

Abstract
Background:
The purpose of this qualitative exploratory study was to explore the views of nursing trainers and students about nursing students’ clinical evaluation problems and drawbacks in Shiraz Nursing and Midwifery School.
Materials and Methods:
A qualitative exploratory approach was used in this study at Shiraz Nursing and Midwifery School in 2012. A purposeful sample of 8 nursing instructors and 40 nursing students was interviewed and the data on their opinions about the problems of the clinical evaluation were collected through semi-structured deep interviews. Initially, four open-ended questions, which were related to the clinical evaluation status, problems, were used to stimulate discussions in the interview sessions. Content analysis was employed in order to analyze the transcribed data. The recorded interviews were initially transcribed, read, and reread on a number of occasions to get an overall feeling of what the participants were saying. Each line or incident was described, and then a code, which reflected the essence of the participants’ comments, was given.
Results:
The codes were compared for similarity and differences, merged together, and categorized. Finally, five themes emerged: In appropriate clinical evaluation method, problems of clinical evaluation Process, problems related to clinical instructors, unsuitable programming of clinical education, and organizational shortcomings.
Conclusion:
Besides focusing on upgrading the current clinical evaluation forms, nursing trainers should improve their knowledge about a complete and comprehensive clinical evaluation. They should also apply other appropriate and objective clinical evaluation methods and tools, and perform a formative and summative clinical evaluation. Also, workload adjustment of the nursing trainers needs revision. Therefore, despite using traditional and sometimes limited evaluation methods for assessing nursing students, a co mprehensive and appropriate evaluation of nursing students’ clinical competencies seems necessary.
Keywords: Baccalaureate, challenges, clinical, evaluation, nursing, student, Iran
INTRODUCTION
Nursing education involves both theoretical and practical training processes. Clinical training is considered as an indispensable and very important part of professional nursing education.[1] Clinical education is recognized as an essential and highly significant component of professional education for nursing.[2] Practical clinical skills lie at the heart of nurses’ professional practice; therefore, the mastery of fundamental clinical skills is an important component of courses leading to registration.[3] Since nursing is a discipline based on practice, there needs to be a curriculum of education that offers students the opportunity to develop their clinical skills, particularly the patient care skills.[4] Clinical practice is one of the ways used to increase the nursing students’ professional competence. Nursing teachers must be in charge of clinical practice because they are the ones ultimately responsible for learning in the clinical practice.[5] Thus, it is in the clinical area that students must relate theory to practice, learn the necessary technical and interpersonal skills, make clinical judgments, become socialized into the profession, and begin to appreciate its values and ethics. The development of competent practice is a primary goal for nursing education. To demonstrate this competence, graduates must be able to practice in the “real word.”[2]
Clinical competence evaluation is defined as an integrated form of evaluation seeking to combine knowledge, understanding, problem solving, technical skills, attitudes, and ethics in evaluation.[6] Evaluation, as a way of determining the clinical competence, is one of the fundamental principles of development and student achievement measurement in nursing education.[7] In clinical evaluation, it must be ensured that the students in clinical settings have an appropriate professional behavior, establish an appropriate interaction with the patients, prioritize the problems, have the basic knowledge about clinical methods, perform the care procedures correctly, and apply critical thinking.[8] The evaluation of clinical practice is a complex process that continues to tax nurse educators.[3] It can be stated that the evaluation of nursing students in clinical practice is a problem and the one which cannot be solved. Nursing literature abounds with papers that discuss this long-running and difficult problem. Much of the discussion centers on the thorny issue of subjectivity and a plethora of clinical evaluation tools has been devised and abandoned in the quest to overcome this ongoing dilemma. Wood (1982) proposes that the problem probably persists because clinical evaluation relies upon the observation of the performance of one individual by another, which itself is inevitably subjective. This suggests that the issue of subjectivity might be addressed only if some other methods of clinical evaluation were to be devised.[9] Clinical evaluation of students is always an area of controversy and concern. Students often register complaints of variations in teacher expectation and of subjectivity in grading.[10] Many issues have been raised in the evaluation of nursing clinical skills, which indicate the existence of various problems in this field. Some of the problems raised in this field include the heterogeneity of devices used from year to year and from period to period, inconsistency in the evaluation process by the clinical instructors, and lack of an appropriate framework for showing the students’ improvements. Evaluation of clinical practice is often faced with problems such as low credit of existing methods of evaluating the students’ performance and inability to evaluate the level of theoretical and practical knowledge of the students. Besides, some students believe that the evaluation tools do not pay much attention to the students’ practical skills. On the other hand, in some studies, the students stated that clinical evaluation by the clinical instructors is one of the major problems experienced in the clinical practice. In general, the problems of clinical evaluation appear in the form of nursing students’ complaints, reporting differences in clinical evaluation and multiple visits between the students and the nursing instructors. Researchers have also seen the students’ dissatisfaction in their evaluation status and the results of the clinical evaluation. Following the announcement of the clinical evaluation results, many students protest about their evaluation scores to the clinical instructors and raise various issues. Despite some considerable efforts made in order to solve the problem, clinical evaluation challenges are still continuing.[8]
In this regard, Imanipour et al. indicated that most students considered their clinical evaluation (by using clinical evaluation forms) inappropriate and disagree with it. Their teachers also have similar attitude, disagree with the current clinical evaluation, and do not consider it appropriate. The research findings also indicated that 96.4% of the students just knew their marks, while they did not know their strengths and drawbacks. Besides, 87.8% of them said that they received their internship marks after they finished their course. 79.6% of the students believed that internship marks represented teachers’ personal attitude and not the clinical evaluation of the students. 82.1% of the teachers believed that various evaluation methods must be applied to evaluate the students’ clinical performance. Some methods recommended in this regard by students and their teachers included written tests, verbal tests, Objective Structured Clinical Examination (OSCE), nurse and head nurses’ views, etc., Besides, 89.3% and 92.3% of teachers stated that the current evaluation forms of students need to be modified to improve their quality. Some of the suggestions proposed by teachers and students regarding the improvement of clinical evaluation included specialization of clinical evaluation forms in accordance with the academic semester, the type of internship, and modification of general items to specific items to be exact in evaluating the students’ performance.[11]
In our nursing and midwifery college, since the beginning of nursing clinical education, the clinical environment has been looked through the training point of view. Moreover, the nursing students were expected to perform clinical practice with the instructors’ supervision and repeat these practices; however, their competency level was never taken into account. This view has also been transferred to the next generations. It seems that the nursing instructors participate in training the students’ function in the clinical environment with the aim of education and training rather than evaluation. These nursing instructors tend to teach and promote the nursing students’ abilities habitually. The purpose of this qualitative exploratory study was to explore the views of nursing trainers and students about nursing students’ clinical evaluation problems and drawbacks in Shiraz Nursing and Midwifery School. Understanding the nursing students’ clinical evaluation problems in this school may provide insights about other Iranian nursing and midwifery schools, as well as the ones which share the same history and challenges.
MATERIALS AND METHODS
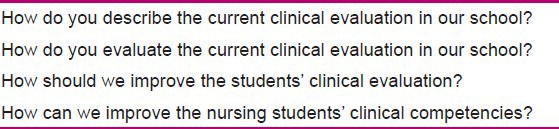
A qualitative exploratory approach[12] was used in this study at Shiraz Nursing and Midwifery School in 2012. A purposeful sample of 8 nursing instructors and 40 nursing students was interviewed and the data on their opinions about the problems of the clinical evaluation were collected through face-to-face deep semi-structured interviews. The enrolment criteria were as follows: (1) participants were female and male senior nursing students; (2) they were willing to participate in the study; (3) and they were nursing trainers with at least 10 years of relevant nursing students’ training experience. Each deep interview lasted for at least 2 h. Data collection and analysis proceeded concurrently, and once the themes were identified and data saturation was achieved, the interviews were discontinued. Prior to recording the interviews, the objective of the study was verbally clarified for each participant and the participants’ questions were answered. A written explanation was also provided to the participants and accepted by them through a written consent form. None of the participants had any concerns about signing the consent. Initially, four open-ended questions, which were related to the clinical evaluation status, were developed and used to stimulate discussions in the interview sessions [Table 1].
Table 1.
Interview probes
DATA ANALYSIS
Directed content analysis was employed in order to analyze the transcribed data. Initial analysis focused on understanding the information, and developing codes and categories through identification of persistent words, phrases, themes, or concepts within the data.[13] The analytic process was utilized to gain familiarity with the data during the transcription and translation. For coding the transcript, it was necessary to go through the transcripts line by line and paragraph by paragraph to look for significant statements and codes according to the topics addressed.
Overall, three levels of coding were selected as appropriate to code the data.
Level 1: Examining the data line by line and making codes taken from the language of the subjects who attended the focus groups and deep interviews
Level 2: Comparing the coded data with other data and creating the categories. In fact, the categories are simply the coded data which seem to cluster together and may result from condensing of the codes
Level 3: Describing the clinical evaluation problem which is the title given to the central themes that emerge from the categories.[14]
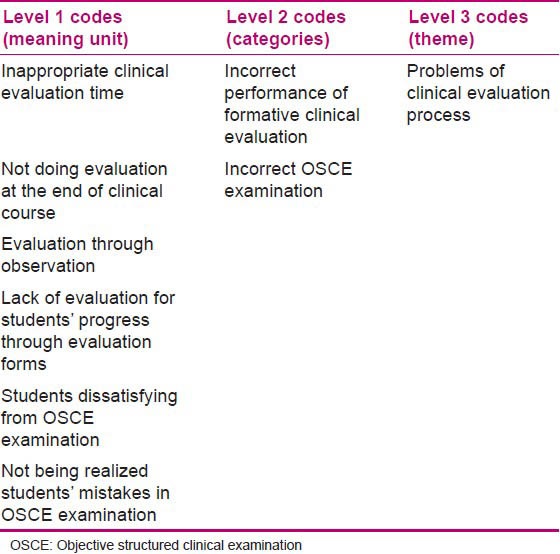
The recorded interviews were initially transcribed, read, and re-read on a number of occasions to get an overall feeling of what the participants were saying. Each line or incident described was then given a code, which reflected the essence of the participants’ comments. Codes were then compared for similarity and differences, merged together, and categorized. Table 2 shows the three levels of codes for one of the themes.
Table 2.
Examples of three levels of coding
Through this process of analysis and comparison, the following themes emerged: Inappropriate clinical evaluation method, problems of clinical evaluation Process, Problems related to clinical instructors, unsuitable programming of clinical education, and organizational shortcomings.
The measures used in the present study for establishing the rigor are “truth value,” “applicability,” “consistency,” and “neutrality.” Truth value reflects the extent to which the study reveals the participants’ descriptions, which they are able to identify later on as their own. The results of the present study were shown to 10 participants, who confirmed the findings as being a reflection of their original descriptions. Applicability is considered as the extent to which the study findings fit outside contexts. It was enhanced in the present study by returning to the participants of the study for confirmation of the findings. Consistency reflects the extent to which the study can be judged as auditable. It was enhanced in the study by ensuring that the interview situation was stable and consistent throughout the data gathering. The interviews were recorded, so that they could be listened over and over again. Neutrality should be judged in qualitative research by confirmability, which is achieved through auditability, applicability, and consistency. To enhance neutrality, the researcher carefully considered his own perceptions and pre-assumptions toward nursing students’ clinical evaluation. This proved to be useful because the researcher had a lot of experience in the field of nursing education.[15]
Ethical considerations
Institutional Review Board's (IRB) approval for the study was obtained from the Ethics Committee of Shiraz University of Medical Sciences (ECSUMS). In addition, permission to conduct the study was obtained from the Dean of the Faculty of Nursing and Midwifery. Furthermore, the confidentiality of the interview data and the personal identity was assured and the participants’ right to withdraw from the study at any time was also explained.
RESULTS
In the present study, 8 nursing instructors and 40 nursing students where sampled; among them, 60% of the students (aged between 19 and 22 years) and 88% of the faculty instructors (aged between 42 and 49 years) were females. The qualitative analysis led to the emergence of five major themes from the deep interview data. From the students’ and their instructors’ points of view, the following five themes and nine categories were considered as the important clinical evaluation problems: “Inappropriate clinical evaluation method (inappropriate evaluation forms for evaluation of other clinical capabilities of nursing students, subjective clinical evaluation),” “problems of clinical evaluation Process (incorrect performance of formative clinical evaluation, incorrect OSCE examination),” “problems related to clinical instructors (lack of instructors’ free time, instructor's weakness in clinical evaluation, collecting insufficient data from the students),” “unsuitable programming of clinical education (the limitation of clinical training time),” and “organizational shortcomings (the lack of unified laws and regulations).”
Inappropriate clinical evaluation method
In spite of the fact that nursing instructors highly rely upon the clinical evaluation forms for evaluating the students, the students are worried that the current clinical evaluation forms are not sufficient and appropriate for their clinical evaluation. Nursing instructors also admit that these evaluation forms are necessary but not adequate for clinical nursing evaluation.
Since other professional nursing students’ clinical competencies, particularly communication skills, decision-making skills, and critical thinking skills, cannot be measured through these evaluation forms, professional skills (affective learning objectives) show themselves more prominently and measurement of this domain also poses the issue of the evaluator bias; therefore, some nursing students are more concerned about this issue. To measure some clinical competencies, particularly clinical procedure skills and clinical decision-making skills, through objective nursing process, other tools are required. Since the clinical evaluation forms are more widely used and these instruments are the only evaluation tools, the inclusion of all clinical learning objectives in these forms leads to problems in scoring the nursing students, resulting in their protest. As the findings indicated, since the learning objectives of the current clinical evaluation forms are numerous, hard to understand, and are not practical, the instructors tend to perform a subjective evaluation and rely on their mentality in order to evaluate the students.
Inappropriate evaluation forms for evaluation of other clinical capabilities of nursing students
Nursing students stated thus:
“Nursing instructors usually use the current evaluation forms to grade the students. The learning objectives of the current clinical evaluation forms are numerous and hard to understand. The learning objectives of the current clinical evaluation are not practical too. They are not able to evaluate the competent students. They cannot distinguish the competent students from the moderately competent ones. These forms emphasize professional skill (the affective learning objectives) of the nursing students more.”
One of the nursing instructors confirmed thus:
“We all believe that these clinical evaluation forms aren’t efficient. They are necessary but not efficient. As you say, these forms, as a primary tool, are helpful for clinical evaluation but they don’t measure all the issues in our mind. Particularly, they don’t measure the student's progress and achievement.”
Subjective clinical evaluation
Regarding this point, one of the nursing instructors said:
“Unfortunately, we cannot perform the nursing student's clinical evaluation objectively. My own evaluation method as an instructor also has problems. The only thing that makes our evaluation subjective and actual is the mentality that we already have about the students’ scores as well as reactions and behavior of the students.”
Another nursing instructor claimed thus:
“We know that a large number of the current evaluation forms options are not objective. We should work more on them. We have revised the current evaluation forms each semester. We should definitely use other evaluation methods in addition to the current evaluation forms to do better clinical evaluation. The current evaluation forms should be revised.”
Problems of clinical evaluation process
Because clinical evaluation is limited to the use of clinical evaluation forms and the instructors complete these forms at the end of the course, and on the other hand, they do not have other clinical evaluation instruments to do formative evaluation, the student's achievement and their clinical learning process cannot be assessed appropriately. In order to improve clinical evaluation, during the course, some OSCE examinations are incoherently performed for some nursing students and instructors do not provide students with feedback during and after OSCE examination; then, the students do not realize where their problems are. So, the students are dissatisfied to participate in it. It seems that formative evaluation such as OSCE examination should be conducted in a higher quality for the students, and other evaluation tools and methods should be added. Incorrect performance of formative clinical evaluation
One of the instructors said:
“Items in the clinical evaluation forms especially don’t measure the students’ progress and achievement. The clinical evaluation forms don’t involve the clinical procedure stages. If we aim to evaluate the students through these forms again, we mark many items in the evaluation forms which haven’t been in clinical evaluation.”
Incorrect OSCE examination
The students stated thus:
“OSCE examination is conducted under time conditions. This examination is stressful. Stress and fraud of the OSCE examination is very high. Most students do not like OSCE examination. They don’t understand where their problem is. No feedback is given to the students. OSCE grading has no value. Since the facilities and stages of performing the clinical procedures during OSCE examinations are not the same as actual issues in the clinical setting, the clinical procedures that we practice at the hospital are highly incomplete compared to the OSCE procedures.
Problems related to clinical instructors
The instructors accepted that they did not perform the clinical evaluation of the students in a timely manner. They stated that their workload is high and they do not have sufficient opportunity and time to identify the students during a semester. Due to the fact that they perform clinical evaluation without having any objective evidence, the students may have objections about their scores, so they try to give higher score to the students.
One of the clinical evaluation objectives that the instructors expect their students to perform in the clinical training was their clinical conference presentations in the clinical wards. The students complained that conference topics were not original and topics were not selected on the basis of ward common diseases; therefore, they were prepared and provided only for performing some tasks by students. In order to perform an objective evaluation of the students, instructors strived to give cognitive written tests at the end of the semester, but the students objected to irrelevant content of these tests compared with those they had experienced during the clinical training.
Students stated that instructors do not know what they expect the students to do during their apprenticeship and what they should learn. Instructors did not have enough information to score the students’ clinical evaluation forms, and the students were not assessed based on their competencies. To score the students based on the evaluation forms, there are options on the evaluation forms which are not related to them. According to the issues mentioned above, the inclusion of abundant clinical objectives for education and evaluation is a difficult task and causes the instructors not to understand the students well enough and not to reach all the identified objectives.
Lack of instructors’ free time
One of the nursing instructors said thus:
“One of our problems is that we do not have enough time. Sometimes, I don’t have time to write the anecdotal note. We cannot reach all the clinical objectives in this short period of time. Due to the lack of time, we assess the students at the end of the semester which isn’t really an appropriate time. The students do not spend much time with the instructor in the clinical field. As a result, the instructors do not have enough opportunity to understand the students; therefore, reduction of the training duration might be the reason why we cannot assess the students better.”
Another nursing instructor stated thus:
“My student doesn’t know where and what her/his weaknesses are. Clinical evaluation method of some of us also has problems because we don’t evaluate the students on-time. I evaluate the students when they have finished their semester, and this isn’t really an appropriate time. Finally, in order to avoid the students’ complaints about their scores, I try to give them higher scores.”
Instructor's weakness in clinical evaluation
One of students said that:
“Our instructors ask their students to present the clinical conferences as a lecture; however, the conference topics are quite irrelevant to the ward diseases. The conference topics are repeated. It is just translated and handed on to the instructors. Some instructors give tests to their students at the end of the course; however, the exam questions are not ideal for that ward.”
Collecting insufficient data from the students
Regarding this point a student said thus:
“Each instructor has his/her own special rule. Each instructor acts as she/he wishes. We don’t know what the nursing instructors want us to do. We don’t know what we are supposed to learn since the instructors score the students based on their speculations; sometimes a student who is very capable and another who performs quite moderately receive the same scores. Once, although I thought I would fail, I got a high score. By performing the current clinical evaluation, positive and quiet students can get good grades. The instructors think that since the student has already passed apprenticeship, he/she knows all the things. I do clinical practice and my instructor doesn’t know what I did. I can say I do this work, but I do nothing. The instructors like the students who show off and give them higher grades. The instructor stated that, I have used feminine ornament when I complained about this issue; she/he says you are right, I made a mistake.”
Unsuitable programming of clinical education
The clinical training and learning highly depend on the clinical environment. There is a variety of clinical practices in medical-surgical nursing. Planning for teaching and learning nursing competencies causes a great number of problems in training and evaluations; it requires much effort for coordinating and integrating its educational objectives. It should be noted that the clinical environment is an unpredictable one and its control is almost beyond the instructors’ capabilities and all the students don’t reach the same level of competency in a period of time. On the other hand, the clinical teaching time is limited and the number of wards needed for the clinical training is also diverse and abundant, which will cause problems for its planning. Instructors expressed that the time period of the students’ clinical training and evaluation is limited, so they cannot identify accurately and adequately the students’ competencies, cannot reach all the objectives of clinical evaluation forms, and do not have enough evidence for evaluating the students. The limitation of clinical training time
One of the nursing instructors said thus:
“In addition to the problems of evaluation tools, another problem is the short period of time that a student spends with an instructor. Most of our training courses last for 6 days. We go to clinical ward for 2 three-day weeks and we may rarely be with our students for 15-16 days and this period of time is quite short for understanding the students’ clinical practice.”
Organizational shortcomings
So far, planning, implementation, and monitoring of most faculties’ educational programs have been performed intra-organizationally, based on the opinion of a low level group of officials and instructors. Although observing the regulations and standards has been mentioned to all the instructors by group authorities, implementation of these regulations has been faced with shortcomings and has not been performed in a coherent manner. This problem has caused the students to be faced with different rules and be dissatisfied with the act of higher level of management in this regard. The students particularly protested against the instructors’ decisions about their absences and tardiness.
Lack of unified laws and regulations
Considering this points one of the students said that:
“All the instructors do not act the same. An instructor cares about the students’ absenteeism, while another one acts differently. For instance, some instructors do not care about the students’ absences and being absent doesn’t affect the students’ scores. Moreover, some instructors let the students have breaks but do not care about their tardiness.”
DISCUSSION
The results of the present study revealed that the most important clinical evaluation problem was lack of a comprehensive and appropriate evaluation tool for assessing the students. On one hand, in the case of lack of objective and credible clinical evaluation tool, the clinical evaluation forms are more appropriate than the students’ observation by instructors. On the other hand, since the options of the current clinical evaluation forms do not objectively measure the students’ clinical competencies and learning process, the instructors cannot differentiate the competent students from moderately competent ones and this leads to instructor's bias.
Our findings in this regard are in agreement with the reports by Norman et al., indicating that clinical evaluation traditionally relies upon observation of the performance of one individual by another, which runs the risk of observer bias. In an attempt to overcome this problem, a plethora of clinical evaluation tools has been developed and subsequently abandoned.[16] The study findings revealed that the girls’ and boys’ capabilities are predominantly different, and since most of the nursing teachers and students were females, the nursing instructors seem to pay more attention to female students. As a result, some male students complained that their clinical competencies are ignored in clinical settings. In spite of the fact that most nursing instructors have got used to the clinical evaluation forms, and they provide and revise them each semester to grade the nursing students however the students were dissatisfied with their gradings. The nursing students complained that the current evaluation forms cannot evaluate the learning psychomotor, decision-making, and critical thinking objectives, as well as the students’ learning progress. To grade the nursing students, some instructors used norm-referenced evaluation and gave the students a grade as a whole; they compared the students with each other and then graded them.
Inherent to the clinical evaluation process is judgment and subjectivity, and this subjective process is further influenced by biases of both the evaluator and student, as well as by variables present in the clinical environment. On one hand, the students must be evaluated in the clinical setting, and on the other hand, at the heart of evaluation is “judgment and bias,” which is inherent in the human evaluation process. They must keep in mind that they are observing the student's behavior, and only that must be evaluated.[17] Evaluation of learning is problematic in practical disciplines because it requires direct observation of the students engaged in actual practice in unpredictable clinical environments.[18]
In a study by Vaismoradi et al. (2010), the participants’ dissatisfaction of the way instructors supervised them in the clinical setting also was revealed. Imprecise and inexplicit supervision conducted by instructors made the students resentful. No connection could be made between their scores and clinical work because they were not seen when caring for patients. The issue of the students’ gender was highlighted as a potential cause for unfair and unexpected evaluation outcomes. The male participants claimed that female instructors discriminate between the students of the opposite sex.[19]
Moreover, the study findings indicated that the nursing instructors did not perform formative clinical evaluation during a semester and did not have tools for doing it. Since they do not have enough information about each nursing student's progress and achievement, they cannot train the nursing students for the next stages of clinical competencies. Finally, they are forced to score the students without any clinical learning evidences.
Before starting any teaching episode, the teacher needs to establish an understanding about where the learner's position is, the level which she/he has reached, his/her past experience, and his/her personal goals. As a part of the overall planning process in a teaching session, the teacher also has to define his/her aims of the session, the learning outcomes or objectives, and possibly an evaluation.[20]
The findings of this study showed that although the nursing instructors had to use the clinical evaluation forms for grading the students, some of the instructors were not willing to use them for assessing their students. It seems that since OSCE examination is new for the nursing students and so far the students have not taken clinical examinations under regulations and timing programs, this examination has been hard for them. On the other hand, nursing instructors also have less experience in performing OSCE examination. Besides, they did not give feedback to the students after the examination; as a result, the nursing students are not willing to take this examination. Probably, because students were not familiar with the scenarios of OSCE stations and they think this examination is very hard for them, it is very common that some students find a way to help them pass OSCE examination. Then, they may attempt to cheat in this test.
The importance of a positive atmosphere during the OSCE was strongly emphasized, especially that the feedback should be given in a positive and constructive manner. If a student is to learn from the feedback, this must be given in a motivating manner. A feedback given in a negative way may also influence the performance of the students at the following stations; therefore, he or she does not receive a fair and realistic evaluation.[21] As mentioned by Vaismoradi et al. (2010), another factor for creating dissatisfaction among the participants was the way instructors assessed and evaluated the coursework. Based on the participants’ words, instructors did not care if anyone cheated in coursework. Some students asked other students or translation agencies to do their assignment, but instructors did not check their coursework to find this.[19]
Feedback is believed to be constructive rather than destructive. Feedback may be the effort to discover deficiencies and urge the student to correct their deficiencies which cause educators to more frequently give the student negative feedback.[22] Students want feedback about their performance to gauge progress concerning knowledge, competence, and faculty expectations, and rate giving feedback as an essential quality of an effective clinical teacher. Despite this, there have been many reports of students’ dissatisfaction with the amount and quality of feedback they receive from their teachers.[23]
The present study showed that having enough time for evaluation was very important for the nursing instructors. It also revealed that the nursing instructors were very busy during each semester and did not assign a specific time for evaluation. They do not have enough time to evaluate the student at the end of the semester; therefore, if they had some evaluation tools, they could save time for themselves. One of the clinical evaluation assignments that the nursing instructors have confirmed was the nursing students’ clinical conference presentations. Nursing students complained that clinical conference lecture topics are irrelevant and repetitive. It seems that the nursing instructors do not have information about the previous clinical conferences presented by the students and the conference topics were not selected based on the patients’ diseases; therefore, the nursing students complained about providing and submitting them as a clinical assignment. Some nursing instructors took multiple questions and essay tests for evaluating the students’ clinical knowledge, but because the content of the tests was not quite relevant to what the students learned during the clinical training, the students were not satisfied with these tests.
In accordance with this study, Vaismoradi et al. (2010) reported that the students indicated that the evaluation process did not encourage them to learn beyond what was expected. They were so busy with doing coursework that the aim of translating and reading articles, which was to improve the students’ critical and creative thinking capabilities, was lost. It seemed that the pressure of coursework caused them to be out of breath. Simply, they handed assignment to get rid of them.[19]
The study findings revealed that most nursing instructors do not have enough information about the students before starting each apprenticeship. They also did not have enough information about each student during the completion of the clinical evaluation forms. It shows that they did not have appropriate clinical evaluation devices and did not assess the students based on clinical evaluation forms. Furthermore, they admitted that they had problems in clinical evaluation methods.
Vaismoradi et al. (2010) reported that the participants talked about some kinds of misconduct, which led to injustice during evaluation process. The majority of them used the word “unfair” to portray their experiences of evaluation process. The participants in this study preferred a score to be given based on practical skills criteria, not mastery on theoretical knowledge. Many clinical instructors are reluctant to give unsatisfactory grades to students who do not meet established standards of practice.[19]
The study findings indicated that to gain some nursing competencies, the students need more time to practice and repeat such capabilities. It seems that the duration of the clinical course is short and most clinical instructors are busy during each semester. Consequently, they used most of their time in clinical teaching and complained about their limited time for clinical evaluation; therefore, they did not have time to identify the students’ clinical competencies.
Another important issue that most of the students complained about was that most of the nursing instructors did not observe the educational laws and regulations. They were concerned about lack of coordination among the instructors. Some instructors were serious about absenteeism and tardiness of the students on entering the clinical ward, while some of them did not care about this issue. In addition, the students complained that the nursing instructors did not follow a similar education regulation.
CONCLUSION
Besides focusing on upgrading the current clinical evaluation forms, nursing trainers should improve their knowledge about a complete and comprehensive clinical evaluation. They should also apply other appropriate and objective clinical evaluation methods and tools, and perform a formative and summative clinical evaluation. Also, workload adjustment of the nursing trainers needs revision. Therefore, despite using traditional and sometimes limited evaluation methods for assessing nursing students, a comprehensive and appropriate evaluation of nursing students’ clinical competencies seems necessary.
ACKNOWLEDGMENTS
The authors would like to thank all nursing instructors and the Dean of Nursing and Midwifery School for participating in the study. They also would like to thank Dr. Nasrin Shokrpour at Center for Development of Clinical Research of Nemazee Hospital for editorial assistance. This article is a part of the PhD dissertation of Gazanfar Rafiee, which is financially supported by Shiraz University of Medical Sciences.
Footnotes
Source of Support: The present article was extracted from the thesis written by Ghazanfar Rafiee and was financially supported by Shiraz University of Medical Sciences, grant number: 90-5627
Conflict of Interest: Nil.
REFERENCES
- 1.Dunn SV, Hansford B. Undergraduate nursing student's perceptions of their clinical learning environment. J Adv Nurs. 1997;25:1299–306. doi: 10.1046/j.1365-2648.1997.19970251299.x. [DOI] [PubMed] [Google Scholar]
- 2.Sundstrom H. Manitoba: University of Manitoba Winnipeg; 2000. The characteristics of effective clinical teachers in baccalaureate nursing programs. [Google Scholar]
- 3.Nicol M, Freeth D. Assessment of clinical skills: A new approach to an old problem. Nurse Educ Today. 1998;18:601–9. doi: 10.1016/s0260-6917(98)80056-7. [DOI] [PubMed] [Google Scholar]
- 4.Becker MK, Neuwirth JM. Teaching strategy to maximize clinical experience with beginning nursing students. J Nurs Educ. 2002;41:89–91. doi: 10.3928/0148-4834-20020201-11. [DOI] [PubMed] [Google Scholar]
- 5.Papp I, Markkanen M, Von Bonsdorff M. Clinical environment as a learning environment: Student nurses’ perceptions concerning clinical learning experiences. Nurse Educ Today. 2003;23:262–8. doi: 10.1016/s0260-6917(02)00185-5. [DOI] [PubMed] [Google Scholar]
- 6.Hanleya E, Higginsb A. Assessment of practice in intensive care: Students’ perceptions of a clinical competence assessment tool. Intensive Crit Care Nurs. 2005;21:276–83. doi: 10.1016/j.iccn.2004.10.004. [DOI] [PubMed] [Google Scholar]
- 7.Wallace B. Practical issues of student assessment. Nurs Stand. 2003;17:33–6. doi: 10.7748/ns2003.04.17.31.33.c3375. [DOI] [PubMed] [Google Scholar]
- 8.Khosravi S, Pazargadi M, Ashktorab T. Nursing Students’ viewpoints on challenges of student assessment in clinical Settings: A Qualitative Study. Iran J Educ Med. 2010;11:736–48. [Google Scholar]
- 9.Chambers MA. Some issues in the assessment of clinical practice: A review of the literature Blackwell Science Ltd. J Clin Nurs. 1998;7:201–8. doi: 10.1046/j.1365-2702.1998.00121.x. [DOI] [PubMed] [Google Scholar]
- 10.Willms LC, Sirotnik M. Challenges and Changes in Clinical Evaluation. College Quarterly. 1994;2:7. [Google Scholar]
- 11.Imanipour M, Jalili M. Nursing teachers and students’ perspective about clinical evaluation. Nurs Res. 2012;7:17–26. [Google Scholar]
- 12.Mcnabb DE. 2nd ed. USA: Library of Congress Cataloging-in-Publication Data; 2010. Research methods for political science quantitative and qualitative approaches. [Google Scholar]
- 13.Morse J, Field L. Thousand Oaks, CA: Sage Publications; 2002. Read Me First for a User's guide to Qualitative Methods. [Google Scholar]
- 14.Polit DF, Hungler BP. 7th ed. Lippincott Williams and wilkins; 1999. Nursing research: Principles and Methods. [Google Scholar]
- 15.Guba EG, Lincoln YS. San Francisco: Jossey-Bass; 1981. Effective evaluation. [Google Scholar]
- 16.Norman IJ, Watson R, Murrells T, Calman L, Redfern S. Evaluation of the Validity and Reliability of methods to assess the competence to Practice of Pre-registration Nursing and Midwifery Students in Scotland. Int J Nurs Stud. 2002;39:133–45. doi: 10.1016/s0020-7489(01)00028-1. [DOI] [PubMed] [Google Scholar]
- 17.Indar-Maraj M. Clinical evaluation of nursing students: Challenges and solutions. Med Surg Matters. 2007;16:6–8. [Google Scholar]
- 18.Mahara MS. A perspective on clinical evaluation in nursing education. J Adv Nurs. 1998;28:1339–46. doi: 10.1046/j.1365-2648.1998.00837.x. [DOI] [PubMed] [Google Scholar]
- 19.Vaismoradi M, Parsa-Yekta Z. Iranian nursing students’ comprehension and experiences regarding evaluation process: A thematic analysis study. Scand J Caring Sci. 2010;25:151–9. doi: 10.1111/j.1471-6712.2010.00805.x. [DOI] [PubMed] [Google Scholar]
- 20.McKimm J, Swanwick T. Assessing learning needs. Br J Hosp Med. 2009;70:348–51. doi: 10.12968/hmed.2009.70.6.348. [DOI] [PubMed] [Google Scholar]
- 21.Selby C, Osman L, Davis M, Lee M. Set up and run an objective structured clinical exam. Br Med J. 1995;310:1187–90. doi: 10.1136/bmj.310.6988.1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Elcigil A, Yildirim Sari H. Determining problems experienced by student nurses in their work with clinical educators in Turkey. Nurse Educ Today. 2007;27:491–8. doi: 10.1016/j.nedt.2006.08.011. [DOI] [PubMed] [Google Scholar]
- 23.Rolfe IE, Sanson-Fisher RW. Translating learning principles into practice: A new strategy for learning clinical skills. Med Educ. 2002;36:345–52. doi: 10.1046/j.1365-2923.2002.01170.x. [DOI] [PubMed] [Google Scholar]