

Abstract
Background:
Pain originating from intramuscular (IM) injection should not be underestimated, because it can damage the nurse–patient relationship. This research aimed at answering two main questions, whether acupressure is effective on pain severity due to IM injection or not and whether pain severity in two groups is different or not.
Materials and Methods:
This research was performed in government-affiliated hospitals of Ilam. The patients were 15-55 years old. Subjects were individually asked to participate in the research, and an informed consent was obtained from them. Before injection, the patients were asked to lie in prone position and the acupressure point UB32 was found. It was pressed for 1 min circularly. Then, the acupressure point was pressed directly (pressure equal to 4.5 kg/cm2) by thumb three times sequentially. After acupressure, 3 ml penicillin 6.3.3 was injected to buttock muscle. In the control group was injected only penicillin 6.3.3 by the conventional method. Collected data were analyzed by SPSS 16 version.
Results:
Means of pain intensity in the acupressure group according to body mass index values (BMIs) were 1.50 ± 0.75 in thin, 1.64 ± 0.72 in normal, 1.38 ± 0.60 in overweight, 1.40 ± 0.54 in obese, and 1 ± 0.0 in severely obese subjects, with a total score of 1.53 ± 0.68. Analysis of variance (ANOVA) showed no significant difference between mean pain intensities based on BMI. There was no significant difference in the two groups concerning BMI and age (age: 30.24 ± 10.98 vs. 29.26 ± 10.07; BMI: 23.74 ± 4.45 vs. 23.88 ± 5.74), but the difference between them in terms of pain intensity mean was statistically significant.
Conclusion:
It is concluded that acupressure in UB32 is effective on reducing the pain severity. Pain severity mean in the acupressure group was lesser than in the other group, and t-test showed a significant difference between the two groups.
Keywords: Acupressure, intramuscular injection, pain
INTRODUCTION
Intramuscular (IM) injections have been an integral part of drug administration for almost half a century. They are a common technique used to deliver medication into the large muscles of the body. More than 12 billion IM injections are administered annually throughout the world, of which about 5% are for immunization and the rest are given for curative purposes.[1] Pain is one of the most common causes of human sufferings, which is considered as a major health problem among adults.[2]
Pain originating from IM injection should not be underestimated, because a painful injection might incite severe fear of injection, which may lead a patient to delay seeking medical help.[3] Reducing patients’ pain is important for all nurses because of many reasons. Unnecessary pain can damage the nurse—patient relationship, whereas knowledge of alternative techniques can improve patient care and satisfaction.[2] Nurses have used various successful methods to control procedural pain, such as local cold therapy to inject heparin. However, this method is not effective with all the injections. Distraction has been effective to decrease the pain caused by blood sampling and intravenous vaccination injections;[2] other related methods have been reported such as music distraction for venipuncture.[4] Since these studies have often investigated venous injections and reported different outcomes, other researchers have recommended further studies in different cultural circumstances and with other painful procedures to improve patients’ pain control at different ages and to be able to generalize the previous findings better.[5]
Nowadays, palliative drugless or behavioral procedures such as acupuncture, acupressure, respiratory techniques, as well as music, touch, massage, and aqua therapies, are recommended.[6] Early healers found that certain techniques of rubbing and pressing relieved hemorrhage, decreased pain, and reduced swelling, all symptoms common to work-related injuries. Over the years, it became common knowledge that pressing in certain areas of the body could be used to treat diseases as well.[7]
There are different techniques for massaging, such as acupressure. Acupressure is a deep and effective hands-on treatment for many conditions as it is very relaxing and provides support for general health and well-being.[1] Experimental and clinical evidences suggest that acupressure may relieve pain and induce relaxation.[8] Acupressure is an ancient healing art that uses the fingers to press key points on the surface of the skin to stimulate the body's natural self-curative abilities. When these points are pressed, they release muscular tension and promote the circulation of blood and the body's life force to aid healing. Acupuncture and acupressure use the same points, but acupuncture employs needles, while acupressure uses the gentle but firm pressure of hands (and even feet).[9] UB31, UB32, UB33, and UB34 together form the “Eight Liao” points and are all useful for local low back and/or sacrum problems and most genital and urinary-related disorders. Of these, UB32 is most often used clinically.[10] It is indicated for low back pain, hernia, irregular menstruation, leukorrhea, dysmenorrhea, nocturnal emission, impotence, enuresis, dysuria, muscular atrophy, pain, numbness, and motor impairment of the lower extremities.[11]
In this research, we used UB32 point for relieving pain, and pain intensity was measured by visual analogue scale (VAS) because evaluation of pain and subsequent nursing care plans to reduce pain are the necessary steps for reduction of pain in young patients. The most reliable way to evaluate the level of pain is to make use of verbal responses to questions about perceived pain.[12]
MATERIALS AND METHODS
This research was performed in government-affiliated hospitals of Ilam (Emam Khomaieni, Shahid Mustafa, and Ayatollah Taleghani hospitals) in the west of Iran after obtaining permission from hospital authorities and approval from nursing and midwifery faculty research council committee. The subjects were selected by purposeful sampling method. The patients who were included in this study were 15-55 years old, had no history of IM injection in two previous weeks, and were not in luteal phase of menstruation. They were prescribed penicillin 6.3.3 and referred to emergency units of the above-mentioned hospitals from April till October 2009.
This was a single-blind clinical trial in which 150 women were assigned randomly to two groups: 75 subjects in convention injection group and 75 in acupressure group. Each sample was individually asked to participate in the research and give an informed consent. The researchers informed them they had the right to withdraw from the study at any time. Before injection, the patients were asked to lie in the prone position. The acupressure point (UB32) was found in the injection side [Figure 1]. UB32, Ciliao (English translation: second crevice), is located in the region of the sacrum, medial and inferior to the posterior superior iliac spine, in the second sacral foramen.[11]
Figure 1.
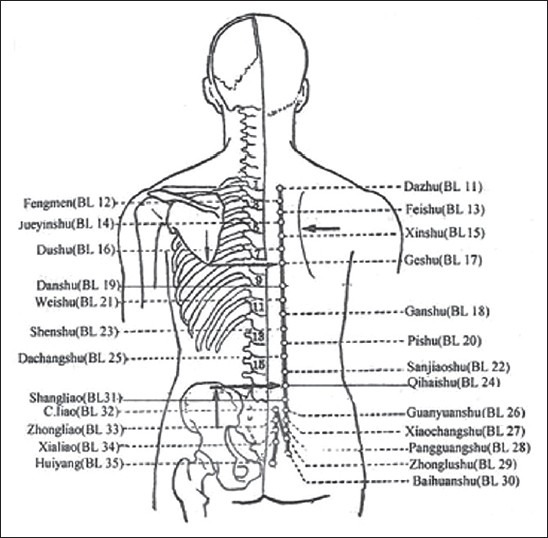
Location of UB32 (Ciliao); adapted from http://www.acupuncture.com[13]
The acupressure point UB32 was pressed for 1 min circularly. Then, the acupressure point was sequentially pressed directly (pressure equal to 4.5 kg/cm2) by thumb three times. After acupressure, 3 ml penicillin 6.3.3 was injected to buttock muscle. In the control group, only penicillin 6.3.3 was injected by the conventional method. All the injections were performed by the researcher who was aware of the anatomical location of acupressure points, especially pelvic ones (such as G.B-30). The researchers explained the questionnaire and VAS to the patients. The most severe pain was scored 10 and no pain was scored 0. Collected data were analyzed by SPSS 16, and statistical tests such as t-test, analysis of variance (ANOVA), and descriptive statistics (concrete frequency).
RESULTS
The findings of the present study showed that with regard to body mass index (BMI), 25 subjects (16.7%) were thin, 50 (50%) normal, 34 (22.7%) overweight, 13 (8.7%) obese, and 3 subjects (2%) were severely obese [Table 1]. Mean and SD of pain severity in the acupressure group based on age groups of 15-25, 25-35, 35-45, and 45-55 years were 1.58 ± 0.62, 1.60 ± 0.75, 1.53 ± 0.87, and 1.27 ± 0.46, respectively, while these indices were 4.1 ± 0.84, 3.63 ± 0.84, 3.69 ± 0.75, and 3.28 ± 1.60, respectively, in the conventional injection group. Table 2 shows that the means of pain intensity in the acupressure group according to BMIs were 1.50 ± 0.75 in thin, 1.64 ± 0.72 in normal, 1.38 ± 0.60 in overweight, 1.40 ± 0.54 in obese, and 1 ± 0.0 in severely obese subjects, with a total score of 1.53 ± 0.68. ANOVA showed no significant difference between mean pain intensities based on BMI.
Table 1.
Frequency distribution of research participants according to BMI
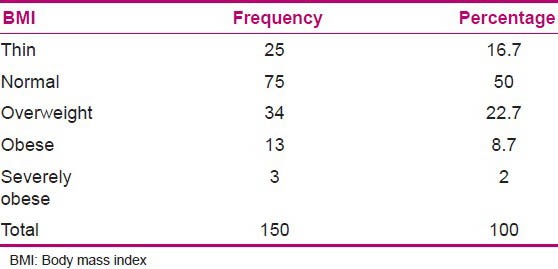
Table 2.
Mean of pain severity in acupressure group according to BMI
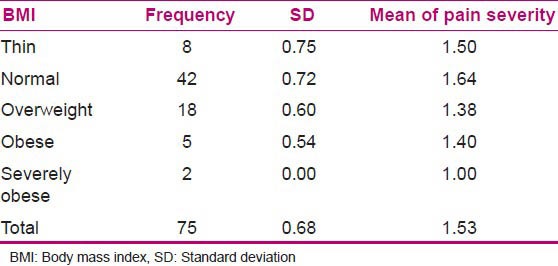
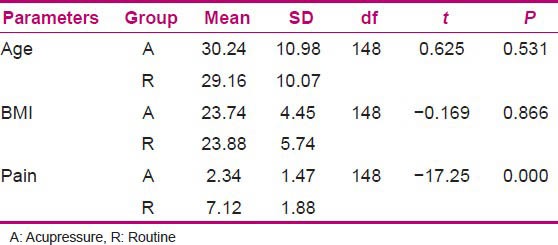
Table 3 shows that the difference between the acupressure and conventional groups concerning BMI and age was not significant (age: 30.24 ± 10.98 vs. 29.26 ± 10.07, t = 0.0625, df = 148, P = 0.531; BMI: 23.74 ± 4.45 vs. 23.88 ± 5.74, t = 17.25, df = 148, P = 0.866), respectively, but the difference between two groups in relation with pain intensity mean was statistically significant (2.34 ± 1.47 in the acupressure group vs. 7.12 ± 1.88 in the conventional group, t = 17.25, df = 148, P = 0.00).
Table 3.
Comparison of mean and SD of age, BMI, and pain in the two groups
DISCUSSION
Literature review showed that there are limited researches in respect to IM injection pain and acupressure.
This research aimed at finding the answers to two main questions. Firstly, it aims to find whether acute pressure in UB32 is effective on pain severity resulting from IM injection or not. According to Table 3, the means of pain severity in acupressure and conventional injection groups were 2.34 and 7.12, respectively. So, the answer to the first question was positive, and we concluded that exertion of pressure in UB32 is effective on severity of pain. With regard to the second question of the research (whether pain severity in two above-mentioned groups is different or not), as observed in Table 3, pain severity mean in acupressure group was 4.78 (less than the other group) and t-test showed a significant difference between the two groups (t = 17.25, P = 0.00); therefore, the answer to the second question was positive too.
The result of this study is consistent with that of Alavi's (2007) research. She studied the effectiveness of acupressure in reduction of IM injection pain in patients referring to emergency center, in which two groups of patients with injections of the same drug were compared. One injection was followed by application of acupressure and the other without it. The numerical VAS from 0 to 10 was used for pain measurement. Findings showed that mean pain score was 5 without acupressure and 3 with it (P < 0.001). Nevertheless, in the above study, the acupressure technique was significantly more effective in males than in females (P < 0.001) and age had a significant reverse relationship with pain sensation. However, in our research, the subjects were females because of the limitations in men giving injection to women. All injections were administered by a female nurse, and with respect to age, in our study, the two groups had no significant difference in pain severity mean.
Our findings are in agreement with Barnhill et al. and Chung et al., studies, but they investigated the use of simple manual pressure to reduce pain in IM injections. They did not assess the effect of pressure to special sites such as acupressure site.[14,15]
CONCLUSION
We conclude that acupressure in UB32 is effective on severity of pain. Pain severity mean in the acupressure group was lesser than in the other group and t-test showed a significant difference between the two groups.
ACKNOWLEDGMENT
We thank all the patients who participated in the study and the emergency units for their contribution to the study.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
REFERENCES
- 1.Alavi N. Effectiveness of acupressure to reduce pain in intramuscular injections. Acute Pain. 2007;9:201–5. [Google Scholar]
- 2.Hasanpour M, Tootoonchi M, Aein F, Yadegarfar G. The effects of two non-pharmacologic pain management methods for intramuscular injection pain in children. Acute Pain. 2006;8:7–12. [Google Scholar]
- 3.Ozdemir L, Pınarcı E, Nisa Akay B, Akyol A. Effect of Methylprednisolone Injection Speed on the Perception of Intramuscular Injection Pain. Pain Manag Nurs. 2010;14:3–10. doi: 10.1016/j.pmn.2010.03.002. [DOI] [PubMed] [Google Scholar]
- 4.Sparks L. Taking the” ouch” out of injections for children: Using distraction to decrease pain. MCN Am J Matern Child Nurs. 2001;26:72–8. doi: 10.1097/00005721-200103000-00005. [DOI] [PubMed] [Google Scholar]
- 5.MacLaren JE, Cohen LL. A comparison of distraction strategies for venipuncture distress in children. J Pediatr Psychol. 2005;30:387–96. doi: 10.1093/jpepsy/jsi062. [DOI] [PubMed] [Google Scholar]
- 6.Taghinejad H, Delpisheh A, Suhrabi Z. Comparison between massage and music therapies to relieve the severity of labor pain. Women's Health (Lond Engl) 2010;6:377–81. doi: 10.2217/whe.10.15. [DOI] [PubMed] [Google Scholar]
- 7.Dune L. Integrating tuina acupressure and traditional Chinese medicine concepts into a holistic nursing practice. Explore (NY) 2006;2:543–6. doi: 10.1016/j.explore.2006.08.011. [DOI] [PubMed] [Google Scholar]
- 8.Cheesman S, Christian R, Cresswell J. Exploring the value of shiatsu in palliative care day services. Int J Palliat Nurs. 2001;7:234–9. doi: 10.12968/ijpn.2001.7.5.12637. [DOI] [PubMed] [Google Scholar]
- 9.Gach MR. Acupressure Foundations and Introduction [11/4/2011] [Last accessed on 2011 Mar 19]. Available from: http://www.acupressure.com/articles/acupressure_foundations.htm .
- 10.UB32 Acupuncture Point - Ci Liao - Bladder Meridian [11/4/2011] 2011. [Last accessed on 2011 Mar 19]. Available from: http://www.yinyanghouse.com/acupuncturepoints/ub32 .
- 11.Urinary Bladder 32 (UB 32). acufinder.com. 2013. [Last accessed on 2013 July 07]. Available from: https://www.acufinder.com/Acupuncture+Points/Ciliao/163 .
- 12.Celebioglu A, Akpinar RB, Tezel A. The pain response of infants in Turkey to vaccination in different injection sites. ApplNurs Res. 2010;23:101–5. doi: 10.1016/j.apnr.2008.03.003. [DOI] [PubMed] [Google Scholar]
- 13.UrinaryBladder32.[12/4/2011] [Last accessed on 2011 Mar 18]. Available from: http://acupuncture.com/education/points/urinarybladder/ub32.htm .
- 14.Barnhill BJ, Holbert MD, Jackson NM, Erickson RS. Using pressure to decrease the pain of intramuscular injections. J Pain Symptom Manage. 1996;12:52–8. doi: 10.1016/0885-3924(96)00049-8. [DOI] [PubMed] [Google Scholar]
- 15.Chung JW, Ng WM, Wong TK. An experimental study on the use of manual pressure to reduce pain in intramuscular injections. J Clin Nurs. 2002;11:457–61. doi: 10.1046/j.1365-2702.2002.00645.x. [DOI] [PubMed] [Google Scholar]