

Abstract
Research into regenerative dentistry has added impetus onto the field of molecular biology. It can be documented as a prototype shift in the therapeutic armamentarium for dental disease. Regenerative endodontic procedures are widely being added to the current armamentarium of pulp therapy procedures. The regenerative potential of platelets has been deliberated. A new family of platelet concentrates called the platelet rich fibrin (PRF) has been recently used by several investigators and has shown application in diverse disciplines of dentistry. This paper is intended to add light on the various prospects of PRF and clinical insights to regenerative endodontic therapy.
Keywords: Platelet rich fibrin, Regenerative endodontics, Scaffold
Introduction
The modern exploration of regenerative dentistry has added impetus onto the field of molecular biology. Assuming the present-day situation, it can be categorically documented as an archetype stint in the therapeutic armamentarium for dental disease. Regenerative endodontic procedures are defined as biologically based procedures designed to replace damaged structures, including dentin and root structures, as well as cells of the pulp-dentin complex.1 The harmonized spurs of biology and mechanical regulators promoting cellular activities have critically enhanced the acceptance of regenerative therapy for dental tissues.
The regenerative potential of platelets has been deliberated. The platelets release growth factors that are trapped inside the fibrin matrix following activation. These are considered to be the stimulant for mitogenic response in the periosteum and are responsible for bone repair during normal wound healing.2 The superior understanding of physiologic properties of platelets in wound healing has led to their augmented therapeutic applications.3 Nevertheless, there is still concern linked to the procedures for production of autologous fibrin adhesives.4,5 Besides, legal restrictions on blood handling with concentrated platelet rich plasma have coexisted. In an effort to overcome these problems, it was contemplated to develop a new family of platelet concentrates, which came to be recognized as the platelet rich fibrin (PRF).5
Choukroun's PRF is a fibrin matrix where platelet cytokines and cells are wedged.6 They serve as a resorbable membrane following their release after a certain time.7 PRF was considered to be a healing biomaterial and was initially used in oral implantology.8 Presently, several investigations have shown its application in diverse disciplines of dentistry.9-14 This paper is intended to add light on the various prospects of PRF and clinical insights to regenerative endodontic therapy. The appraisal focused on original research articles and case reports entailing the use of PRF in endodontics. The search terminologies used on PubMed database were 'platelet rich fibrin (PRF)'. The criteria were further specified by use of Boolean operators (AND, OR, NOT) and permutation of precise keywords as 'platelet rich fibrin dental' and 'platelet rich fibrin endodontics'.
Review
What is PRF?
PRF is often named as Choukroun's PRF after its inventor.5,6 It is a second-generation platelet concentrate. The PRF constitutes components of blood sample that are beneficial to improve wound healing and immunity. Ross et al. were amongst the pioneers who first described a growth factor from platelets.15
Preparation
The procedure involves drawing of blood that is collected into test tubes without an anticoagulant and needs to be centrifuged instantaneously. A tabletop centrifuge can be used for this purpose for 2 minutes at 2,700 rpm.6 The resultant product consists of the three layers.16
Straw colored fraction of acellular platelet poor plasma (PPP) at peak level
PRF clot in intermediate level
Red fraction of red blood cell (RBCs) at the base level
The blood coagulation starts instantaneously as it comes in contact with the glass surface due to the lack of anticoagulant. If the time necessary to collect blood and launch centrifugation is exceedingly prolonged, the fibrin will polymerize in a diffuse way in the tube and only a small blood clot without consistency will be obtained.5 Consequently, blood collection should be prompt and instant centrifugation is a prerequisite in the production protocol for PRF.5
Recently, PRF box (Process, Nice, France) has been announced.2 It is formulated to produce homogenously thickened hydrated membrane and an exudate rich in platelets, leukocytes, vitronectin and fibronectin expressed from the fibrin clots.17 It has improved the issues regarding the handling of the PRF clot.18
Biological properties of PRF
PRF can be considered as an immune concentrate with specific composition and a three dimensional architecture.17,19,20 It contains multitude of growth factors like platelet derived growth factor (PDGF), transforming growth factor β1 (TGF β1), insulin like growth factor (IGF), etc., exhibiting varied potent local properties such as cell migration, cell attachment, cell proliferation, and cell differentiation.19,21 It has been shown as an ideal biomaterial for pulp-dentin complex regeneration.22 PRF is both a healing and interpositional biomaterial.23 It accelerates wound closure and mucosal healing due to fibrin bandage and growth factor release. In addition, it prevents the early invagination of undesired cells, and thus acts as a viable barrier between desired and undesired cells.19,23
Biochemical analysis of PRF
PRF consists of an intimate assembly of cytokines, glycan chains, structural glycoproteins enmeshed within a slowly polymerized fibrin network.17 These biochemical components have well known synergistic effects on healing processes.24 Fibrin is the natural guide of angiogenesis. Fibrin constitutes a natural support to immunity.20
Proposed mechanism of action
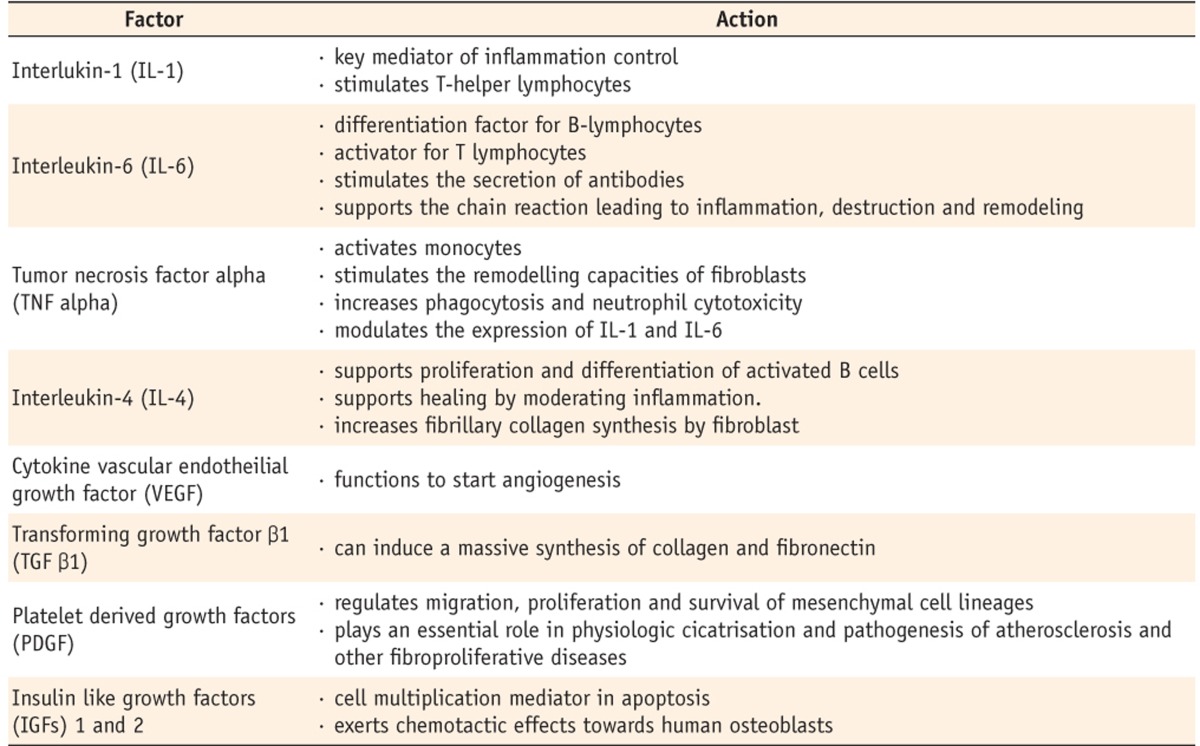
In vitro release of growth factors from PRF and the results of in vivo studies have now put forward a proposal to optimize the clinical application of PRF.25 PRF is a concentrated suspension of the growth factors found in platelets (Table 1).18,26,27 These growth factors are involved in wound healing and are postulated as promoters of tissue regeneration.17,20
Table 1.
PRF growth factors and their specific role
PRF as a tissue-engineering scaffold for endodontics
In any tissue engineering procedure, the cell growth and differentiation are related to an apposite scaffold.28-31 Furthermore, the differentiation of stem cells is controlled by extracellular matrix molecules.32 In this regard, it is anticipated that a suitable scaffold that contains growth factors might be promising tool to enrich the rate of tissue differentiation as it would selectively bind and localize cells and undergo biodegradation over time.33 PRF can be considered as an appropriate scaffold for regenerative endodontics as it fulfills all the properties as mentioned above. As a potential scaffold for regenerative endodontic therapy, PRF entails prospective research.
Review of regenerative endodontic applications of PRF
Following is a brief literature review on the various applications of PRF in endodontic therapy. Shivashankar et al. described a case report highlighting the combined use of graft material (PRF and hydroxyapatite [HA]) and barrier membrane in the treatment of large periapical lesion.23 The authors hypothesized that the use of PRF in conjunction with HA crystals accelerates the resorption of the graft crystals and induces rapid rate of bone formation. Likewise, Sculean et al. in their study concluded that the combination of barrier membrane and grafting materials might result in histological evidence of periodontal regeneration, predominantly bone repair.34 Gassling et al. demonstrated that PRF membranes are suitable for cultivation of periosteal cells for bone tissue engineering.35 Pradeep et al. concluded that when HA is combined with PRF, it increases the regenerative effects observed with PRF in the treatment of human three wall intrabony defects.36
Jayalakshmi et al. used PRF in combination with beta tricalcium phosphate (β-TCP) bone graft in the treatment of periapical cyst.37 The authors reported progressive, significant, and predictable clinical and radiographic bone regeneration/healing with the use of PRF. The authors suggested that the combined use of PRF and β-TCP for bone augmentation in treatment of periapical defects is a potential treatment alternative for faster healing than using biomaterials alone. Similar results were reported by Kim et al. using combination therapy of PRF with β-TCP.38
Keswani et al. reported that PRF might serve as a potentially ideal scaffold in revascularization of immature permanent teeth with necrotic pulps as it is rich in growth factors, enhances cellular proliferation and differentiation, and acts as a matrix for tissue ingrowth.39 In this context, Simonpieri et al. reviewed advantages of the use of PRF as it acts as a stabilizing sheath and offers mechanical sustenance.40 Also, the authors proposed that PRF fragments act as biological connectors and the cellular migration is accelerated which is critical for neo-angiogenesis and vascularization. Furthermore, the platelet cytokines (PDGF, TGF-alpha, IGF-1) are gradually released as the fibrin matrix is resorbed, thus creating a perpetual process of healing.
Bains et al. reported the applicability of PRF for the management of an iatrogenic perforation of pulpal floor in the furcation region of mandibular first molar.13 According to the authors, the autologous and biocompatible nature of PRF and mineral trioxide aggregate (MTA) appeared to be favorable for the long-term clinical results. Shivashankar et al. reported a case of revitalization of tooth with necrotic pulp and open apex using PRF.22 They described evidence of continued thickening of the dentinal walls, root lengthening, regression of the periapical lesion and apical closure with use of PRF. The authors considered PRF to be an excellent biomaterial for pulp-dentin complex regeneration. Analogously, Rudagi et al. also reported a case demonstrating the successful healing and apexification with combined use of MTA as an apical barrier, and autologus platelet rich fibrin membrane as an internal matrix.41
Huang et al. conducted an investigation into the biological effects of PRF on human dental pulp cells.42 PRF was found to increase dental pulp cell proliferation as well as osteoprotegerin (OPG) expression in a time-dependent manner. Alkaline phosphatase (ALP) activity was also significantly up-regulated by PRF. These findings might serve as a basis for preclinical studies that address the role of PRF in reparative dentin formation.
In regard to regenerative endodontic procedures with PRF, it is assumed that some amounts of human dental pulp cells present in the apical papilla usually remain vital even in case of a large periapical lesion. After the regression of the inflammation and under the influence of Hertwigs epithelial root sheath, these dental pulp cells differentiate into odontoblasts like cells. OPG and ALP expression are generally regarded as markers of odontoblastic differentiation. The only disadvantage associated with PRF is its manipulation to place inside the canal. Clinical trials are crucial to equate the effect of PRF in the revitalization of tooth with necrotic pulp and open apex on a long term basis.
Hiremath et al. reported affirmative results with pulpotomy using PRF.43 However, the authors suggested that long term trials with larger sample sizes are required to justify the use of PRF for treatment of pulpitis. It was concluded that pulpotomy with PRF could be a substitute treatment to MTA or other materials.
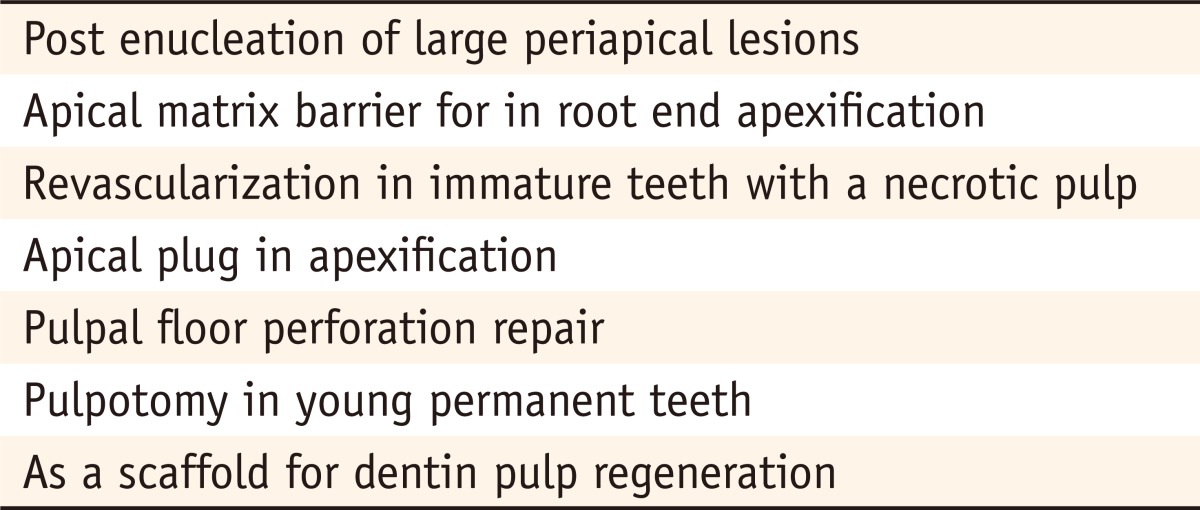
It is apparent persuasively that PRF, when used as a scaffolding material in an infected necrotic immature tooth for pulpal regeneration and tooth revitalization, satisfies many criteria of an ideal physical scaffold. Another advantage of using PRF as a scaffold is that it has a trimolecular or equilateral fibrin branch junction that makes its architecture flexible and can support cytokine enmeshment and cellular migration.5 However, long-term exploration still needs to be focused for therapeutic benefits of PRF. We present a summary of the potential regenerative endodontic applications of PRF as reported by various clinical studies (Table 2).
Table 2.
Role of PRF in regenerative endodontics
Conclusions
With the present knowledge, it can be confirmed that PRF can be considered a therapeutic biomaterial. However, despite the evident regenerative benefits of PRF, substantiation of its clinical applications is still limited. Consequently, there is a constraint for the rationalization of its use. Additional randomized, controlled clinical trials are defensible to test the long-term benefits and ultimate outcomes associated with PRF.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Murray PE, Garcia-Godoy F, Hargreaves KM. Regenerative endodontics: a review of current status and a call for action. J Endod. 2007;33:377–390. doi: 10.1016/j.joen.2006.09.013. [DOI] [PubMed] [Google Scholar]
- 2.Khiste SV, Tari RN. Platelet-rich fibrin as a biofuel for tissue regeneration. ISRN Biomaterials. 2013 Available from: http://dx.doi.org/10.5402/2013/627367. [Google Scholar]
- 3.Naik B, Karunakar P, Jayadev M, Marshal VR. Role of platelet rich fibrin in wound healing: a critical review. J Conserv Dent. 2013;16:284–293. doi: 10.4103/0972-0707.114344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mazzocca AD, McCarthy MB, Chowaniec DM, Cote MP, Romeo AA, Bradley JP, Arciero RA, Beitzel K. Platelet-rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012;94:308–316. doi: 10.2106/JBJS.K.00430. [DOI] [PubMed] [Google Scholar]
- 5.Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, Gogly B. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part I: technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e37–e44. doi: 10.1016/j.tripleo.2005.07.008. [DOI] [PubMed] [Google Scholar]
- 6.Choukroun J, Adda F, Schoeffler C, Vervelle A. An opportunity in perio-implantology: the PRF (in French) Implantodontie. 2001;42:55–62. [Google Scholar]
- 7.Mosesson MW. Fibrinogen and fibrin structure and functions. J Thromb Haemost. 2005;3:1894–1904. doi: 10.1111/j.1538-7836.2005.01365.x. [DOI] [PubMed] [Google Scholar]
- 8.Aroca S, Keglevich T, Barbieri B, Gera I, Etienne D. Clinical evaluation of a modified coronally advanced flap alone or in combination with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: a 6-month study. J Periodontol. 2009;80:244–252. doi: 10.1902/jop.2009.080253. [DOI] [PubMed] [Google Scholar]
- 9.Arunachalam LT, Merugu S, Sudhakar U. A novel surgical procedure for papilla reconstruction using platelet rich fibrin. Contemp Clin Dent. 2012;3:467–470. doi: 10.4103/0976-237X.107443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bansal C, Bharti V. Evaluation of efficacy of autologous platelet-rich fibrin with demineralized-freeze dried bone allograft in the treatment of periodontal intrabony defects. J Indian Soc Periodontol. 2013;17:361–366. doi: 10.4103/0972-124X.115663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hauser F, Gaydarov N, Badoud I, Vazquez L, Bernard JP, Ammann P. Clinical and histological evaluation of postextraction platelet-rich fibrin socket filling: a prospective randomized controlled study. Implant Dent. 2013;22:295–303. doi: 10.1097/ID.0b013e3182906eb3. [DOI] [PubMed] [Google Scholar]
- 12.Xuan F, Lee CU, Son JS, Jeong SM, Choi BH. A comparative study of the regenerative effect of sinus bone grafting with platelet-rich fibrin-mixed Bio-Oss and commercial fibrin-mixed Bio-Oss: an experimental study. J Craniomaxillofac Surg. 2013 Aug 01;:pii: S1010-5182(13)00159-5. doi: 10.1016/j.jcms.2013.05.029. doi: 10.1016/j.jcms.2013.05.029. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 13.Bains R, Bains VK, Loomba K, Verma K, Nasir A. Management of pulpal floor perforation and grade II Furcation involvement using mineral trioxide aggregate and platelet rich fibrin: a clinical report. Contemp Clin Dent. 2012;3(Suppl 2):S223–S227. doi: 10.4103/0976-237X.101100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Clipet F, Tricot S, Alno N, Massot M, Solhi H, Cathelineau G, Perez F, De Mello G, Pellen-Mussi P. In vitro effects of Choukroun's platelet-rich fibrin conditioned medium on 3 different cell lines implicated in dental implantology. Implant Dent. 2012;21:51–56. doi: 10.1097/ID.0b013e31822b9cb4. [DOI] [PubMed] [Google Scholar]
- 15.Ross R, Glomset J, Kariya B, Harker L. A plateletdependent serum factor that stimulates the proliferation of arterial smooth muscle cells in vitro. Proc Natl Acad Sci U S A. 1974;71:1207–1210. doi: 10.1073/pnas.71.4.1207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sunitha Raja V, Munirathnam Naidu E. Platelet-rich fibrin: evolution of a second-generation platelet concentrate. Indian J Dent Res. 2008;19:42–46. doi: 10.4103/0970-9290.38931. [DOI] [PubMed] [Google Scholar]
- 17.Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, Gogly B. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part II: plateletrelated biologic features. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e45–e50. doi: 10.1016/j.tripleo.2005.07.009. [DOI] [PubMed] [Google Scholar]
- 18.Toffler M, Toscano N, Holtzclaw D, Corso MD, Dohan Ehrenfest DM. Introducing Choukroun's platelet rich fibrin (PRF) to the reconstructive surgery milieu. J Implant Adv Clin Dent. 2009;1:21–30. [Google Scholar]
- 19.Del Corso M, Sammartino G, Dohan Ehrenfest DM. Re: 'Clinical evaluation of a modified coronally advanced flap alone or in combination with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: a 6-month study'. J Periodontol. 2009;80:1694–1697. doi: 10.1902/jop.2009.090253. [DOI] [PubMed] [Google Scholar]
- 20.Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, Dohan SL, Dohan AJ, Mouhyi J, Dohan DM. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part IV: clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e56–e60. doi: 10.1016/j.tripleo.2005.07.011. [DOI] [PubMed] [Google Scholar]
- 21.Kaigler D, Cirelli JA, Giannobile WV. Growth factor delivery for oral and periodontal tissue engineering. Expert Opin Drug Deliv. 2006;3:647–662. doi: 10.1517/17425247.3.5.647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shivashankar VY, Johns DA, Vidyanath S, Kumar MR. Platelet rich fibrin in the revitalization of tooth with necrotic pulp and open apex. J Conserv Dent. 2012;15:395–398. doi: 10.4103/0972-0707.101926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shivashankar VY, Johns DA, Vidyanath S, Sam G. Combination of platelet rich fibrin, hydroxyapatite and PRF membrane in the management of large inflammatory periapical lesion. J Conserv Dent. 2013;16:261–264. doi: 10.4103/0972-0707.111329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, Gogly B. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part III: leucocyte activation: a new feature for platelet concentrates? Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e51–e55. doi: 10.1016/j.tripleo.2005.07.010. [DOI] [PubMed] [Google Scholar]
- 25.Cromack DT, Porras-Reyes B, Mustoe TA. Current concepts in wound healing: growth factor and macrophage interaction. J Trauma. 1990;30(12 Suppl):S129–S133. doi: 10.1097/00005373-199012001-00026. [DOI] [PubMed] [Google Scholar]
- 26.Su CY, Kuo YP, Tseng YH, Su CH, Burnouf T. In vitro release of growth factors from platelet-rich fibrin (PRF): a proposal to optimize the clinical applications of PRF. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:56–61. doi: 10.1016/j.tripleo.2009.02.004. [DOI] [PubMed] [Google Scholar]
- 27.Dohan Ehrenfest DM, de Peppo GM, Doglioli P, Sammartino G. Slow release of growth factors and thrombospondin-1 in Choukroun's platelet-rich fibrin (PRF): a gold standard to achieve for all surgical platelet concentrates technologies. Growth Factors. 2009;27:63–69. doi: 10.1080/08977190802636713. [DOI] [PubMed] [Google Scholar]
- 28.Howard D, Buttery LD, Shakesheff KM, Roberts SJ. Tissue engineering: strategies, stem cells and scaffolds. J Anat. 2008;213:66–72. doi: 10.1111/j.1469-7580.2008.00878.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mikos AG, Herring SW, Ochareon P, Elisseeff J, Lu HH, Kandel R, Schoen FJ, Toner M, Mooney D, Atala A, Van Dyke ME, Kaplan D, Vunjak-Novakovic G. Engineering complex tissues. Tissue Eng. 2006;12:3307–3339. doi: 10.1089/ten.2006.12.3307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yoo YJ, Baek SH, Son HH. Pulp tissue regeneration and root formation of permanent teeth with pulpal/periapical deseases. J Korean Acad Conserv Dent. 2010;35:238–245. [Google Scholar]
- 31.Forghani M, Parisay I, Maghsoudlou A. Apexogenesis and revascularization treatment procedures for two traumatized immature permanent maxillary incisors: a case report. Restor Dent Endod. 2013;38:178–181. doi: 10.5395/rde.2013.38.3.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Chan BP, Leong KW. Scaffolding in tissue engineering: general approaches and tissue-specific considerations. Eur Spine J. 2008;17(Suppl 4):467–479. doi: 10.1007/s00586-008-0745-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hargreaves KM, Giesler T, Henry M, Wang Y. Regeneration potential of the young permanent tooth: what does the future hold? J Endod. 2008;34(7 Suppl):S51–S56. doi: 10.1016/j.joen.2008.02.032. [DOI] [PubMed] [Google Scholar]
- 34.Sculean A, Nikolidakis D, Schwarz F. Regeneration of periodontal tissues: combinations of barrier membranes and grafting materials-biological foundation and preclinical evidence: a systematic review. J Clin Periodontol. 2008;35(8 Suppl):106–116. doi: 10.1111/j.1600-051X.2008.01263.x. [DOI] [PubMed] [Google Scholar]
- 35.Gassling V, Douglas T, Warnke PH, Acil Y, Wiltfang J, Becker ST. Platelet-rich fibrin membranes as scaffolds for periosteal tissue engineering. Clin Oral Implants Res. 2010;21:543–549. doi: 10.1111/j.1600-0501.2009.01900.x. [DOI] [PubMed] [Google Scholar]
- 36.Pradeep AR, Rao NS, Agarwal E, Bajaj P, Kumari M, Naik SB. Comparative evaluation of autologous platelet-rich fibrin and platelet-rich plasma in the treatment of 3-wall intrabony defects in chronic periodontitis: a randomized controlled clinical trial. J Periodontol. 2012;83:1499–1507. doi: 10.1902/jop.2012.110705. [DOI] [PubMed] [Google Scholar]
- 37.Jayalakshmi KB, Agarwal S, Singh MP, Vishwanath BT, Krishna A, Agrawal R. Platelet-rich fibrin with beta-tricalcium phosphate-a noval approach for bone augmentation in chronic periapical lesion: a case report. Case Rep Dent. 2012;2012:902858. doi: 10.1155/2012/902858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kim BJ, Kwon TK, Baek HS, Hwang DS, Kim CH, Chung IK, Jeong JS, Shin SH. A comparative study of the effectiveness of sinus bone grafting with recombinant human bone morphogenetic protein 2-coated tricalcium phosphate and platelet-rich fibrin-mixed tricalcium phosphate in rabbits. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113:583–592. doi: 10.1016/j.tripleo.2011.04.029. [DOI] [PubMed] [Google Scholar]
- 39.Keswani D, Pandey RK. Revascularization of an immature tooth with a necrotic pulp using platelet-rich fibrin: a case report. Int Endod J. 2013;46:1096–1104. doi: 10.1111/iej.12107. [DOI] [PubMed] [Google Scholar]
- 40.Simonpieri A, Del Corso M, Sammartino G, Dohan Ehrenfest DM. The relevance of Choukroun's platelet-rich fibrin and metronidazole during complex maxillary rehabilitations using bone allograft. Part II: implant surgery, prosthodontics, and survival. Implant Dent. 2009;18:220–229. doi: 10.1097/ID.0b013e31819b5e3f. [DOI] [PubMed] [Google Scholar]
- 41.Rudagi KB, Rudagi B. One-step apexification in immature tooth using grey mineral trioxide aggregate as an apical barrier and autologus platelet rich fibrin membrane as an internal matrix. J Conserv Dent. 2012;15:196–199. doi: 10.4103/0972-0707.94582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Huang FM, Yang SF, Zhao JH, Chang YC. Platelet-rich fibrin increases proliferation and differentiation of human dental pulp cells. J Endod. 2010;36:1628–1632. doi: 10.1016/j.joen.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 43.Hiremath H, Saikalyan S, Kulkarni SS, Hiremath V. Second-generation platelet concentrate (PRF) as a pulpotomy medicament in a permanent molar with pulpitis: a case report. Int Endod J. 2012;45:105–112. doi: 10.1111/j.1365-2591.2011.01973.x. [DOI] [PubMed] [Google Scholar]