [8]. This would increase the clinical and surgical perspective of anatomy teaching, as well as provide a more contextualised approach to the skills imparted and their practice. For example, in our course, teaching surgical chest drain insertion could be markedly augmented by the select use of cadavers and pro-sections. Such experiences could be re-visited prior to clinical rotations to reinforce parallel training on anatomical plastic models, and would serve as reminders allowing skills practice as near to ‘real’ as possible. This could then be complemented by performing the procedures in a clinical setting under direct supervision by surgical faculty.
There are, however, also benefits for students not as interested in or decided upon, a surgical career. A well-rounded doctor is aware of the technical skills and activities of surgeons, and that the practical side of what they do is important. Basic surgical skills are also useful for all students during their acute care rotations, especially for those interested in allied surgical specialties (e.g., Accident and Emergency [A&E], Dermatology), and even in traditionally non-surgical specialties such as General Practice (GP). Overall 50% of medical students will choose a career in GP [9]. In the current evolution of primary care medicine in UK, the role of the GP with Specialty Interest (GPwSI) physician in Dermatology and Skin Surgery is becoming increasing popular. This has been augmented by a recently updated National Institute for Health and Care Excellence (ICE) and Department of Health (DOH) guidance on skin cancer that allow GPs and GPwSIs with the appropriate skill base to treat low-risk basal cell carcinomas (BCCs) without the need for referral to specialists [10]. Development of surgical skills as undergraduates would thus be useful for the majority of students regardless of their intended career.
For undergraduate students with an interest in surgery, it is potentially their first encounter and interaction with surgical faculty and identification of potential surgical ‘role models’. They can learn and practise skills that will increase their confidence and ability, and ultimately build motivation to be more actively involved as part of the team and in the OR. It provides the student-surgeon with the basic skills and confidence to make the most of, and perform their best during, their surgical rotations.
In conclusion, we have described the effectiveness and success of a simple undergraduate BSS programme in increasing the confidence and motivation of undergraduate medical students interested in surgery as a potential career, in preparation for their surgical rotations and operation room experience. The KCLSS BSS course is a novel student-led initiative that is reproducible and feasible. Student feedback suggests its integration into the undergraduate medical curriculum would be most beneficial and welcomed. The low cost and high benefits of such a programme would make it a logical addition to undergraduate training. Such a course should augment rather than replace clinical learning in order to enhance the learning experience, and ultimately, patient care.
Footnotes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported
SUPPLEMENTARY MATERIAL
Audio recording of the abstract.
REFERENCES
- 1.Wass V. Monitoring the medical education revolution. BMJ. 2003;327:1362. doi: 10.1136/bmj.327.7428.1362. http://dx.doi.org/10.1136/bmj.327.7428.1362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Naylor R a, Hollett L a, Castellvi A, Valentine RJ, Scott DJ. Preparing medical students to enter surgery residencies. Am J Surg. 2010;199:105–109. doi: 10.1016/j.amjsurg.2009.09.003. http://dx.doi.org/10.1016/j.amjsurg.2009.09.003. [DOI] [PubMed] [Google Scholar]
- 3.Sanfey H, Dunnington G. Verification of proficiency: a prerequisite for clinical experience. Surg Clin North Am. 2010;90:559–567. doi: 10.1016/j.suc.2010.02.008. http://dx.doi.org/10.1016/j.suc.2010.02.008. [DOI] [PubMed] [Google Scholar]
- 4.Meyers MO, Meyer AA, Stewart RD, Dreesen EB, Barrick J, Lange PA, Farrell TM. Teaching technical skills to medical students during a surgery clerkship: results of a small group curriculum. J Surg Res. 2011;166:171–175. doi: 10.1016/j.jss.2010.05.019. http://dx.doi.org/ 10.1016/j.jss.2010.05.019. [DOI] [PubMed] [Google Scholar]
- 5.Zaid H, Ward D, Sammann A, Tendick F, Topp KS, Maa J. Integrating surgical skills education into the anatomy laboratory. J Surg Res. 2010;158:36–42. doi: 10.1016/j.jss.2008.08.012. http://dx.doi.org/10.1016/j.jss.2008.08.012. [DOI] [PubMed] [Google Scholar]
- 6.Sadideen H, Kneebone R. Practical skills teaching in contemporary surgical education: how can educational theory be applied to promote effective learning? Am J Surg. 2012;204:396–401. doi: 10.1016/j.amjsurg.2011.12.020. http://dx.doi.org/10.1016/j.amjsurg.2011.12.020. [DOI] [PubMed] [Google Scholar]
- 7.Kneebone R, Arora S, King D, Bello F, Sevdalis N, Kassab E, Aggarwal R, Darzi A, Nestel D. Distributed simulation--accessible immersive training. Med teach. 2010;32:65–70. doi: 10.3109/01421590903419749. http://dx.doi.org/10.3109/01421590903419749. [DOI] [PubMed] [Google Scholar]
- 8.DiMaggio PJ, Waer AL, Desmarais TJ, Sozanski J, Timmerman H, Lopez JA, Poskus DM, Tatum J, Adamas-Rappaport WJ. The use of a lightly preserved cadaver and full thickness pig skin to teach technical skills on the surgery clerkship: a response to the economic pressures facing academic medicine today. Am J Surg. 2010;200:162–166. doi: 10.1016/j.amjsurg.2009.07.039. http://dx.doi.org/10.1016/j.amjsurg.2009.07.039. [DOI] [PubMed] [Google Scholar]
- 9. Royal College of General Practitioners [Internet]. London: Royal College of General Practitioners; [cited 2013 Apr 16]. Available from: http://www.rcgp.org.uk/new_professionals/students.aspx.
- 10. NICE update of guidance on the treatment and care of people with skin cancer May 2010 [Internet]. London: National Institute for Health and Care Excellence; 2010 [cited 2013 June 6] Available from: http://www.nice.org.uk/newsroom/pressreleases/NICEUpdatesSkinCancerGuidance.jsp?domedia=1&mid=CFD181FC-19B9-E0B5-D4A6D733187B4EE6.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Audio recording of the abstract.