

Abstract
Background/Aim:
The Andhra Pradesh Eye disease Study (APEDS) was a conventional cross-sectional study conducted in four locations during 1996-2000. Ten years later, a Rapid Assessment of Refractive Errors (RARE) survey was conducted in one of the geographical regions. The prevalence of visual impairment (VI), uncorrected refractive error (URE), spectacles use obtained from both the surveys was compared.
Settings and Design:
Rural settings; cross-sectional studies.
Materials and Methods:
In both the surveys, distance visual acuity (VA) was assessed using a logMAR chart. Pinhole VA was assessed if presenting VA was <20/20 in APEDS and <20/40 in RARE. VI was defined as presenting VA <20/40 in the better eye. URE was defined as presenting VA <20/40 and improving to ≥20/40 with a pinhole.
Statistical Analysis Used:
Performed using Statistical Package for Social Sciences (SPSS). Chi square tests and t-test were used.
Results and Conclusions:
The results from a RARE survey with 3,095 subjects were compared with an APEDS dataset that had 1,232 subjects in the same age group of 15-49 years. The prevalence of VI has decreased from 9.5% (95% CI, 7.7-11.1) in APEDS to 2.7% (95% CI, 2.1-3.3) in RARE. Similarly, the prevalence of URE in the better eye decreased from 5.8% (95% CI, 4.5-7.1) to 2.3% (95% CI, 1.8-2.8). The usage of spectacles increased from 6.6% (95% CI, 5.2-8.0) to 9.7% (95% CI, 8.7-10.7). There is a decreasing trend in the prevalence of VI and URE in Mahbubnagar district in Andhra Pradesh over a decade.
Keywords: Prevalence, rapid, rapid assessment of refractive errors, spectacles use, uncorrected refractive errors, visual impairment
Visual impairment is a public health challenge that affects over 285 million people worldwide including 39 million blind and 246 million with low vision.[1] Over 43% of the visual impairment is due to uncorrected refractive errors that can be corrected by a pair of spectacles.[1] Service delivery models that address this public health challenge are needed. Epidemiological data are a prerequisite for planning and monitoring eye care services. In Andhra Pradesh, India, a large epidemiological cross-sectional study, the Andhra Pradesh Eye Disease Study (APEDS), conducted during 1996-2000 provided this information and helped in the development of eye care in the region. APEDS was conducted in four regions (one urban and three rural)-Hyderabad, West Godavari district, Adilabad, and Mahbubnagar districts in Andhra Pradesh. In total, 10,293 individuals participated in this study.[2]
It is over a decade since the APEDS was concluded and a new eye care service delivery model was implemented. Understanding the changes in prevalence that has occurred over the past decade can provide insight on the effect of services in addressing the needs of people with visual impairment. A low cost rapid assessment methodology, Rapid Assessment of Refractive Errors (RARE) was conducted in Mahbubnagar district in Andhra Pradesh, India.[3] This rapid assessment method has advantages over other rapid assessment methods, as it provides information on use of spectacles and service providers.[4]
The current paper compares the results obtained from two surveys conducted a decade apart. As RARE was conducted among 15-49 year old age groups, the corresponding subset that included the same age group from the same geographical location (Mahbubnagar district) from APEDS dataset was used for comparison.
Like many other districts in the state, in Mahbubnagar, healthcare facilities in general and primary eye care in particular are restricted to large towns. Ophthalmologists from the neighboring cities visit most of the towns on a regular basis and provide eye care consultations. A few optical outlets are available but the quality of their services is often questionable.[5] Over the past decade, there has been a very steady increase in number of service providers, especially the optical shops in this region.
Materials and Methods
The design and the protocols of APEDS have been published previously.[2] A multi-stage cluster random sampling was used to recruit participants. The selected individuals were transported to a specially designed clinic, where clinical procedures were performed by a team including an ophthalmologist and two optometrists. Distance visual acuity (VA) was measured using a logMAR (logarithm of minimum angle of resolution) chart with the subject's current refractive correction, if being used. Visual Acuity was re-assessed with a pinhole, if VA was less than logMAR 0.0 (20/20) in each eye. In addition, a comprehensive eye examination was conducted on all individuals.
The RARE protocol is a rapid assessment method that was derived from other rapid assessment methods in eye care.[4] A cluster random sampling method was used to select 3,300 individuals aged between 15-49 years from five administrative divisions (mandals) in Mahbubnagar district [Fig. 1]. Two teams, each comprising of a Vision Technician (paramedical ophthalmic personnel trained to provide primary eye care, including refraction) and community eye health workers visited the selected households and performed examination procedures. The detailed examination protocol is described elsewhere.[3] In brief, the examination procedures included, distance VA assessment and use of the pinhole, if presenting VA was less than logMAR 0.3 (20/40). The VA assessment procedure was similar in both APEDS and RARE.
Figure 1.
Map showing the study area
All individuals with visual impairment including those requiring eye care service were referred to the nearby facility for management. Both the study protocols were reviewed and approved by the Institutional Review Board (IRB) of L V Prasad Eye Institute and followed the tenets declaration of Helsinki. APEDS was carried out during 1996 and 2000 and RARE was conducted during the year 2008.
Visual impairment was defined as binocular presenting VA worse than 20/40. Uncorrected refractive error was defined as presenting VA worse than 20/40 but improving to 20/40 or better on using a pinhole. Data management and analysis wase done using Statistical Package for Social Sciences (SPSS) 16.0 (SPSS Inc., Chicago, IL). Point prevalence estimates and 95% CI (confidence intervals) were calculated. Chi-square test and Fisher's Exact Test were used to compare proportions. A t-test was applied to compare the means between the two groups.
Results
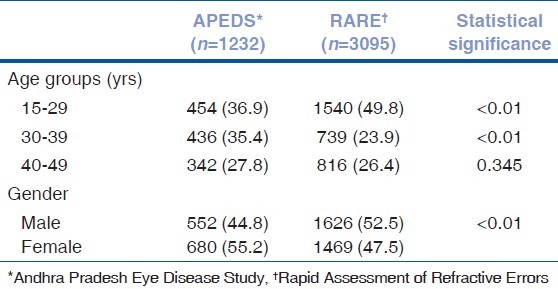
The APEDS dataset had 1,232 subjects (response rate 86%) in the age group of 15-49 years, while RARE sample had 3,095 subjects (response rate-98%). The mean age of the participants in APEDS was higher than in the RARE sample, 32.7 (±9.5 years) versus 30.4 (±10.0 years) years. Nearly 50% of the sample in RARE was between 15 and 29 years of age compared to 37% in APEDS. However, the representation of 40-49 years age group was similar in both the studies. The participation of female subjects was higher in APEDS compared to RARE [Table 1].
Table 1.
APEDS and RARE sample comparison
The age and gender adjusted prevalence of visual impairment was 9.5% (95% CI, 7.9-11.1) in APEDS compared to 2.7% (95% CI, 2.1-3.3) in RARE. Similarly, the prevalence of uncorrected refractive error in the better eye was 5.8% (95% CI, 4.5-7.1) in APEDS compared to 2.3% (95% CI, 1.8-2.8) in RARE. Uncorrected refractive error in either eye was 10.9% (95% CI, 9.2-12.6) and 3.6% (95% CI, 2.9-4.3) in APEDS and RARE, respectively.
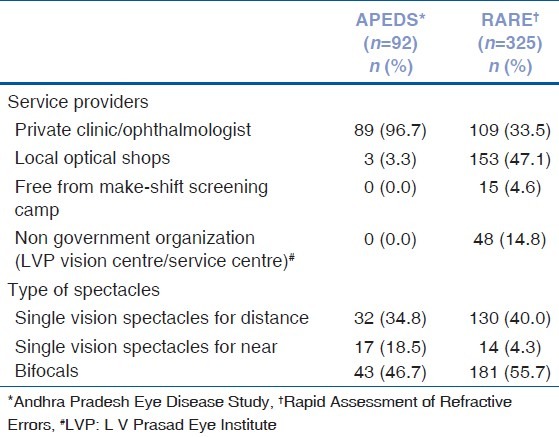
The prevalence of use of spectacles has increased from 6.6% (95% CI, 5.2-8.0) in APEDS to 9.7% (95% CI, 8.7-10.7) in RARE [Table 2]. In APEDS, nearly 97% of the individuals using spectacles reported to have obtained spectacles from private clinic/ophthalmologists, while in RARE, the majority had obtained spectacles from local optical shops [Table 3]. In both the surveys, bifocals were the most common type of spectacles (46.7% in APEDS and 55.7% in RARE).
Table 2.
APEDS and RARE comparison-visual impairment, uncorrected refractive errors and spectacle use
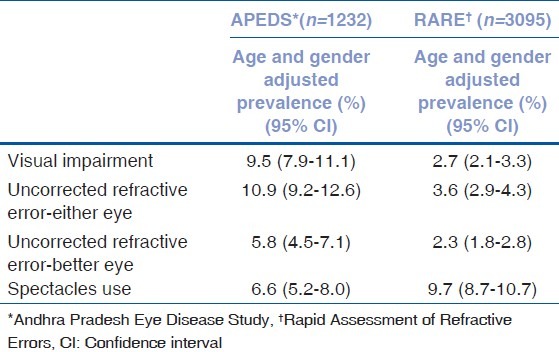
Table 3.
APEDS and RARE comparison-spectacle providers and type of spectacles
Discussion
We found a significant decrease in visual impairment between APEDS and RARE. There was also a significant decrease in uncorrected refractive errors and corresponding with an increase in use of spectacles use in the second survey. These changes can partly be attributed to increased number of service providers and uptake of services in this region over the 10 year period. This change could partially be explained by changing secular trends such as increasing literacy rates, changing health seeking behavior, and other socio economic demographic factors which are difficult to quantify.
The APEDS provided vital data based on which the eye care service delivery model was planned in the region by L V Prasad Eye Institute, Hyderabad, India. This has evolved into the L V Prasad Eye care service delivery pyramid of which the “village vision complex” is an integral part. These complexes consist of one secondary eye care centre linked to 10 vision centres or primary eye care centres, together serving a population of 0.5-1 million.[6] However, a secondary centre was established before the APEDS study was undertaken but the vision centres were established after the APEDS. The vision centres were found to be an important service provider for spectacles in this region.[7,8] In the years following APEDS, several private optical outlets have also been established in the area covered by the survey.
In APEDS, the leading service providers for spectacles were eye doctors while 10 years later RARE revealed that local optical shops had emerged as the leading providers of spectacles. It can be inferred that those who needed spectacles 10 years ago had to travel longer distances as eye doctors were available only in the bigger towns. This is the case even today, however, today optical shops are available in smaller towns and cities and are more numerous compared to the number of eye doctors. Therefore, the cost and convenience to people in procurement of spectacles could be lower now than a decade ago.
We recently published a report that compared the findings from APEDS with a rapid assessment survey and showed a significant decrease in visual impairment, with better visual outcomes after cataract surgery in older individuals.[9] Repeat surveys in The Gambia in 1986 and 1996 reported a 40% relative decrease in the prevalence of blindness.[10] A decrease in the prevalence of blindness is also reported from Nepal over a 10 year period.[11] From these surveys, it can be concluded that there is a general decrease in the prevalence of visual impairment in most areas. The global estimates also reveal a decreasing trend in the prevalence of visual impairment over the years.[1,12]
Research in other areas in public health have demonstrated that rapid assessment provide results that are similar to the conventional sample surveys and are more cost-effective.[13] The conventional epidemiological surveys are expensive and difficult to repeat at regular intervals. Rapid assessment methods can be used, even though they are not as robust and comprehensive as classical cross sectional studies. They are inexpensive and quick which enables repetition at intervals of 5-10 years.
We found that the increase in use of spectacles did not commensurate with decrease in number of people with unaided refractive errors. It is possible that a proportion of people who reported using spectacles may not have significant refractive errors or using spectacles with small powers in either study. This cannot be substantiated as lensometry and refractions were not performed in RARE study.
The major limitation of this study is the comparison of results from two studies that differ in methodology. Ideally, APEDS type of study needs to be repeated to understand the trends in prevalence of visual impairment over time. However, the enormity of the survey with huge resource implication makes it difficult to repeat such study again. The rapid assessment method that we have used provided close estimates on trends in visual impairment over time. Though not as accurate, these estimates are useful for monitoring eye care programmes in developing countries such as India where data from previous studies is available.
Acknowledgments
Authors thank the volunteers who have participated in the study. The authors also thank the vision technician, G Bhaskar, for his assistance in data collection. Dr David S Friedman (Director, Dana Center for Preventive Ophthalmology, Wilmer Eye Institute at Johns Hopkins) is acknowledged for reviewing the earlier drafts of this manuscript.
Footnotes
Source of Support: The financial support for RARE study was provided in part by the Vision Co-operative Research Centre, Australia as part of Srinivas Marmamula's doctoral program and by Hyderabad Eye Research Foundation. APEDS study was supported by Hyderabad Eye Research Foundation, Hyderabad, India, and Christoffel-Blindenmission, Bensheim, Germany.
Conflict of Interest: None declared.
References
- 1.Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96:614–8. doi: 10.1136/bjophthalmol-2011-300539. [DOI] [PubMed] [Google Scholar]
- 2.Dandona R, Dandona L, Naduvilath TJ, Nanda A, McCarty CA. Design of a population-based study of visual impairment in India: The Andhra Pradesh Eye Disease Study. Indian J Ophthalmol. 1997;45:251–7. [PubMed] [Google Scholar]
- 3.Marmamula S, Keeffe JE, Rao GN. Uncorrected refractive errors, presbyopia and spectacle coverage: results from a rapid assessment of refractive error survey. Ophthalmic Epidemiol. 2009;16:269–74. [PubMed] [Google Scholar]
- 4.Marmamula S, Keeffe JE, Rao GN. Rapid assessment methods in eye care: An overview. Indian J Ophthalmol. 2012;60:416–22. doi: 10.4103/0301-4738.100539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Thomas R, Paul P, Rao GN, Muliyil JP, Mathai A. Present status of eye care in India. Surv Ophthalmol. 2005;50:85–101. doi: 10.1016/j.survophthal.2004.10.008. [DOI] [PubMed] [Google Scholar]
- 6.Rao GN. An infrastructure model for the implementation of VISION 2020: The right to sight. Can J Ophthalmol. 2004;39:589. doi: 10.1016/s0008-4182(04)80023-1. [DOI] [PubMed] [Google Scholar]
- 7.Kovai V, Rao GN, Holden B. Key factors determining success of primary eye care through vision centres in rural India: Patients’ perspectives. Indian J Ophthalmol. 2012;60:487–91. doi: 10.4103/0301-4738.100558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kovai V, Rao GN, Holden B, Sannapaneni K, Bhattacharya SK, Khanna R. Comparison of patient satisfaction with services of vision centers in rural areas of Andhra Pradesh, India. Indian J Ophthalmol. 2010;58:407–13. doi: 10.4103/0301-4738.67056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Khanna RC, Marmamula S, Krishnaiah S, Giridhar P, Chakrabarti S, Rao GN. Changing trends in the prevalence of blindness and visual impairment in a rural district of India: Systematic observations over a decade. Indian J Ophthalmol. 2012;60:492–7. doi: 10.4103/0301-4738.100560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Faal H, Minassian DC, Dolin PJ, Mohamed AA, Ajewole J, Johnson GJ. Evaluation of a national eye care programme: Re-survey after 10 years. Br J Ophthalmol. 2000;84:948–51. doi: 10.1136/bjo.84.9.948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sherchan A, Kandel RP, Sharma MK, Sapkota YD, Aghajanian J, Bassett KL. Blindness prevalence and cataract surgical coverage in Lumbini Zone and Chetwan District of Nepal. Br J Ophthalmol. 2010;94:161–6. doi: 10.1136/bjo.2008.155408. [DOI] [PubMed] [Google Scholar]
- 12.Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008;86:63–70. doi: 10.2471/BLT.07.041210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.MacIntyre K. Rapid assessment and sample surveys: Trade-offs in precision and cost. Health Policy Plan. 1999;14:363–73. doi: 10.1093/heapol/14.4.363. [DOI] [PubMed] [Google Scholar]