

Abstract
Allogeneic hematopoietic stem cell transplantation is a successful treatment for hematologic malignancies and a variety of genetic and metabolic disorders. In the period following stem cell transplantation, the immune-compromised milieu allows opportunistic pathogens to thrive. Epstein-Barr virus-associated post-transplant lymphoproliferative disease can be a life-threatening complication for transplanted patients because of suppressed T-cell-mediated immunity. We analyzed possible risk factors associated with post-transplant lymphoproliferative disease in a cohort of over 1,000 patients. The incidence of post-transplant lymphoproliferative disease was 4%. Significant risk factors identified by multivariate analysis were: human leukocyte antigen-mismatch (P<0.001), serological Epstein-Barr virus mismatch recipient−/donor+ (P<0.001), use of reduced intensity conditioning (P=0.002), acute graft-versus-host disease grade II to IV (P=0.006), pre-transplant splenectomy (P=0.008) and infusion of mesenchymal stromal cells (P=0.015). The risk of post-transplant lymphoproliferative disease has increased in more recent years, from less than 2% before 1998 to more than 6% after 2011. Additionally, we show that long-term survival of patients with post-transplant lymphoproliferative disease is poor despite initial successful treatment. The 3-year survival rate among the 40 patients with post-transplant lymphoproliferative disease was 20% as opposed to 62% among patients without post-transplant lymphoproliferative disease (P<0.001). The study identifies patients at risk of post-transplant lymphoproliferative disease after transplantation in need of pre-emptive measures.
Introduction
Epstein-Barr virus (EBV)-associated post-transplant lymphoproliferative disease (PTLD) is a severe complication after allogeneic hematopoietic stem cell transplantation (SCT).1,2 In immune-competent individuals EBV activity is strictly regulated by specific T cells. In the immune-compromised milieu created by SCT, pathogen control is lost with viral reactivation and viremia as possible results.3 Several risk factors have been associated with PTLD after SCT.1,4 It is particularly common with EBV-related complications when different in vivo T-cell depletion strategies have been used for the prevention of graft-versus-host disease (GVHD) and/or following reduced intensity conditioning (RIC).5,6 This is a reflection of the impaired T-cell-mediated EBV-directed immunity and the presence of residual recipient B cells. A donor/recipient human leukocyte antigen (HLA) mismatch has also been associated with increased risk of PTLD,7 probably due to impaired immune reconstitution. In solid organ transplantation serological donor/recipient mismatch of EBV has been shown to increase the risk of PTLD.8 Primary immunodeficiency as the indication for SCT and older donor age are other previously identified risk factors.4,9,10
Historically PTLD was seen in heavily immunosuppressed solid organ transplant recipients and the primary treatment strategy was reduction of the immunosuppressive treatment.11 Some studies have also suggested the use of chemotherapy, with varying success.12,13 The later introduction of the monoclonal anti-CD20 antibody rituximab has decreased the PTLD mortality rate substantially with the short-term response rate being around 60%.14,15 However, few studies have reported a long enough follow-up of patients after the initial viral clearance.
Second-line treatment with both un-manipulated donor lymphocyte infusion and EBV-specific cytotoxic T-lymphocytes (CTL) has been tried.16–20 If available, the latter is preferable due to the decreased risk of developing GVHD.
The use of adoptive CTL transfer has been shown to be successful in larger cohorts.16,21 However, due to time-limiting factors it is not always possible to infuse EBV-specific CTL before the development of uncontrolled PTLD and subsequent death. Several alternative approaches have been tried in order to decrease the lag time for CTL transfer. Among other things, interferon-gamma capture of virus-specific CTL and allogeneic CTL banks containing CTL against the most common HLA haplotypes have been used with some success.16,22,23 Our group has tried separation of peptide-specific T cells with the help of magnetic beads and MHC multimers.17,18 Even though this has shown promising results, none of these strategies is yet part of standard clinical practice.
In this retrospective analysis we analyzed possible risk factors associated with the development of PTLD after SCT at our center. The earlier part of the cohort of patients was previously included in the studies by Sundin et al. and Omar et al.1,24 We found several factors that were independently associated with an increased risk of PTLD. Some of the factors seem to act synergistically, which adds additional risk of PTLD in the patients. Moreover, in spite of improved prophylaxis and rituximab use, the long-term survival of affected patients is poor.
Methods
Patients
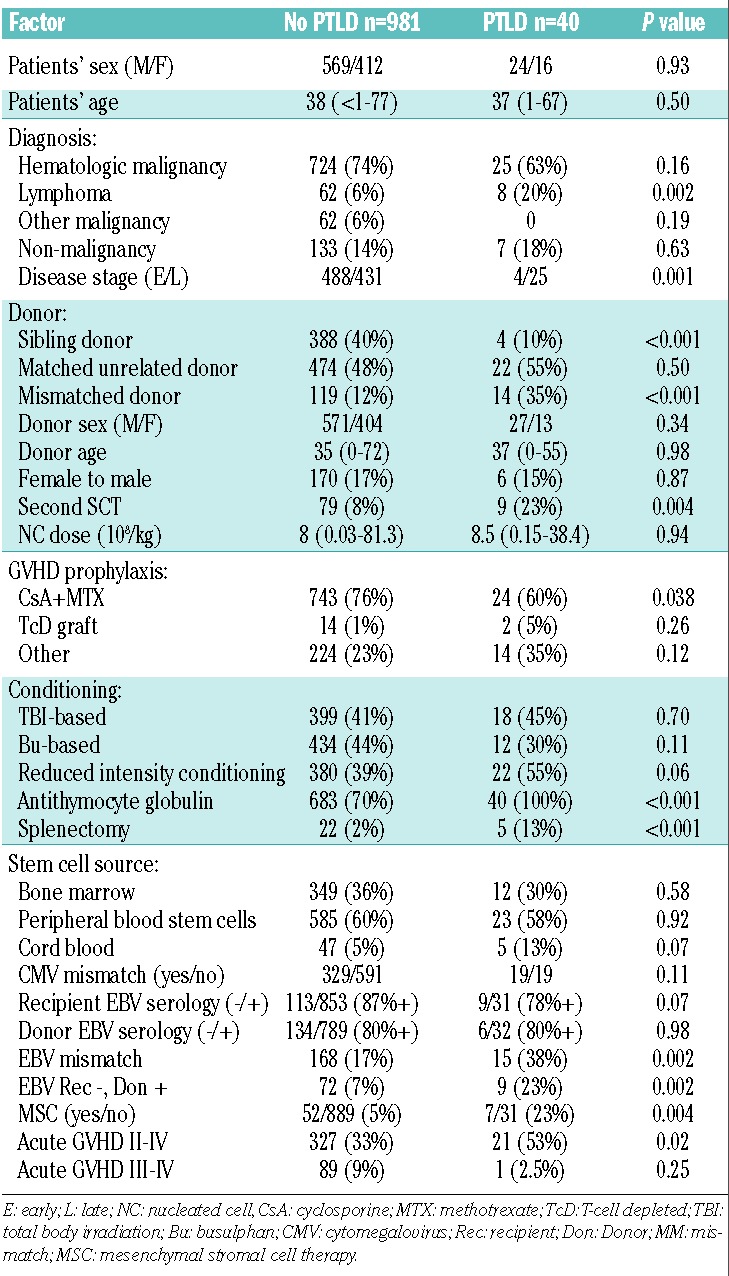
In total 1021 patients who underwent SCT at Karolinska University Hospital in Huddinge, Stockholm, between 1996 and 2011 were included in this retrospective analysis of risk factors for and clinical outcome of PTLD. This study was approved by the regional ethical committee in Stockholm (n. 425/97). A review of patients’ charts and the clinical database identified 40 cases of verified PTLD. The characteristics of patients with and without PTLD are displayed in Table 1.
Table 1.
Patients’ characteristics and univariate analysis.
Diagnosis and treatment of Epstein-Barr virus-associated post-transplant lymphoproliferative disease
The diagnosis of PTLD was made according to the histological criteria reported for B-cell lymphoproliferative states following transplantation.25
After July 2005 (total of 446 individuals) all patients considered to be at high risk of developing PTLD were screened weekly or biweekly for EBV during the first 3 months post-SCT. In patients at low risk, quantitative polymerase chain reaction (PCR) analysis was performed if EBV reactivation was suspected. From July 2005 all patients were treated with rituximab if the EBV load was >10 000 copies/mL.
Thirty-five of the patients were treated with rituximab. More details are available in the Online Supplementary Methods section.
Conditioning regimen, graft-versus-host disease prophylaxis and stem-cell source
RIC was used in 402 patients, while myeloablative conditioning was given to 619 patients. Antithymocyte globulin (ATG) was given to 705 patients as part of the conditioning with the last dose on day −1. ATG was used in all patients with an unrelated or mismatched donor and in all patients with a non-malignant disease, independently of the type of donor. A few patients with a sibling donor treated with RIC (n=44) were also given ATG. The graft source was bone marrow in 361 cases, peripheral blood in 608 and umbilical cord blood in 52. For more details regarding conditioning regimens, GVHD prophylaxis and stem-cell source see the Online Supplementary Methods section.
Statistics
Overall survival was calculated using the Kaplan-Meier method and compared with the log-rank test. Survival time was calculated from the day of transplantation until death or last follow-up. The incidence of PTLD was estimated using an estimator of cumulative incidence curves. Death without PTLD was considered as a competing event. Predictive analyses for PTLD were based on the proportional hazard model for sub-distribution of competing risk. Univariate and multivariate analyses were then performed using the Gray test and the proportional sub-distribution hazard regression model of Fine and Gray.26 A stepwise backward procedure was used to construct a set of independent predictors. All predictors with a P-value below 0.10 were considered and sequentially removed if the P-value in the multiple model was above 0.05. All tests were two-sided. The type I error rate was fixed at 0.05 for factors potentially associated with time-to-event outcomes. Several factors were analyzed in the univariate analysis (Online Supplementary Methods). Time-dependent variables were only included if they occurred before the diagnosis of PTLD (minimum interval >1 week). Categorical parameters were compared using the χ2 test and continuous variables were compared using the Mann-Whitney test. Analyses were performed using the cmprsk package (developed by Gray, June 2001), Splus 6.2 software and Statistica software.
Results
Incidence of post-transplant lymphoproliferative disease
PTLD was diagnosed in 40 (4%) of the 1021 patients transplanted between 1996 and 2011 (Figure 1). The median time of PTLD onset was 71 (range, 38–1199) days post-SCT. In 30 (75%) patients, the PTLD occurred within 100 days after SCT. The majority (93%) of the PTLD diagnoses were based on positive PCR of EBV in peripheral blood in combination with an EBV-positive biopsy, whereas in the remaining the diagnosis was clinical and corroborated with computed tomography scans. All patients with PTLD, in contrast to 70% of the unaffected patients, had received ATG as GVHD prophylaxis. In the PTLD group 23% received infusions of mesenchymal stromal cells (MSC) at the time of hematopoietic stem cell infusion as support of engraftment and GVHD prophylaxis, or as salvage therapy of GVHD or hemorrhagic cystitis treatment. Only 5% of the patients without PTLD received MSC (Table 1).
Figure 1.
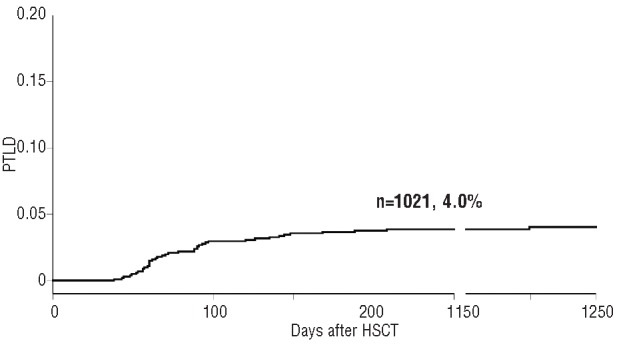
Incidence of PTLD in 1021 patients transplanted between 1996 and 2012.
Univariate analysis of risk factors for post-transplant lymphoproliferative disease
In the univariate analysis 11 factors that had a significant association with PTLD after SCT were identified. In order of significance level, these factors were: ATG as GVHD prophylaxis (P<0.001), splenectomy (P<0.001), HLA-identical non-sibling donor (P<0.001), HLA-mismatched donor (P<0.001), lymphoma (P=0.002), EBV serological mismatch (P=0.002), EBV recipient-negative/donor-positive (P=0.002), use of MSC (P=0.004), second SCT (P=0.004), acute GVHD grades II–IV (P=0.02) and not using cyclosporine A and methotrexate as GVHD prophylaxis (P=0.038). Factors with a statistical trend were the use of RIC (P=0.06), cord blood grafts (P=0.07) and negative recipient EBV serology (P=0.07) (Table 1). The splenectomized patients had the following indications for SCT: non-malignant disease (n=3), acute leukemia (n=4), lymphoma (n=10), chronic lymphocytic leukemia (n=2), myelodysplastic syndrome (n=6) and solid tumor (n=2).
Multivariate analysis of risk factors for post-transplant lymphoproliferative disease
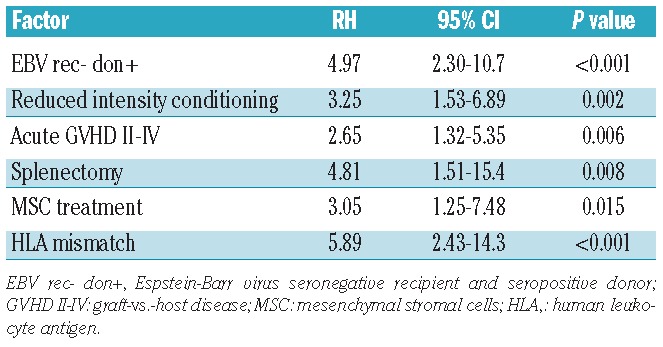
A multivariate analysis identified six significant risk factors for PTLD after SCT. The risk factors, ordered in degree of significance, were: HLA-mismatch, serological EBV mismatch recipient-negative/donor-positive, use of RIC, the appearance of acute GVHD grades II–IV, splenectomy prior to SCT and the infusion of MSC (Table 2). All patients developing PTLD also received ATG; consequently, this factor had to be excluded, otherwise it would have interfered with the further multivariate analysis. The statistical software is not able to calculate correct predictions if all PTLD patients are positive for one factor (i.e. ATG in this case).
Table 2.
Multivariate analysis of risk factors for EBV-PTLD after hematopoietic stem cell transplantation.
Risk factors and the cumulative incidence of post-transplant lymphoproliferative disease
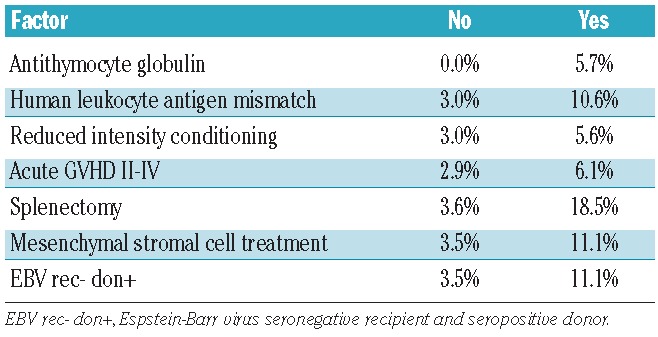
The cumulative incidences of PTLD in patients with and without the risk factors found in the multivariate analysis are shown in Table 3.
Table 3.
Cumulative incidence of PTLD for the risk factors found in multivariate analysis.
After correction for multiple comparisons, EBV recipient-negative/donor-positive (P=0.002), RIC (P=0.034) and HLA mismatch (P<0.001) remained statistically significant factors associated with PTLD.
We also performed a multivariate analysis stratified for SCT before or after 2005, which showed no major difference compared to the non-stratified analysis regarding risk factors, incidence and outcome after PTLD. The reason for applying this time period cutoff was the introduction of routine PCR monitoring of patients at high risk of developing PTLD.
To illustrate the impact of several simultaneous risk factors on PTLD incidence, a risk factor index was created comparing the risk for patients developing PTLD dependent on how many risk factors they had. The seven included risk factors were the ones found to be statistically significant in the multivariate analysis (Table 3). In individuals with one risk factor (ATG included) the cumulative incidence of PTLD was 0.4%. For individuals with two risk factors the incidence increased to 3.0%. For patients with three, four and five risk factors the cumulative incidences were 10.4%, 26.5% and 40%, respectively (Figure 2). None of the patients was found to have six or seven risk factors simultaneously.
Figure 2.
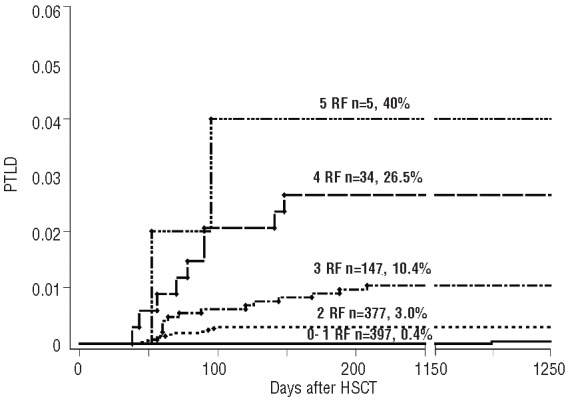
Risk of PTLD after allogeneic stem cell transplantation according to number of risk factors (RF) identified in multivariate analysis. Categories; 0–1, 2, 3, 4 or 5 risk factors.
Development of post-transplant lymphoproliferative disease over time
Survival after allogeneic SCT has been reported, by our and other centers, to have increased during the last decade.27 It was, therefore, of interest to study the incidence of PTLD with regard to the year of transplantation. We divided the time-period into six 3-year intervals starting from 1996 (Figure 3A). We observed a significant increase in the cumulative incidence of PTLD in 2011–2012 compared to that in the earliest periods studied, 1996–98 and 1999–01 (Figure 3A). When studying the incidence of risk factors during the different time periods it became clear that the majority of this increase is due to the extended use of RIC in the later time periods. The decreases in the number of patients with mismatches in MHC or recipient-negative/donor-positive EBV serology in later years were also notable (Figure 3B).
Figure 3.
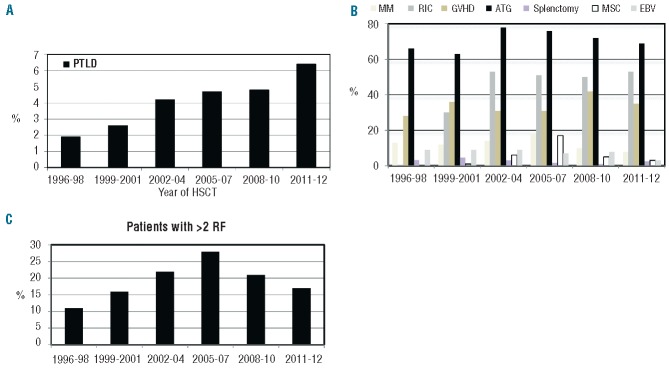
Incidence of PTLD and frequencies of risk factors over time. (A) Incidence of PTLD in percentage divided in the indicated time periods. (B) The frequency of identified risk factors (RF) in the patients during the indicated time periods. Chosen risk factors were found to be statistically significant in multivariate analysis. MM denotes HLA mismatch; RIC, reduced intensity conditioning; GVHD, graft-vs.-host disease grade II–IV; MSC, mesenchymal stromal cell treatment; EBV, EBV serology mismatch. (C) The frequency of patients with more than two risk factors in the indicated time periods.
Treatment and outcome of post-transplant lymphoproliferative disease
Many studies have described a response rate for viral clearance with rituximab of over 50%, but few have reported on long-term survival.15,16 The survival rates for patients who developed PTLD in this study were 28%, 23% and 20% at 1, 2 and 3 years after SCT, respectively (Figure 4). The survival rate at 100 days after the diagnosis of PTLD was 33%. There was no significant difference between patients diagnosed with PTLD early or late in the period studied (1996–2004 compared to 2005–2012). Thirty-two of the 40 patients (80%) with PTLD died, and the median time to death was 16 days (range, 0–674) after development of PTLD. PTLD was the primary or contributing cause of death in 26 patients (81%), while two patients died from relapse, three of other infections and one patient died of cerebral hemorrhage. All received rituximab except five patients (diagnosed between 1996 and 2004). One of these five patients was diagnosed with PTLD post-mortem while the others were diagnosed before the introduction of rituximab therapy. Eight patients were treated with donor lymphocyte infusion and eight patients with virus-specific T cells. Four of the virus-specific T-cell products were prepared from donor blood by repetitive stimulation with lymphoblastoid cell lines.20 In one patient the cells were obtained from an allogeneic CTL bank.22 In two patients the T cells were purified from haplo-identical relatives by the interferon-gamma capture technique. One patient received T cells, obtained by separation by MHC-multimers and magnetic beads, from the haploidentical mother.17
Figure 4.
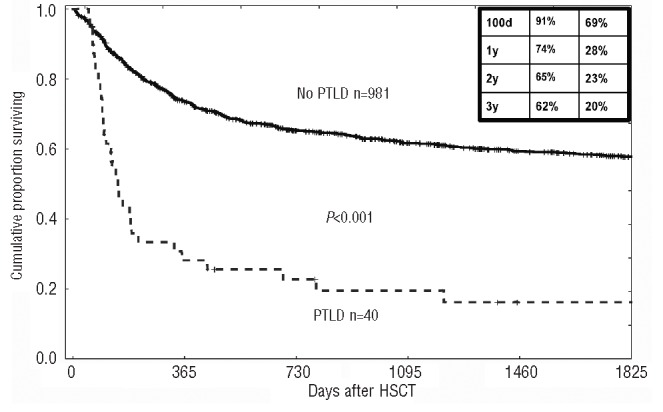
Cumulative survival of patients with (dotted line) our without (solid line) diagnosed PTLD.
In order to investigate the efficacy of different PTLD treatments, the patients were divided into groups depending on treatment strategy. Five patients did not receive rituximab, 21 patients received only rituximab and 14 individuals received rituximab and additional treatment (chemotherapy, donor lymphocyte infusion or virus-specific CTL). The rates of complete response (defined according to Cheson et al.28) were 0% for patients with no treatment, 29% in the rituximab group and 50% for those receiving rituximab with additional treatment (P=0.11). The 1-year overall survival rates in the corresponding groups were 20%, 24% and 40%, respectively (P>0.5).
Discussion
EBV-PTLD is a result of SCT-induced compromised virus-specific immunity.29 RIC in combination with in vivo or ex vivo T-cell depletion has been shown to be a particularly important risk factor.1,30 This is logical since the natural site of EBV tropism is B cells. After RIC these lymphocytes have a prolonged period to undergo virus-driven blast cell transformation in the absence of the normally strictly regulated control from EBV-specific T cells. This previous finding was confirmed in our study by the multivariate statistical analysis (Table 3). Our study also verifies other earlier reported risk factors for PTLD after SCT, e.g. mismatches in HLA and serological EBV status between donor and recipient.1,7 These two factors were highly significant in our study also after multivariate analysis (Table 3).
Acute GVHD is a known risk factor for PTLD due to the impairment in specific immune responses induced by the pro-inflammatory cytokine storm.31 The chronic antigen stimulation seen in GVHD and the use of profound immunosuppressive treatment probably contribute as risk factors for PTLD. It was not possible to evaluate the role of chronic GVHD as only ten cases of PTLD occurred later than 100 days after SCT and some of the cases occurred before chronic GVHD developed.
The use of ATG is a known risk factor for PTLD. ATG is used with the aim of reducing the risk of graft rejection and GVHD by in vivo removal of both recipient and donor T cells. This will immunosuppress the patient paving the way for EBV reactivation and PTLD. In our study all patients with PTLD had received ATG which made it impossible to include this factor in the multivariate analysis. No correlation was found between any specific brand of ATG and the development of PTLD.
In agreement with the findings of our previous study, splenectomy was a significant risk factor for EBV-PTLD.1 Patients with lymphoma as the indication for SCT are often splenectomized prior to the transplant. Lymphoma, itself, as a risk factor for PTLD was only demonstrated by univariate analysis in the present study, in contrast to splenectomy which was also found to be significant by multivariate analysis. This may argue for a distinct role of the spleen per se in the control of PTLD. The spleen is an important part of the immune system, especially with regards to humoral immunity. In addition to T-cell immunity, there might be a role for B cells and immunoglobulins in the defense against EBV.32 Recent studies have re-discovered other B-cell related functions.33 Certain B-cell sub-populations, such as CD5+ B-1 cells, are dependent on, and reside almost exclusively in the spleen. CD5+ B-cells are not only responsible for T-cell-independent antibody production, but also for important immune regulatory functions.34 A potential scenario is that CD5+ maintenance is impaired in patients after splenectomy and the regulatory B-cell function may, therefore, also be impaired, resulting in increased EBV-blast expansion.
MSC, which have an immune inhibiting effect,35 were also identified as a separate risk factor for PTLD in both our univariate and multivariate statistical analyses. EBV-PTLD was earlier reported in a patient who was treated with MSC for chronic GVHD and the possibility of MSC-induced EBV PTLD was discussed in this context.36 MSC have been used to treat GHVD, as attempts to treat hemorrhagic cystitis, and to support hematopoietic engraftment.37–39 Results of an in vitro study suggested that MSC selectively inhibit allo-induced CTL, but not EBV-specific CTL.40 This has not, however, been verified in vivo. In addition to the immunosuppressive effect of MSC infusions as an explanation for the increased risk of PTLD, a stimulatory effect on the EBV-transformed blast cells could also be considered in analogy with bone marrow stromal cells supporting B-cell development.41,42
Serological EBV mismatch between donor and recipient has been shown to be a risk factor for EBV-PTLD after solid organ transplantation.8 The risk following SCT is not as clear, with some studies favoring this,1 and others failing to find the association.43 Both after solid organ transplantation and SCT, an EBV-negative recipient and an EBV-positive donor is the most unfavorable combination with regards to the risk of EBV-PTLD1,8 (Table 2).
The overall frequency of PTLD in our cohort was 4% which is in line with some of the earlier reports.1,44 It is interesting that the incidence of PTLD has increased with time (Figure 3). Large parts of this increase can probably be explained by the introduction of RIC (Figure 3B). Additional explanations may be the increased awareness regarding EBV-driven PTLD and the easy availability of PCR for monitoring.24 It is likely that PTLD was somewhat under-diagnosed in our institute before 2003, when routine PCR monitoring was introduced.
The introduction of rituximab has decreased the short-term mortality in patients with PTLD, but reports on long-term follow-up are lacking in the literature. In our cohort only 28% of patients with PTLD were alive 1 year after diagnosis (Figure 4). Thirty-five patients (88%) were treated with rituximab according to the standard protocol. In addition, ten and seven patients were treated with EBV-specific CTL or donor lymphocyte infusion, respectively, alone or in combination with rituximab.
No significant differences were found between survival rates of PTLD patients who were untreated, treated with rituximab or treated with rituximab in combination with other therapies. This apparent lack of impact of treatment is probably an effect of the small sample size. When assessing the response rate and actual survival rates in the different groups they showed rather different patterns.
It is clear from our data that even if rituximab initially resolves the PTLD in most cases, a considerable proportion of patients still eventually succumb from other causes. Whether this meager long-term survival mirrors a poor immune reconstitution in these individuals and/or additional suppression due to the PTLD treatment strategy is difficult establish. It does, however, illustrate that these individuals would benefit from pre-emptive measures rather than therapeutic ones. Pre-emptive therapy with rituximab has been elegantly used to inhibit viral EBV reactivation and prevent or treat PTLD.14,15 The increased risk of PTLD in individuals with multiple risk factors is clearly shown in our cohort, in which patients with more than three risk factors had a 26.5% probability of developing PTLD (Figure 2). This is a highly relevant and manageable group to select for future pre-emptive measures, such as rituximab and EBV-specific CTL if possible.
Supplementary Material
Acknowledgments
This study was supported by the Signe and Olof Wallenius Foundation, the Foundation Olle Engkvist Byggmästare, the Swedish Childhood Cancer Foundation (proj12/006), the Swedish Research Council (VR) (2011–2377), the Swedish Society for Medical Research (SSMF), Stockholm County Council and Karolinska Institutet.
Footnotes
The online version of this article has a Supplementary Appendix.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Sundin M, Le Blanc K, Ringden O, Barkholt L, Omazic B, Lergin C, et al. The role of HLA mismatch, splenectomy and recipient Epstein-Barr virus seronegativity as risk factors in post-transplant lymphoproliferative disorder following allogeneic hematopoietic stem cell transplantation. Haematologica. 2006;91(8):1059–67 [PubMed] [Google Scholar]
- 2.Heslop HE. How I treat EBV lymphoproliferation. Blood. 2009;114(19):4002–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Christopeit M, Janssen N, Weber T, Bacher U, Lautenschlager C, Oehme A, et al. Cyclosporine area under the curve after allogeneic hematopoietic stem cell transplantation is an indicator of Epstein-Barr virus DNAemia. Leuk Lymphoma. 2013;54(1):133–7 [DOI] [PubMed] [Google Scholar]
- 4.Juvonen E, Aalto SM, Tarkkanen J, Volin L, Mattila PS, Knuutila S, et al. High incidence of PTLD after non-T-cell-depleted allogeneic haematopoietic stem cell transplantation as a consequence of intensive immunosuppressive treatment. Bone Marrow Transplant. 2003;32(1):97–102 [DOI] [PubMed] [Google Scholar]
- 5.Cohen J, Gandhi M, Naik P, Cubitt D, Rao K, Thaker U, et al. Increased incidence of EBV-related disease following paediatric stem cell transplantation with reduced-intensity conditioning. Br J Haematol. 2005;129(2):229–39 [DOI] [PubMed] [Google Scholar]
- 6.Brunstein CG, Weisclorf DJ, DeFor T, Barker JN, Tolar J, van Burik JAH, et al. Marked increased risk of Epstein-Barr virus-related complications with the addition of antithymocyte globulin to a nonmyeloablative conditioning prior to unrelated umbilical cord blood transplantation. Blood. 2006;108(8): 2874–80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cockfield SM. Identifying the patient at risk for post-transplant lymphoproliferative disorder. Transpl Infect Dis. 2001;3(2):70–8 [DOI] [PubMed] [Google Scholar]
- 8.Walker RC, Marshall WF, Strickler JG, Wiesner RH, Velosa JA, Habermann TM, et al. Pretransplantation assessment of the risk of lymphoproliferative disorder. Clin Infect Dis. 1995;20(5):1346–53 [DOI] [PubMed] [Google Scholar]
- 9.Gross TG, Steinbuch M, DeFor T, Shapiro RS, McGlave P, Ramsay NK, et al. B cell lymphoproliferative disorders following hematopoietic stem cell transplantation: risk factors, treatment and outcome. Bone Marrow Transplant. 1999;23(3):251–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gerritsen EJ, Stam ED, Hermans J, van den Berg H, Haraldsson A, van Tol MJ, et al. Risk factors for developing EBV-related B cell lymphoproliferative disorders (BLPD) after non-HLA-identical BMT in children. Bone Marrow Transplant. 1996;18(2):377–82 [PubMed] [Google Scholar]
- 11.Reshef R, Vardhanabhuti S, Luskin MR, Heitjan DF, Hadjiliadis D, Goral S, et al. Reduction of immunosuppression as initial therapy for posttransplantation lymphoproliferative disorder. Am J Transplant. 2011;11 (2):336–47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fohrer C, Caillard S, Koumarianou A, Ellero B, Woehl-Jaegle ML, Meyer C, et al. Long-term survival in post-transplant lymphoproliferative disorders with a dose-adjusted ACVBP regimen. Br J Haematol. 2006;134(6): 602–12 [DOI] [PubMed] [Google Scholar]
- 13.Choquet S, Trappe R, Leblond V, Jager U, Davi F, Oertel S. CHOP-21 for the treatment of post-transplant lymphoproliferative disorders (PTLD) following solid organ transplantation. Haematologica. 2007;92(2):273–4 [DOI] [PubMed] [Google Scholar]
- 14.Messahel B, Taj MM, Hobson R, Hadzic N, Ramsay A, Hann I, et al. Single agent efficacy of rituximab in childhood immunosuppression related lymphoproliferative disease: a United Kingdom Children’s Cancer Study Group (UKCCSG) retrospective review. Leuk Lymphoma. 2006;47(12):2584–9 [DOI] [PubMed] [Google Scholar]
- 15.Styczynski J, Einsele H, Gil L, Ljungman P. Outcome of treatment of Epstein-Barr virus-related post-transplant lymphoproliferative disorder in hematopoietic stem cell recipients: a comprehensive review of reported cases. Transpl Infect Dis. 2009;11(5):383–92 [DOI] [PubMed] [Google Scholar]
- 16.Haque T, Wilkie GM, Jones MM, Higgins CD, Urquhart G, Wingate P, et al. Allogeneic cytotoxic T-cell therapy for EBV-positive posttransplantation lymphoproliferative disease: results of a phase 2 multicenter clinical trial. Blood. 2007;110(4):1123–31 [DOI] [PubMed] [Google Scholar]
- 17.Uhlin M, Okas M, Gertow J, Uzunel M, Brismar TB, Mattsson J. A novel haplo-identical adoptive CTL therapy as a treatment for EBV-associated lymphoma after stem cell transplantation. Cancer Immunol Immunother. 2010;59(3):473–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Uhlin M, Gertow J, Uzunel M, Okas M, Berglund S, Watz E, et al. Rapid salvage treatment with virus-specific T-cells for therapy-resistant disease. Clin Infect Dis. 2012; 55(8):1064–73 [DOI] [PubMed] [Google Scholar]
- 19.De Pasquale MD, Mastronuzzi A, De Vito R, Cometa A, Inserra A, Russo C, et al. Unmanipulated donor lymphocytes for EBV-related PTLD after T-cell depleted HLA-haploidentical transplantation. Pediatrics. 2012; 129(1):e189–94 [DOI] [PubMed] [Google Scholar]
- 20.Gustafsson A, Levitsky V, Zou JZ, Frisan T, Dalianis T, Ljungman P, et al. Epstein-Barr virus (EBV) load in bone marrow transplant recipients at risk to develop posttransplant lymphoproliferative disease: prophylactic infusion of EBV-specific cytotoxic T cells. Blood. 2000;95(3):807–14 [PubMed] [Google Scholar]
- 21.Rooney CM, Smith CA, Ng CY, Loftin SK, Sixbey JW, Gan Y, et al. Infusion of cytotoxic T cells for the prevention and treatment of Epstein-Barr virus-induced lymphoma in allogeneic transplant recipients. Blood. 1998;92 (5):1549–55 [PubMed] [Google Scholar]
- 22.Haque T, Wilkie GM, Taylor C, Amlot PL, Murad P, Iley A, et al. Treatment of Epstein-Barr-virus-positive post-transplantation lymphoproliferative disease with partly HLA-matched allogeneic cytotoxic T cells. Lancet. 2002;360(9331):436–42 [DOI] [PubMed] [Google Scholar]
- 23.Moosmann A, Bigalke I, Tischer J, Schirrmann L, Kasten J, Tippmer S, et al. Effective and long-term control of EBV PTLD after transfer of peptide-selected T cells. Blood. 2010;115(14):2960–70 [DOI] [PubMed] [Google Scholar]
- 24.Omar H, Hagglund H, Gustafsson-Jernberg A, LeBlanc K, Mattsson J, Remberger M, et al. Targeted monitoring of patients at high risk of post-transplant lymphoproliferative disease by quantitative Epstein-Barr virus polymerase chain reaction. Transpl Infect Dis. 2009;11(5):393–9 [DOI] [PubMed] [Google Scholar]
- 25.Loren AW, Porter DL, Stadtmauer EA, Tsai DE. Post-transplant lymphoproliferative disorder: a review. Bone Marrow Transplant. 2003;31(3):145–55 [DOI] [PubMed] [Google Scholar]
- 26.Fine J, Gray R. Proportional hazard model for the sub-distribution of competing risks. J Am Stat Assoc. 1999;94:496–509 [Google Scholar]
- 27.Remberger M, Ackefors M, Berglund S, Blennow O, Dahllof G, Dlugosz A, et al. Improved survival after allogeneic hematopoietic stem cell transplantation in recent years. A single-center study. Biol Blood Marrow Transplant. 2011;17(11):1688–97 [DOI] [PubMed] [Google Scholar]
- 28.Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25(5):579–86 [DOI] [PubMed] [Google Scholar]
- 29.Shapiro RS, McClain K, Frizzera G, Gajl- Peczalska KJ, Kersey JH, Blazar BR, et al. Epstein-Barr virus associated B cell lymphoproliferative disorders following bone marrow transplantation. Blood. 1988;71(5):1234–43 [PubMed] [Google Scholar]
- 30.Peric Z, Cahu X, Chevallier P, Brissot E, Malard F, Guillaume T, et al. Features of Epstein-Barr Virus (EBV) reactivation after reduced intensity conditioning allogeneic hematopoietic stem cell transplantation. Leukemia. 2011;25(6):932–8 [DOI] [PubMed] [Google Scholar]
- 31.Curtis RE, Travis LB, Rowlings PA, Socie G, Kingma DW, Banks PM, et al. Risk of lymphoproliferative disorders after bone marrow transplantation: a multi-institutional study. Blood. 1999;94(7):2208–16 [PubMed] [Google Scholar]
- 32.Abedi MR, Linde A, Christensson B, Mackett M, Hammarstrom L, Smith CI. Preventive effect of IgG from EBV-seropositive donors on the development of human lymphoproliferative disease in SCID mice. Int J Cancer. 1997;71(4):624–9 [DOI] [PubMed] [Google Scholar]
- 33.Mauri C, Bosma A. Immune regulatory function of B cells. Annu Rev Immunol. 2012;30: 221–41 [DOI] [PubMed] [Google Scholar]
- 34.Gary-Gouy H, Harriague J, Bismuth G, Platzer C, Schmitt C, Dalloul AH. Human CD5 promotes B-cell survival through stimulation of autocrine IL-10 production. Blood. 2002;100(13):4537–43 [DOI] [PubMed] [Google Scholar]
- 35.Le Blanc K, Ringden O. Immunobiology of human mesenchymal stem cells and future use in hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2005;11 (5):321–34 [DOI] [PubMed] [Google Scholar]
- 36.Ringden O, Uzunel M, Rasmusson I, Remberger M, Sundberg B, Lonnies H, et al. Mesenchymal stem cells for treatment of therapy-resistant graft-versus-host disease. Transplantation. 2006;81(10):1390–7 [DOI] [PubMed] [Google Scholar]
- 37.Le Blanc K, Frassoni F, Ball L, Locatelli F, Roelofs H, Lewis I, et al. Mesenchymal stem cells for treatment of steroid-resistant, severe, acute graft-versus-host disease: a phase II study. Lancet. 2008;371(9624):1579–86 [DOI] [PubMed] [Google Scholar]
- 38.Le Blanc K, Samuelsson H, Gustafsson B, Remberger M, Sundberg B, Arvidson J, et al. Transplantation of mesenchymal stem cells to enhance engraftment of hematopoietic stem cells. Leukemia. 2007;21(8):1733–8 [DOI] [PubMed] [Google Scholar]
- 39.Ringden O, Uzunel M, Sundberg B, Lonnies L, Nava S, Gustafsson J, et al. Tissue repair using allogeneic mesenchymal stem cells for hemorrhagic cystitis, pneumomediastinum and perforated colon. Leukemia. 2007;21(11): 2271–6 [DOI] [PubMed] [Google Scholar]
- 40.Karlsson H, Samarasinghe S, Ball LM, Sundberg B, Lankester AC, Dazzi F, et al. Mesenchymal stem cells exert differential effects on alloantigen and virus-specific T-cell responses. Blood. 2008;112(3):532–41 [DOI] [PubMed] [Google Scholar]
- 41.Tokoyoda K, Hauser AE, Nakayama T, Radbruch A. Organization of immunological memory by bone marrow stroma. Nat Rev Immunol. 2010;10(3):193–200 [DOI] [PubMed] [Google Scholar]
- 42.Moser K, Tokoyoda K, Radbruch A, MacLennan I, Manz RA. Stromal niches, plasma cell differentiation and survival. Curr Opin Immunol. 2006;18(3):265–70 [DOI] [PubMed] [Google Scholar]
- 43.Hoegh-Petersen M, Goodyear D, Geddes MN, Liu S, Ugarte-Torres A, Liu Y, et al. High incidence of post transplant lymphoproliferative disorder after antithymocyte globulin-based conditioning and ineffective prediction by day 28 EBV-specific T lymphocyte counts. Bone Marrow Transplant. 2011;46(8):1104–12 [DOI] [PubMed] [Google Scholar]
- 44.Immunotherapy with Mycobacterium vaccae in patients with newly diagnosed pulmonary tuberculosis: a randomised controlled trial. Durban Immunotherapy Trial Group Lancet. 1999;354(9173):116–9 [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.