

Abstract
Suspected transient ischaemic attack (TIA) is a common diagnostic challenge for physicians in neurology, stroke, general medicine and primary care. It is essential to identify TIAs promptly because of the very high early risk of ischaemic stroke, requiring urgent investigation and preventive treatment. On the other hand, it is also important to identify TIA ‘mimics’, to avoid unnecessary and expensive investigations, incorrect diagnostic labelling and inappropriate long-term prevention treatment. Although the pathophysiology of ischaemic stroke and TIA is identical, and both require rapid and accurate diagnosis, the differential diagnosis differs for TIA owing to the transience of symptoms. For TIA the diagnostic challenge is greater, and the ‘mimic’ rate higher (and more varied), because there is no definitive diagnostic test. TIA heralds a high risk of early ischaemic stroke, and in many cases the stroke can be prevented if the cause is identified, hence the widespread dissemination of guidelines including rapid assessment and risk tools like the ABCD2 score. However, these guidelines do not emphasise the substantial challenges in making the correct diagnosis in patients with transient neurological symptoms. In this article we will mainly consider the common TIA mimics, but also briefly mention the rather less common situations where TIAs can look like something else (‘chameleons’).
Keywords: stroke, cerebrovascular disease, diagnosis
Definition and pathophysiology
TIA is defined as temporary focal neurological symptoms resulting from cerebral, retinal—or, very occasionally, spinal—ischaemia. The concept of TIA emerged in the 1950s, with the observation by C Miller Fisher, and others, that ischaemic stroke often followed transient neurological symptoms in the same arterial territory. An arbitrary maximum duration of 24 h for TIA is now recognised to be unhelpful—and should be abandoned—for the following reasons: up to 50% of TIAs, including brief attacks (minutes), can be associated with infarction on diffusion-weighted MRI; acute ischaemic stroke requires urgent treatment within minutes, and certainly long before 24 h; and the vast majority of TIAs last well under an hour (usually less than 30 min). More recently, the American Heart Association recommended a ‘tissue-based’ definition of TIA: “a transient episode of neurological dysfunction caused by a focal brain, spinal cord, or retinal ischaemia, without acute infarction”.1 This definition usefully eliminates the 24-h time limit, but is highly dependent on timely access to diagnostic tests (mainly MRI), which is hugely variable, even in developed countries like the UK. Thus, for the moment, TIA remains a clinical diagnosis based around accurate history interpretation skills.2 With regard to patient pathways, the most important distinction is not between TIA and stroke, but between TIA and disabling stroke, or between non-disabling stroke (which can be managed in an outpatient setting) and disabling stroke (which is usually managed as an inpatient stay).
Like ischaemic strokes, TIAs are due to locally decreased blood flow to the brain, causing focal neurological symptoms. Decreased blood flow results from either embolism into a cerebral supply artery (from the heart, or the great proximal vessels, extracranial or intracranial arteries, usually affected by atherosclerosis), or in situ occlusion of small perforating arteries; resolution of symptoms probably occurs by spontaneous lysis or distal passage of the occluding thrombus or embolus, or by compensation through collateral circulation restoring perfusion into the ischaemic brain area. Rarely, focal hypoperfusion due to critical arterial stenosis can cause TIA, often stereotyped and related to upright posture. Blood pressure and blood oxygenation or viscosity may also impact upon the duration and pattern of symptom evolution or resolution.
Specific challenges in diagnosing TIA
The main diagnostic challenge of TIA is that the symptoms and signs have usually resolved by the time of assessment.3 There is no test for TIA: the gold standard remains assessment as soon as possible by a clinical expert. The diagnosis relies heavily on the patient's account of their history and on expert interpretation of that history. Interobserver agreement for the diagnosis of TIA between different stroke-trained physicians and non-neurologists is poor.4–7 As in stroke, in some patients a collateral history may be essential.
Subsequent stroke risk and importance of accurate diagnosis
Patients with a diagnosis of TIA have an increased risk of future ischaemic stroke. Fifteen per cent to 30% of ischaemic strokes are preceded by TIA symptoms, often on the same day.8 A meta-analysis found a cumulative early risk at 7 days of 5.2%.9 The risk of stroke is highest within the first 24 h,10 so prompt and accurate diagnosis is critical11; misdiagnosis can expose patients to unnecessary investigation and long-term secondary prevention treatment, as well as anxiety.12
The ABCD2 score (which includes age, blood pressure, clinical features, duration and diabetes) is a popular clinical prediction tool used to identify those patients with suspected TIA at high risk of developing early ischaemic stroke,3 but may not always be used appropriately. It is of limited practical relevance in modern stroke clinical practice, since the aspiration is to see all patients with suspected TIA within 24 h. The ABCD2 is not designed as—and should not be used as—a diagnostic instrument, although a high ABCD2 score may predict subsequent stroke, in part because such patients are more likely to have had a TIA rather than a mimic.3 13 14 The ABCD2 score does not include other known predictors of high stroke risk, including carotid disease, recurrent TIAs and evidence of tissue damage on MRI.15 Finally, the validity of the ABCD2 score in the hands of general practitioners and other non-stroke doctors may be limited and is not extensively studied.
Role of brain imaging in TIA
Even transient deficits can be associated with evidence of persistent tissue ischaemia on diffusion-weighted imaging (DWI). In those cases, positive DWI supports a clinical diagnosis of TIA. In early series, 35–67% of patients with TIAs had restricted diffusion suggesting cerebral ischaemic injury.16 The likelihood of a DWI lesion increases with symptom duration. Recent risk scores incorporating DWI suggest that this imaging modality can help to identify individuals at highest risk of early ischaemic stroke.15
Clinical features of TIA
The key rule here is that symptoms of TIA should mimic known stroke syndromes, and so depend on the arterial territory involved. Distinguishing the territory is important to guide further investigation and secondary prevention. Some common patterns of presentation (eg, hemiparesis) are not very helpful in distinguishing the arterial territory, as they can occur with both anterior and posterior circulation TIAs. Others can be more localising: for example, aphasia or transient monocular visual loss suggest carotid territory ischaemia, while bilateral limb weakness, vertigo, hearing loss, haemianopia or diplopia are features of vertebrobasilar (brainstem) ischaemia. TIAs due to perforating artery disease should mimic a known lacunar syndrome (most often hemisensory or hemimotor symptoms affecting the face, arm and leg); moreover, such ‘lacunar’ TIAs may be recurrent and stereotyped over a short period (days) as in the “capsular warning syndrome”. Increased awareness of symptoms means that patients can now present with very restricted transient syndromes, including isolated vertigo, dysarthria or hemisensory disturbance: in such cases, clinicians should consider other causes before diagnosing TIA.
Abrupt onset of maximal symptoms predicts a final diagnosis of TIA,12 but there is no evidence for a statistical difference between duration of symptoms in patients with TIA and mimics.14 These findings may of course be rather circular, since sudden symptoms are part of the usual criteria for diagnosis of TIA, and part of what makes a mimic is its similar time course to TIA. Nevertheless, other key aspects of the history that are useful to help identify TIA from mimics are as follows:
Age and other demographic data: is there a high a priori probability of a cerebrovascular event?
Nature of the symptoms: ‘positive’ versus ‘negative’?
Onset and progression
Duration
Precipitating factors
Associated symptoms, for example, headache, loss of awareness, during or after the attacks
Age and other demographic data
TIAs are rare in young people without vascular risk factors (eg, hypertension, ischaemic heart disease, diabetes mellitus, smoking, haematological disease, etc). In otherwise healthy pregnant women, transient neurological symptoms are a common reason for neurological referral, but are often related to migraine. Seizures and syncope occur at all ages, although the underlying causes may differ. Syncope is more common in women, but seizures have no sex predilection. TIAs are more common in men at younger ages, but the sex difference reduces after the menopause.
Nature of the symptoms
Positive symptoms indicate an ‘excess’ of central nervous system neurone electrical discharges and may be visual (eg, flashing lights, zigzag shapes, lines, shapes, objects), somatosensory (eg, pain, paraesthesia) or motor (eg, jerking limb movements).
Negative symptoms indicate a loss or reduction of central nervous system neurone function (eg, loss of vision, hearing, sensation or limb power).
Seizures and migraine auras typically start as positive symptoms, while TIAs typically begin with negative symptoms (but may develop positive symptoms as well). Seizures only occasionally cause paresis from the outset, but even then close questioning or examination may reveal minor positive motor or sensory symptoms or signs. Of course, postictal paresis is very common after seizures, so an accurate history of the sequence of events is essential.
Transient speech disturbance is a challenging symptom for TIA diagnosis. It is important to try to distinguish between dysphasia and dysarthria, as this may affect classification of arterial territory and subsequent management. However, in practice this may be impossible. A history of ‘slurring’ suggests dysarthria, while altered word content or grammatical structure, with or without impaired reading suggests a language disturbance. Asking some of the following questions may be helpful. For the patient: did they know exactly which words they were trying to say? For the witness: were the words that you heard the right ones, albeit slurred? Were there any nonsense words, or any that were clearly the wrong word for the context?
Judging the time of onset of speech or language difficulties can be challenging. Recently descriptions report abnormal texting on mobile devices (‘dystextia’) as a useful guide to a language disturbance and precise onset time of neurological deficit. Isolated complete and brief speech arrest, particularly if recurrent and stereotyped, is probably more commonly related to seizures than TIA.
Likewise determining the onset time and nature (monocular vs binocular) of visual disturbance can be difficult unless the patient deliberately covers one eye during the attack, but is crucial.
Onset and evolution of the symptoms
Symptoms of TIA usually start abruptly, followed by gradual offset, usually over minutes. TIA symptoms are usually negative, and if there are multiple symptoms, they all typically occur more or less together from onset. By contrast, migraine aura typically progresses slowly over minutes to tens of minutes, and positive symptoms may be followed by negative ones in the same functional domain or modality. For example, paraesthesias may begin in the hand, then gradually progress up the arm to the shoulder, trunk, and then the face and leg, frequently followed by numbness. In the visual domain, a visual aura may migrate across the field and be followed by a visual field defect. Although at onset only one sensory modality is usually affected, migraine aura may subsequently progress to other modalities, as adjacent cortical regions are affected; such evolution is not a feature of a single TIA.
Seizures usually progress very quickly (seconds) in a single functional neurological domain. Loss of consciousness is common in seizures and syncope. Seizures are usually recurrent stereotyped attacks. In most cases TIAs do not cause recurrent stereotyped attacks; exceptions to this are lacunar TIAs (the most dramatic form of which is the capsular warning syndrome, see below), TIAs due to distal intracranial stenosis, and occasionally haemodynamic TIAs due to critical perfusion relating to a large artery stenosis. Loss of consciousness is extremely rare in TIAs (but not impossible, see ‘Chameleons’).
Duration of the symptoms
Migrainous auras usually last 10–30 min, but may persist for many hours. TIAs nearly always last less than 1 h. Seizures last usually up to about 5 min. Syncope usually lasts a few seconds, unless the patient stays upright. Episodes recurring over some years are very likely due to syncope, seizures or migraine. By contrast, TIAs usually occur over a relatively short space of time (days to weeks), and may occur as a series of attacks in a much shorter time (days to weeks; so-called ‘crescendo’ TIAs).
Precipitating factors
Seizure triggers include hyperventilation, intercurrent sepsis, altered alcohol intake or missing antiepileptic medication. Haemodynamic “jerking” TIAs (see ‘Chameleons’) may occur upon sudden standing, after taking antihypertensive medication, or following a large meal or hot bath. Benign paroxysmal positional vertigo is triggered by sudden head movements (see case study). Syncope may be precipitated by emotional stimuli (eg, seeing blood) or fluid loss (eg, diarrhoea and vomiting).
Associated symptoms
Tongue biting (especially if lateral) and muscle pains after the event are markers of seizure. Vomiting is common after migraine and occasionally follows syncope, but is extremely rare in TIA or seizures. Nausea, sweating, pallor and a need to urinate or defaecate commonly precede or follow syncope.
Mimics
Up to 60% of patients referred to a TIA clinic do not have a final diagnosis of TIA,12 17–19 but this will depend on how patients are referred and the method of diagnosis. Any cause of transient neurological symptoms is a potential TIA mimic, giving a huge range of alternative diagnoses. Of 1532 consecutive patients attending our TIA service, 1148 (75%) had either definite or possible TIA, 46 (3%) had minor stroke and the remaining 338 (22%) had one of 25 alternative diagnoses (figure 1).
Figure 1.

Frequency of transient ischaemic attack (TIA) mimics from 1532 consecutive suspected TIA referrals to the University College London comprehensive stroke service.
Frequent causes of transient neurological symptoms that can mimic TIA include:
Migraine aura
Seizure
Syncope
Functional or anxiety related
Table 1 shows some useful clinical distinguishing features for these common mimics.
Table 1.
Clinical features of transient ischaemic attack (TIA) and some common mimics
| TIA | Migraine | Seizure | Syncope | Functional/anxiety | |
|---|---|---|---|---|---|
| Demographic | Older age Vascular risk factors More common in men |
Younger age More common in women |
Any age | Any age, often younger More common in women |
Younger More common in women |
| Neurological symptoms | Negative symptoms, usually maximal at onset: for example, numbness, weakness, visual loss. Transient diplopia and monocular visual loss are often due to TIA Does not spread into other sensory modalities. Alteration or loss of consciousness almost never occur |
Positive, spreading symptoms at onset. Visual the most common. May be followed by negative symptoms in the same domain Symptoms may evolve into another modality (eg, visual followed by somatosensory) True alteration or loss of consciousness almost never occur, though there may be ‘confusion’ or muddled thinking |
Positive symptoms including painful sensory disturbance, limb jerking, head turning, dystonic posturing, lip smacking. Loss of awareness and amnesia for event unless simple partial seizures Postictal negative symptoms (eg, Todd's paresis) may persist for days |
Faint or light headed (presyncopal). Vision may darken, or hearing becomes muffled. Loss of awareness |
Isolated sensory symptoms common |
| Timing | Abrupt onset, gradual offset (minutes). Usually total duration minutes, nearly always <1 h Recur over days or weeks, usually not months or years. |
Usually last 20–30 min, but may be much longer Can recur over years or decades. |
Usually less than 2 min. Can recur over years |
Seconds to less than a minute. Can recur over years |
Tend to be recurrent and stereotyped |
| Associated symptoms | Headaches may occur, usually during the attacks | Headache usually afterwards with migrainous features (nausea, vomiting, photophobia, phonophobia, mechanosensitivity) | Tongue biting (especially lateral), incontinence, muscle pains, exhaustion or disorientation, headache follow | Sweating, pallor, nausea, rapid recovery to full alertness | May be preceded by emotional or psychosocial stressors Anxiety |
We will now consider in more detail some of the key TIA mimics likely to be encountered in clinical practice.
Migraine aura
Up to about 20% of patients with suspected TIA have migraine aura2; this is the most common mimic in our experience (figure 1). The diagnostic challenge arises particularly when the aura occurs with minimal or no headache. This phenomenon, described by Miller Fisher as ‘late-life migraine accompaniment’, is now usually referred to as acephalgic migraine.20 A migraine aura reflects cortical spreading depression, so classically has a spreading onset corresponding to adjacent cortical regions over minutes, usually resolving within 30 min and only rarely lasting over an hour. Visual disturbances, sometimes with scintillating scotomata, geometric (especially zigzag) patterns or other positive symptoms with varied descriptions (‘like looking through a heat haze’; ‘like looking through raindrops moving down a window’; ‘like looking through a kaleidoscope’, etc), are the most common. It may help to ask the patient to draw their visual aura (figure 2). Auras can include sensory, motor or speech disturbances. In migraine, different modalities may be involved (eg, visual and somatosensory) but they often occur sequentially, with one resolving as the other begins, rather than all simultaneously as in TIAs. Although auras are typically experienced just before or simultaneously with headache, headache onset can occasionally be delayed for more than an hour after the end of the aura.
Figure 2.
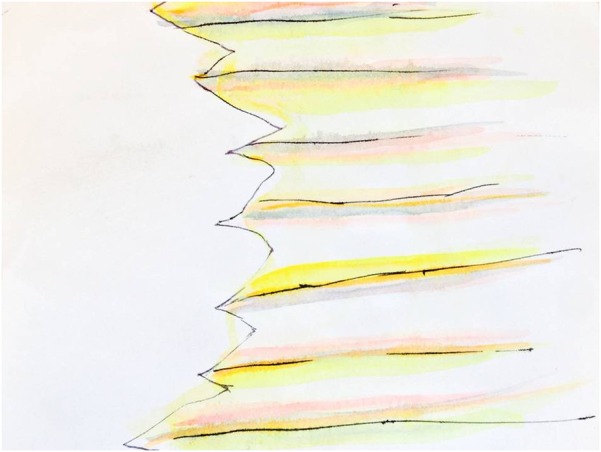
Drawing of a visual migraine aura by a patient showing a characteristic zigzag pattern.
Headache may also occur at TIA or stroke onset, especially in young women with a prior history of migraine,21 where it is probably triggered by the stroke (ie, a ‘symptomatic’ rather than “primary” migraine). Thus the presence of typical migrainous aura or headache does not exclude TIA (or stroke). The concept of migrainous infarction is controversial and the safest initial policy is to assume that migraine does not cause cerebrovascular events, and to investigate all patients for alternative causes.
Seizures
Generalised seizures without partial features should not be difficult to distinguish from TIA, provided there is an adequate witnessed account. In generalised seizures with partial features, postictal confusion,14 headache, involuntary movements and incontinence may be helpful pointers against TIA (see table 1). ‘Negative’ motor symptoms (eg, haemiparesis) are very rare as the sole manifestation of seizures, but not unheard of.22 Complete speech arrest may be more likely in seizures than in TIA. Todd's paresis—a focal neurological deficit following about 1 in 10 generalised seizures—can last for hours, or occasionally longer. Postictal dysphasia can follow seizures involving the dominant hemisphere. The key is a witnessed account of seizure activity at onset. While focal seizures are often very stereotyped even over multiple events, recurrent TIAs may be totally different in character. Finally, a previous history of epilepsy is clearly useful.
Syncope
Syncope is a transient loss of consciousness with loss of postural tone and rapid recovery. It is not usually characterised by truly focal symptoms. Presyncopal symptoms may be a helpful pointer, including a faint feeling, dimming of vision and muffling of hearing, reflecting global, retinal and cochlear hypoperfusion, respectively. Common causes are reflex (vasovagal) syncope, postural hypotension and carotid sinus hypersensitivity. The most important serious causes of syncope are cardiac arrhythmias. Vertebrobasilar TIAs can rarely cause loss of consciousness if thalamic structures are involved (‘top of the basilar’ syndrome) but this is very rarely transient (but see ‘Chameleons’). Upon hearing a clinical history consistent with syncope, a diagnosis of TIA seems to be more likely to be considered by a non-neurologist in comparison with a neurologist.19
Peripheral vestibular disturbance
Complaints of acute vertigo or ‘dizziness’ are common in TIA clinics, primary care and emergency departments. It is important to assess whether the symptom is ‘true vertigo’—a feeling of usually rotatory movement with respect to the environment—or is in fact unsteadiness without vertigo, or faintness. The words ‘dizzy’ or ‘giddy’ may be used by patients to describe vertigo or presyncope, and always deserve further detailed exploration. Even with a detailed history it can be difficult to distinguish clinically between a vertebrobasilar TIA and peripheral vestibular disturbance, particularly in older patients with comorbidities. This challenge is compounded as often the clinical examination is normal (the head-impulse test and Hallpike's test are specific but not sensitive). Overall, isolated ‘dizziness’ is much more likely to be due to peripheral vestibular disturbance than TIA: a population-based study reported that only 3.2% of patients presenting to the emergency department with ‘dizziness’ have a final diagnosis of TIA or stroke.23 Even an expert taking a careful history may remain uncertain, and in those cases MRI with diffusion-weighted sequences can be very helpful since it has high sensitivity for posterior circulation ischaemic injury.
Transient global amnesia
Transient global amnesia is a rare but striking condition characterised by the temporary loss of anterograde episodic memory,24 usually in people aged over 50 years. Risk factors for vascular disease are common. Neurologists are familiar with the typical attacks, which usually last for several hours after which there is a filling in of old memory and a restoration of ability to lay down new ones; a gap for the episode persists. Procedural memory is intact but repetitive questions are common. EEG during the attacks has not demonstrated seizure activity, but a witnessed account should be sought to seek clinical evidence (eg, lip-smacking, dystonic limb posturing, etc). Attacks rarely recur, and patients can be reassured that the risk of future stroke does not appear to be increased. Functional imaging during attacks has demonstrated transient hypoperfusion mainly in the mesial temporal lobes. Memory loss from TIA only occurs very rarely in posterior circulation TIAs affecting bilateral medial temporal structures, so it strongly suggests a TIA mimic.14
Functional/anxiety disorder
The rate of functional disorder in TIA clinics has been reported to be as high as 7%.12 Approximately 60% of patients with functional weakness present initially with symptoms of sudden onset or on waking.25 Symptoms may be stereotyped and recurrent and may be accompanied by panic, pain or physical injury at the time of onset. There may be dissociative or multiple symptoms. Other features of a functional presentation include inconsistency between symptoms and examination, or examination and functional observations, or ‘collapsing’ weakness. Functional symptoms are more common in younger patients without conventional vascular risk factors and may affect the non-dominant side more often than the dominant side. Panic attacks may follow an otherwise typical TIA, which may occasionally cause a diagnostic challenge.
Amyloid ‘spells’ and cerebral convexity subarachnoid haemorrhage
Cerebral amyloid angiopathy, a common cause of lobar cerebral haemorrhage in older patients, can also present with transient focal neurological episodes, which are sometimes known as ‘amyloid spells’.26 These are stereotyped, recurrent, transient neurological episodes of paraesthesias, numbness or weakness of spreading onset over seconds to minutes, resolving over a similar period. The events are presumed to be secondary to focal seizures or cortical spreading depression. Recent data suggest that symptoms are equally likely to be predominantly positive (spreading paraesthesias, positive visual phenomena, or limb jerking) or negative symptoms (weakness, language impairment or visual loss).27 Blood-sensitive MRI (gradient echo T2*-weighted or susceptibility-weighted sequences) are critical in investigating attacks of this sort, since superficial cortical siderosis or acute sulcal haemorrhage is commonly found, suggesting a causative role in generating these symptoms. The key clinical point here is that the future risk of symptomatic intracerebral haemorrhage after such transient neurological events seems to be very high (figure 3). It is currently difficult to estimate how often in clinical practice focal transient symptoms are related to small areas of haemorrhage because so few centres routinely acquire the necessary MRI sequences; this is an important topic for future research. If imaging findings suggest cerebral amyloid angiopathy—especially with lobar cerebral haemorrhage and superficial siderosis—we suggest that antithrombotic drugs should generally be avoided due to the high risk of further cerebral haemorrhage (figure 3).
Figure 3.

(A) MR scan of brain from an 82-year-old woman who presented with recurrent episodes of sudden onset needles affecting the face, gum and hand, with facial drooping, lasting about 20 min. The patient was treated with clopidogrel. (B) CT scan of head following admission 1 month later with sudden left haemiparesis. Note large right frontal intracerebral haematoma.
Structural brain lesions
Occasionally structural intracranial lesions, particularly meningiomas, can cause TIA-like symptoms. These symptoms are thought to arise due to mass effect resulting in a partial impairment of cerebral blood flow.28 A diagnostic difficulty can also arise because of associated seizures with prominent negative symptoms. For example arteriovenous malformations may undergo dynamic changes in flow due to haemorrhage or thrombosis, or may disturb local cerebral blood flow. Tumours may undergo haemorrhage or infarction or can cause partial seizures. Clues to a structural TIA mimic include a gradual or stuttering onset over a longer period (eg, weeks), or associated symptoms of raised intracranial pressure.
Paroxysmal symptoms due to demyelination
Two types of paroxysmal symptoms that can mimic TIA are seen in multiple sclerosis. They are rare, but highly characteristic of mutliple sclerosis. The first is paroxysmal dysarthria, where there are recurrent stereotyped episodes of slurred speech; the second is ‘tonic spasms’, manifesting as painful brief posturing often affecting the upper limb on one side. These are usually recurrent and stereotyped and occur typically in younger people with few vascular risk factors. Usually these can be recognised, particularly in the context of established multiple sclerosis, but occasionally can be the first manifestation.
Chameleons
Limb-shaking TIAs
Rhythmic, involuntary jerky limb movements can occur in haemodynamic TIAs, which may thus be mistaken for focal motor seizures.29 30 The presence of limb shaking is a well-established sign of hemisphere hypoperfusion, due to severe carotid or middle cerebral artery disease.29–32 The episodes tend to be brief (<5 min), recurrent and avoid the face. They can be precipitated by activities that may reduce cerebral blood flow (such as postural change, coughing and exercise).32 Previously reported cases do not exhibit the Jacksonian march typical of focal motor seizures,29–31 the other main differential for this presentation. MRI, including DWI sequences, can help in showing a classical ‘borderzone’ pattern of established or recent ischaemia, especially if symptoms are prolonged or recurrent (figure 4).
Figure 4.

Imaging from a patient who presented with recurrent attacks of rhythmic jerking of the left arm, related to changing from a sitting to standing position. (A) MR angiogram showing critical right middle cerebral artery stenosis. (B) Fluid-attenuated inversion recovery (FLAIR) MRI showing high signals in the right hemisphere white matter in a ‘borderzone’ distribution.
TIAs with altered conscious level or other brainstem symptoms
Loss of consciousness is not characteristic of a TIA.33 However, transient ischaemia of the thalami or brainstem can very rarely cause such symptoms. We have very occasionally seen patients who give a classical history of transient quadriparesis with intact cognition suggesting a ‘locked-in’ TIA due to brainstem ischaemia.
Spontaneous limb movements or posturing due to brainstem ischaemia
Occasionally, rhythmic movements of the limbs can accompany acute brainstem ischaemia. These movements may be seizure-like rhythmic jerking, sometimes with prolonged tonic muscle contractions. The movements may be intermittent, and easily confused with a seizure. It is vitally important clinically to recognise the possibility of brainstem ischaemia in such cases, as they may be a warning of impending brainstem infarction from basilar thrombosis.34 The pathophysiology of these movements is not well understood: they may represent a ‘release phenomenon’ resembling ‘decerebrate’ posturing, or disturbance of function of the reticular formation.
Capsular warning syndrome
The capsular warning syndrome is one of the most dramatic presentations in stroke medicine. In this striking phenomenon, in situ disease of a single penetrating artery is thought to cause fluctuating ischaemia and neuronal dysfunction limited to the internal capsule. The early stroke risk is high.35 Many attacks can occur in a short period of time (eg, 24–48 h) leading to suspicions of seizures or functional disorder in some patients. A similar phenomenon relating to pontine perforating artery ischaemia (“pontine warning syndrome”) is also described.
Summary
Suspected TIA remains a common and important diagnostic challenge for physicians in primary and secondary care, including neurologists. The transience of symptoms makes historical features paramount in establishing the diagnosis among the many ‘mimics’. The pathophysiological differences between TIA and the most common mimics (including migraine, seizures and syncope) mean that careful consideration of clinical features can be very helpful in establishing the diagnosis. However, the clinical history does not allow complete certainty. Indeed, recent studies show that haemorrhagic cerebrovascular disease can mimic TIA (especially cortical superficial siderosis in association with cerebral amyloid angiopathy), with sometimes devastating consequences if antithrombotic drugs are started or continued; the proportion of patients with transient symptoms who may be harmed by incorrect diagnosis requires formal study. It nevertheless seems reasonable to recommend MRI (including optimum sequences to detect ischaemia and haemorrhage) as the imaging modality of choice in assessing TIA, since it may provide positive evidence of ischaemic injury and can exclude significant haemorrhage. Together with careful clinical evaluation this should allow the most effective distinction of TIA from the myriad of ‘mimics’.
Footnotes
Contributors: DJW: idea for the review, drafting and editing the manuscript. VN: drafting and editing the paper. RJP: drafting and editing the paper. JJ: editing the paper and critical revisions.
Competing interests: None.
Provenance and peer review: Commissioned; externally peer reviewed. This paper was reviewed by William Whiteley, Edinburgh, UK.
References
- 1.Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke 2009;40:2276–93 [DOI] [PubMed] [Google Scholar]
- 2.Schrock JW, Glasenapp M, Victor A, et al. Variables associated with discordance between Emergency Physician and Neurologist Diagnoses of transient ischaemic attacks in the emergency department. Ann Emerg Med 2012;59:19–26 [DOI] [PubMed] [Google Scholar]
- 3.Sheehan OC, Merwick A, Kelly LA, et al. Diagnostic usefulness of the ABCD2 score to distinguish transient ischemic attack and minor ischemic stroke from noncerebrovascular events: the North Dublin TIA Study. Stroke 2009;40:3449–54 [DOI] [PubMed] [Google Scholar]
- 4.Castle J, Mlynash M, Lee K, et al. Agreement regarding diagnosis of transient ischemic attack fairly low among stroke-trained neurologists. Stroke 2010;41:1367–70 [DOI] [PubMed] [Google Scholar]
- 5.Tomasello F, Mariani F, Fieschi C, et al. Assessment of inter-observer differences in the Italian multicenter study on reversible cerebral ischemia. Stroke 1982;13:32–5 [DOI] [PubMed] [Google Scholar]
- 6.Kraaijeveld CL, van Gijn J, Schouten HJ, et al. Interobserver agreement for the diagnosis of transient ischemic attacks. Stroke 1984;15:723–5 [DOI] [PubMed] [Google Scholar]
- 7.Koudstaal PJ, Gerritsma JG, van Gijn J. Clinical disagreement on the diagnosis of transient ischemic attack: is the patient or the doctor to blame? Stroke 1989;20:300–1 [DOI] [PubMed] [Google Scholar]
- 8.Rothwell PM, Warlow CP. Timing of TIAs preceding stroke: time window for prevention is very short. Neurology 2005;64:817–20 [DOI] [PubMed] [Google Scholar]
- 9.Giles MF, Rothwell PM. Risk of stroke early after transient ischaemic attack: a systematic review and meta-analysis. Lancet Neurol 2007;6:1063–72 [DOI] [PubMed] [Google Scholar]
- 10.Chandratheva A, Mehta Z, Geraghty OC, et al. Population based study of risk and predictors of stroke in the first few hours after a TIA. Neurology 2009;72:1941–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS Study): a prospective population-based sequential comparison. Lancet 2007;370:1432–42 [DOI] [PubMed] [Google Scholar]
- 12.Prabhakaran S, Silver AJ, Warrior L, et al. Misdiagnosis of transient ischemic attacks in the emergency room. Cerebrovasc Dis 2008;26:630–5 [DOI] [PubMed] [Google Scholar]
- 13.Josephson SA, Sidney S, Pham TN, et al. Higher ABCD2 score predicts patients most likely to have true transient ischaemic attack. Stroke 2008;39:3096–98 [DOI] [PubMed] [Google Scholar]
- 14.Amort M, Fluri F, Schafer J, et al. Transient ischaemic attack versus transient ischaemic attack mimics: frequency, clinical characteristics and outcome. Cerebrovasc Dis 2011;32:57–64 [DOI] [PubMed] [Google Scholar]
- 15.Merwick A, Albers GW, Amarenco P, et al. Addition of brain and carotid imaging to the ABCD2 score to identify patients at early risk of stroke after transient ischaemic attack: a multicentre observational study . Lancet Neurol 2010;9:1060–9 [DOI] [PubMed] [Google Scholar]
- 16.Warach S, Kidwell CS. The redefinition of TIA: the uses and limitations of DWI in acute ischaemic cerebrovascular syndromes. Neurology 2004;62:359–60 [DOI] [PubMed] [Google Scholar]
- 17.Ferro JM, Falcao I, Rodrigues G, et al. Diagnosis of transient ischemic attack by the nonneurologist. A validation study. Stroke 1996;27:2225–9 [DOI] [PubMed] [Google Scholar]
- 18.Martin PJ, Young G, Enevoldson TP, et al. Over diagnosis of TIA and minor stroke: experience at a regional neurovascular clinic. QJM 1997;90:759–63 [DOI] [PubMed] [Google Scholar]
- 19.Calanchini PR, Swanson PD, Gotshall RA, et al. Cooperative study of hospital frequency and character of transient ischaemic attacks. IV. The reliability of diagnosis. JAMA 1977;238:2029–33 [PubMed] [Google Scholar]
- 20.Fisher CM. Late-life migrainous accompaniments—further experience. Stroke 1986;17:1033–42 [DOI] [PubMed] [Google Scholar]
- 21.Tentschert S, Wimmer R, Greisenegger S, et al. Headache at stroke onset in 2196 patients with ischemic stroke or transient ischemic attack. Stroke 2005;36:e1–3 [DOI] [PubMed] [Google Scholar]
- 22.Kaplan PW. Focal seizures resembling transient ischaemic attacks due to subclinical ischaemia. Cerebrovascular Dis 1993;3:241–3 [Google Scholar]
- 23.Kerber KA, Brown DL, Lisabeth LD, et al. Stroke among patients with dizziness, vertigo, and imbalance in the emergency department: a population-based study. Stroke 2006;37:2484–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Harrison M, Williams M. The diagnosis and management of transient global amnesia in the emergency department. Emerg Med J 2007;24:444–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Stone J, Warlow C, Sharpe M. Functional weakness: clues to mechanism from the nature of onset. J Neurol Neurosurg Psychiatry 2012;83:67–9 [DOI] [PubMed] [Google Scholar]
- 26.Charidimou A, Law R, Werring DJ. Amyloid “spells” trouble. Lancet 2012;380:1620. [DOI] [PubMed] [Google Scholar]
- 27.Charidimou A, Peeters A, Fox Z, et al. Spectrum of transient focal neurological episodes in cerebral amyloid angiopathy: multicentre magnetic resonance imaging cohort study and meta-analysis. Stroke 2012;43:2324–30 [DOI] [PubMed] [Google Scholar]
- 28.Ueno Y, Tanaka A, Nakayama Y. Transient neurological deficits simulating transient ischemic attacks in a patient with meningioma--case report. Neurol Med Chir (Tokyo) 1998;38:661–5 [DOI] [PubMed] [Google Scholar]
- 29.Schulz UG, Rothwell PM. Transient ischaemic attacks mimicking focal motor seizures. Postgrad Med J 2002;78:246–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Baquis GD, Pessin MS, Scott RM. Limb shaking--a carotid TIA. Stroke 1985;16:444–8 [DOI] [PubMed] [Google Scholar]
- 31.Tatemichi TK, Young WL, Prohovnik I, et al. Perfusion insufficiency in limb-shaking transient ischemic attacks. Stroke 1990;21:341–7 [DOI] [PubMed] [Google Scholar]
- 32.Persoon S, Kappelle LJ, Klijn CJ. Limb-shaking transient ischaemic attacks in patients with internal carotid artery occlusion: a case-control study. Brain 2010;133(Pt3): 915–22 [DOI] [PubMed] [Google Scholar]
- 33.Special report from the National Institute of Neurological Disorders and Stroke Classification of cerebrovascular diseases III. Stroke 1990;21:637–76 [DOI] [PubMed] [Google Scholar]
- 34.Wilson LK, Benavente OR, Woolfenden AR, et al. Sponaneous limb movements and posturing secondary to acute basilar artery occlusion: a potentially devastating seizure mimic. Pract Neurol 2014;14:42–4. [DOI] [PubMed] [Google Scholar]
- 35.Donnan GA, O'Malley HM, Quang L, et al. The capsular warning syndrome: pathogenesis and clinical features. Neurology 1993;24:957–62 [DOI] [PubMed] [Google Scholar]