

Abstract
Background:
Fatigue is considered as a major problem in hemodialysis patients and can impair their quality of life. The purpose of this study was to investigate the effectiveness of acupressure on fatigue in hemodialysis patients.
Materials and Methods:
This is a clinical trial study in which 96 hemodialysis patients participated. Patients were randomly assigned into acupressure, placebo, and control groups (32 subjects fulfilling the inclusion criteria assigned to each group). The measures included the form of demographic characteristics, visual analog scale of fatigue, and Piper Fatigue Scale. Patients in the acupressure and placebo groups received acupressure intervention during the early 2 h of dialysis on six acupoints with massage for 20 min/day, 3 days per week for 4 weeks. In the placebo group, acupressure intervention was performed as mentioned above with a distance of 1 cm away from the actual intervention site. Patients in the control group received routine unit care only. Chi- quare test, Kruskal-Wallis, paired t-test, one-way analysis of variance (ANOVA), and Duncan test were used for data analysis.
Results:
One-way ANOVA tests showed significant differences in the total mean score of fatigue and fatigue mean scores in the behavioral, emotional, sensory, and cognitive dimensions in the acupressure, placebo, and control groups.
Conclusion:
The results of this study showed that acupressure may reduce fatigue in hemodialysis patients, and use of this non-pharmacologic technique for hemodialysis nurses is suggested.
Keywords: Acupressure, fatigue, hemodialysis, Iran, nursing
INTRODUCTION
One of the very common chronic diseases is chronic renal failure,[1] which may lead to end-stage renal disease (ESRD) as a part of that.[2] Its yearly incidence has been reported 330 cases out of 1 million in the US and 253 cases out of 1 million people in Iran. Based on the last statistics in 2007, there are 16,600 hemodialysis patients in Iran.[3]
ESRD patients need renal replacement therapy to survive,[4] and hemodialysis is the most prevalent conventional renal replacement therapy in Iran.[5] ESRD patients undergoing chronic hemodialysis suffer from numerous complications including fatigue.[6] The range of fatigue prevalence has been reported to be 60%-97% among hemodialysis patients.[7] This sign is a complicated concept and its diagnosis and assessment is difficult for the nurses.[8] In ESRD patients, untreated fatigue may highly affect the quality of life and lead to patients’ increased dependency on others, weakness, loss of physical and psychological energy, social isolation, and depression. The elements that can affect the level of fatigue include depression, anemia, sleep disorders, and restless leg syndrome.[9] Medicational interventions such as consumption of growth hormone, anti-depressant and anti-anxiety medications, and levocarnitine and erythropoietin stimulating hormone, as well as non-medicational interventions such as nutrition therapy, sleep disorder treatment, stress management, sport, Yoga, depression treatment, drug abuse, and acupressure are used to lower hemodialysis patients’ fatigue.[7] Because of medications’ side effects and incomplete relief of fatigue after taking anti-fatigue medications, the patients are driven to complementary medicine methods such as acupressure medicine.[10] Based on the reported researches, acupressure medicine is one of the interventions with the highest application by nurses in clinical settings,[11] and is considered as a clinical and comprehensive nursing intervention.[12] This is also among the manual treatments for which the nurses have an excellent position to use.[13] Acupressure medicine, as a healing art, is beautifully integrated with nursing[14] as it is non-invasive and has advantages such as cost efficacy, lack of complications, no need for special tools, and the ease of learning for the patients and their accompanying persons.[12]
The only study conducted on hemodialysis patients’ fatigue was Cho and Tsay's study (2004) in Taiwan, which showed that acupressure medicine can lower the level of fatigue in patients of experimental group compared to control group.[8] Nasiri et al. (2007) in a study on the association between the effect of acupressure medicine and sleep quality of hemodialysis patients showed a significant difference in the sleep quality of experimental and control groups based on Pittsburgh Sleep Scale.[3] Previous studies include a systematic review on the effect of acupressure medicine on hemodialysis patients’ signs including fatigue,[15] and meta-analysis studies on the effect of acupressure medicine on labor pain management in labor unit[16] as well as its effect on post-operation vomiting and nausea in adults.[17] Their results showed that despite poor methodology, high risk of bias, and low number of subjects, it cannot be absolutely indicated that acupressure medicine is effective on patient's signs. Tsay (2004) in a study on the effect of acupressure medicine on hemodialysis patients’ fatigue stated that with regard to cultural and lifestyle differences of the patients in various countries, the results of these studies cannot be generalized for the patients in other geographic areas.[18] Therefore, with regard to the difference between the Iranian culture and the culture in other countries,[19] and as no study has been conducted on the effect of acupressure medicine on hemodialysis patients’ fatigue on the one hand and due to the high application of acupressure medicine in clinical nursing interventions on the other hand (as this type of medicine can provide the patients with a cost-effective and safe nursing intervention), this study was conducted as there was no need of any special tools but just trained finger tips and it could be conducted within a shorter time. Therefore, the researcher decided to conduct a study with the goal of defining the effect of acupressure on hemodialysis patients’ fatigue.
MATERIALS AND METHODS
This is a three-group clinical trial. Study population included all ESRD patients undergoing chronic hemodialysis in three hemodialysis centers of Nour, Alzahra, and Shariati, hospitals. The subjects were selected from the study population based on the inclusion criteria. Inclusion criteria were age of over 18, diagnosis of ERSD, undergoing hemodialysis at least for 3 months, the patients with chief complaint of fatigue and having fatigue score ≥5 based on fatigue severity visual analogue scale, lack of any wound or fracture, being in complete psychological and mental health to attend the study and fill the questionnaire, and not having undergone complementary medicine treatment in the past 3 months of the study. Exclusion criteria were patient's absence for two sessions of acupressure intervention and lack of interest to continue the study. The sampling was convenient continuous sampling. The number of the subjects was estimated to be 96. After random subjects’ allocation through minimization method, 32 subjects were assigned to each group of the study, placebo and control. The data were collected by a three-section questionnaire whose first section contained demographic characteristics including age, sex, education level, marital status, occupation status, and disease etiology. The second section contained Fatigue Severity Scale (FSS) with a visual analogue scale ranked between 0 and 10, which was scored and commented as fatigue (0), minor fatigue (1-3), moderate fatigue (4-6), and severe fatigue (7-10). If the patients had fatigue severity score of ≥5, they attended the study. FSS is a standard scale whose validity and reliability have been confirmed by Gift,[20] and has been frequently used in various studies. The third section included Piper Fatigue Scale with 27 items on four dimensions of mental fatigue including behavioral, emotional, sensory, and cognitive dimensions. Each item was scored from 0 to 10, with score zero given for lack of fatigue, 1-3 for minor fatigue, 4-6 for moderate fatigue, and 7-10 for severe fatigue. Piper Fatigue Scale is a standard scale whose validity (content and concurrent) and reliability have been confirmed. In the study of Masoodi et al.,[21] its scientific validity was confirmed by the professors of Tarbiat Modares, Tehran, and Iran universities. Its reliability was confirmed in the study of Masoodi et al. by a correlation coefficient of r = 0.89. In the present study, its internal validity was α = 0.77 and its reliability was calculated as 81.2% by test retest. This scale was distributed among the patients once before the intervention and once after the intervention to score the subjects’ fatigue severity. Intervention was conducted in the first 2 h of hemodialysis in the experimental and placebo groups. This intervention was carried out among the subjects regularly undergoing hemodialysis, in both legs, hands, and the waist in three weekly sessions for 4 weeks.[18] In the experimental group, the intervention was conducted on the major acupoints K1, GB 34, ST 36, SP 6, BL 23, and HT7.[22,23] In the placebo group, it was carried out with 1 cm distance from the major above-mentioned acupoints. Each session lasted for 20 min, of which 2 min were devoted for primary superficial stroking of the acupoints[24] and the rest of the time (18 min) was for acupressure of the determined six acupoints (3 min for each acupoint).[25] The researcher and a male co-researcher were trained under the supervision of the second supervisor, and then the intervention started by her approval. The researcher (female) and her male co-researcher conducted the intervention separately for the female and male subjects, respectively. Determination of acupoints was made based on the second supervisor's guidance on the acupoints’ standard location. The amount of needed pressure was practiced by standard scales of 20 g to 6 kg, and the reliability of pressure level was confirmed as 100% after 40 times of practice with mean of 3-4 kg on the scales for both researchers’ hands. The details about the process of research, goals, and conditions were given to the patients, and consequently, those interested to join entered the study after filling the written consent form.
Sampling and intervention were conducted after obtaining approval from ethical consideration committee of Nursing and Midwifery School of Isfahan University of Medical Sciences. The data were analyzed by chi-square, Kruskal-Wallis, paired t-test, one-way analysis of variance (ANOVA), and Duncan's test through SPSS version 19.
RESULTS
Mean age of the subjects in the experimental group was 53.4 (13.9) years, in the placebo group 55.4 (11.5) years, and in the control group 54.3 (13.4) years. In the experimental, placebo, and control groups, there were 14 female (43.75%) and 18 male (56.25%) subjects, respectively. The most prevalent etiology of the disease was diabetes in 11 subjects (34.4%) in the study group, hypertension in 14 subjects (43.8%) in the placebo group, and diabetes in 12 subjects (37.5%) in the control group. Before intervention, subjects’ matching was conducted concerning demographic characteristics in the three groups of study, placebo, and control through minimization program, and there was no significant difference in the demographic characteristics between the groups (P > 0.05). One-way ANOVA showed that there was no significant difference between the total mean score of fatigue and the mean scores of Piper Fatigue Scale dimensions before intervention in all the three groups, but these means showed a significant difference after intervention in the three groups (P < 0.001). Post-hoc Duncan test showed that in the study group, total score of fatigue and score of fatigue in emotional, cognitive, and behavioral dimensions were significantly less than in the two groups of placebo and control after intervention (P < 0.05), but there was no significant difference between the control and placebo groups (P > 0.05). Mean score of fatigue in the sensory dimension in the study group was significantly less than in the placebo group (P < 0.05), and in the placebo group, it was significantly less that in the control group (P < 0.05). As observed in Table 1, the total mean score of fatigue and the mean scores of fatigue in sensory, behavioral, cognitive, and emotional dimensions in the two groups of study and placebo were less after intervention compared to before intervention, and paired t-test showed a significant difference (P < 0.05). The total mean score of fatigue and the mean score of fatigue in sensory, behavioral, cognitive, and emotional dimensions showed no significant difference before and after intervention (P > 0.05). As observed in Table 2, there was a significant difference in the total mean score change of fatigue and the mean score change of fatigue severity in all dimensions in the three groups after intervention (P < 0.001). Post-hoc Duncan test showed that reduction of mean fatigue score in behavioral and emotional dimensions was more in the study group compared to the other two groups of placebo and control (P < 0.05), but it showed no significant difference in the two groups of control and placebo (P = 0.3). Post-hoc Duncan test showed that mean reduction of total fatigue score and mean reduction of fatigue scores in sensory and cognitive dimensions in the study group were more than in the placebo group, and they were more in the placebo group compared to the control group (P < 0.05).
Table 1.
Comparison of total mean scores of fatigue, behavioral, emotional, sensory, and cognitive dimensions before and after intervention in the three groups of study, placebo, and control
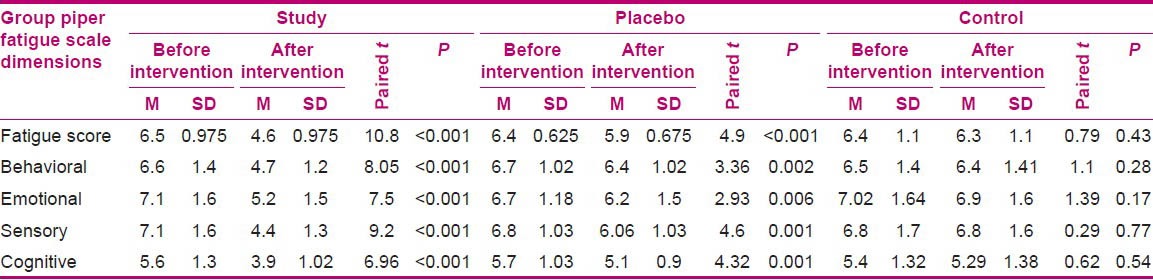
Table 2.
Comparison of fatigue score changes and dimensions of piper fatigue scale after intervention in the three groups of study, placebo, and control

DISCUSSION
The results of acupressure medicine on severity of fatigue in hemodialysis patients showed that the study group experienced less fatigue severity compared to the placebo and control groups. As the subjects’ mean age in the present study was over 50 years, it is concluded that ESRD seems to be more prevalent at higher ages. Tsay and Chen (2003) reported more ESRD prevalence at higher ages.[26] The higher number of male subjects in the present study reveal that ESRD prevalence seems to be more prevalent among men, which concords with the findings of Nasiri et al.[3] Most of the subjects were retired or jobless in the present study. Studies show that the rate of joblessness is high among hemodialysis patients.[27] Diabetes and hypertension are the major etiologies for ESRD,[18] which is consistent with the finding of the present study. Stimulation of acupoints results in improvement of vital energy circulation in the body and increase of opioids like endorphin and enkephalin, which may play a role in the reduction of patients’ fatigue in all behavioral, sensory, cognitive, and emotional dimensions.[18] The obtained results showed that there was a significant reduction in the total mean score of fatigue in the study group after intervention compared to the placebo and control groups. Although a similar improvement was observed in the placebo group based on Duncan test, the improvement was more in the study group.
It seems that in the placebo group, in addition to verbal and psychological communication between the researcher and the patients, due to the physiologic and psychological effects of acupressure, the patients expect the acupressure to have a positive effect on their body, named as Hawthorne phenomenon. So et al. (2007) in a study aimed to define the effect of Transcutaneous Electrical Acupoint Stimulation (TEAS) on improvement of muscular fatigue among athletes and showed a significant difference between TEAS and placebo groups in return of muscular power.[28] This study is in line with the present study except for the lack of a significant difference in the placebo groups after intervention. The difference between these two studies seems to be as a result of the study population, intervention method and the number of subjects. The results showed that the mean score of fatigue in emotional dimension significantly diminished in the study group after intervention compared to the placebo and control groups. From psychological aspect, acupressure induces alpha brain wave stimulation that consequently leads to relaxation and reduction of fatigue and anxiety.[28] This medicine has a positive effect on the body and mind and brings about mental joyfulness and health through stimulation of opioid — endogen systems such as endorphin and enkephalin.[29] Molassiotis et al. (2007)[30] reported the significant effect of acupuncture and acupressure on cancer patients’ fatigue in three groups of acupressure, acupuncture, and placebo in the dimensions of general fatigue, activity, and physical fatigue, although it had no significant effect on the dimension of motivation and psychological fatigue. The difference, observed even in the control group, seems to be as a result of the effect of researcher's psychological factors. Their results showed that acupuncture was more effective than acupressure and acupressure was more effective than placebo. This finding is not consistent with our study, possibly due to the difference in the study population, the scale used, and the length of intervention. Our obtained results showed a significant reduction in the mean score of fatigue in sensory dimension in the study group after intervention compared to placebo and control groups. The study results of Tsay et al.[29] and the results of the present study are consistent due to use of similar acupoints and length of intervention. The only difference is that there was no placebo group in their study, and in the control group, the mean score of sensory dimension had a reduction, possibly as a result of psychological and mental elements. Our results showed a significant reduction in the mean score of fatigue in cognitive dimension in the study group after intervention compared to the placebo and control groups, which can be due to the effects to acupressure mechanism and researcher's psychological and mental factors during the study. In the study of Harris et al.[31] in which the effect of the two methods of stimulating acupressure medicine and relaxation on students’ consciousness and fatigue was studied, stimulating acupressure significantly diminished students’ fatigue and increased their daytime consciousness. Their consistent results with the present study may be due to the effect of acupressure mechanism, while there was no difference in the placebo group in this study.
Our results showed a significant reduction in the mean score of fatigue in behavioral dimension after intervention in the study group compared to the placebo and control groups, as the acupoints used in the present study could have had a synergic effect to reduce fatigue.
Hosseinabadi et al.[32] reported that acupressure was effective on the daily function of Pittsburgh Sleep Quality Scale in the elderly in the study group, and there was a significant difference between the study and placebo groups, which is not consistent with our study possibly due to the difference in study population.
The results showed a significant reduction in the mean score of fatigue severity in the study group after intervention compared to the placebo and control groups. In a study of Molassiotis et al.,[30] the mean reduction score of fatigue severity in acupuncture group was more than in acupressure and placebo groups, which is not consistent with the results of the present study. This difference seems to be as a result of the type of intervention, length of time, frequency of intervention, the acupoints used, and/or the measurement scale used.
Based on most of the experts’ ideas, sham acupoints also have a treatment effect as most of the time, positive effects also occur in the placebo groups.[33] With regard to the inefficiency of the used acupoint in the placebo group, patients’ reduction of signs can be as a result of their expectation concerning a positive effect from the intervention domination and/or they felt secure by the presence of the researcher as well as Hawthorne effect.
CONCLUSION
The results of the present study with regard to consideration of fatigue as a problem in hemodialysis patients and application of acupressure medicine by nurses in most of their clinical interventions showed that this non-invasive, cost-effective, learnable, and complication-free method can be used to lower the fatigue in hemodialysis patients. Therefore, this caring method of complementary medicine is suggested to be used by nurses in hemodialysis wards to lower the patients’ fatigue.
ACKNOWLEDGMENTS
This article is from an MS thesis approved by Isfahan University of Medical Sciences, project number is 390303. The authors appreciate the Research Deputy and the Chief of School of Nursing and Midwifery, Isfahan University of Medical Sciences. They would like to thank all the participating patients, management of social security in Isfahan, and all the staff of dialysis centers in Dr. Shariati, Alzahra, and Noor hospitals for their assistance in conducting the present study.
Footnotes
Source of Support: Research Deputy of School of Nursing and Midwifery, Isfahan University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Atashpeikar S, Jalilaza T, Heidarzadeh M. Self-Care Ability in Hemodialysis Patients. JCS. 2012;6:29–33. doi: 10.5681/jcs.2012.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fauci B, Brounwald E, Kasper DL. 17th ed. Philadelphia: McGraw-Hill Co; 2008. Harrison's Principles of Internal Medicine; pp. 1761–72. [Google Scholar]
- 3.Nasiri E, Raei M, Vatani J, Kazemi R. Effect of acupressure on quality of sleep in hemodialysis patients. J Med Sci. 2011;11:236–40. [Google Scholar]
- 4.Bonner A, Wellard S, Caltabiano M. The impact of fatigue on daily activity in people with chronic kidney disease. J Clin Nurs. 2010;19:3006–15. doi: 10.1111/j.1365-2702.2010.03381.x. [DOI] [PubMed] [Google Scholar]
- 5.Mottahedian Tabrizi Z, Najafi Mehri S, Einollahi B, Babaei GH. Effect of programmed nursing care in prevention of hemodialysis complications. J Crit Care Nurs. 2009;2:55–9. [Google Scholar]
- 6.Kaba E, Bellou P, Iordanou P, Andrea S, Kyritsi E, Gerogianni G. Problems experienced by haemodialysis patients in Greece. Br J Nurs. 2007;16:868–72. doi: 10.12968/bjon.2007.16.14.24325. [DOI] [PubMed] [Google Scholar]
- 7.Jhamb M, Weisbord SD, Steel JL, Unruh M. Fatigue in patients receiving maintenance dialysis: A review of definitions, measures, and contributing factors. Am J Kidney Dis. 2008;52:353–65. doi: 10.1053/j.ajkd.2008.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cho Y, Tsay SL. The effect of acupressure with massage on fatique and depression in patients with end stage renal disease. J Nurs Res. 2004;12:51–8. doi: 10.1097/01.jnr.0000387488.63438.9a. [DOI] [PubMed] [Google Scholar]
- 9.O’Sullivan D, McCarthy G. Exploring the symptom of fatigue in patients with end stage renal disease. Nephrol Nurs J. 2009;36:37–9. 47. [PubMed] [Google Scholar]
- 10.Taylor CR, Lillis C, LeMone P, LeBon M, Lynn P. Philadelphia: Lippincott Williams and Wilkins; 2010. Study Guide for Fundamentals of Nursing: The Art and Science of Nursing Care. [Google Scholar]
- 11.Snyder M, Linquist R. New York: Springer Publishing Company; 2009. Complementary and alternative therapies in nursing. [Google Scholar]
- 12.Maa SH. Application of acupressure in nursing practice. Hu Li Za Zhi. 2005;52:5–10. [PubMed] [Google Scholar]
- 13.Monahan FD, Sands JK, Nighbors M, Marek JF. Phipps’ Medical-Surgical Nursing, Health and Illness Perspectives-EMEA Edition. Recherche. 2006;67:02. [Google Scholar]
- 14.Lee A, Done ML. The use of nonpharmacologic techniques to prevent postoperative nausea and vomiting: A meta-analysis. Anesth Analg. 1999;88:1362–2. doi: 10.1097/00000539-199906000-00031. [DOI] [PubMed] [Google Scholar]
- 15.Kim KH, Lee MS, Won Kang K, Choi S. Role of acupressure in symptom management in patients with end-stage renal disease: A systematic review. J Palliat Med. 2010;13:885–92. doi: 10.1089/jpm.2009.0363. [DOI] [PubMed] [Google Scholar]
- 16.Smith C, Collins C, Crowther C, Levett K. Acupuncture or acupressure for pain management in labour. Cochrane Database Syst Rev. 2011;7:1–58. doi: 10.1002/14651858.CD009232. [DOI] [PubMed] [Google Scholar]
- 17.Shiao SY, Dune LS. Metaanalyses of acustimulations: Effects on nausea and vomiting in postoperative adult patients. Explore (NY) 2006;2:202–15. doi: 10.1016/j.explore.2006.02.005. [DOI] [PubMed] [Google Scholar]
- 18.Tsay SL. Acupressure and fatigue in patients with end-stage renal disease-a randomized controlled trial. Int J Nurs Stud. 2004;41:99–106. doi: 10.1016/s0020-7489(03)00079-8. [DOI] [PubMed] [Google Scholar]
- 19.Kazemi M, Nasrabadi AN, Hasanpour M, Hassankhani H, Mills J. Experience of Iranian persons receiving hemodialysis: A descriptive, exploratory study. Nurs Health Sci. 2011;13:88–93. doi: 10.1111/j.1442-2018.2011.00586.x. [DOI] [PubMed] [Google Scholar]
- 20.Chang MY, Wang SY, Chen CH. Effects of massage on pain and anxiety during labour: A randomized controlled trial in Taiwan. J Adv Nurs. 2002;38:68–73. doi: 10.1046/j.1365-2648.2002.02147.x. [DOI] [PubMed] [Google Scholar]
- 21.Masoodi R, Mohammadi I, Nabavi SM, Ahmadi F. Affect of Orem based self-care program on physical quality of life in multiple sclerosis patients. Shahrekord Univ Med Sci J. 2008;10:21–9. [Google Scholar]
- 22.Zick SM, Alrawi S, Merel G, Burris B, Sen A, Litzinger A, et al. Relaxation acupressure reduces persistent cancer-related fatigue. Evid Based Complement Alternat Med 2010. 2011:32. doi: 10.1155/2011/142913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhuo F, Yong P, Wu F. Traditional Chinese medicine non medical therapy for regulation and treatment of chronic fatigue syndrome. Acupunct Tuina Sci. 2008;6:376–80. [Google Scholar]
- 24.Wu HS, Wu S, Lin JG, Lin LC. Effectiveness of acupreesure in improving dyspnoea in chronic obestructive pulmonary disease. J Adv Nurs. 2004;54:252–9. doi: 10.1046/j.1365-2648.2003.02886.x. [DOI] [PubMed] [Google Scholar]
- 25.Shin BC, Lee M. Effects of aromatherapy acupressure on hemiplegic shoulder pain and motor power in stroke patients: A pilot study. J Altern Complement Med. 2007;13:247–52. doi: 10.1089/acm.2006.6189. [DOI] [PubMed] [Google Scholar]
- 26.Tsay SL, Chen M. Acupressure and quality of sleep in patients with end-stage renal disease — A randomized controlled trial. Int J Nurs Stud. 2003;40:1–7. doi: 10.1016/s0020-7489(02)00019-6. [DOI] [PubMed] [Google Scholar]
- 27.Williams AG, Crane P, Kring D. Fatigue in African American women on hemodialysis. Nephrol Nurs J. 2007;34:610–7. 644. [PubMed] [Google Scholar]
- 28.So RC, NJ GK, Ng GY. Effect of transcutaneous electrical acupoint stimulation on fatigue recovery of the quadriceps. Eur J Appl Physiol. 2007;100:693–700. doi: 10.1007/s00421-007-0463-2. [DOI] [PubMed] [Google Scholar]
- 29.Tsay SL, Cho Y, Chen M. Acupressure and Transcutaneous Electrical Acupoint Stimulation in improving fatigue, sleep quality and depression in hemodialysis patients. Am J Chin Med. 2004;32:407. doi: 10.1142/S0192415X04002065. [DOI] [PubMed] [Google Scholar]
- 30.Molassiotis A, Sylt P, Diggins H. The management of cancer-related fatigue after chemotherapy with acupuncture and acupressure: A randomised controlled trial. Complement Ther Med. 2007;15:228–37. doi: 10.1016/j.ctim.2006.09.009. [DOI] [PubMed] [Google Scholar]
- 31.Harris RE, Jeter J, Chan P, Higgins P, Kong FM, Fazel R, et al. Using acupressure to modify alertness in the classroom: A single-blinded, randomized, cross-over trial. J Alternat Complement Med. 2005;11:673–9. doi: 10.1089/acm.2005.11.673. [DOI] [PubMed] [Google Scholar]
- 32.Hosseinabadi R, Norouzi K, Poursmaili Z, Karimlou M, Maddah SS. Acupoint massage in improving sleep quality of older adults. J Rehabil. 2008;9:8–14. [Google Scholar]
- 33.Kermanshahi S, Sadrizadeh R, Nafisi S. The effect of auto acupressure on reliefing headache in Migraine. Behbood. 2010;13:290–8. [Google Scholar]