

Abstract
Background/Aims
Stereotactic body radiation therapy (SBRT) for gastrointestinal malignancies requires the placement of fiducials to guide treatment delivery. This study aimed to determine the safety and technical feasibility of endoscopic ultrasonography (EUS)-guided fiducial placement for SBRT.
Methods
From November 2010 to August 2012, 32 consecutive patients who were scheduled to receive SBRT for pancreatic and hepatic malignancies were referred for EUS-guided fiducial placement. Primary outcome measurements included technical success, the fiducial migration rate, and procedural complications.
Results
All 32 patients had successful fiducial placement under EUS guidance. The mean number of fiducials placed per patient was 2.94±0.24 (range, 2 to 3 seeds). Spontaneous fiducial migration was noted in one patient (3.1%). Of the 32 patients with fiducials placed, 29 patients (90.6%) successfully underwent SBRT. One patient (3.1%) developed mild pancreatitis, requiring a 2-day prolonged hospitalization after fiducial placement. Five patients (15.6%) underwent same-session, EUS-guided fine needle aspiration for histologic confirmation at the time of fiducial placement, without any procedure-related complication.
Conclusions
EUS-guided fiducial placement is a safe and technically feasible technique for preparing patients with both pancreatic and hepatic malignancies for SBRT. The fiducial markers facilitate safe and accurate targeting of the tumor during SBRT.
Keywords: Fiducial markers, Endosonography, Radiosurgery, Pancreatic neoplasms, Liver neoplasms
INTRODUCTION
Stereotactic body radiation therapy (SBRT) allows for the delivery of high radiation doses while minimizing toxicity on adjacent organs.1,2 This technique demands high targeting accuracy, taking into account respiratory and other involuntary motion of the target lesion during radiation therapy.2 SBRT needs fiducial markers for target localization and tracking.2 Fiducial markers serve as reference points for computed tomography (CT) planning and allow for simultaneous correction of target motion. Traditionally, fiducial markers have been placed either intraoperatively or percutaneously under ultrasound (US) or CT guidance.3 Percutaneous approaches for fiducial placement can be taken for superficial lesions, but may not be feasible for deeper lesions. Given the capability of endoscopic ultrasonography (EUS) to allow for close proximity to deeper abdominal structures that are not easily accessible via percutaneous approaches, EUS-guided fiducial placement is a more effective method of localizing these tumors.
EUS-guided fiducial placement has recently been reported as a technically feasible technique for mediastinal and other abdominal malignancies,4-9 including the pancreas, oesophagus, stomach, or porta hepatis. The aim of our study was to demonstrate the safety and technical feasibility of EUS-guided fiducial placement for pancreatic and hepatic malignancy.
MATERIALS AND METHODS
1. Patients
From November 2010 to August 2012, 32 consecutive patients (21 male, 11 female) who were scheduled to receive SBRT for malignancy were referred for EUS-guided fiducial placement. Patients with coagulopathy (international normalized ratio >1.5, platelets <50,000) were transfused with the appropriate blood products for correction of coagulopathy. An allergy to gold or concomitant inflammatory disease was considered a contraindication for gold marker implantation. All procedures were performed in the endoscopy unit at the Asan Medical Center by single experienced endosonographers (D.W.S.), who perform more than 350 EUS procedures annually for pancreaticobiliary diseases. This study was approved by the Institutional Review Board at Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. Informed patient consent was obtained before each procedure.
2. Preparation
Patients were sedated with intravenous injections of 3 to 5 mg midazolam. Periprocedural intravenous antibiotics (cefotaxime 2 g or ciprofloxacin 400 mg) were administered prophylactically in all patients for 1 day. Anticoagulation and antiplatelet medications were discontinued according to the guidelines for endoscopic procedures.10
3. Instruments
A linear array echoendoscope (GF-UC240P-AL5; Olympus Co., Tokyo, Japan or EG-3870 UTK; Pentax, Hamburg, Germany) was used to perform the EUS. A standard 19-gauge needle (Echotip; Cook Medical, Winston-Salem, NC, USA) was used to deploy a gold fiducial marker measuring 0.8×3 mm (CIVCO Medical Solutions, Orange City, IA, USA). The system used by our hospital for SBRT was RapidArc (Varian Medical Systems, Palo Alto, CA, USA).
4. Endoscopic technique
Using sterile forceps, each cylindrical gold seed was back-loaded into the tip of a 19 G Echotip needle with the stylet withdrawn 7 to 8 mm. The needle was then pressed into bone wax (Ethicon, Somerville, NJ, USA) to seal it into place. Once a safe needle direction had been identified under EUS guidance, the needle with the backloaded fiducial was passed through the working channel of the scope and the fiducial was deployed into or near the tumor by advancing the stylet (Fig. 1). The needle was then withdrawn from the echoendoscope and reloaded with a new fiducial marker, and the procedure was repeated with the placement of two or three fiducials about 1.5 cm apart. Fiducial positioning was confirmed with a real time EUS image, as well as an abdominal roentgenogram after the procedure (Fig. 2). A marker was usually seen as a hyperechoic structure with a ringdown artifact behind it. After implanting all markers, we checked the position of each marker in the transverse and sagittal planes to determine the distance between fiducial markers, which is essential for treatment planning. All patients were admitted to the hospital for one day to monitor any complications. An outpatient course of oral antibiotics was not given upon patient discharge, but patients were instructed to report any delayed symptoms such as fever, chills, abdominal pain, or any other unexpected symptoms for a period of 1 month.
Fig. 1.

Endoscopic ultrasonography-guided fiducial placement. (A) Needle delivering fiducial into a pancreatic mass. (B) Hyperechoic fiducial (arrow) in a mass.
Fig. 2.

Three fiducial markers (arrows) identified by abdominal radiography.
5. Outcome
Technical success was defined as puncturing the target lesion accurately and the ability to implant more than two fiducials in the appropriate location for SBRT. Fiducial migration was defined as seed dislodgement outside the volume of the original injection site and unusable for guiding SBRT as determined by planning CT.
6. Treatment planning and delivery
The SBRT technique used in our institute is described as follows. First, patients were immobilized in a stereotactic body frame (Elekta Oncology, Norcross, GA, USA). CT simulations were performed 10 to 14 days after fiducial marker placement and reviewed by a radiation oncologist to verify the feasibility of using SBRT enabled by the fiducial markers (Fig. 3). For lesions that moved more than 5-mm on fluoroscopic imaging, 4-dimensional CT scanning and gated delivery was performed using the Real-Time Position Management System (Varian Medical Systems). Treatment planning was formulated with the Eclipse Planning System (Varian Medical Systems). Fractional doses of 6 to 8 Gy were delivered to target volume for consecutive 4 days. Fractionated schedules were employed as follows: 26 to 28 Gy in four fractions for pancreatic cancer (28 patients), 30 Gy in four fractions for celiac lymph node metastasis (one patient). We checked daily setup accuracy with cone-beam CT and/or fluoroscopy.
Fig. 3.
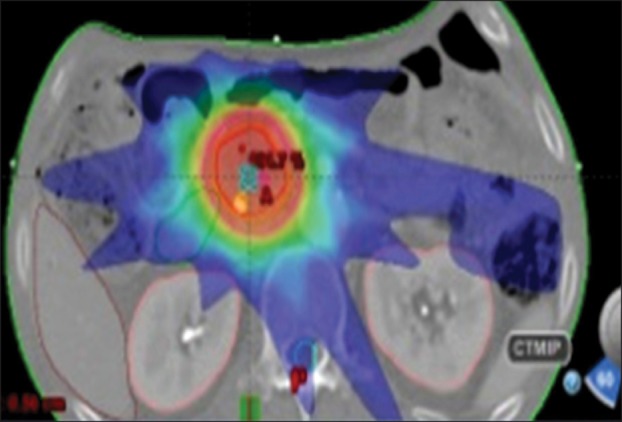
Treatment-planning computed tomography demonstrating pancreatic head localization based on fiducial markers for stereotactic body radiation therapy.
RESULTS
1. Patient and tumor characteristics
Thirty-two patients (21 male, 11 female) underwent EUS-guided fiducial placement. The mean age of patients was 66 years (range, 46 to 90 years). The location and pathologic diagnosis of tumors were as follows: celiac lymph node (lymph node metastasis from hepatocellular carcinoma), caudate lobe (hepatocellular carcinoma), retrocrural area (metastatic carcinoma from hepatocellular carcinoma), and pancreas. Of the pancreatic cancers, 10 were located in the head, two in the uncinate process, and 17 in the body/tail. The mean size of the tumors was 3.2±1.1 cm (range, 1.9 to 7.0 cm). Patient and procedural characteristics are described in Table 1.
Table 1.
Patient and Procedural Characteristics for Endoscopic Ultrasonography-Guided Fiducial Placement
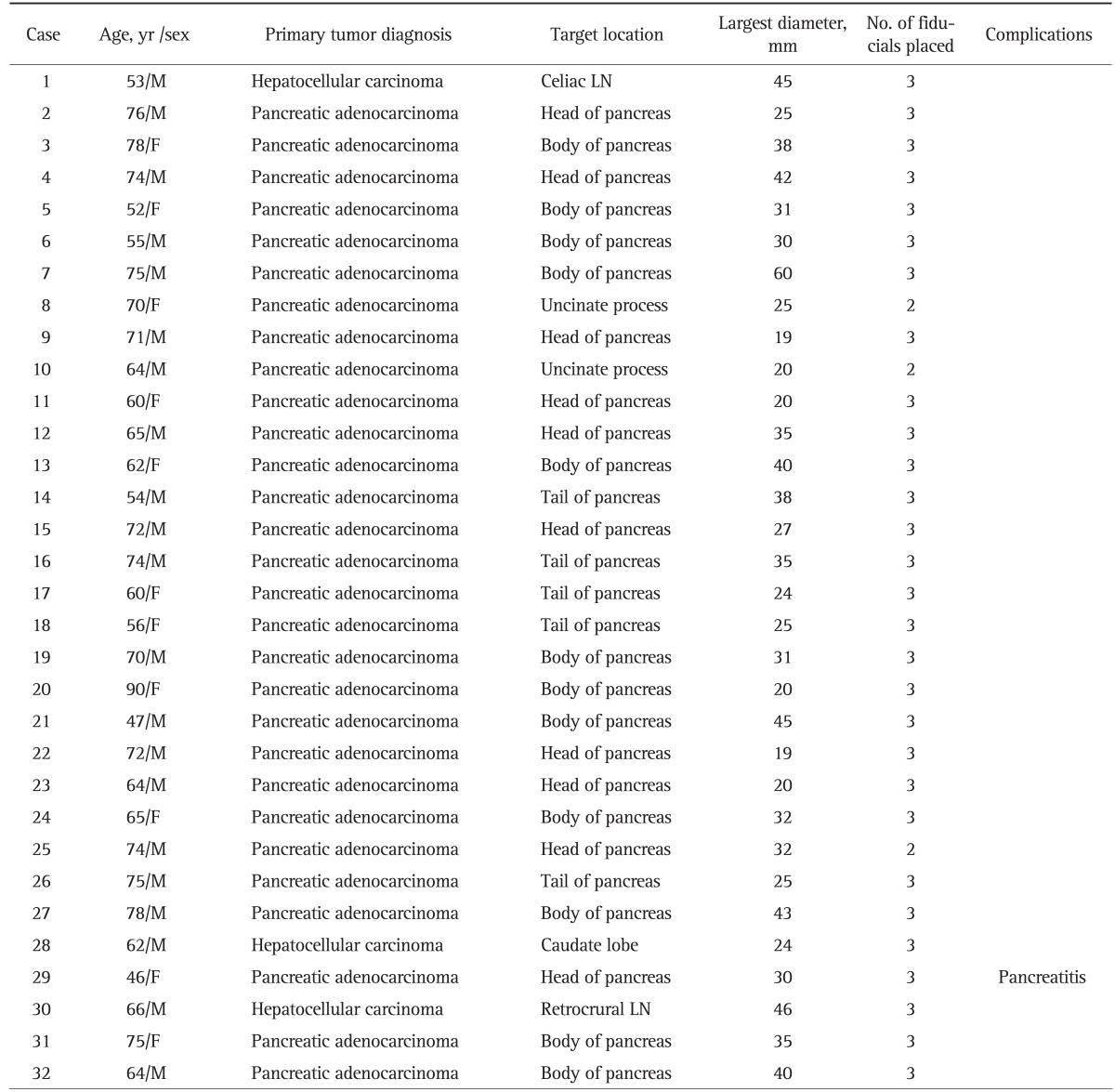
M, male; F, female; LN, lymph node.
2. EUS-guided fiducial placement
The fiducial placement under EUS guidance was technically successful in 32 out of 32 patients (100%). Only one patient (3.1%) developed a mild pancreatitis requiring a 2-day prolonged hospitalization after fiducial placement. The patient presented worsening abdominal pain 18 hours after the placement of three fiducials in the pancreatic body mass. The patient's serum lipase was elevated to 420 IU/L. An abdominal CT scan showed mild swelling of the pancreas around the implanted fiducials. The patient was treated conservatively and recovered before the scheduled SBRT.
Five patients (15.6%) underwent same session EUS-guided fine needle aspiration (FNA) for tissue diagnosis at the time of fiducial placement without any procedure related complications.
Among the 32 patients who had fiducial placement under EUS guidance, 29 patients (90.6%) successfully underwent SBRT. Three patients did not undergo planned SBRT due to disease progression (n=2), transfer to another institution (n=1).
Generally, two or three fiducials were implanted into and around the tumor. A total of 94 fiducials were implanted in 32 patients, 34 using a transgastric approach and 60 using a transduodenal approach. The mean number of fiducials per patients was 2.94±0.24 (range, 2 to 3 seeds). Two patients with pancreatic head cancer were implanted with two fiducials because they already had a biliary metallic stent that can be used as reference marker, thereby allowing three-dimensional configuration with only two implanted fiducials.
Spontaneous fiducial migration was noted in one patients (3.1%). Three gold fiducials were inserted under EUS, and two fiducials were seen on subsequent planning CT; however, the ability to use the remaining fiducial markers for SBRT was adequate without requiring a repeat EUS procedure. Overall, fiducial migration occurred in one of 94 seeds placed (1.1%). There was no further reported fiducial migration throughout the course of radiation therapy. This was verified by comparing the cone beam CT images acquired before each day of therapy with the initial planning CT images.
DISCUSSION
In current study, we demonstrated the technical feasibility and safety of EUS-guided fiducial placement in either hepatic or pancreatic malignancy using a 19-gauge needle. The technical success rate of 100% demonstrates the feasibility of this technique for these cancers. Of the 32 patients who had EUS-guided fiducials implanted, 29 patients (90.6%) successfully underwent SBRT. We encountered no severe resistance while deploying the fiducial seeds. As the study was retrospective, it should be appreciated that preferential candidates for EUS-guided fiducial placement may have been included, thereby resulting in a high success rate. In addition, a previous study noted that failure to place a fiducial in the target lesion was attributable to an anatomical alteration or a limitation of the use of 5-mm-long fiducials.5,7 However, the present study included only one patient with surgically altered anatomy and used gold fiducials measuring 3 mm in length, potentially influencing our high success rate. In our experience, the fluoroscopic assistance was not necessary during the procedure of fiducial placement. We could identify the fiducials placed under EUS alone, thereby verifying the proper placement immediately.
There have been several published studies on the feasibility of EUS-guided fiducial placement for various mediastinal and abdominal malignancies.4-9 Four studies investigated the feasibility of EUS-guided fiducial placement using a 19-gauge FNA needle to deploy cylindrical gold seeds measuring 2.5 to 5 mm in length with 0.8 mm diameter, reporting a high success rate.5-7,9 Two studies demonstrated the feasibility of EUS-guided fiducial placement using a 22-gauge FNA needle to deploy gold coil fiducials measuring 10 mm in length with 0.35 mm diameter, offering potential advantages over the use of a 19-gauge needle.4,8 EUS-guided fine-needle injection using a 19-gauge needle performed in pancreatic lesions of the head and uncinate process is often challenging because of the acute angulation. Larghi et al.11 stated that the degree of deflection of the echoendoscope tip is the major factor responsible for bringing the target lesion into an appropriate position, which precludes extension of the needle from the accessory channel. For such hard to reach tumors, it is preferable to place the fiducial markers around the periphery of the tumor, rather than directly in the tumor, provided there is not a substantial difference between respiratory movement of the fiducials and the actual target tumor. Recently, one retrospective study comparing traditional fiducials (5-mm length, 0.8-mm diameter) and Visicoil fiducial (10-mm length, 0.35-mm diameter) demonstrated that there was no significant difference between the two fiducial types in terms of technical success, complications, and migration.12 However, it remains unclear whether the use of a 22-gauge needle instead of a 19-gauge needle affects the technical success and complication rates of the procedure until prospective randomized study is completed. It is also unclear whether the thinner caliber 0.35 mm fiducials affect the accurate tracking of the fiducials by the SBRT system compared to the standard 0.8 mm fiducials. Further prospective randomized studies are warranted to evaluate the technical success and complication rates of the EUS-guided fiducial placement using 19-gauge and 22-gauge needles. In previous studies, the target lesions for fiducial placement have been located in the mediastinum, abdomen and GI system including the pancreas, stomach, liver, and porta hepatis. The success rates for EUS-guided fiducial placement were reported to range from 85% to 100%.4-8 Reported procedure related complications were cholangitis (n=2), mild pancreatitis (n=1), fever (n=1), or minor bleeding (n=1).4-8,13 Based on previous literature and the current study, the overall technical success and complication rates of EUS-guided fiducial placement in GI malignancy were 96% and 2%, respectively (Table 2).
Table 2.
Summary of Published Studies and Current Study on Endoscopic Ultrasonography-Guided Fiducial Placement in Gastrointestinal Malignancy
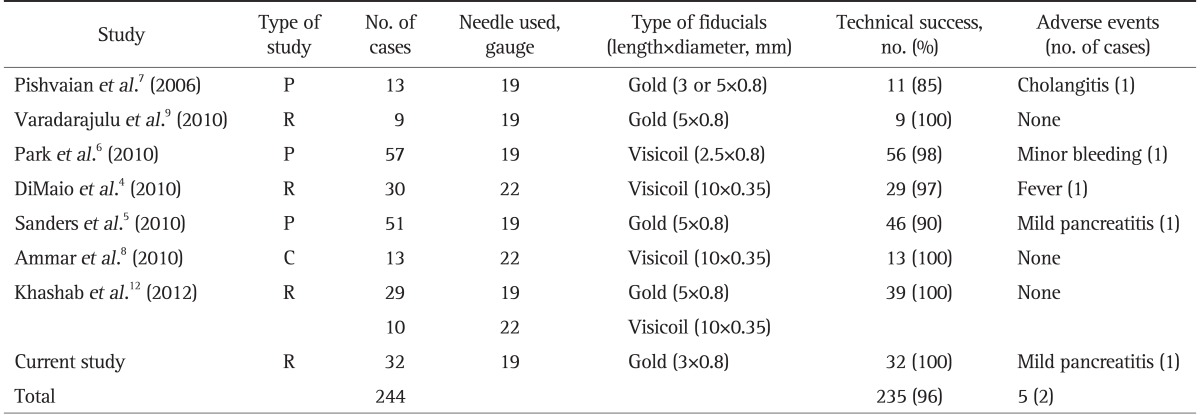
P, prospective; R, retrospective; C, case series.
The fiducial placement may introduce air bubbles into the target lesion, which obscures EUS visualization and leads to difficulty in confirming fiducial placement. To prevent the introduction of air into the lesion, the stylet was withdrawn 7 to 8 mm while backloading the fiducial into the needle and was sealed in place with bone wax. No air bubbles were noted after fiducial deployment using this technique. Although the optimal seed number and location required for SBRT has not been established, we tried implanting at least two fiducials within or adjacent to the mass to account for the possibility of potential migration requiring repeat EUS procedures. In the present study, overall fiducial migration occurred in one of 94 seeds placed (1.0%).
In five cases, the lesion was presumed to be malignant on the basis of the imaging studies and the patient's history. Thus, five patients underwent same session EUS-FNA followed by fiducial placement without subsequent complication. Performing both procedures in the same session has several advantages such as expediting treatment and reducing the length of hospital stay. If EUS-FNA is planned for tissue diagnosis, our results indicate that it can be performed at the time of EUS-guided fiducial placement. Nonetheless, there remains a theoretical concern that performing both procedures simultaneously may cause trauma, resulting in procedure-related complications. Mild pancreatitis has been previously reported as a potential complication of EUS-guided fiducial placement with simultaneous EUS-guided celiac plexus neurolysis.5 For this issue, additional study may be considered.
Tumor seeding due to FNA is extremely rare. In percutaneous FNA under either US or CT guidance, the incidence ranges from 0.005% to 0.009%; however, in the case of EUS-FNA, it is considered to be even lower due to the shorter puncture path. Thus far, only three cases have been reported.14-16 Whether placement of the fiducial implantation within the tumor rather than adjacent to the tumor affects the seeding remains to be evaluated.
Following a previous report of procedure-related cholangitis,7,13 it is recommended that all patients receive prophylactic antibiotics, although strong evidence for this precaution, e.g., a prospective study, is lacking.17 In previous feasibility studies, all patients received an arbitrary 5-day course of antibiotics for infection prophylaxis.5,6,8 In the present study, all patients received a 1-day course of preprocedural and postprocedural intravenous antibiotics. There is ambiguity regarding the role of routine antibiotic prophylaxis prior to EUS-guided fiducial placement. More data are needed to evaluate the role of prophylactic antibiotics and the administering schedule of antibiotics if necessary.
Our study has several limitations. This was a retrospective study at a single tertiary medical center where all EUS procedures were undergone by a single experienced endosonographer. This study was not designed to evaluate a survival benefit or quality of life associated with EUS-guided fiducial placement as a method to support SBRT.
In conclusion, EUS-guided fiducial placement for SBRT in pancreatic and hepatic malignancy appears to be a safe and feasible technique when performed by an experienced endosonographer. This novel application of interventional EUS further expands the role of EUS in the multidisciplinary team approach to patients with pancreatic and hepatic malignancy. The fiducial markers would facilitate safe and accurate targeting of the tumor during SBRT.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Seo Y, Kim MS, Yoo S, et al. Stereotactic body radiation therapy boost in locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2009;75:1456–1461. doi: 10.1016/j.ijrobp.2009.01.042. [DOI] [PubMed] [Google Scholar]
- 2.Chang BW, Saif MW. Stereotactic body radiation therapy (SBRT) in pancreatic cancer: is it ready for prime time? JOP. 2008;9:676–682. [PubMed] [Google Scholar]
- 3.Kothary N, Dieterich S, Louie JD, Chang DT, Hofmann LV, Sze DY. Percutaneous implantation of fiducial markers for imaging-guided radiation therapy. AJR Am J Roentgenol. 2009;192:1090–1096. doi: 10.2214/AJR.08.1399. [DOI] [PubMed] [Google Scholar]
- 4.DiMaio CJ, Nagula S, Goodman KA, et al. EUS-guided fiducial placement for image-guided radiation therapy in GI malignancies by using a 22-gauge needle (with videos) Gastrointest Endosc. 2010;71:1204–1210. doi: 10.1016/j.gie.2010.01.003. [DOI] [PubMed] [Google Scholar]
- 5.Sanders MK, Moser AJ, Khalid A, et al. EUS-guided fiducial placement for stereotactic body radiotherapy in locally advanced and recurrent pancreatic cancer. Gastrointest Endosc. 2010;71:1178–1184. doi: 10.1016/j.gie.2009.12.020. [DOI] [PubMed] [Google Scholar]
- 6.Park WG, Yan BM, Schellenberg D, et al. EUS-guided gold fiducial insertion for image-guided radiation therapy of pancreatic cancer: 50 successful cases without fluoroscopy. Gastrointest Endosc. 2010;71:513–518. doi: 10.1016/j.gie.2009.10.030. [DOI] [PubMed] [Google Scholar]
- 7.Pishvaian AC, Collins B, Gagnon G, Ahlawat S, Haddad NG. EUS-guided fiducial placement for CyberKnife radiotherapy of mediastinal and abdominal malignancies. Gastrointest Endosc. 2006;64:412–417. doi: 10.1016/j.gie.2006.01.048. [DOI] [PubMed] [Google Scholar]
- 8.Ammar T, Coté GA, Creach KM, Kohlmeier C, Parikh PJ, Azar RR. Fiducial placement for stereotactic radiation by using EUS: feasibility when using a marker compatible with a standard 22-gauge needle. Gastrointest Endosc. 2010;71:630–633. doi: 10.1016/j.gie.2009.11.023. [DOI] [PubMed] [Google Scholar]
- 9.Varadarajulu S, Trevino JM, Shen S, Jacob R. The use of endoscopic ultrasound-guided gold markers in image-guided radiation therapy of pancreatic cancers: a case series. Endoscopy. 2010;42:423–425. doi: 10.1055/s-0029-1243989. [DOI] [PubMed] [Google Scholar]
- 10.Adler DG, Baron TH, Davila RE, et al. ASGE guideline: the role of ERCP in diseases of the biliary tract and the pancreas. Gastrointest Endosc. 2005;62:1–8. doi: 10.1016/j.gie.2005.04.015. [DOI] [PubMed] [Google Scholar]
- 11.Larghi A, Verna EC, Stavropoulos SN, Rotterdam H, Lightdale CJ, Stevens PD. EUS-guided trucut needle biopsies in patients with solid pancreatic masses: a prospective study. Gastrointest Endosc. 2004;59:185–190. doi: 10.1016/s0016-5107(03)02538-0. [DOI] [PubMed] [Google Scholar]
- 12.Khashab MA, Kim KJ, Tryggestad EJ, et al. Comparative analysis of traditional and coiled fiducials implanted during EUS for pancreatic cancer patients receiving stereotactic body radiation therapy. Gastrointest Endosc. 2012;76:962–971. doi: 10.1016/j.gie.2012.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Varadarajulu S. Antibiotic prophylaxis is recommended for endoscopic ultrasound-guided fiducial placements. J Clin Gastroenterol. 2011;45:179. doi: 10.1097/MCG.0b013e3181efb1a7. [DOI] [PubMed] [Google Scholar]
- 14.Doi S, Yasuda I, Iwashita T, et al. Needle tract implantation on the esophageal wall after EUS-guided FNA of metastatic mediastinal lymphadenopathy. Gastrointest Endosc. 2008;67:988–990. doi: 10.1016/j.gie.2007.10.025. [DOI] [PubMed] [Google Scholar]
- 15.Paquin SC, Gariépy G, Lepanto L, Bourdages R, Raymond G, Sahai AV. A first report of tumor seeding because of EUS-guided FNA of a pancreatic adenocarcinoma. Gastrointest Endosc. 2005;61:610–611. doi: 10.1016/s0016-5107(05)00082-9. [DOI] [PubMed] [Google Scholar]
- 16.Shah JN, Fraker D, Guerry D, Feldman M, Kochman ML. Melanoma seeding of an EUS-guided fine needle track. Gastrointest Endosc. 2004;59:923–924. doi: 10.1016/s0016-5107(04)00340-2. [DOI] [PubMed] [Google Scholar]
- 17.Van Dam J, Varadarajulu S, Jin Z EUS 2008 Working Group. EUS 2008 Working Group document: evaluation of EUS-guided implantation therapy (with video) Gastrointest Endosc. 2009;69(2 Suppl):S49–S53. doi: 10.1016/j.gie.2008.10.058. [DOI] [PubMed] [Google Scholar]